Embed Size (px)
DESCRIPTION
Contrast induced nephropathy (CIN) is agenerally reversible form of acute kidney injury (AKI) that occurs soon after the administration of radiocontrast media.
Citation preview

By
Waleed Abd El-Malek El-Refaey
Ass. Lecturer of Internal Medicine and Nephrology
Faculty of Medicine
Tanta University

• Contrast-induced nephropathy (CIN) is a generally reversibleform of acute kidney injury (AKI) that occurs soon after theadministration of radiocontrast media.
• After intravascular CM injection, immediate renal toxicitymay occur, and in most cases it remains fortunately free ofsignificant clinical consequences.
Sandler CM. Contrast-agent-induced acute renal dysfunction – is iodixanol the answer? N Engl J Med. 2003;348(6):551–3.

of CIN includes:
Mehran R, Nikolsky E. Contrast-induced nephropathy: definition, epidemiology, and patients at risk. Kidney Int Suppl. 2006(100):S11–5.
an absolute increase in serum creatinine of ≥0.5 mg/dL or a ≥25% relative increase
in serum creatinine from
the baseline value
at 48–72 hours after exposure
to contrast agent, peaks at
3–5 days
in the absence of alternative
causes for acute kidney
injury

1 2 3 4 Weeks
SerumCreatinine
In most cases, the decline in renal
function is mild and transient
S. Cr. usually returns
to the baseline value
after 1–3 weeks
Some patients have
a persistent decline
in renal function and
require RRT
(in patients with CIN risk factors)

Incidence of CIN
Risk Factors
Contrast Dose
Type of Radiologic procedure
Contrast Type

• According to the US FDA, the incidence of renal failure aftercontrast administration, ranged from 0.6% to 2.3%.
• However, rates of CIN may be as high as 50%, depending onthe presence of well characterized risk factors, the mostimportant of which are baseline chronic renal insufficiencyand DM.
Rihal CS, Textor SC, Grill DE, et al. Incidence and prognostic importance
of acute renal failure after percutaneous coronary intervention.
Circulation. 2002;105(19):2259–2264.


• The Pathogenesis of CIN is multifactorial.

Risk factors for the development of CIN

• A decreased incidence of contrast nephropathy appears to beassociated with nonionic agents, which, are either low osmolal(500 to 850 mosmol/kg) or iso-osmolal (approximately 290 mosmol/kg).
Lautin EM, Freeman NJ, Schoenfeld AH, et al. Radiocontrast-associated renal dysfunction: a comparison of lower-osmolality and conventional high-osmolality contrast media. AJR Am J Roentgenol 1991;157:59.

Iodine containing
agents
Iodine content
OsmolarityDegree of
polymerization Level of
ionization Viscosity

Iodixanol, the only currently available iso-osmolal nonionic contrast agent(approximately 290 mosmol/kg), may be associated with a lower risk of nephropathythan some low-osmolal agents, particularly iohexol

• Most of the studies indicate that the higher volume of CM isespecially deleterious in the presence of other risk factors , withlower doses of contrast being safer, but not free of risk.
• Even relatively low doses of contrast (less than 100 ml) can inducepermanent renal failure and the need for dialysis in patients withchronic kidney disease.
Vlietstra RE, Nunn CM, Narvarte J, Browne KF. Contrast nephropathy after coronary angioplasty in chronic renal insufficiency. Am Heart J 1996; 132: 1049–1050.

• In this study, low dose was defined by a formula as:
• However, diabetic patients with a serum creatinine concentration >5 mg/dL (440 micromol/L) may be at risk from as little as 20 to 30 mL of contrast.

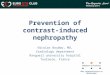
To assess the cumulative risk of several variables on renalfunction, a simple CIN risk score that could be readily applied wasdeveloped.

Mehran R, Aymong ED, Nikolsky E, et al. A simple risk score for prediction of contrast-induced nephropathy after
percutaneous coronary intervention: development and initial validation. J Am Coll Cardiol 2004;44:1393-9.
Predicting the Risk of CIN after PCI
CIN

• There is no specific treatment once CI-AKI develops, andmanagement must be as for any cause of ATN, with the focus onmaintaining fluid and electrolyte balance.
• The best treatment of contrast-induced kidney injury isprevention.

Indication for contrast-based
procedures
potentialrisk of CIN

• Consider alternate Imaging studies not requiring iodinatedcontrast medium.
• The use of lower doses of low- or iso-osmolal nonionic contrastagents and avoidance of repetitive studies that are closely spaced(within 48 to 72 hours).
• Avoidance of volume depletion.

• Concomitant nephrotoxic drugs such as NSAID and nephrotoxicantibiotics, ACEI and diuretics should be discontinued 48 hoursprior to contrast administration.
• Metformin should be discontinued on the day of the proposedCM administration and for the subsequent 48 hours.


Goals of Hydration
Maintenance of sufficient intravascular volume to increase
renal perfusion
Establishment of adequate diuresisprior to contrast media
Avoidance of hypotension

• Isotonic saline is superior to one-half isotonic saline since isotonicsaline is a more effective volume expander.
• In a study by Mueller et al, intravenous administration of isotonicsaline was found to be superior, compared with half-isotonicsaline, in reducing the rates of CIN after percutaneous coronaryintervention (0.7% versus 2%, respectively).
Mueller C, Buerkle G, Buettner HJ, et al. Prevention of contrast media-associated nephropathy: randomized comparison of 2 hydration regimens in 1620 patients undergoing coronary
angioplasty. Arch Intern Med. 2002;162(3):329–336.

• Since alkalinization may protect against free radical injury, the possibility that sodium bicarbonate may be superior to isotonic saline has been examined in a number of randomized trials and meta-analyses.
• The results were conflicting as some showed a significantly lower rate of contrast-induced nephropathy with sodium bicarbonate, while others found equivalent rates.
• Briguori C, Airoldi F, D'Andrea D, et al. Renal Insufficiency Following Contrast Media Administration Trial (REMEDIAL): a randomized comparison of 3 preventive strategies. Circulation 2007; 115:1211.
• Vasheghani-Farahani A, Sadigh G, Kassaian SE, et al. Sodium bicarbonate plus isotonic saline versus saline for prevention of contrast-induced nephropathy in patients undergoing coronary angiography: a randomized controlled trial. Am J Kidney Dis 2009; 54:610.

Hydration with Saline
IVF = 1 mL/kg/hr (MAX 100 ml/hr) 12 hours pre & 12 hours post contrast
CHF or left ventricular ejection fraction (LVEF) < 40%?0.5 ml/kg/hr (max 50 ml/hr) 12 hrs pre & post contrast
Emergent procedure? (suggested regimen):Fluid bolus of 3ml/Kg prior to procedure. Hydration during procedure and/or 12 hrs after if possible (dependent on clinical status)

• Given that an increasing number of individuals receive contrast asoutpatients, this trial has evaluated the effectiveness of oral hydrationin preventing contrast nephropathy.
• 53 patients were randomly assigned to either unrestricted oral fluids orto normal saline at 1 mL/kg per hour for 24 hours beginning 12 hoursprior to the scheduled catheterization . AKI was significantly morecommon with oral hydration (35 versus 4 %).

Bicarbonate Dosing
IVF = 150 meq of sodium bicarbonate in 850 ml of D5W
3 ml/kg bolus (MAX 300 ml) 1 hour prior to procedure and 1 mL/kg/hour (MAX 100 ml/hr) during and for 6 hours post-procedure.
Glycemic control issues (including patients with diabetes)?Consider mixing sodium bicarbonate in 1 liter of sterile water instead of D5W

Methods to guide fluid repletion
Left ventricular end-diastolic pressure RenalGuard System
• Brar SS, Aharonian V, Mansukhani P, et al. Haemodynamic-guided fluid administration for the prevention of contrast-induced acute kidney injury: the POSEIDON randomised controlled trial. Lancet 2014; 383:1814.
• Briguori C, Visconti G, Focaccio A, et al. Renal Insufficiency After Contrast Media Administration Trial II (REMEDIAL II): RenalGuard System in high-risk patients for contrast-induced acute kidney injury. Circulation 2011; 124:1260.

Left ventricular (LV) end-diastolic pressure

Left ventricular (LV) end-diastolic pressure
• A randomized trial tested the benefit of a fluid replacement protocolguided by LV end-diastolic pressure among patients with CKD and otherrisk factors for CIN.
• In this trial, 350 patients were assigned to LV end-diastolic pressure-guided fluid management or to a control group.
• All patients received intravenous isotonic saline 3 mL/kg for one hourprior to cardiac catheterization. LV end-diastolic pressure wasdetermined in all patients prior to administration of contrast.

Left ventricular (LV) end-diastolic pressure
• Both groups received intravenous fluid throughout and for four hours following the procedure.
IV infusion rate
LV end-diastolic pressure
<13 mmHg
5 mL/kg/hour
13 - 18 mmHg
3 mL/Kg/hour
>18 mmHg
1.5 mL/Kg/hour
Control 1.5 mL/kg/hour
Contrast-induced AKI occurred less
frequently in the LV end-diastolic
pressure group, compared with
control (6.7 versus 16.3, respectively).

RenalGuard system

RenalGuard system
• The RenalGuard™ System is a real-time measurement and matchedfluid replacement device designed to accommodate the RenalGuardtherapy, which is based on the theory that creating and maintaining ahigh urine output is beneficial by allowing a quick elimination ofcontrast media, and, therefore, reducing its toxic effects.
Patients with
eGFR≤30 mL /min
or a risk score ≥11
Control group
NaHco3 + NAC
RenalGuard group
Isotonic saline + NAC + furosemide

RenalGuard system
• Contrast-induced acute kidney injury occurred in 16 of 146 patients in the RenalGuard group (11%) and in 30 of 146 patients in the control group (20.5%).
• Conclusion:
RenalGuard therapy, including hydration with normal saline plus high doses of NAC in combination with a limited (0.25 mg/kg) dose of furosemide, seems to be an effective renoprotective strategy for patients at high risk for CI-AKI.

Nephroprotective drugs
• There are great heterogeneity and conflicting results in theavailable clinical trials and meta-analyses examining theeffectiveness of acetylcysteine in the prevention of contrastnephropathy .
• Being a precursor for glutathione synthesis, NAC has the potentialto diminish oxidative stress by directly scavenging superoxideradicals and increasing intracellular glutathione.
Drager LF, Andrade L, Barros de Toledo JF, Laurindo FR, Machado Cesar LA, Seguro AC. Renal effects of N acetylcysteine in patients at risk for contrast nephropathy: decrease in oxidant stress-mediated renal tubular
injury. Nephrol Dial Transplant. 2004;19(7):1803–7.

Nephroprotective drugs

Nephroprotective drugs
• This trial studied 83 patients with chronic renal insufficiency whowere undergoing computed tomography.
• Patients were randomly assigned either to receive the antioxidantacetylcysteine (600 mg orally twice daily) and 0.45 percent salineintravenously, before and after administration of the contrastagent, or to receive placebo and saline.
• Conclusion:
Prophylactic oral administration of acetylcysteine, along withhydration, prevents the reduction in renal function induced bythe contrast.

Nephroprotective drugs
• 2308 patients undergoing angiography received eitheracetylcysteine (1200 mg orally twice daily) or placebo on the daybefore and after angiogram.
• Patients had at least one of the following risk factors: age >70years, CKD, diabetes mellitus, heart failure or LV ejection fraction<45 percent, or shock.
• There was no difference in the development of CI-AKI (12.7percent in both groups).

Nephroprotective drugs
Since the agent is potentially beneficial, well tolerated, and relatively inexpensive, 2012KDIGO guidelines that suggest administration of acetylcysteine to patients at high risk.
Acetylcysteine Dosing
Tolerating PO intake?600-1200 mg capsules PO Q12h X 4 doses2 doses pre-contrast and 2 doses post-contrast is optimalEmergent Procedure?1 dose before and 3 doses post cath or procedure is acceptable (Q12h x 4 doses total)IV Acetylcysteine?600-1200 mg IV x 1 over 15 minutes, then 600-1200 mg PO/PT q12h x 4 doses post-procedure: For a high risk patient undergoing cardiac catheterization or PE protocol CT scan with no PO access

Nephroprotective drugs
• Statins may improve endothelial function, reduce arterialstiffness, and reduce inflammation and oxidative stress.
• There are no sufficient data to support the use of statins solely forthe prevention of contrast nephropathy.
Sugiyama M, Ohashi M, Takase H, et al. Effects of atorvastatin on inflammation and oxidative stress. Heart Vessels 2005; 20:133.

Nephroprotective drugs
• 2998 patients with type 2 diabetes and CKD were assigned to receiverosuvastatin or to a control group prior to a diagnostic angiogram withor without percutaneous intervention.
• Patients assigned to rosuvastatin received 10 mg daily two days priorand three days after the scheduled procedure.
• Contrast-induced was less common among patients assigned torosuvastatin compared with control (2.3 versus 3.9 percent,respectively).

Nephroprotective drugs
• A prospective, single-center study of 304 patients with baselineestimated creatinine clearance <60 ml/min were randomized to receiveatorvastatin 80 mg/day or placebo for 48 hours before and 48 hoursafter contrast medium administration.
• All patients received intravenous saline hydration and oral N-acetylcysteine 1,200 mg 2 times/day.
• CIN occurred in 31 patients, 16 (11%) in the placebo group and 15 (10%)in the atorvastatin group (no benefit of atorvastatin compared withplacebo).

Vasoactive drugs
• Low-dose dopamine failed to show a protective effect on renal functionin patients undergoing contrast media exposure, and was evenassociated with a deleterious effect on the severity of renal failure andits duration.
Gare M, Haviv YS, Ben-Yehuda A, et al. The renal effect of low-dose dopamine in high-risk patients undergoing coronary angiography. J Am Coll Cardiol. 1999;34(6):1682–1688.

Vasoactive drugs
• Fenoldopam is a specific dopamine-1 receptor agonist that augments renal plasma flow while decreasing systemic vascular resistance.
• A prospective randomized trial (CONTRAST) assessed the effectiveness of fenoldopam in 315 patients undergoing a cardiovascular procedure who had CKD with an estimated creatinine clearance <60 mL/min.
• Unfortunately it also fails to reduce CIN incidence in CKD patients.

Vasoactive drugs
• In a retrospective series of 285 patients,Weisz et al. reported a 71% decreased in CINincidence with local fenoldopam therapy(0.05–0.8 μg/kg/min).
Weisz G, Filby SJ, Cohen MG, Allie DE, Weinstock BS, Kyriazis D, et al. Safety and performance of targeted renal therapy: the Be-
RITe! Registry. J Endovasc Ther. 2009;16(1):1–12.

Vasoactive drugs
• The clinical benefit of the competitive adenosine antagonisttheophylline is debated.
• In a randomized study by Huber et al, prophylactic intravenousadministration of theophylline 200 mg reduced the incidence of CIN in100 patients at risk, as compared with placebo (4% versus 16%).
• However, in other randomized studies, administration of theophyllinedid not provide any benefit in reduction of CIN rates compared withplacebo.
• Huber W, Ilgmann K, Page M, et al. Effect of theophylline on contrast material-nephropathy in patients withchronic renal insufficiency: controlled, randomized, double-blinded study. Radiology. 2002; 223(3):772–779.
• Shammas NW, Kapalis MJ, Harris M, McKinney D, Coyne EP. Aminophylline does not protect against radiocontrastnephropathy in patients undergoing percutaneous angiographic procedures. J Invasive Cardiol. 2001;13(11):738–740.

Vasoactive drugs
• A 20 ng/kg/min PGE1 infusion has a significant protective effect on post-PCI SCr elevation,
• But higher infusion rates are not associated with increased benefits, probably due to the associated decrease in systemic blood pressure.
Koch JA, Plum J, Grabensee B, Modder U. Prostaglandin E1: a new agent for the prevention of renal dysfunction in high risk patients caused by radiocontrast media? PGE1 Study Group. Nephrol Dial
Transplant. 2000;15(1):43–9.

Vasoactive drugs
• In a small, randomized, placebo controlled study of 35 patients, eGFRwas preserved in patients treated with nitrendipine but decreased in patients that received placebo.
Neumayer HH, Junge W, Kufner A, Wenning A. Prevention of radiocontrast-media-induced nephrotoxicity by the calcium channel blocker nitrendipine: a prospective randomised clinical trial.
Nephrol Dial Transplant. 1989;4(12):1030–1036.
• By contrast, in three other studies, the change in serum creatinine level did not differ significantly with calcium antagonists.
Carraro M, Mancini W, Artero M, et al. Dose effect of nitrendipine on urinary enzymes and microproteins following non-ionic radiocontrast administration. Nephrol Dial Transplant.
1996;11(3):444–448.

Hemodialysis• Iodinated contrast agents are readily dialyzable.
• The plasma clearance of most modern contrast media is 50–70 mL/min, with more than 80% removed from the plasma within 4–5 hours ofhemodialysis.
• However, Reduction of CIN with dialysis is also not biologically plausiblesince the CM would reach the kidneys within one or two cardiac cycle.
• Subsequent removal of CM is unlikely to stop the cascade of renalinjury, which would have already begun.
Dawson P. Contrast agents in patients on dialysis. Semin Dial. 2002;15(4):232–236.

Hemofiltration
• In patients with chronic renal failure who are undergoingpercutaneous coronary interventions,
• periprocedural hemofiltration given in an ICU setting appears tobe effective in preventing the deterioration of renal function dueto CIN
• and is associated with improved in-hospital and long-termoutcomes.
Marenzi G, Marana I, Lauri G, et al. The prevention of radiocontrast-agent-induced nephropathy by hemofiltration. N Engl J Med 2003; 349:1333.

• A 2012 meta-analysis that included eight studies of hemodialysisand three studies of hemofiltration/hemodiafiltration showed no benefit of RRT.
• Routine hemofiltration or hemodialysis for the prevention of contrast nephropathy in patients with CKD is not recommended.
Cruz DN, Goh CY, Marenzi G, et al. Renal replacement therapies for prevention of radiocontrast-induced nephropathy: a systematic review. Am J Med 2012; 125:66.