Embed Size (px)
Citation preview

MYCOTIC & VIRAL KERATITIS
SUGIN GLEN BAISIL JMBBS-PREF INAL YEAR
KANYAKUMARI GOVT. MEDICAL COLLEGE
A AS ARIPALL AM

FUNGAL KERATITIS• Major cause of visual loss on Tropical &
Developing countries
CAUSATIVE ORGANISMSMainly 2 types1. Yeasts (eg. Candida)
Common in Temperate climates2. Filamentous fungi (eg. Fusarium &
Aspergillus)Common in Tropical climates

PREDISPOSING FACTORS
i. Chronic occular surface diseasesii. Long term use of Topical steroidsiii. Contact lens weariv. Systemic immunosuppressionv. Diabetes

Candida & Filamentous KeratitisCLINICAL FEATURES:Symptoms:
• Gradual onset of pain• Grittiness• Photophobia• Blurred vision• Watery/ Mucopurulent discharge

Signs:a) Candida keratitis:
▪ Yellow white densely suppurative infiltrate
▪ Collar stud morphologyb) Filamentous Keratitis:
▪ Grey/Yellow white stromal infiltrate▪ Progressive infiltration with satellite
lesion▪ Feathery branch like extension as a ringshaped infiltrate▪ Rapid progression with thinning &
necrosis▪ Penetration of intact Descemet’s
membrane may occur and lead to endophthalmitis

Candida keratitis▫ yellow white dense infiltrate is
seen

Filamentous keratitis▫ feathery branch like
extension

Other Features: ▪ Epithelial defect ▪ Anterior Uveitis ▪ Hypopyon ▪ Endothelial plaque ▪ Raised IOP ▪ Scleritis ▪ Sterile or Infective
endophthalmitis
Differential diagnosis: □ Bacterial Keratitis □ Herpetic keratitis □ Acanthamoebal keratitis

Investigation:I. Staining:
a) Gram & Giemsa staining (50% sensitive)b) Periodic acid schiff(PAS) Grocott- Gomori Methenamine Silver(GMS)
II. Culture:In Sabouraud’s dextrose agar(Corneal scrapes, contact lenses & cases, etc.)
III. Corneal biopsy:Indication- Absence of clinical improvement for 3-4 days (or) no growth in culture for 1 week
2-3 mm block→ culture & histopathological analysis
IV. Confocal microscopyV. PCR

Treatment:Improvement may be slow compared to bacterial infection
1. General measuresHospital admission-usually
2. Removal of epithelium(to enhance penetration of antifungal drugs)
3. Topical treatment(48 hours)For Candida
Amphotericin B (0.1-0.3%) or Econazole 1% Alt: Natamycin 5%, Fluconazole 2%, Clotrimazole 1%For Filamentous
Natamycin 5% or Econazole 1% Alt: Amphotericin B 0.15%, Miconazole 1%

▪Broad spectrum Antibiotics- to prevent bacterial contamination▪Cycloplegics- for bacterial keratitis
4. Subconjunctival fluconazole- in severe cases5. Systemic antifungals (2-3 weeks)
Voriconazole- 400mg bd for 1 day shift- 200mg bd daily
Itraconazole- 200mg daily shift- 100mg daily
Fluconazole- 200mg BD6. Tetracyclins (Doxycycline-100mg BD)
→Anticollagenase effect in case of thinning7. Superficial keratectomy8. Therapautic penetrating keratoplasty

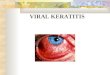
VIRAL KERATITISCommonly includes1) Herpes simplex keratitis2) Herpes zoster ophthalmicus3) Adenovirus keratitis

Herpes Simplex keratitis
Most common cause for blindness in developing countriesHSV-I → by kissing or close contactHSV-II→ to neonates through infected
genitalia of mother

Primary Herpes
1) Skin lesions2) Conjunctiva
▪ Acute follicular Conjunctivitis
3) Cornea ▪ Fine epithelial punctate keratitis ▪ Coarse epithelial punctate keratitis ▪ Dendritic ulcer
Recurrent Herpes
1) Active epithelial keratitis ▪ Punctate epithelial keratitis ▪ Dendritic ulcer ▪ Geographical ulcer
2) Stromal keratitis ▪ Disciform keratitis ▪ Diffuse stromal necrotic keratitis
3) Trophic keratitis(meta-herpetic)
4) Herpetic iridocyclitis

Primary Ocular herpes
Incidence:Occur in a nonimmune personChildren of 6 months to 5 years of age and
in teenagersClinical Features:1) Systemic: Fever, Malaise & non-
suppurative lymphadenopathy2) Skin lesions: Vesicular lesions3) Occular lesions:
▪ Acute follicular conjuctivitis ▪ Keratitis

Recurrent Ocular Herpes
Involvement of trigeminal nervePredisposing factors:▪ Fever▪ Exposure to UV rays▪ General ill health▪ Emotional or physical exhaustion▪ Mild trauma▪ Menstrual stress following steroids and
immunosuppressive drugs administration

Herpes simplex keratitis

Epithelial keratitis (dendritic/geographical)
Symptoms• Redness• Mild discomfort• Photophobia• Watering• Blurred vision

Signs1. Swollen opaque epithelial cells arranged
in coarse or punctate or stellate pattern.2. Central desquamation results in linear
branching ulcer mostly at the centre.3. Ends of the ulcer have characteristic
terminal buds and bed of ulcer skin with fluorescein.
4. The virus laden cells at the margin of the ulcer stain with rose bengal.
5. Corneal sensation is reduced.6. ↑ IOP.7. Mild subepithelial scarring may develop.

Differential diagnosis:• Herpes zoaster keratitis• Healing corneal abrasion• Acanthamoeba keratitis• Epithelial rejection in a corneal graft

Treatment:1) Topical antiviral drugs
▪ Aciclovir 3% ointment. 5 times a day for 14-21 days ▪ Ganciclovir (0.15% gel) 5 times a day until the ulcer heals and then 3 times a day for 5 days ▪ Trifluorothymidine 1% drops 2 hourly until ulcer heals and then 3 times a day for 5 days ▪ Adenine arabinose(Vidarabine) 3% ointment 5 times a day until ulcer heals and then 3 times a day for 5 days.

2) Mechanical debridementCorneal surface is wiped with a
sterile cellulose sponge 2 mm beyond the edge of ulcer
Antivirals must be used in conjunctiva
3) Systemic antiviral drugs ▪ Acyclovir 400 mg p.o. tid to bid, or ▪ Famcyclovir 250 mg p.o. bid, or ▪ Valacyclovir 500 mg p.o. bidfor a period of 10-21 days
4) Interferon monotherapyNucleoside antivirals +
Interferon/debridement

Disciform KeratitisClinical features:Symptoms:▪ Gradual onset of blurred vision▪ Halos around light▪ Discomfort▪ RednessSigns:1. Central zone of stromal edema2. Keratic precipitates underlying3. Folds in descemet’s membrane4. Wessley’s immune ring5. ↑IOP & ↓corneal sensation

Disciform keratitis

Treatment:▫ Diluted steroid eye drops 4-5 times a day
with antivirals(acyclovir 3%) twice a day▫ Non specific & supportive treatment

Necrotizing stromal keratitis
Active viral replication within the stromaSigns:1. Stromal necrosis & melting; profound
interstitial opacification2. Anterior uveitis with keratic precipitates3. Epithelial defect4. Progression to scarring, vascularisation
and lipid depositsTreatment▫ Systemic antiviral drugs for 10-21 days▫ Keratoplasty

Metaherpetic keratitis
▪ Occurs at the site of previous herpetic ulcers
▪ Persistant defect in BM of corneal epithelium
Clinical features1. Indolent linear or ovoid epithelial defect2. Margin- grey/thickenedTreatment▫ Artificial tears▫ Bandage soft contact lens▫ Lid closure(tarsorhaphy)

Herpes Zoster Ophthalmicus
Causative: Varicella zoster virus
Risk of ocular involvement▫ Hutchinson’s sign▫ Age: 6th and 7th decades▫ AIDS - predominant


General features:1. Prodromal phase 3-5 days
tiredness, fever, malaise, headache2. Skin lesions
▫ Midline rashes ▫ Erythematous areas with maculopapular rashes
3. Boggy edema of upper & lower eyelids4. Vesicle → pustule; dry, crest5. Large deep hemorrhagic lesion


Treatment:Systemic therapy:1. Acyclovir 800mg 5 times daily for 10 days2. Strong oral analgesics for treating pain
during first 2 weeks3. Systemic steroids for progressive
proptosis with 3rd nerve palsy & optic neuritis
4. NSAIDs like oxyphenbutazone in severe scleritis

Topical agents: ▪ Antiviral and antibiotic ointments ▪ In case of Herpetic infection,
Dexamethasone 0.1% drops 4 hourly + antiviral ointment 5 times a day + steroid ointment at night
▪ In case of dryness, artificial tears are required

THANK YOU