Embed Size (px)
Citation preview

COMMON CASES
Dr. Riyad Banayot

Lids, Conjunctiva and Sclera

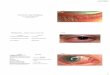
Ocular cicatricial pemphigoid
Loss of caruncle, shallowing of the lower, tear film is poor, cornea may be opacified with neovascularization
Shallowing of the lower fornix and symblepharon, entropion, ectropion and trichiasis
Look for ulcers on the tongue or buccal mucosa, skin lesions

What conditions may simulate ocular cicatricial pemphigoid ?
Chemical burnt Steven-Johnson's syndrome Conjunctival malignancies

How would you treat this condition?
Ocular lubricant with artificial tears and ointments
Topical steroid for acute inflammation Severe cases may need systemic steroid
and immunosuppressants such as dapsone or cyclophosphamide
Oculoplastic surgery for trichiasis and entropion to reduce further damage to the cornea.

What do you see?
• There is exposure of the underlying dark uveal tissue (usually covered by the upper lid) with thinning of the surrounding sclera & conjunctiva. There are large abnormal blood vessels crossing areas of scleral loss.
• Seen mainly in women with rheumatoid arthritis.
• Look for: signs of rheumatoid arthritis (symmetrical deformities of the hand joints)
• Occasionally this condition is seen in Wegener's granulomatosis and relapsing polychondritis.

What are the types of scleritis ? Anterior scleritis:
Diffuse scleritis (most benign). 30% has underlying connective tissue disease
Nodular scleritis deep red to purple color, immobile nodule
Necrotizing scleritis (most destructive). 60% of affected patients develop ocular and systemic complications. 40% suffer from loss of vision and 29% die within 5 years of onset due to complications from vasculitis. There are two types: With inflammation & Without
inflammation Posterior scleritis:
least common, present with pain, proptosis, visual loss and restricted motility.
Can find: choroidal folds, exudative RD, papilloedema and ACG from choroidal effusion

Limbal dermoid
There is a round, raised, whitish lesion in the limbus.
Pre-auricular skin tag
Further examination: • Significant astigmatism is present due to distortion of the cornea• The condition is associated with Goldenhar's syndrome. • look for: Preauricular skin tag, Duane's syndrome and facial asymmetry (with
mandibular under-development which may be ipsilateral or contralateral, small mouth

Name other mandibulofacial dystoses ?
Treacher-Collins' syndrome: This is an autosomal dominant condition Malar hypoplasia Absent zygomatic arch Anti-mongoloid slant of the palpebral fissure Coloboma of the outer third of the lower lids. In the lower face, there is hypoplasia of the
lower jaw with macrostomia and abnormal dentition.
The ears are usually malformed.

Basal cell carcinoma
There is a lesion in the lower lid, nodular with an ulcerated center. The surface is pearly and has telangiectasia.
Forms of lesion?

Basal cell carcinoma
- Check if the lesion is attached to the underlying structure by gently moving the lesion - Check if the punctum is involved (if present, there is a potential risk of orbital extension) - Look for loss of eyelashes (this indicates of malignancy if the nature of lesion is uncertain) - Assess the amount of skin laxity which would be important in reconstructive surgery
Further examination

What is the D.D. of BCC?
Squamous cell carcinoma Sebaceous cell carcinoma Amelanotic melanoma

What are the treatment options for BCC?
Cryotherapy Radiotherapy Excision. This is the treatment of choice.
Techniques: Frozen section techniques: After the tumor has been
excised. 1-2 mm wide strips of tissue is excised form the adjacent tissue for frozen section examination. Reconstruction is undertaken only when all margins are found to be tumor free.
Moh's micrographic surgery: Tissue is removed in lamellar layers which provide a three-dimensional mapping of the tumor excision. (it allows for retention of the maximum amount of tissue)

What do you see?
• Always examine the undersurface of the UL if you find UL entropion and/or diffuse corneal opacities. The inferior fornix is deep and there are no symblepharon (the presence of symblepharon should make one consider ocular cicatricial pemphigoid, Steven-Johnson's syndrome or chemical injury).
Other features that may suggest trachoma: • Micropannus in the superior cornea • Pits at the limbus (Herbert's pits which results from necrosis of the follicles)
On everting the eyelids, there is subtarsal fibrosis
Diffuse corneal opacities (+/- vascularization)

Differences between trachoma & adult inclusion conjunctivitis ?
Trachoma
Caused by Chlamydia trachomatis
Transmitted by flies Caused by serotypes
A, B, Ba or C. Commonly seen in
tropical countries where sanitation is poor
Causes blindness through corneal scarring from keratitis and entropion
Adult inclusion conjunctivitis Caused by Chlamydia
trachomatis Transmitted sexually Caused by serotypes
D, E, F, G, H, I, J or K Common in developed
countries