Embed Size (px)
Citation preview

LOWER GI HEMORRHAGE
COLORECTAL
CARCINOMA
Dr.B.SELVARAJ MS;Mch;FICS:
PROFESSOR OF SURGERY
MELAKA MANIPAL MEDICAL COLLEGE
MELAKA 75150 MALAYSIA

COLORECTAL CARCINOMA
Causes of Lower GI Hemorrhage
Epidemiology
Etiology
Pathogenesis
Clinical Features
Investigations
Staging & Prognosis
Treatment
Followup
Mindmap
Diagnostic Algorithm
Management Algorithm

Causes for Lower GI Hemorrhage
Diverticular disease
Angiodysplasia- AV Malformation
Colorectal carcinoma
Hemorrhoids
Fissure-in-ano
Ischemic colitis
Inflammatory bowel disease
Meckel’s diverticulum
Upper GI hemorrhage

CLASSICAL CLINICAL VIGNETTE
A 57-year-old obese man is seen by his primary care physician for his yearly physical. He endorses a 20 Kgs weight loss in the past few months without changing his diet or exercise. He also reports pencil-thin stools and intermittent constipation
He feels that he cannot adequately evacuate his stool- tenesmus. He has smoked one pack per day for the past 20 years. He has a history of type 2 diabetes. He has never had a colonoscopy.
There was two episodes of bleeding per rectum
Family history is negative for any cancer.

CLASSICAL CLINICAL VIGNETTE
On exam, he is afebrile with a heart rate of 78/min and blood pressure of 132/74 mmHg. His abdomen is soft and non-tender. No abdominal masses are palpated and he is non-distended.
On rectal exam, he has no masses and no gross blood. Laboratory examination reveals a hematocrit of 37 % (normal 40–52 %).
Diagnosis: Left sided Colonic Cancer
Colonoscopy: This diagnosis should be confirmed by Colonoscopy

CRC- EPIDEMIOLOGY
Colorectal cancer is the second most common malignancy in the United States ,with more the 155,000 new cases diagnosed annually.
Incidence is highest in industrialized countries and is age specific, increasing steadily from the second to the ninth decades
Women: Third most lethal cancer after lung and breast
Men: Third most lethal cancer after lung and prostate
Site: More common in Recto sigmoid area. Incidence of cancers in the right colon as compared to the left has increased; therefore, screening should be of the entire colon and not just the recto sigmoid.

CRC- EPIDEMIOLOGY

CRC- ETIOLOGY
Genetics: Increased incidence in first-degree relatives of CRC patients, especially with age less than 50 years at diagnosis
A. Familial Adenomatous Polyposis (FAP): < 1% of CRC
- The gene responsible has been identified on the short arm of chromosome 5
- The condition is diagnosed when a patient has more than100 adenomatous polyps in the colon. It is autosomal dominant in character.
- Polyps are usually visible on endoscopy by the age of 15 years. Carcinomatous change occurs 10 to15 years after the onset of polyposis.
CRC- ETIOLOGY
B.HNPCC (Hereditary Non Polyposis Colonic Cancer):5 to10% of CRC
- Lynch syndrome: The genetic abnormality is usually on chromosome 17 or 18 and autosomal dominant in nature.
- Amsterdam criteria: a. Three or more relatives with CRC, spanning two generations, one of whom is a first-degree relative.
b. One or more CRC cases diagnosed before age 50 years
Premalignant Conditions: IBD- Crohn’s and Ulcerative Colitis
C.Environmental Factors: Diet Unsaturated fats induce progression from adenomas to carcinoma.
- Exposure to food additives, alcohol, lionizing radiation, bile acids promotes development of carcinoma.
CRC- PATHOGENESIS
Development of carcinoma is a multistep process
The mucosal epithelium progresses through a series of molecular and cellular events
Further genetic alteration results in higher degrees of cellular atypiaand glandular disorganization
The adenoma-to-carcinoma sequence is always associated with genetic changes, even in sporadic colon cancers

CRC- PATHOGENESIS
CRC- PATHOLOGY
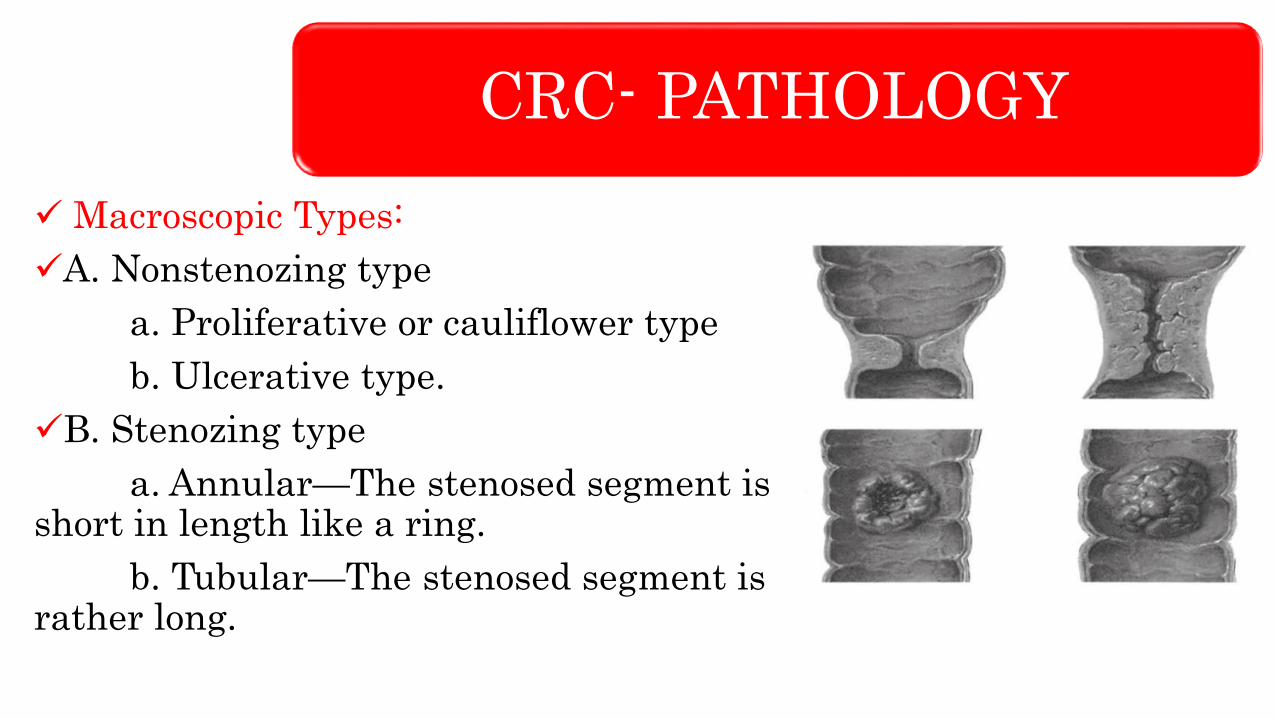
Macroscopic Types:
A. Nonstenozing type
a. Proliferative or cauliflower type
b. Ulcerative type.
B. Stenozing type
a. Annular—The stenosed segment is short in length like a ring.
b. Tubular—The stenosed segment is rather long.

CRC- PATHOLOGY
Spread:
Local spread: By continuity along the bowel wall.
By contiguity to adjacent structures
Lymphatic spread: Lymph nodes draining the colon are arranged in three groups viz. paracolic nodes lying in the immediate vicinity of the bowel wall. Intermediate nodes along the ileo colic, right colic, middle colic and sigmoid arteries and the apical nodes around the origins of superior and inferior mesenteric arteries.
Bloodstream spread: Metastasis may occur, quite early in the liver via the portal system. Lower rectal ca spread to lungs.
Clinical Features
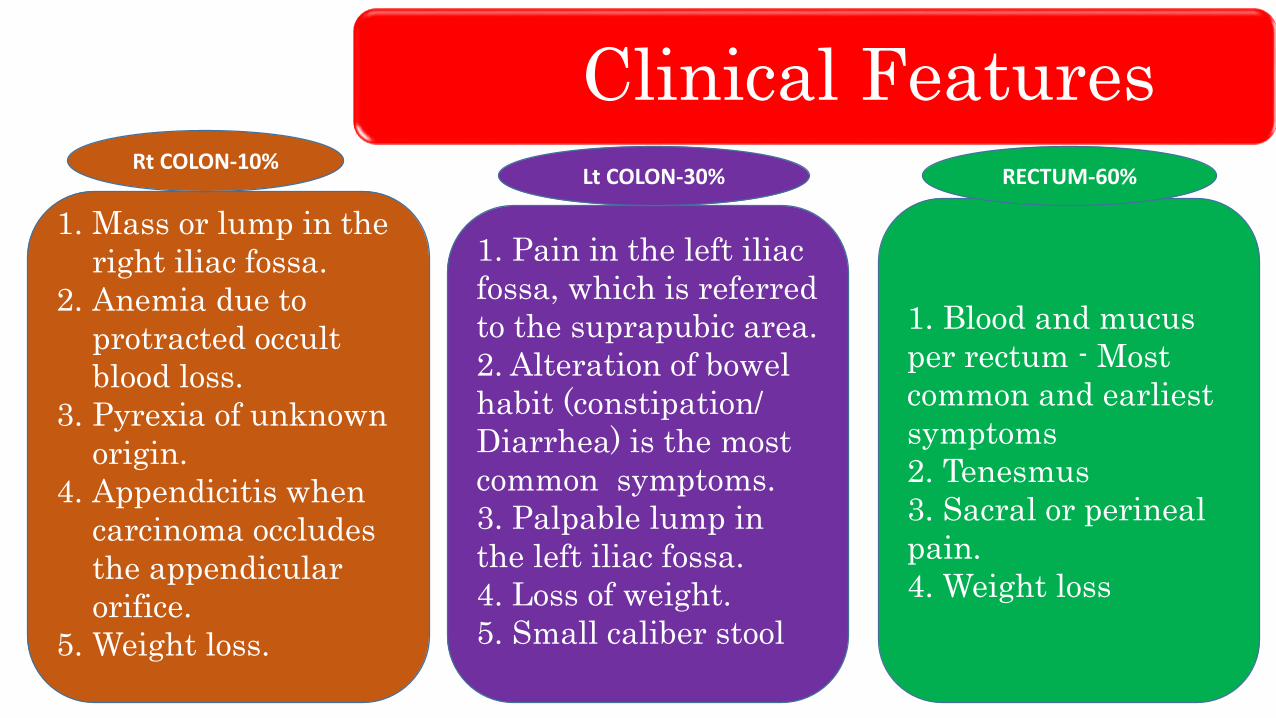
1. Mass or lump in the
right iliac fossa.
2. Anemia due to
protracted occult
blood loss.
3. Pyrexia of unknown
origin.
4. Appendicitis when
carcinoma occludes
the appendicular
orifice.
5. Weight loss.
1. Pain in the left iliac
fossa, which is referred
to the suprapubic area.
2. Alteration of bowel
habit (constipation/
Diarrhea) is the most
common symptoms.
3. Palpable lump in
the left iliac fossa.
4. Loss of weight.
5. Small caliber stool
1. Blood and mucus
per rectum - Most
common and earliest
symptoms
2. Tenesmus
3. Sacral or perineal
pain.
4. Weight loss
Rt COLON-10%Lt COLON-30% RECTUM-60%

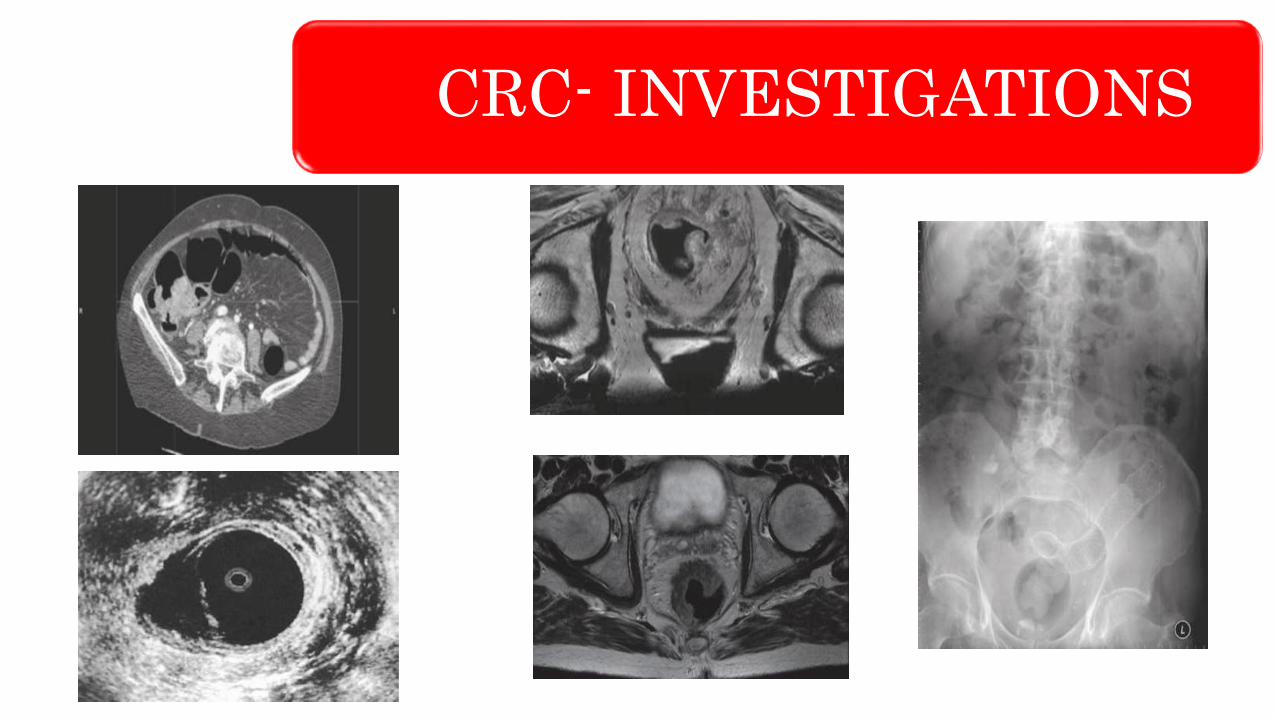
CRC- INVESTIGATIONS
Laboratory studies: include hemoglobin/hematocrit, fecal occult blood, liver enzymes and Carcino Embryonic Antigen- CEA
Sigmoidoscopy: both rigid and flexible
Colonoscopy: necessary to confirm the diagnosis and exclude any synchronous lesions proximally
DCBE( Double Contrast Barium Enema): Apple core appearance-demonstrates the site and configuration of the lesion
Endorectal ultrasound: information of the depth of invasion into the bowel wall by a rectal tumor and involvement of lymph nodes
CT scan is used to evaluate the chest and abdomen for metastases

CRC- INVESTIGATIONS
Apple CoreAppearance
MULTIPLE LIVERSECONDARIES
CRC- INVESTIGATIONS

CRC- STAGING

CRC- STAGING & PROGNOSIS
CRC-TREATMENTCarcinoma right colon Radical Rt Hemicolectomy
Ca Hepatic fexure & Rt Transverse colon Radical Extended Rt
Hemicolectomy
Ca Transverse colon Radical Transverse Colectomy
Ca left colon Radical Lt Hemicolectomy
Ca sigmoid colon Radical Sigmoidectomy
Ca in upper1/3rd of Rectum High anterior resection- >15cms from
anal verge
Ca in lower 1/3rd of Rectum Low anterior resection if > 8cms from
anal verge or Abdomino Perineal Resection with Total Mesorectal
Excision if < 6cms from anal verge
Hartman’s procedure In emergency situation in an unprepared
large bowel

TREATMENT
COLON RESECTIONS LOW ANTERIOR RESECTION PERINEAL PART OF APR
CRC- FOLLOWUP
Most tumors recur in the first 2 years after curative resection.
Colonoscopy and Ba enema are done in the postoperative period to
establish a base line.
Colonoscopy is repeated annually for at least 4 years, then every 2 to
3 years.
CEA level is done every 2 months for 2 years, every 4 months for 2
years, then annually. CEA level is sign of recurrence.
CXR every 6 months for 3 years, then annually.
Complete blood count and liver function tests should be performed
every 3 months for 2 years, then every 6 months for 2 years, and then
annually.
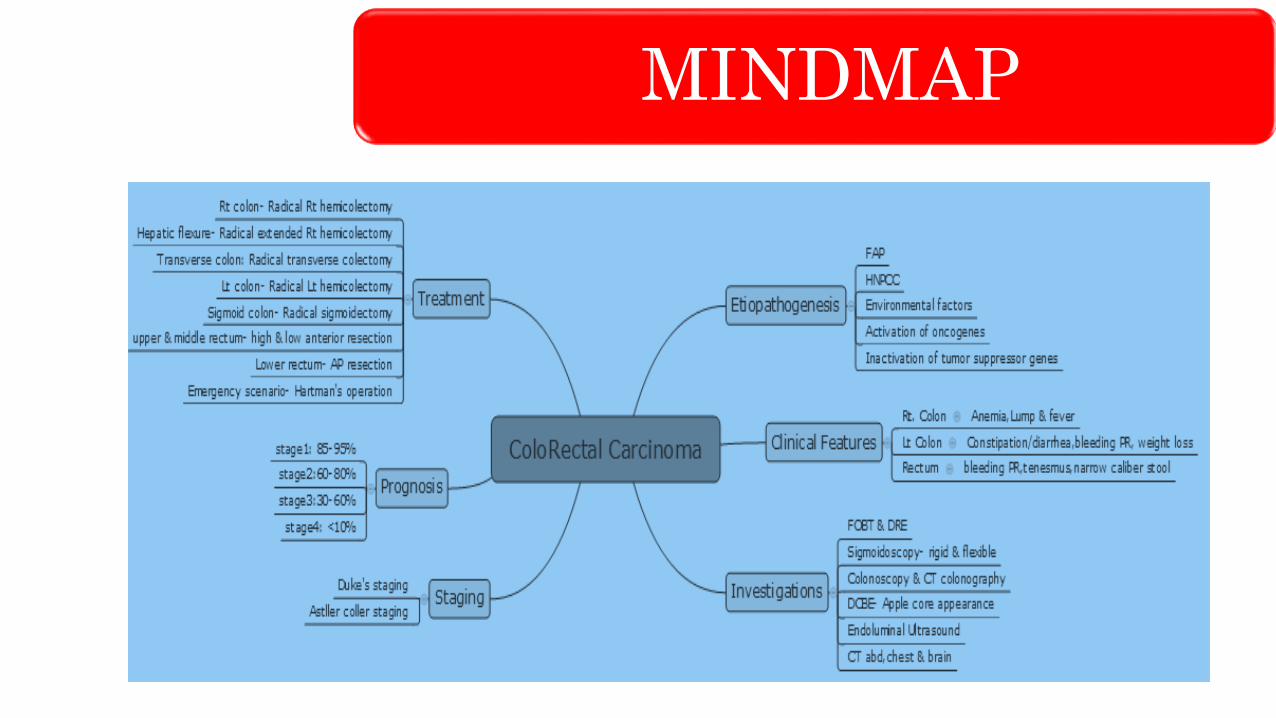
MINDMAP
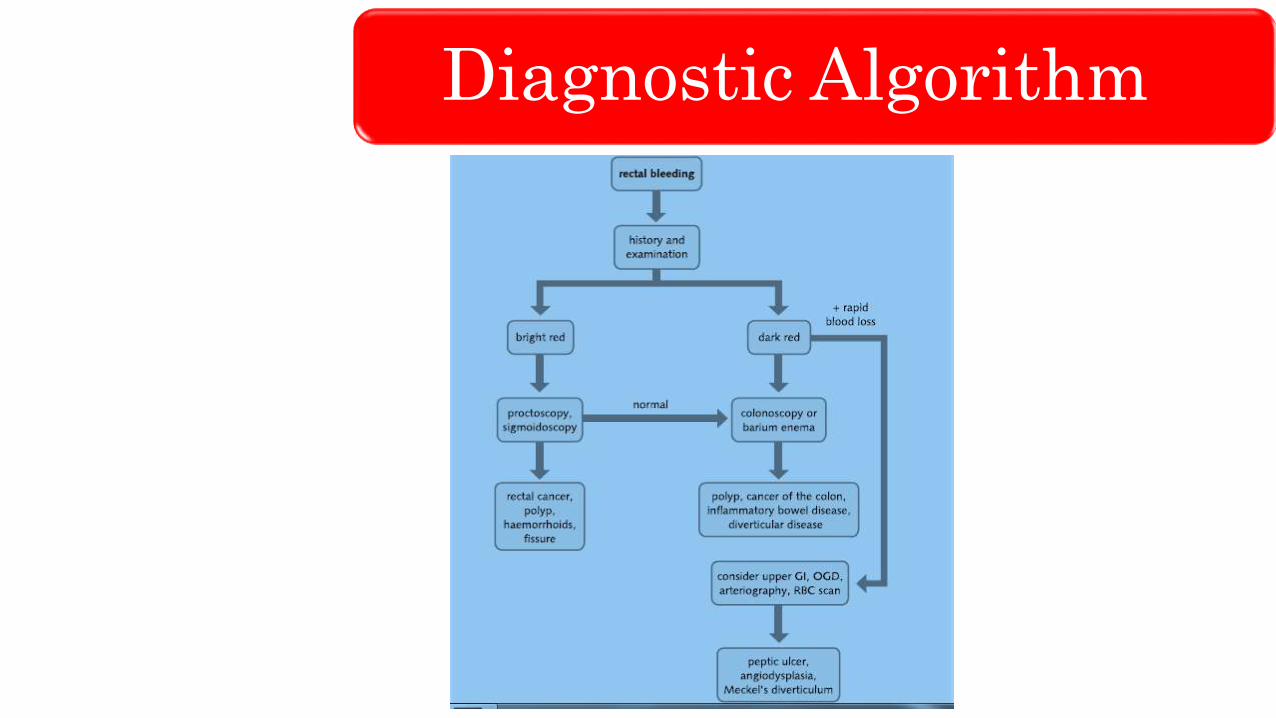
Diagnostic Algorithm
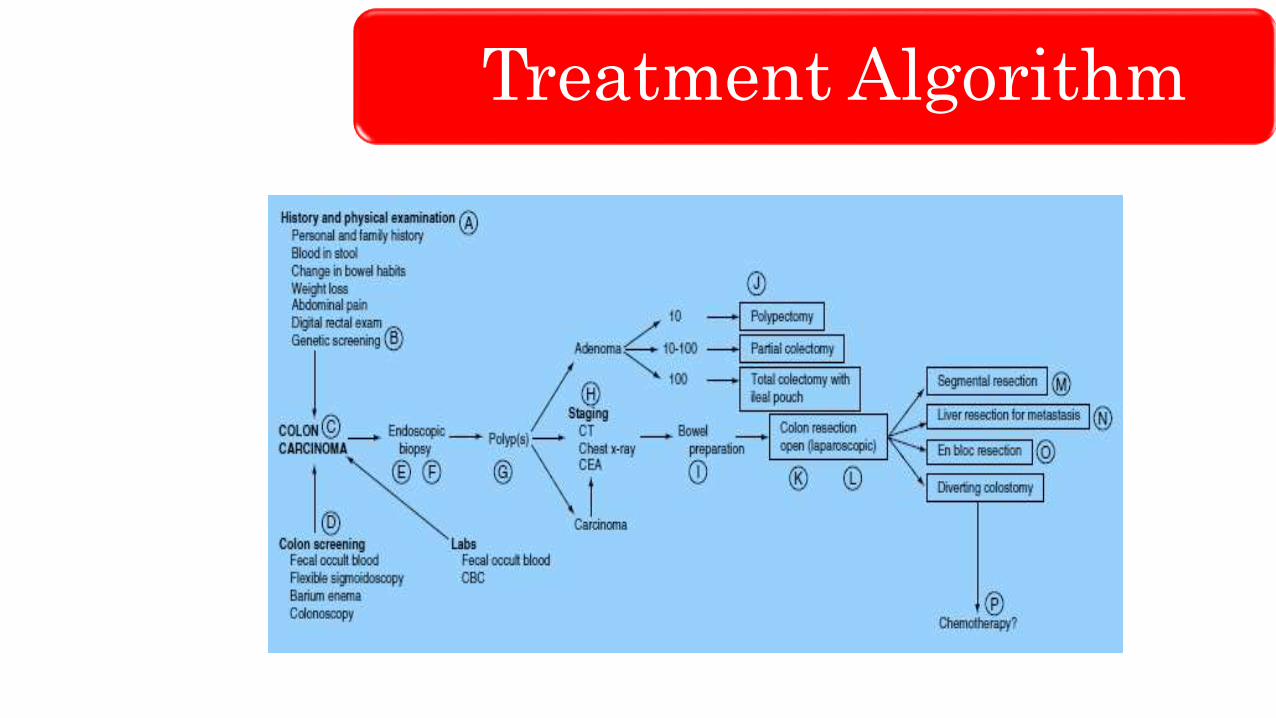
Treatment Algorithm

Treatment Algorithm

THANK YOU
LIKE
SHARE
SUBSCRIBE





























