Embed Size (px)
Citation preview
Changes in newborn pregnancy and old age

The Newborn
•Neonatal or newborn period:
-The first four weeks of extra uterine life.
-Skin similar in structure to adult skin.

Skin Characterized
Histological Peculiardifferences cutaneous reactions

Skin functions in the newborn
1-Barrier function :
• Full term baby: fully developed
• Pre-term infants: (infants born before the 37wks), -epidermis is thinner. -The stratum corneum thin. -Intracytoplasmic keratin fiber bundles fewer and smaller, larger amounts of glycogen in the cytoplasm of the cells of the stratum spinosum.
Impairment of its barrier functions
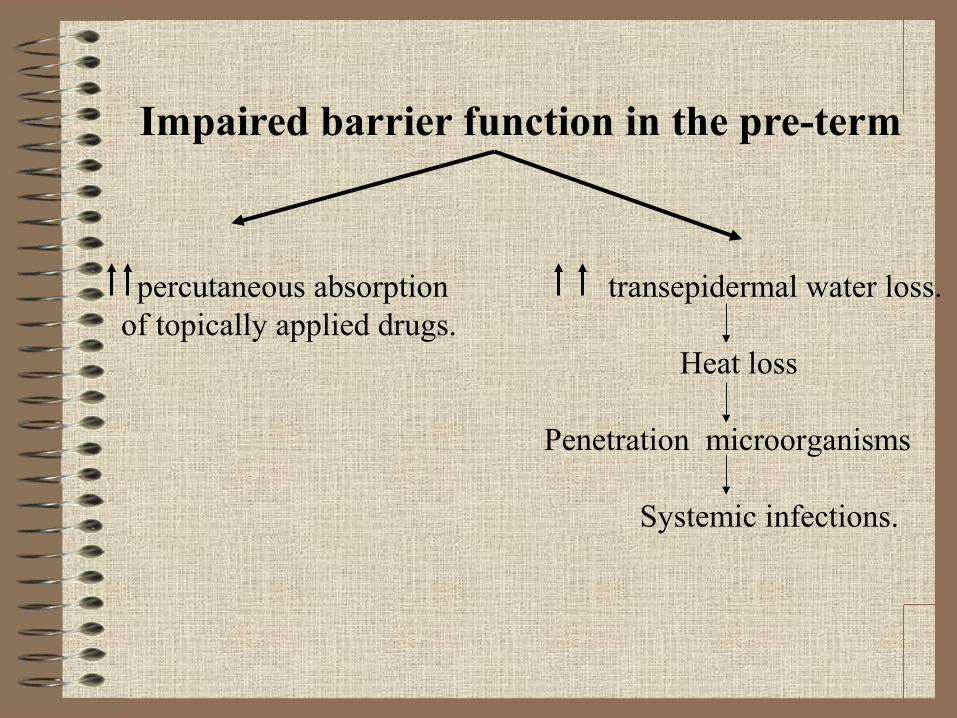
Impaired barrier function in the pre-term
percutaneous absorption transepidermal water loss.of topically applied drugs. Heat loss
Penetration microorganisms Systemic infections.

2 -Eccrine sweating:
• 28th week of gestation: anatomically normal.
• Full-term: sweat in response to thermal stress.
• Inefficient as a thermoregulatory mechanism.
• The forehead site of thermally induced sweating.
3-Sebaceous gland secretion• Hyperplasia maternal androgens.
-C\P: Multiple, uniform, pinpoint, yellowish papules.
- Site: nose, cheeks, upper lip, forehead, areola and genitalia.
Peculiar skin reactions
“Physiological”
Epidermis Dermis

Peculiar reactions of the newborn epidermis
A. Vernix Caseosa:
-Thin, whitish, greasy film.
- Covers the entire skin.
- Protect from infection.
-Composed of sebum and epidermal lipids.
-The sebum: antibacterial and antiviral properties.
- Flake within few hours after birth.
B. Scalp hair: -5th month of fetal life: shedding.-Re-grows shed a few weeks before birth.
-After birth:
occipital area telogen phase occipital alopecia.
- End of the 6th month: anagen hair.

C. Body hair
•Pre-term infants lanugo hair. •Dense: face, limbs, and trunk.
• 1 month before term: shedding shorter lanugo hair (full-term infants).
• First month of life:shedding and is replaced by villous hair.

D. Superficial cutaneous desquamation
-Physiological scaling.
-Occurs in 75% of normal neonates.
-It usually appears around the ankle
-First day of life.
- Localized or become more widespread.

Peculiar reactions of the newborn
dermis:
Dermal Vasculature
A. Peripheral cyanosis
-Site: palms, soles, and around the mouth.
- Normal phenomenon during the first 48 hours, if it is not associated with central cyanosis (cyanosis of the tongue).
B. Erythema neonatorum
-Generalized hyperaemia.
-Involves many babies few hours after birth.-Fades spontaneously within 24 to 48 hours.
C. Marbling (cutis marmorata)
- Reticulate blue vascular pattern.
-Occurs on cooling and disappears on re-warming.
- May be seen throughout infancy.
D. Harlequin color changes -Vivid color difference.
-Along the midline during the first week of life. - Immaturity of hypothalamic center responsible for the control of the peripheral vascular tone. - Lying on his side upper half pale, lower half deep red with a sharp midline demarcation. -On the other side, the color changes reverse.
-Duration : half to 20 minutes. - Subsides spontaneously within 4 weeks.

SummarySkin functions in the newborn:1-Barrier function
2-Eccrine sweating 3-Sebaceous gland secretion
Physiological peculiar reactions: -EpidermisA. Vernix Caseosa B. Scalp hair
C. body hair D. Superficial cutaneous desquamation -Dermis
A- Peripheral cyanosis. B-Erythema neonatorum C-Marbling (cutis marmorata)
D-Harlequin color changes

Physiological changes of pregnancy

Causes:
-The de novo production of a variety of protein and steroid hormones by the fetoplacental unit.
-Increased activity of the maternal pituitary, thyroid, and adrenal glands.

1 Pigmentation-Generalized .
-More marked in dark-skinned women.
-Areas: nipple, areola, genital areas and mid line of the abdominal wall.
-Usually fades after delivery.
- Increase in size, activity and number of melanocytic naevi.
-Chloasma:
-Second half of pregnancy.-Iirregular, sharply marginated areas of pigmentation -symmetrical pattern.- Site: forehead, temple, or on the centre of the face, or both.
-Usually fades completely after delivery, may persist.

Physiology of hyperpigmentation
Increased production of estrogens.
Increased levels of progesterone.
Increased melanocyte-stimulating hormone.

2-Hair changes
-Pregnancy: Scalp hair growth is usually increased.
- proportion of hair in the anagen phase.
-After delivery: compensatory shedding of hair resulting in noticeable alopecia (physiological telogen effluvium).

3. Nail changes: - Brittleness.
-Distal onycholysis.
4. Eccrine, apocrine and sebaceous gland activity: -Eccrine gland activity: increased
increased frequency of miliara.
-Apocrine gland activity: often reduced during pregnancy,
-Rate of sebum secretion increase ,
-due to the release of sebotrophic hormones from the pituitary gland.

5. Connective tissue changes.-Most common change
striae distensae -Site: abdomen, hips, buttocks and sometimes breast. - Cause: unknown,
combination of hormonal factors (adrenocortical hormone, estrogen and relaxin) associated with increased lateral stress on the connective tissue. -C\P:- pink to purple atrophic bands,
-mild pruritus.
-After delivery, they become pale and less.
- Skin tags (mollascum fibrosum graviderum)
6-Vascular changes
Hyperemia.
Vascular proliferation palmar erythema and/or spider angiomas
Cause: increase in vascularity + high estrogen levels. - Edema and venous varicosities: - common
- legs and feet.
Hemorrhoids: common.
Cause: vascular distention increased intraabdominal pressure. -Vascular tumors: Glomus tumor or Hemangiomas may appear or enlarge.Other vascular changes include:-Gingival edema and redness.- Pyogenic granuloma (Granuloma graviderum or pregnancy epulis), caused by the general increase in vascularity associated with high estrogen levels.

Physiology of aging

Aging is the decline of power of self-maintenance, the increase
susceptibility to disease and the growing probability of death as
age advances
Types
Intrinsic Extrinsic

1. Intrinsic -Genetically determined.
-Inevitable process attributed to the passage of time.
Cause:a- Telomer shortening: (terminal portion of chromosome)
-each round of cell division.
b- Cellular senescence: which is the limited capacity of cells to undergo cell division. It is regarded as a cancer-prevention mechanism .
2. Extrinsic Aging (photoaging)
The superimposition (on intrinsic aging) of changes attributable to external factors such as:
1- Chronic sun exposure
2-Premature aging syndromes
3-Alcohol consumption
4-Smoking
5-Exposure to pollution.
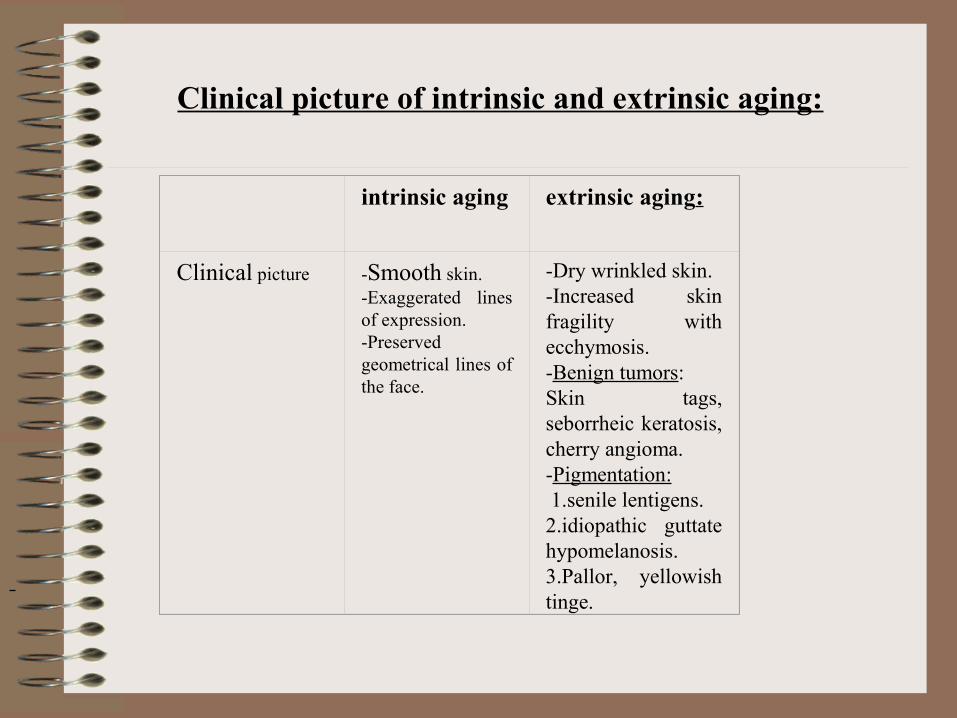
Clinical picture of intrinsic and extrinsic aging:
intrinsic aging extrinsic aging:
Clinical picture -Smooth skin.-Exaggerated lines of expression.-Preserved geometrical lines of the face.
-Dry wrinkled skin.-Increased skin fragility with ecchymosis.-Benign tumors:Skin tags, seborrheic keratosis, cherry angioma.-Pigmentation: 1.senile lentigens.2.idiopathic guttate hypomelanosis.3.Pallor, yellowish tinge.

Pathology of intrinsic and extrinsic aging:Pathology intrinsic aging extrinsic aging:
Epidermis -Flattened epidermis.-Lost rete ridges.-Decreased melanocyte number. -Decrease in langerhans cells.
-Flattened epidermis.-Lost rete ridges.-Decreased melanocyte number, but are irregularly distributed.-Decrease in langerhans cells.
Dermis -Atrophy.-Decrease in collagen fibers.- Decrease in elastic fibers.
-Atrophy.-Collagen is irregularly thickened.-Elastic fibers:Early: solar elastosis.Late: degeneration.-Blood vessels: decrease in number and size.

Effects of aging on skin adnexae
1. Hair follicles-Decrease in number of hair follicles,-Cause: - atrophy and fibrosis.
- increase in the proportion of telogen hair follicles.
Graying of hair:progressive and total loss of melanocytes from the hair bulb ( more rapidly in hair than in skin because the cells proliferate and manufacture melanin at maximal rate during anagen phase. Whereas, epidermal melanocytes are comparatively inactive throughout their life span).
2. Nails:-From the third decade nail growth starts to decrease:
-Brittleness.- Beaded ridging, “sausage links”.
-Brittleness: content of lipophilic sterols and free fatty acids.
3. Eccrine, apocrine and sebaceous glands:-Decrease in the number and function of sweat glands,
eccrine sweating decrease by 15%

-Apocrine glands: size and function decrease. -Lipofuscin “age pigment” gradually accumulates in the secretory cells of both eccrine and apocrine glands.
-Sebaceous glands: size and number not changed with age. - sebum production: 23% per decade. decrease in production of gonadal or adrenal androgens to which sebaceous glands are sensitive.
Grades of aging of the skinAt age 20-30 years: -No wrinkles. -No pigmentation. -No keratosis. At 40 years: -Wrinkles with emotions. -No pigmentation. -No keratosis. At 50 years: -Wrinkles at rest. -Pigmentation. -Keratosis. At 60 years: -advanced wrinkles. -Pigmentation and keratosis. -Benign tumors and precancerous lesions.
Pathogenesis of skin aging

1. Decreased barrier function of the skin:
-Thickness of the stratum corneum constant.- Corneocytes larger.
-Slow replacement of neutral lipids in the newly formed lamellar bodies, delays the recovery of barrier function in damaged stratum corneum.
- Remarkable age-associated decrease in the content of epidermal Filaggrin, which is required for binding of keratin filaments into macrofibrils.
2. Ultraviolet rays (UVR)UVA versus UVB
-Extremely hazardous effect on the skin.
-(UVB) photons are more energetic than UVA photons
-Mainly responsible for sunburn, and photocarcinogenesis.
- UVA larger role in photoaging because of:
a- Its 10-fold greater abundance in terrestrial sunlight.
b-Greater year-round and day-long average irradiation.
c-And greater average depth penetration into the dermis.
Effects of UVR on collagen:
-Exposure to sunlight damage to dermal collagen and elastin
photoaging

Repeated UVR exposure leads to enzymatic breakdown of collagen.
UVB exposure
AP-1 and NF-KB
MMPs: matrix & IL-1 & TNF-α:
collagen damage. collagenase& matrix damage.
IL-1 & TNF-α:
Recruitment of neutrophils
Secretion of neutrophil collagenase.

3. Infrared rays
Infrared rays:- sun,
-smoking
-heat sources.
deposition of elastic tissue into the tissues leading to solar elastosis.
Elastosis is characterized clinically by fine nodularity and/or coarseness, inelasticity, telangiectasia, venous lakes, purpura, comedones or sebaceous hyperplasia.

4. Smoking Smoking
- Infrared rays solar elastosis
-Nicotine.
Nicotine:
-Diuretic stratum corneum content of water and dryness.
-Accelerates hydroxylation of estradiol decreased estrogens in the skin dryness and atrophy.
-Nicotine leads to decreased vitamin C content
- pallor,
- coldness of the skin
-delayed wound healing.
- vitamin A deficiency, with reduced capacity to quench free oxygen radicals, and increased DNA damage.

5. Hormones -Levels of sex hormones gradually decline:
-In males: decrease
androgens, dehydroepiandrosterone (DHEA) and melatonin, leading to:
-Decreased vitality of skin.
-Decreased anticancer, antioxidant, antiangiogenesis effects.
-Less protection of DNA from UVR.
-In females: decrease
estrogens, progesterone, androgens, DHEA and melatonin., leading to decreased synthesis of collagen and glycosaminoglycans.

To sum upPathogenesis of skin aging:1. Decreased barrier function of the skin
2. Ultraviolet rays (UVR)
3. Infrared rays4. Smoking
5. Hormones