Embed Size (px)
Citation preview

By:Pratik yadavMDS 1st yrDept of orthodontics

INTRODUCTION
The development of dentition is an important part of craniofacial growth as the formation, eruption, exfoliation and exchange of teeth take place during this period. This helps in assimilation of facts, predictions of teeth
eruption , the factors influencing them and implicate clinically for treatment .

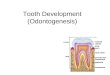
PRE-NATAL DEVELOPMENTOF TEETH
The embryonic oral cavity is lined by stratified squamous epithelium known as the oral ectoderm
Around the 6th week of intra uterine life, the infero-lateral border of maxillary arch and supero- lateral border of mandibular arch shows localised proliferation of oral ectoderm resulting in the formation of a horse-shoe shaped band of tissue called dental lamina
Dental lamina plays a important role in the development of dentition


In certain areas the dental lamina proliferate
and forms knob like structure that grows into underlying mesenchyma.
Each knob represents a future deciduous tooth and is called enamel organ
Enamel organ passes through a number of stages ultimately forming the teeth
Based on shape of the enamel organ develops can be divided into,
Bud stage Cap stage Bell stage

BUD STAGE Differentiation of dental lamina leads to formation of round,
ovoid swelling at 10 different points corresponding to future position of deciduous teeth. These are the primordia of enamel organ.
Enamel organ consists of peripherally located low columnar cells and centrally located polygonal cells.
Dental papilla : It is the area of ectomesenchymal condensation subjacent to enamel organ. Cells of dental papilla will form tooth pulp & dentine.
Dental sac: It is area of ectomesenchymal condensation surrounding the tooth bud & dental papilla. Cells of dental sac will form cementum & periodontal ligament.



Bud Stage

CAP STAGE : Characterized by a shallow invagination of deep surface
of a bud. Cuboidal cells cover the convexity of the cap
outer enamel epithelium. Columnar cells cover the concavity of the cap
Inner enamel epithelium.
Stellate Reticulum: Polygonal cells begin to separate as more
intercellular fluid is produced and forms cellular network called stellate reticulum.
Enamel Knot: Cells in center of the enamel organ are densely packed.
This knot projects towards underlying dental papilla . Vertical extension of enamel knot forms enamel cord. Both the structures disappear before enamel formation begins.

Cap Stage of Tooth
Development Dental (enamel) organ
Dental papilla
Dental follicle
©Copyright 2007, Thomas G. Hollinger, Gainesville, Fl

BELL STAGE :
1. The cell of inner enamel epithelium differentiate into tall columnar tissue called ameloblast
2. A few layers of flat squamous cells are seen between stelate reticulum and inner enamel epithelim this layer is called stratum intermedium
3. Stellate reticulum expands due to accumulation of intra cellular fluid , they r star shaped & as the enamel formation stars it collapse to a narrow zone thereby reducing the distance between inner & outer enamel epithelium
4. Before inner enamel epithelium begins to produce enamel, the peripheral cells of the dental papilla differentiate into odontoblast


FORMATION OF ROOT
Root start forming after dentin formation has reached future cementoenamel junction. Both dental organ and dental papilla play part in formation of root.
Hertwig's epithelial root sheath :
* The outer and inner dental epithelium meets one another at future cervical area and is called cervical loop.* This cervical loop forms epithelial sheath of Hertwig, which moulds the shape of the root and initiates dentin formation.

The root sheath consists of only outer and inner dental epithelium.
The inner layer of cells remains short and do not produce enamel. These cells induce the differentiation of cell of dental papilla into Odontoblasts, which lay a layer of dentin. At the same time the continuity of Hertwig's sheath is destroyed due to infiltration of connective tissue and the root sheath breaks up into small strands of epithelium called epithelial rests of Molassez.
While the coronal part of the sheath degenerates, the apical part continues to grow in length and aid in lengthening of root.

Occlusion Term occlusion is derived from the Latin word, “occlusio”; defined as the relationship between all the components of the masticatory system
in normal function, dysfunction and parafunction.
An ideal occlusion is the perfect interdigitation of the upper and lower teeth, which is a result
of developmental process consisting of the three main events, jaw growth, tooth formation
and eruption

EvolutionTo develop a functional occlusion it became necessary for the teeth and bones to develop
synchronously. Over a period of time there was loss or fusion of cranial and facial bones, the number of bones have reduced and the dental formula has also
undergone changes.

Periods of Occlusal DevelopmentOcclusal development can be divided into the following
development periods:
o Neo-natal period.o Primary dentition period.o Mixed dentition period.o Permanent dentition period.

Neonatal Period(lasts upto 6 months after birth)

Gum Pads• Alveolar processes at the time of birth- gum pads.
• Pink in colour, firm and are covered by a dense layer of fibrous periosteum.

Gum Pads contd…• The gum pad soon gets segmented by a groove called transverse groove, & each segment is a developing tooth site.
•The pads get divided into ‘labio-buccal’ & ‘lingual portion’, by a dental groove.
• The groove between the canine and the 1st molar region is called the lateral sulcus, useful for judging the inter arch relationship at a very early stage.

Gum Pads contd…The upper gum pad is horse shoe
shaped & shows:o Gingival groove: separates
gum pad from the palate.o Dental groove: starts at the
incisive papilla, extends backward to touch the gingival groove in the canine region & then
moves laterally to end in the molar region.o Lateral sulcus.

Gum Pads contd…
The lower gum pad is ‘U’ shaped and rectangular,
characterized by:o Gingival groove: lingual extension of the gum pads.o Dental groove.o Lateral sulcus.

Relationship of Gum Padso Anterior open bite is seen at rest with contact only at the molar region.
o Complete overjet.
o Class II pattern with maxillary gum pad being more prominent.
o Mandible is distal to the maxilla of 2.7 mm- male and 2.5- female. ( Sillman JH 1938)
oThe range of variation of this distal relationship is from 0 to 7 mm. . ( Sillman JH 1938)

Relationship of Gum Pads
o Mandibular lateral sulci lies posterior to maxillary lateral sulci.
o Mandibular functional movements are mainly vertical, and to a little extent antero-posterior. Lateral movements are absent.

Neonatal Jaw RelationshipA ‘precise bite’ or jaw
relationship is not yet seen. Therefore, neonatal jaw
relationship cannot be used as a diagnostic criterion for
reliable prediction of subsequent occlusion in the
primary dentition.

Status of Dentition at Birth

Precociously Erupted Primary Teeth
Natal tooth Neonatal teeth
Pre-erupted teeth’ or ‘Early Infansive teeth’ are teeth that erupt during the 2nd or 3rd month.

Natal/neonatal teeth
Classification Hebling (1997) classified natal teeth into 4 clinical categories:
1. Shell-shaped crown poorly fixed to the alveolus by gingival
tissue and absence of a root;
2. Solid crown poorly fixed to the alveolus by gingival tissue and little or no root;
3. Eruption of the incisal margin of the crown through gingival
tissue
4. Edema of gingival tissue with an unerupted but palpable
tooth.

Gender Predilection for females Kates et al (1984) reported a 66% proportion for females
against a 31% proportion for males.
EtiologyIt has been related to several factors, such as:- Superficial position of the germ Infection or malnutrition Eruption accelerated by febrile incidents or hormonal
stimulation, Hereditary transmission of a dominant autosomal gene hypovitaminosis

Natal/neonatal teeth
Complications Interfere with feeding Risk of aspiration Traumatic injury to the baby’s tongue
and/or to the maternal breast Riga-Fede disease- oral condition
found, rarely in newborns manifests as an ulceration on the ventral surface of the tongue or on the inner surface of the lower lip. Caused by trauma to the soft tissue from erupted baby teeth.
Riga-Fede disease

Diagnosis A radiographic verification of the relationship
between a natal and/or neonatal tooth and adjacent structures, nearby teeth, and the presence or absence of a germ in the primary tooth area would determine whether or not the tooth belongs to the normal dentition ( Almeida CM et al 1997)
Most natal and neonatal teeth are primary teeth of the normal dentition and are not supernumerary teeth ( Brandt Sk et al 1983)
Correspond to teeth of the normal primary dentition in 95% of cases, while 5% are supernumerary (Hawkins C 1932)

Treatment If the erupted tooth is diagnosed as a tooth of the normal
dentition -- maintenance of these teeth in the mouth is the first treatment option, unless this would cause injury to the baby (Chow MH 1980, Roberts MW 1992)
When well implanted-- these teeth should be left in the arch and their removal should be indicated only when they interfere with feeding or when they are highly mobile, with the risk of aspiration (Toledo AO 1996)
Reasons for removal -- The risk of dislocation and consequent aspiration, traumatic injury to the baby’s tongue and/or to the maternal breast, (Kates GA et al 1984)

Martins et al (1998) suggested smoothing of the incisal margin to prevent wounding of the maternal breast during breast feeding.
If the treatment option is extraction, certain precautions should be taken :
Avoiding extraction up to the 10th day of life to prevent hemorrhage
Assessing the need to administer vitamin K before extraction (0.5-1.0 mg IM)
Considering the general health condition of the baby Avoiding unnecessary injury to the gingiva Being alert to the risk of aspiration during removal.

Primary Dentition Period(From around the 6th month to 6 years)

Sequence of Eruption

Primary(upper)
First evidence of calcification(Weeks in utero)
Crown completed(months)
Eruption(months)
Root completed(years)
Central 14 (13-16) 11/2 10 11/2
Lateral 16 21/2 11 2
Canine 17 9 19 31/4
1st molar 151/2 6 16 21/2
2nd molar 19 11 29 3
Chronology of Primary Dentition
Wheelers…

Primary(Lower
First evidence of calcification(Weeks in utero)
Crown completed(months)
Eruption(months)
Root completed(years)
Central 14 (13-16) 21/2 8(6-10) 11/2
Lateral 16 3 13( 10-16) 11/2
Canine 17 9 20(17-23) 31/4
1st molar 151/2 51/2 16( 14-18) 21/4
2nd molar 18 10 27 3
Wheelers…

Status of Dentition(during primary dentition period)

At around 5 – 6 Years There are 48 teeth/parts of teeth present in the jaw. It is at this
time that there are more teeth in the jaws than at any other time.

Features Of Primary Dentition
• Spacing- 2 types of dentition are seen:•A) Spaced dentition - usually seen in the deciduous dentition to accommodate the larger permanent teeth in the jaws.
• More prominent in the anterior region, and are called ‘physiological spacing’ or ‘developmental spacing’.• Absence of spaces in the primary dentition is an indication that crowding of teeth may occur when the larger permanent teeth erupt.

Features Of Primary Dentition contd…
• Most subhuman primates have it through out life and use it for interdigitation of the opposing canines. This space is used for early mesial shift.
primate spaces’, ‘simian spaces’ or ‘anthropoid spaces’.

Features Of Primary Dentition contd…
Shallow overjet & overbite. Initially a deep bite may occur due to the fact that the deciduous incisors are more upright than their successors. The lower incisal edges often contact the cingulum area of the maxillary incisors. This deep bite
is later reduced by:oEruption of deciduous molars.oAttrition of incisors.oForward movement of the mandible due to growth.

Features Of Primary Dentition contd…
Almost vertical inclination of anteriors.

Features Of Primary Dentition contd…
Ovoid arch form.

Molar RelationshipThe molar relationship in the primary dentition can be classified
into 3 types:oStraight/flush terminal plane.oMesial step.oDistal step.

Flush Terminal Plane• If the distal surface of maxillary and mandibular deciduous second molars are in the same vertical plane; then it is called a flush terminal plane
• Normal molar relationship in the primary dentition, because the mesiodistal width of the mandibular molar is greater than the mesiodistal width of the maxillary molar.

Mesial Step
Distal surface of mandibular deciduous second molar is mesial to the distal surface of maxillary deciduous second molar.

Distal Step
Distal surface of mandibular second deciduous molar is more distal to the distal surface of the maxillary second deciduous molar

Mixed
Dentition
Period

Mixed Dentition Period(Around 6 years- 12 years)
The mixed dentition period can be divided into three
phases:
o First transitional period.
o Inter-transitional period.
o Second transitional period.

First Transitional Period

Eruption of 1st Permanent MolarThe location & relation of the 1st permanent molar depends much upon the distal surface of the upper & lower 2nd deciduous molar.

Transition to Class I Molar Relation
The shift in lower molar from a flush
terminal plane to a class I relation can
occur in two ways:
oEarly shift.
oLate shift.

Early Shift• Early shift occurs during the early mixed dentition period.
• Since this occurs early in the mixed dentition, it is called early shift , the eruptive force of first permanent molar push the deciduous 1st & 2nd
deciduous molar to close the primate space .

Late ShiftThis occurs in the late mixed
dentition period when the second deciduous molar
exfoliate the first permanent molar drift mesialy & use
leeway space and is thus called late shift.

Leeway Space of Nance
• Described by Nance in 1947
Maxilla: 0.9 mm/segment = 1.8 mm. Mandible: 1.7 mm/segment = 3.4mm.

Secondary spacing
• Term was coined by Baume
• Observed in closed primary dentition
• Secondary spacing can also occur during the eruption of permanent central incisors

Distal Step
When the deciduous second molars are in a distal step, the
permanent first molar will erupt into a class II relation.
This molar configuration is not self correcting and will cause a class II malocclusion despite Leeway space and differential
growth.

Mesial Step
Primary second molars in mesial step relationship lead to
a class I molar relation in mixed dentition. This may
remain or progress to a half or full cusp class III with
continued mandibular growth.

Exchange of IncisorsDuring the first transitional period the deciduous incisors are replaced by the permanent incisors. The mandibular central
incisors are usually the first to erupt. The permanent incisors are considerably larger than the deciduous teeth they replace. This
difference between the amount of space needed for the accomodation of the incisors and the amount of space available
for this, is called ‘Incisal liability’.
The incisal liability is roughly about 7.6 mm in the maxillary arch & about 6 mm in the mandibular arch (Wayne).

Transition of IncisorsThe incisal liability is over come by the
following factors:Interdental physiological spacing in the primary incisor region.
(4 mm in maxillary arch & 3 mm in mandibular arch)

Transition of Incisors contd…
Increase in inter-canine arch width: Significant amount of growth occurs with the eruption of
incisors and canines.

Transition of Incisors contd…Increase in anterior length of the dental arches:
Permanent incisors erupt labial to the primary incisors to obtain an added space of around 2-3 mm.

Transition of Incisors contd…
Change in inclination of permanent incisors:
Primary teeth are upright but permanent teeth incline to the labial surface, thus decreasing
the inter-incisal angle from about 151 degrees in the
deciduous dentition to 124 degrees in the permanent
dentition. This increases the arch parameter.

Inter-Transitional Period
This is a stable phase where little changes take place in the dentition. The teeth present are the permanent incisors and first molar along with the deciduous canines and molars. This phase
prepares for the second transitional phase. Some of the features of this stage are:
o Any asymmetry in emergence and corresponding differences in height levels or crown lengths between
the right and left side teeth are made up.

Inter-Transitional Period contd…
Root formation of emerged incisors, and molars
continues, along with concomitant increase in alveolar process height.

Inter-Transitional Period contd…
Resorption of roots of deciduous canines and
molars.

Second Transitional Period
The second transitional period is characterized by the replacement of the deciduous molars and canines by the premolars and permanent
canines respectively.
At around 10 years of age the deciduous canines shed, but just before the shedding
there is a transient or self correcting malocclusion seen in the maxillary incisor
region between the age of 8 – 9 years.

Ugly Duckling Stage(Broadbent’s phenomenon)
Around the age of 8 - 9 years, a midline diastema is commonly seen in the upper arch, which
is usually misinterpreted by the parents as a malocclusion.
Its typical features are:oFlaring of the lateral incisors.oMaxillary midline diastema.

Ugly Duckling Stage contd…
Crowns of canines on young jaws impinge on developing
lateral incisor roots, thus driving the roots medially and
causing the crowns to flare laterally.

Ugly Duckling Stage contd…
The roots of the central incisors are also forced together, thus causing a maxillary midline diastema.

Ugly Duckling Stage contd…
With the eruption of the canines, the impingement from
the roots shift incisally thus driving the incisor crowns
medially, resulting in closure of the diastema as well as the correction of the flared lateral
incisors.

Ugly Duckling Stage contd…Hence this unaesthetic metamorphosis, eventually leads to an
aesthetic result.

Self correcting anomalies

Sequence of EruptionThe canines in the upper arch erupt only after the premolars
have replaced the deciduous molars, whereas the canine erupt before the premolars in the lower arch.

Second Transitional Period contd…
Favorable occlusion in this area is largely dependent on:
o Favorable eruption sequence.o Satisfactory tooth size to available
space ratio.o Attainment of normal molar
relation with minimum diminution of space available for the bicuspids.

Second Transitional Period contd…
Eruption of permanent second molars Before emergence- second molars, oriented in a mesial &
lingual direction
Teeth- formed palatally, guided into occlusion by Cone Funnel mechanism , upper palatal cusps (cone) slides into the lower occlusal fossa (funnel)
Arch length is reduced by mesial eruptive forces
Thereby, crowding if present is accentuated

The Permanent Dentition Period

The Permanent Dentition
This period is marked by the eruption of the four permanent
second molars.

The Permanent Dentition contd…
Calcification begins at birth with the calcification of the cusps of the first permanent molar and extends as late as
the 25th year of life. Complete calcification of incisor crowns take place by 4 – 5 years and
of the other permanent teeth by 6 – 8 years except for third
molars.

Permanent(Upper)
First evidence of calcification ( weeks in utero)
Crown completed(months)
Eruption( months)
Root completed(years)
Central 3-4 mo 4-5 yr 7-8 yr 10
Lateral 10-12 mo 4-5 yr 8-9 yr 11
Canine 4-5 mo 6-7 yr 11-12 yr 13-15
1st premolar 11/2-13/4 yr 5-6 yr 10-11 yr 12-13
2nd premolar 2-21/4 yr 6-7 yr 10-12 yr 12-14
1st molar At birth 21/3-3 yr 6-7 yr 9-10
2nd molar 21/3-3 yr 7-8 yr 12-13 yr 14-16
3rd molar 7-9 yr 12-16 yr 17-21 yr 18-25
Chronology of Permanent Dentition
Wheelers…

Permanent(Lower)
First evidence of calcification ( weeks in utero)
Crown completed(months)
Eruption( months)
Root completed( years)
Central 3-4 mo 4-5 yr 6-7 yr 9
Lateral 3-4 mo 4-5 yr 7-8 yr 10
Canine 4- 5 mo 6-7 yr 9-10 yr 12-14
1st premolar 13/4-2yr 5-6 yr 10-12 yr 12-13
2nd premolar 21/4-21/2 yr 6-7 yr 11-12 yr 13-14
1st molar At birth 21/2-3yr 6-7 yr 9-10
2nd molar 21/2-3yr 7-8 yr 11-13 yr 14-15
3rd molar 8-10 yr 12-16 yr 17-21 yr 18-25
Wheelers…

The Permanent Dentition contd…
The permanent incisors develop lingual to the
deciduous incisors and move labially as they erupt.

The Permanent Dentition contd…
The premolars develop below the diverging roots of the
deciduous molars.

The Permanent Dentition contd…
At approximately 13 years of age all
permanent teeth except third molars are fully erupted.

Features of Permanent Dentition
Coinciding midline. Class I molar relationship.

Features of Permanent Dentition contd…
Vertical overbite of about one third the clinical crown height of the mandibular central
incisors. Overjet and over bite decreases throughout the second decade of life
due to greater forward growth of the mandible.

Andrews keys to normal occlusion
Key I – Molar relationship
MB cusp of the max 1st molar falls into the mesiobuccal groove of the mand 1st molar and that the distal surface of the DB cusp of the upper first permanent molar should make contact and occlude with mesial surface of the MB cusp of the lower second molar.

Andrews keys to normal occlusion
Key II Crown angulation (Tip)
The angulation of the facial axis of every clinical crown should be positive
The gingival portion of the long axis of the all crowns must be distal than the incisal portion.

Andrews keys to normal occlusion
Key III Crown inclination
In upper incisors, the gingival portion of the crown’s labial surface is lingual to the incisal portion.

Andrews keys to normal occlusion
Key IV – Rotations
The fourth key to normal occlusion is that the teeth should be free of undesirable rotations.

Andrews keys to normal occlusion
Key V – Tight contacts
contact points should be tight
(no spaces).
In absence of abnormalities such as genuine tooth size discrepancies, contact point should be tight.

Andrews keys to normal occlusion
Key VI – Occlusal plane or curve of spee
The curve of Spee should have no more than a slight arch.
Intercuspation of teeth is best when the plane of occlusion is relatively flat.
A deep curve of spee results in a more contained area for the upper teeth, making normal occlusion impossible.

Andrews keys to normal occlusion
Key VII – Correct tooth size or the bolton’s ratio
Bennett and McLaughlin in 1993 gave seventh key to normal occlusion. i.e. the upper and lower tooth size should be correct.

Thank
You.