Embed Size (px)
Citation preview
NHS Eastern Cheshire CCG
Financial Recovery Plan 2016-18

Executive Summary
The financial position of NHS Eastern Cheshire CCG for 2016-17 has been impacted by a number of recurrent and non recurrent pressures. These pressures include additional national commissioning requirements, forecast demand growth in activity/expenditure, settlement of an historic Continuing Health Care funding dispute with Cheshire East Council and a cost pressure transfer from our main provider of care; East Cheshire NHS Trust.
The 2016-17 Financial Plan delivers a £3.8m deficit. In order to deliver this deficit a QIPP (Quality Innovation Prevention and Productivity) Plan designed to deliver the underlying £16.4m required to deliver the NHS England Business Rules of a balanced budget, 1% surplus, 1% non recurrent head room and 0.5% contingency.
The CCG QIPP Plan has been developed to deliver the benefits over a two year timeline with £9.66m savings in 2016-17 with the full £16.4m delivered in 2017-18.
In Year One the CCG Programme is primarily based around the themes of:
• Improving Efficiency and Productivity (Year one £3,522k) (Year two £7,432k);
• Recommissioning Services for Better Value (Year one £1,660k) (Year two £4,246k);
• Decommissioning, Curtailment and One off Benefits (Year one £4,378k) (Year two £1,944k).
In Year Two the benefits of the above themes will continue to be realised but there will be an increased focus upon wider system change through:
• Caring Together Programme (Year one £100k) (Year two £1,307k);
• Wider NHS Reform (Year two £3,519k)
A Turnaround Director has been appointed to oversee the programme and governance arrangements have been developed to drive delivery and provide assurance to the CCG Governing Body. This will be supported by CCG Programme Management Office arrangements.
The CCG has already begun engagement with stakeholders of the likely impact of the schemes within the Programme including members of the public and local politicians. The CCG will commence formal discussions with the local Health and Social Care Overview and Scrutiny Committee in early June and will continue with a constructive approach to engagement throughout the programme.

NHS Eastern Cheshire CCG Financial Plan 2016-17
The CCG Plan for 2016-17 leads to a
deficit position of £3.8m • CHC and Funded Nursing Care (FNC) set at 2015/16 outturn;
• Known pressures that are arising, although not clarified at the point of finalising the Financial Prescribing budget set at 2015/16 outturn;
• Expected growth in contracts (over performance against agreed baseline contracts) to reflect either increases in complexity, case mix or planned contract amendments;
• NHS Business Rules (contingency and 1% Non Recurrent Headroom only);
• Non recurrent expenditure has been removed from the Plan;
• Non recurrent commitments, e.g. CHC Restitution
Key Messages
In 2015-16 the
CCG achieved a
£1.4m surplus .
The plan for
2016-17 delivers
a £3.8m deficit.
With a
challenging QIPP
target of £9.7m
the CCG is
required to
achieve the plan.
(£16.4m is the
total amount
needed to deliver
the NHS England
business rules).
The plans have
been affected by
recurrent and
non recurrent
pressures
including growth
and settlement of
a historic dispute
related to
Continuing
Healthcare
Income Spend (Surplus) /
Deficit
£000s £000s £000s
2015/16 Forecast Outturn (243,837) 242,424 (1,413)
Less Non Recurrent 2,166 (2,778)
Plus 2015/16 Full Year Effect 3,674
2016/17 Additional Spend
Primary Care (tfr) (25,564) 25,564
Recurrent (7,513) 17,290
QIPP (9,660)
Non Recurrent (1,413) 3,500
16/17 Financial Plan (276,161) 280,014 3,853
Table One-A: NHS Eastern Cheshire Clinical Commissioning Group's (ECCCG's) 2016/17
Financial Plan Summary
Category
Within the plan there is a requirement to deliver
£9.7m Quality Innovation Prevention and
Productivity (QIPP) savings. In order to deliver the
NHS England Business Rules QIPP savings of
£16.4m would need to be found.
In setting this plan the following key criteria have
been used:
• Confirmed revenue allocations (income) for the
CCG;
• Provider contracts have been set on either the
2016/17 agreed contract values or estimated
values derived from 2015/16 outturn, adjusted
for the impact of changes to the national tariff
plus any agreed amendments to the services or
values historically commissioned;
Table Two-A: NHS Eastern Cheshire Clinical Commissioning Group's (ECCCG's) 2016/17 Financial
Bridge
2015
/16
Non
Rec
urrent
2015
/16
FYE
Tariff
Gro
wth
Press
ures
Non R
ecurr
ent
Press
ures
Plannin
g Guid
ance
Contin
gency
Productiv
ity
Finalised
Ongoing
£0.4m
20
15
/16
Fo
rec
as
t O
utt
urn
( in
clu
din
g P
rim
ary
Ca
re)
£2
67
,98
8k
20
16
/17
Dra
ft P
lan
£2
80
,01
4k
Income £276,161
£3.7m£3.0m
£1.4m
£9.7m
£3.9m
Deficit
£5.5m £5.3m £5.1m
£2.8m

The Local Health and Social Care Economy is unsustainable
We are now needing to implement the system wide
solutions to deliver the changes needed and the
outcomes we have identified. The partners have
agreed robust governance arrangements and to
assign resource to make this happen.
However; Early economic modelling undertaken by
Ernst & Young have highlighted that even with our
proposed radical service reconfigurations and
productivity gains the development of a sustainable
system remains extremely challenging.
Key Messages
The local health and social care economy has an established “Caring Together” programme which aims to develop a sustainable system
Addressing the wider systems economic challenges will require substantial service and organisational reform, significant productivity gains and potential restrictions to historically funded services/products
The Eastern Cheshire population is
predominately older than the national average,
with 1 in 5 over 65. The number of very elderly
(over 80) is growing more rapidly, when
compared to the English average.
The case for change, underpinned by extensive
and independent modelling completed by McKinsey
– Carnell Farrer. The cumulative deficit is now
projected to grow to as much as £132m by the end
of 2018/19, if we fail to radically transform services
within Eastern Cheshire.
The transformation proposals require significant
system change, organisational change, and major
steps forward in productivity against a care system
already comparable with our peer economies. The
partners in the Eastern Cheshire Health and Social
Care Economy have agreed priorities for the
coming year (Urgent Care, Implementing Integrated
Community Teams, Maternity Care, Paediatric
Services and Specialised Services).
Our work to date has been focussed on identifying
the scale of changes needed and successfully
implementing early infrastructure changes critical to
the long term transformation.

How do we compare with the rest of our peers?
Key Messages
• Eastern Cheshire receives the lowest funding per head in the Cheshire & Merseyside STP area
• We have high levels of residents who are “over 60” and also “over 80” years of age
• We have high rates of disease prevalence in those high cost disease areas most associated with old age such as dementia, cancer and stroke
• Expenditure on Primary Care and most significantly Specialised Services is having a negative impact on the CCG funding allocation (distance from target)
Need Funding Area Indicator England NHS Eastern
Cheshire CCG
NHS
South
Cheshire
CCG
NHS Vale
Royal CCG
NHS West
Cheshire
CCG
NHS
Warrington
CCG
NHS
Wirral
CCG
NHS
Halton
CCG
NHS
Knowsley
CCG
NHS
South
Sefton
CCG
NHS
Southport
and
Formby
CCG
NHS St
Helens
CCG
NHS
Liverpool
CCG
1 Percentage aged 60-79 18 23 21 21 22 19 21 20 18 21 25 21 16
2 Percentage aged 80+ 4.9 7 5 5 6 4 6 4 5 6 8 5 4
3
Annual percentage
growth in population
aged 60-79
1 1 1 1 1 1 1 2 1 1 1 1 1
4
Annual percentage
growth in population
aged 80+
2 3 3 3 3 3 2 3 3 3 3 3 2
Cancer 2 2.7 2.7 2.6 2.7 2.3 2.5 2.3 2.5 2.6 3.2 2.6 2.1
COPD 2 1.6 1.8 2.3 1.8 1.8 2.4 2.8 3.5 2.8 2 3 2.9
CHD 3 3.5 3.7 3.7 3.5 3.6 3.9 4.3 4.4 4.2 4.2 4.5 3.6
Dementia 1 1 0.8 0.7 0.8 0.7 0.9 0.7 0.7 0.8 1.1 0.8 0.7
Diabetes (17+) 6 5.9 6.3 6.5 6.3 6.2 6.8 7.6 7 6.5 6.4 7.1 6
Obesity (16+) 9 7 8.7 11 9.1 8.5 10.4 12.3 11 10.8 8.7 11.1 10.6
Stroke/TIA 2 2.1 2.1 1.9 2 1.7 2.2 1.9 1.7 2 2.3 1.9 1.7
Number in Upper Quartile 3/7 2/7 2/7 1/7 0/7 3/7 4/7 4/7 3/7 4/7 4/7 1/7
DFT (Financial
difference £m)
-ve £36m
to +£83m-8.7 -9.5 -4.5 -9.1 -5.1 -11.4 5.5 11.5 12.5 3.6 -0.5 40.1
DFT (%)-ve 5% to
30%-3.43 -4.14 -3.65 -2.7 -1.87 -2.3 2.98 4.59 5.56 2.07 -0.17 5.5
DFT (Financial
difference £m)
-ve £9m
to +£10m0.7 0.8 -0.0 1.5 -0.3 0.1 -0.0 6.8 -1.5 -0.0 1.1 -6.5
DFT (%)-ve 12%
to +29%2.9 3.8 -0.4 4.7 -1.3 0.3 -0.1 29 -6.8 -0.3 4 -11.3
DFT (Financial
difference £m)
-ve £24m
to +£31m8.8 3.2 1.7 3.9 -0.8 5.7 1.2 1.9 5 0.7 2.9 5
DFT (%)-ve 25%
to +23%17.62 8.59 7.56 6.98 -1.51 7.1 3.61 4.06 10.7 2.37 6.04 3.37
Funding allocations
received by CCGs
Funding allocations aligned
to CCGs for Primary Medical
Care
Funding allocations aligned
to CCGs for Specialised
Services
Distance from target -
closing FY 16/17
Distance from target -
closing FY 16/17
Distance from target -
closing FY 16/17
5
Population Characteristics
for Healthcare needed
Elderley Poplation %
Disease Prevalence (for
high cost disease
categories)

Are we efficient when compared to comparator CCGs in our STP footprint or national peers?
Are there other opportunities?
• The CCG is currently funded 3.43% below the target funding allocation however, we know that there
are CCGs with lower “funding per head of population” who are not in financial deficit; the CCG will use
benchmarking and peer review of “like CCGs” in order to identify how they have reduced their
expenditure.
• The national “Right Care” programme indicates further opportunities exist to improve outcomes and
productivity however the resource intensity will mean this will be planned to commence later in the year.
• Shared initiatives with our commissioning and provider organisations will enable savings to be
generated at a system level as well as being fully aligned with our Caring Together transformation
initiative.
Where we are in the top Quartile nationally?
• Eastern Cheshire CCG has the lowest rate of emergency admissions (and emergency bed days used per 1000 population).
• The second highest recovery rate for Improving Access to Psychological Therapies (IAPT).
• We have the highest rate of Annual Health Checks for people with a Learning Disability.
• We have the second most people feeling supported to manage their long term condition.
• Second best prescribing of antibiotics in primary care.
• Third best survival from cancer after one year.
• Fourth highest rates of Dementia diagnosis.
• Lowest levels of childhood obesity.
• We have the second lowest levels of elective and day case admissions in our national CCG Peer Group.
Key Messages
In terms of financial productivity opportunities the CCG generally performs well against peers
Eastern Cheshire CCG has very low levels of elective and emergency hospital admissions and bed days used
The type of change required will need to be more radical to address our health economy deficit
Where can we be more efficient?
• Compared to national peers we can reduce
levels of first outpatient attendance (whilst
above the mean for England not in the upper
quartile).
• Patients with diabetes being compliant with
NICE treatment targets.
• Sixth lowest access levels to IAPT.
• Second most people per 1000 population
eligible for CHC.
• Highest rates of Delayed Transfers of Care

What factors have led to the CCG planning for a £3.8m deficit?
The deterioration of the CCG’s financial position compared to 2015/16 can be related to three main contributing factors:
• 2016/17 CCG allocation;
• Non-recurrent costs;
• Sustainability & Transformation Costs.
The 2016/17 CCG Allocations resulted in an unanticipated deterioration in the CCG’s “distance from target” allocation which when combined with the place based allocation and associated overspend in specialised commissioning resulted in an allocation uplifted lower than planned for, based on NHSE 2015/16 allocation information.
In addition the 3.0% growth contained a number of non-recurrent commitments previously funded separately by NHSE (GPIT) or mandated in the 2015/16 Planning Guidance (Mental Health). The net available funding growth was therefore insufficient to cover the mandated tariff uplifts and the general cost pressures which are projected to occur particularly in relation to CHC, Prescribing and Acute Hospital expenditure.
Within the CCG plans there are significant non recurrent cost pressures; including settlement of a historical dispute in relation to Continuing Health Care (CHC) with Cheshire East Council (CEC).
Key Messages
Even delivering a
significant QIPP
of £9.7m leaves a
deficit position
meaning the true
CCG figure is
£16.2m
The underlying
Eastern Cheshire
Health and Social
Care Economy
deficit
(commissioner
and provider) is
materially higher
and is projected
to reach £132m
by 2018-19
QIPP plans will
enable the CCG
to fulfil our
financial duties by
the end of 2017-
18
The CCG is seeking to address long term
sustainability issues within the economy as
articulated in its Five Year Strategic Plan and the
Caring Together Programme.
During 2015/16 and in 2016/17 the CCG has
disproportionately funded the local economy costs of
transformation. In addition, a number of actions
taken within/outside the CCG’s control have
materially impacted on 2016/17. For example: Our
main care provider (East Cheshire NHS Trust) has a
significant underlying financial deficit and as part of
the 2016-17 contract settlement a number of
financial pressures have been transferred to the
CCG. These include funding for Intermediate
Care bed based services, Stroke Services,
Specialist Nurse services and Appliances.
In all cases the CCG intend to either transform
(recommission) services to mitigate the impact or
have projected, through this recommissioning, there
will be benefits realisation however this will not
materialise until 2017/18
The requirement for the CCG to restructure PMS
contracts in 2015/16 was successfully completed
and recommissioned through a new Primary Care
contract which will not fully yield a return on
investment until 2017/18.

Developing Our Recovery Plan
The scale of the financial challenges in Eastern Cheshire require commitment from all partner agencies to deliver significant productivity improvement as individual statutory bodies, in partnership within the Caring Together Transformation Programme, and as part of wider potential management and system reform.
For the purpose of this Recovery Plan: all three areas are referenced, in this Executive Summary but the majority of the focus in the remaining pages is on the CCG’s own delivery.
CCG Financial Recovery (QIPP) Plan
In order to achieve a £3.8m deficit the CCG needs to deliver an in-year QIPP of £9.7m which is a significant step change in delivery against previous years (in 2015-16 the level achieved was £2.4m).
Key Messages
Even delivering
a significant
QIPP of £9.7m
leaves a deficit
position
meaning the
true CCG figure
is £16.2m
QIPP plans will
enable the CCG
to fulfil our
financial duties
by the end of
2017-18
In addition to the £9.7m QIPP required to
achieve the £3.8m deficit in 2016-17 a higher
QIPP level of £16.2m will be required to deliver
the NHS England business rules (of a 1%
surplus and 0.5% contingency and1% Non
Recurrent “head room”). This will be delivered
by the end of 2017-18.
The reality is that to deliver this scale of QIPP in
the current year then plans equating to a much
higher value are need to account for the part
year effect that will occur as projects are
implemented. The CCG will therefore develop
QIPP plans which also support the position in
2017-18.
The table below summarises how the CCG will
focus on three distinct areas to deliver its
recovery plan. Further work is on-going to
identify additional QIPP opportunities in all three
areas
Qtr 1 Qtr 2 Qtr 3 Qtr 4 Qtr 1 Qtr 2 Qtr 3 Qtr 4
£655 £1,395 £622 £3,522 £1,855 £3,709 £5,566 £7,432
£20 £136 £622 £1,660 £1,061 £2,123 £3,184 £4,246
£102 £283 £1,182 £4,378 £354 £707 £1,590 £1,944
2016-17 (£000s) 2017-18 (£000s)Cumulative Benefits
Improving Efficiency
and Productivity
Recommmissioning
for Better Value
Decommissioning,
Curtailment and One
Developing Our Recovery Plan
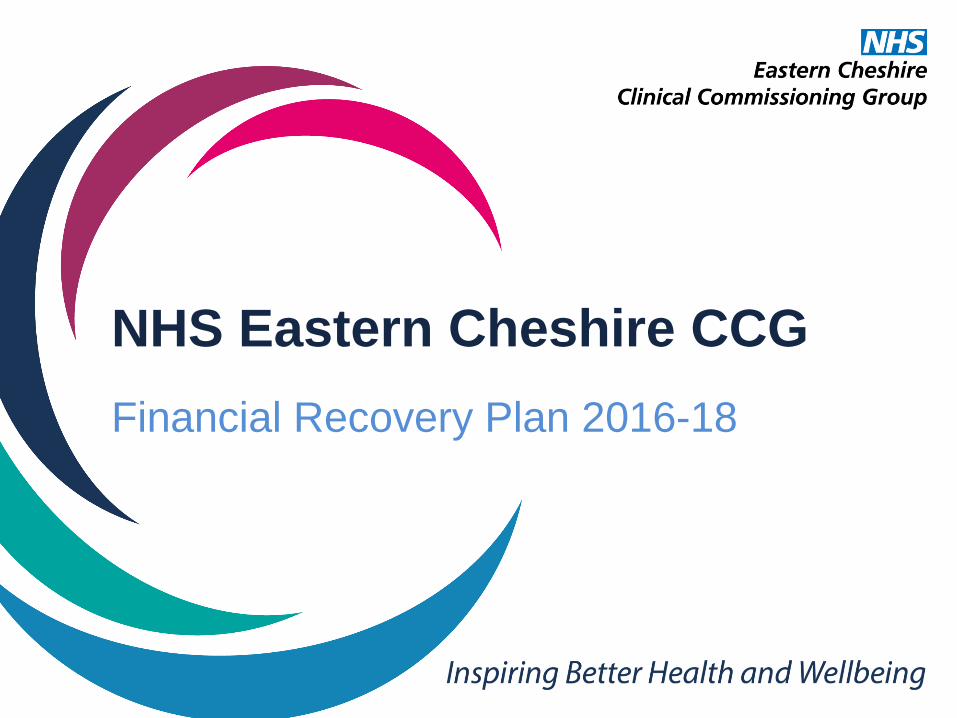
Caring Together Programme The development and introduction of Integrated Health and Social Care Community Based Coordinated Care is a key element of the programme and is strongly based on international evidence. Without investment, roll-out in 2016/17 will be based on existing resources, significantly curtailing the greater QIPP benefits and the pace to releasing costs. This also includes some of the benefits associated with investment in Primary Care as the infrastructure to work with practices will not be in place to the scale or speed we would ideally like. Other wider economic benefits from large scale change are not reflected in this recovery plan, as they are contingent on decisions taken outside the statutory authority of the CCG.
Key Messages
The underlying Eastern Cheshire Health and Social Care Economy deficit (commissioner and provider) is materially higher and is projected to reach £132m by 2018-19
The most material area of “excess” expenditure is specialised services (£8.8m / 17%) and needs to be a core part of our financial recovery
Wider NHS System QIPP Opportunities
The CCG is committed to wider management
efficiencies through the STP and CWW Alliance and is
key to explore economies of scale in QIPP, and
potentially the establishment of a cluster type
arrangement.
The significant overspend (17%) in specialised
services in Eastern Cheshire represents the single
highest area of potential productivity gain. The CCG is
keen to explore and enter a gain share agreement to
release significant savings to the economy.
The table below provides indicative costs of the wider
system opportunities which are possible and included
in our QIPP programme for 2016-18.
Qtr 1 Qtr 2 Qtr 3 Qtr 4 Qtr 1 Qtr 2 Qtr 3 Qtr 4
£0 £30 £60 £100 £326 £653 £979 £1,307
£0 £0 £0 £0 £878 £1,757 £2,635 £3,519
Grand Total £778 £1,843 £2,486 £9,660 £4,474 £8,949 £13,955 £18,448
Cumulative Benefits 2016-17 (£000s) 2017-18 (£000s)
Caring Together
Programme
Wider NHS Reforms

Improving Productivity and Efficiency
Initiative Description2016-17
(£000s)
2017-18
(£000s)
Delivery
due
Project
Lead
Clinical
Lead
Exec
Sponsor
1
Delivering the productivity
benefits in the Primary Care
Contract
The contract delivers a reduction in diagnostics, secondar
care referrals and non elective activity £1,565 £3,001 Q2
Dean
Grice
Dr Mike
Clark
Neil
Evans
2Medicines Management
Efficiencies
Schemes include policies on over the counter
medications, switches in medication (including high cost
drugs) and efficiency schemes.
£799 £1,371 Q2Janet
Kenyon
Dr Graham
Duce
Neil
Evans
3 Invoice validation efficiencies
The CCG has agreed a more advanced programme of
invoice challenges with GEM and Arden CSU which will
ensure the CCG is only billed for approproate activity.
£200 £200 Q1Lana
Davidson
Dr James
Milligan
Neil
Evans
4 Urgent Care Access Changes
Through changes in the new GP contract and a review of
exsiting "low complexity" urgent care activity a saving in
A&E/MIU activity is being delivered.
£150 £300 Q2Bernadet
te Bailey
Dr Mike
Clark
Neil
Evans
5Repatriation of out of area AMD
treatment
Patients currently accessing out of area services have
been contacted to offer local services commissioned
using a local specification/tariff
£102 £160 Q1Lana
Davidson
Dr James
Milligan
Neil
Evans
6 Running CostsOpportunities to control running cost expenditure have
been applied as part of the annual planning process£200 £250 Complete
Sammy
Brown
Not
Applicable
Jerry
Hawker
7Direct Access Pathology
Efficiencies
Working with Keele University, Cheshire Pathology
Services and Clinicians a review of test usage is taking
place to improve the efficiency of test ordering in
Primary Care
£50 £150 Q2Lana
Davidson
Dr James
Milligan
Neil
Evans
8
Benchmarking of Commissioning
by CCGs at same funding level and
Right Care Programme
Opportunities
The CCG is researching the "programme budgeting"
approach of CCGs funded in the lowest 10% nationally in
order to apply learning. In addition new right care
initiatives will be developed with support from the
national support team (when available to the CCG)
£456 £2,000 Q4Juliet
Thomson
Dr Mike
Clark
Neil
Evans
Subtotal £3,522 £7,432
IMPROVING PRODUCTIVITY & EFFICIENCY

Recommissioning for Better Value
Initiative Description2016-17
(000)
2017-18
(000)
Delivery
due
Project
Lead
Clinical
Lead
Exec
Sponsor
1
Intermediate Care/Community
Beds commissioned in line with
national levels of expenditure
The costs of intermediate care have risen and the current
model is neither clinically nor financially sustainable.
Benchmarking shows the expenditure is considerably
higher than national peers. A revised model will be
developed with the expenditure reduced accordingly.
£800 £1,000 Q2Jo
Williams
Dr Julia
Huddart
Jacki
Wilkes
2
Continuing Healthcare Approvals
and Review Processes and
Contracting Improvements
A combination of schemes are being delivered including:
Revised access policies to CHC and Personal Health
Budgets, Contracting Processes and a review of high cost
individual packages
£275 £638 Q1Sally
Rogers
Karen
Smith
Neil
Evans
3
Clinical Treatment Thresholds and
Procedures of Limited Clinical
Value
Implementation of national and international best
practice approaches is to be researched and applied. The
CCG will assess the need to change access/treament
thresholds to a wide range of services.
£200 £1,500 Q3Julia
Curtis
Dr Mike
Clark
Neil
Evans
4
Recommission Community
Musculoskeletal Services
(including Physiotherapy)
The CCG has served notice on current Community
Physiotherapy and Musculoskeletal services and is
redesigning/reprocuring them with a forecast 25% saving.
£162 £324 Q2Sarah
Sewell
Dr Imran
Ahmed
Fleur
Blakeman
5Recommissioning of Primary
Mental Health services (IAPT)
Existing services have been decommissioned from
October 2016 and a procurement process is underway.£125 £250 Q2
Emma
Leigh
Dr Ian
Hulme
Jacki
Wilkes
6
Relocation of Acute Stroke
Services and Community
Rehabilitation
Currently additional non-recurrent funding is being used
to maintain safety in the East Cheshire Trust Stroke
Service. From Quarter 3 our two main Tertiary Providers
will provide all hospital based stroke care and the CCG
will shift investment into community based care with a
net financial benefit; in addition to improving clinical
outcomes.
£0 £400 Q3Jacki
Wilkes
Dr Julia
Huddart
Jacki
Wilkes
7
Mental Health Reablement
Contract with local Housing
Provider
Following a review of the service a revised contractual
and care package arrangement are being negotiated.£18 £54 Q1
Lana
Davidson
Dr Ian
Hulme
Alex
Mitchell
8 Non PTS transport Following a procurement process the CCG expenditure
has reduced.£80 £80 Complete NA NA
Alex
Mitchell
Subtotal £1,660 £4,246
RECOMMISSIONING FOR BETTER VALUE

Decommissioning, Curtailment and One off benefits
Initiative Description2016-17
(000)
2017-18
(000)
Delivery
due
Project
Lead
Clinical
Lead
Exec
Sponsor
1Suspension of planned
investment in CAHMS
In previous years the CCG has increased funding into
CAMHS services and will therefore not increase in line
with national guidance
£409 £409 Complete NA NAJacki
Wilkes
2 Systems Resilience Prioritisation
The SRG has reviewed previous years schemes to assess
the most effective plans for 2016-17. Schemes not
delivering sufficient return on investment have been
decommissioned
£301 £448 Q1Karen
Burton
Dr Julia
Huddart
Jacki
Wilkes
3
Withdraw support to Cheshire
East Council for Mental Health
Reablement
Following assessment of the return on investment of this
funding it has been withdrawn£231 £347 Q1
Alex
Mitchell
Dr Ian
Hulme
Alex
Mitchell
4Withdraw grants to "deprioritised
commissioning areas"
A full review of all discretionary grant payments has
taken place and services decommissioned£147 £211 Complete Complete
Dr Julia
Huddart
Jacki
Wilkes
5 Non Recurrent Headroom
It is expected that during Quarter 4 NHS England will
release the 1% Non Recurrent Headroom and this has
been factored into plans
£2,761 £0 Q4Niall
O'Gara
Not
Applicable
Alex
Mitchell
6 Quality Premium AchievementAn estimate of the projected income from the 2015-16
scheme£529 £529 Complete
Julia
Curtis
Dr James
Milligan
Sally
Rogers
Subtotal £4,378 £1,944
DECOMMISSIONING, CUTAILMENT AND ONE-OFF BENEFITS

Caring Together & Wider NHS Schemes
Initiative Description2016-17
(000)
2017-18
(000)
Delivery
due
Project
Lead
Clinical
Lead
Exec
Sponsor
1Community Based Coordinated
Care implemented
Caring Together Partners are working together on a
revised implementation programme to reflect that
"pump-priming" investment is not available
£0 £1,057 Q4 B BaileyDr Paul
Bowen
Fleur
Blakeman
2Achieving a DTOC level < 7% of
bed stock
DTOC levels in Eastern Cheshire are significantly above
acceptable standards contributing to wider economy
costs and excess bed days costs to the CCG. Improved
efficiency and capacity utilisation will resease costs
£100 £250 Q3Jackie
Wilkes
Dr Julia
Huddart
Jerry
Hawker
Sub total £100 £1,307
Initiative Description2016-17
(000)
2017-18
(000)
Delivery
due
Project
Lead
Clinical
Lead
Exec
Sponsor
1
Establishment of a single
Cheshire CCG "cluster
board/alliance" to reduce
Governing Body and running costs
The CCG will explore with our Governing Body, other
CCGs and NHS England whether the "running cost"
economies that could be generated from a reduced
number of CCGs outweighs the loss of local focus in
commissioning
£0 £1,069 2017-18 TBCDr Paul
Bowen
Jerry
Hawker
2 Specialised Services
NHS England allocations indicate that the CCG overspends
against our target allocation by 17% (£8.8m). This directly
impacts on the wider allocation and the CCG intends
working on a joint programme with NHS England to
address this
£0 £2,200 Q4 TBCDr Mike
Clark
Neil
Evans
3
Development of Commercial
Service sponsorship
arrangements (research and
innovation)
The CCG is working with the Academic Health Science
Network and has appointed a Lead Clinician to bring
external investment into the CCG area.
£0 £250 Q4Neil
Evans
Dr Pete
Wilson
Neil
Evans
Subtotal £0 £3,519
Stretch
Total£9,660 £18,448
Wider Partner & NHS System Reform
Caring Together Transformation Programme
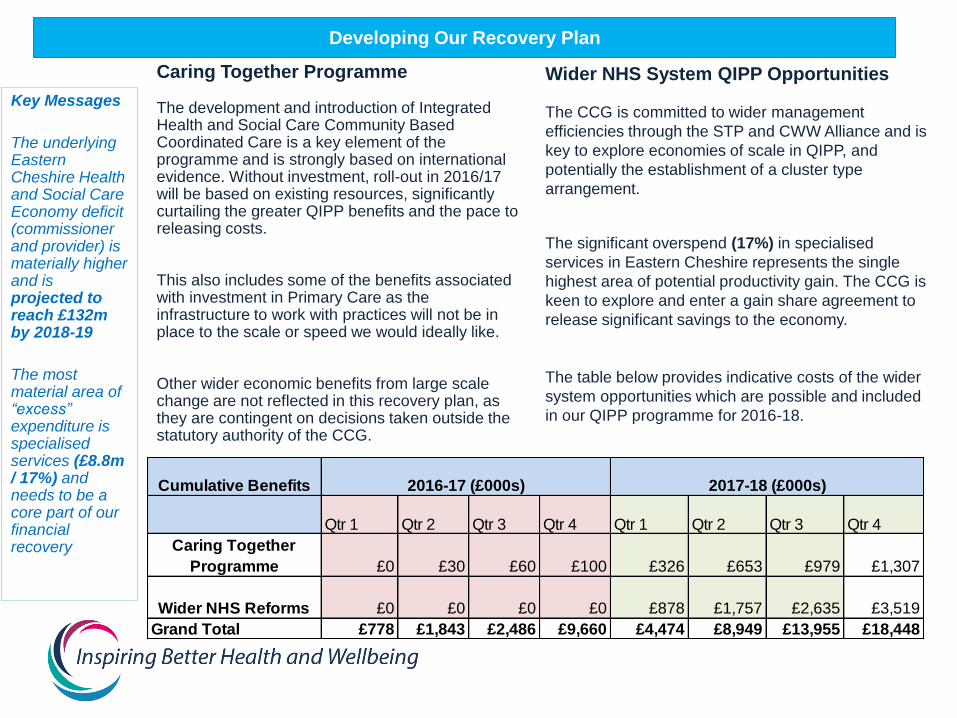
How will the CCG be assured that the programme is being delivered?
Governance Structure Diagram
In order to provide impetus and assurance as to the delivery of
the CCG QIPP plans the CCG has responded by reassigning
resources to this programme. This is through a combination of a
dedicated “Turnaround Team” and clear accountability for those
schemes being managed outside of this team.
Neil Evans, an Executive Director, has been appointed to the role
of “Turnaround Director” and released from a range of existing
commitments to concentrate on delivery of our QIPP Programme.
Supporting this post will also be Dr Mike Clark, who is a Senior
GP and is an existing member of the CCG Governing Body and
Executive Team.
The core Turnaround Team will comprise of Programme
Management Office, Project Managers, Finance, Communications
and Engagement, Clinicians and Medicines Management.
The Governing Body will receive monthly updates on progress
implementing the QIPP plans with a direct line of assurance
through the CCG Governance and Audit Committee. The Lay
Member Chair of the GAC will take a lead assurance role.
The CCG Finance Committee will operationally hold the
Turnaround Team to account with the Clinical Quality and
Performance Committee assessing scheme Quality/Equality
Impact Assessments and ensuring that the programme does not
detrimentally affect quality, including compliance with National
Care Standards such as the NHS Constitution.
CCG
Governing
Body
Clinical
Quality and
Performance
Committee
Finance
Committee
QIPP
Development
Group
QIPP (Turnaround) Team
Accountable Director - Neil Evans
Executive Clinical Lead – Dr Mike
Clark
HealthVoice
Governance
and Audit
Committee
Executive
Committee

Managing Risk
The £9.7m QIPP for 2016-17 is based on a
national assumption as to the levels of savings
expected from CCGs in financial deficit. The
deliverability is recognised as containing a high
level of risk. In 2015-16 the CCG achieved a
£2.4m QIPP plan which is less than a quarter of
what is required to deliver the 16-17 plan.
An independent assessment of QIPP plans by
PWC identified a £5.8m to £6.5m of schemes
were at risk of delivery. A particular challenge is
the “part year” nature of benefits realisation.
Whilst schemes may benefit the commissioner‘s
financial position they may have a detrimental
impact on service providers.
Some of the schemes may require consultation
which may impact upon implementation.
It is recognised that the longer term financial
viability of the local health economy needs
radically different models of care. There is a
danger that the CCG focus on short term financial
savings at the expense of long term sustainable
change.
Whilst growth has been built into 2016-17 plans, if
it exceeds forecast levels then this would increase
the savings value required. “Business as Usual”
Key Messages
The levels of
savings within
the QIPP plan is
very ambitious
and has a high
margin of risk
(based on
internal and
external
assessment)
There is a need
to maintain focus
on
transformational
change in order
to achieve long
term financial
sustainability
Emerging
pressures will be
managed
closely to ensure
that the CCG
position is
delivered
activity processes and delivery will be closely monitored to ensure that we constrain growth in activity/expenditure.
Mitigating Actions To increase the pace of delivery additional resource is being assigned to this programme through redeployment and recruitment to temporary posts. The CCG is also planning schemes which will deliver into 2017-18 in order to maximise delivery next year. A clear governance process and accountability for delivery (see slide 7) will assist in increasing the effectiveness and speed of delivery. The CCG Governing Body will be directly assured as to progress in delivering the QIPP Programme. The role of the Governance and Audit Committee and Finance Committee will ensure that initiatives are delivered to plan. In addition the Finance Committee provides direct oversight of any new emerging pressures in order they will not counteract the benefits being realised through the QIPP Programme. Stakeholders will be actively engaged in order to ensure that the wider system plans are aligned to those of the CCG. The Caring Together governance arrangements will support this. The CCG is already engaging with our public as well as local politicians to gain support for plans in a timely way.

Communication and Engagement
Working in partnership with our public and clinicians
Some of the changes associated with our programme of work are likely to be sensitive to specific populations and therefore a proactive approach to engaging our public, and local stakeholders is required.
NHS Eastern Cheshire CCG has a vibrant independent advisory group who have been supporting the CCG in development of our commissioning plans for sometime. This approach has been built upon to develop QIPP plans. The group provides a public and service user perspective on plans enabling plans to be challenged and refined.
www.echealthvoice.info/
The CCG holds a monthly forum with our Member Practices; Locality Meeting of which QIPP is a standing item for discussion. This includes delivering the benefits associated with the new Primary Care Caring Together contract.
Fortnightly meetings are being held with a combination of clinicians and members of the public. This allows Project Managers to present initiatives for refinement.
The CCG has already sent a number of key individuals on training to show how to run effective public consultation processes. Where more specialist consultation advice is needed the CCG will procure this externally. Midlands and Lancashire CSU provide the CCG with expertise in relation to Equality Impact Assessments.
The CCG has already held discussions with the Chair and Lead Officer responsible for the Cheshire East Health and Social Care Overview and Scrutiny Committee (OSC) to agree how best to engage with OSC and the first proposals are being taken to OSC in June 2016.
Local politicians are also to be engaged proactively through their involvement in our Caring Together Programme and regular meetings and briefings with local MPs.
A public awareness campaign is being developed and the CCG has arranged briefing sessions with local journalists to engage them in positively supporting this process.
Headlines
In order to
deliver our
programme in
an effective and
timely way a
proactive
approach to
communications
and
engagement will
be required.
Existing
relationships
and forums will
be utilised with
more targeted
approaches
developed for
individual
schemes