Embed Size (px)
Citation preview

Asthma Updates
Gamal Rabie Agmy, MD, FCCP Professor of chest Diseases, Assiut university
Definition of Asthma
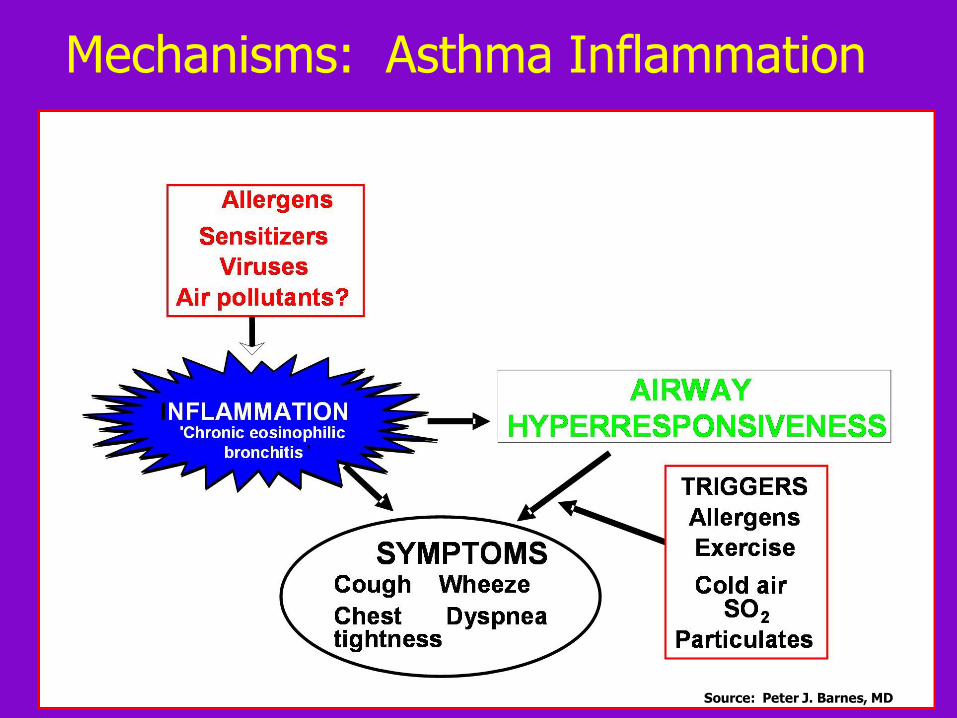
A chronic inflammatory disorder of the airways
Many cells and cellular elements play a role
Chronic inflammation is associated with airway hyperresponsiveness that leads to recurrent episodes of wheezing, breathlessness, chest tightness, and coughing
Widespread, variable, and often reversible airflow limitation
Source: Peter J. Barnes, MD
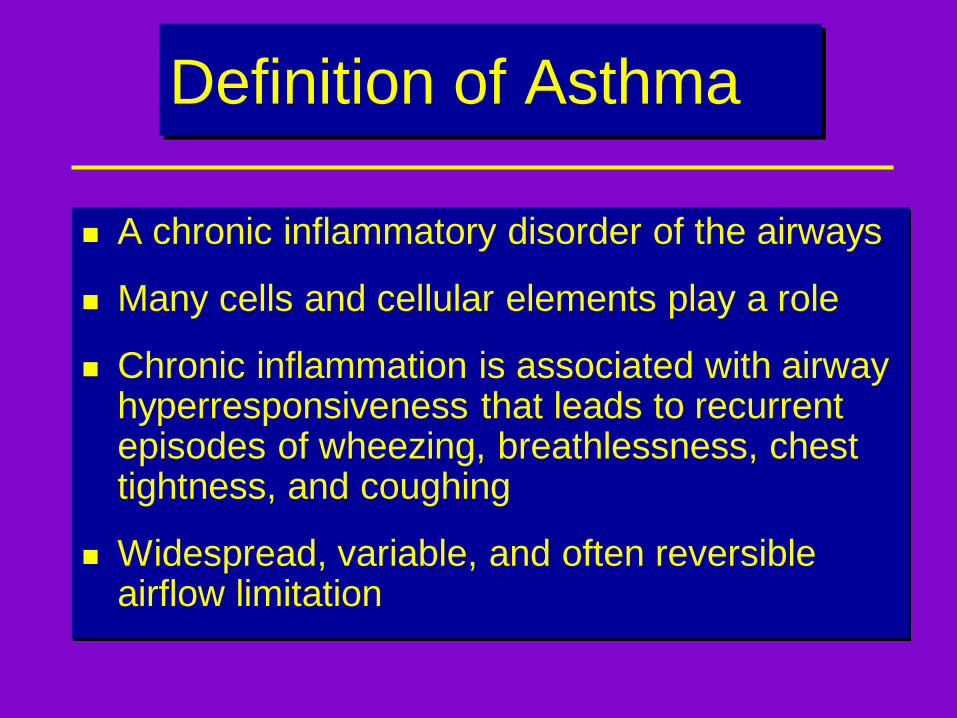
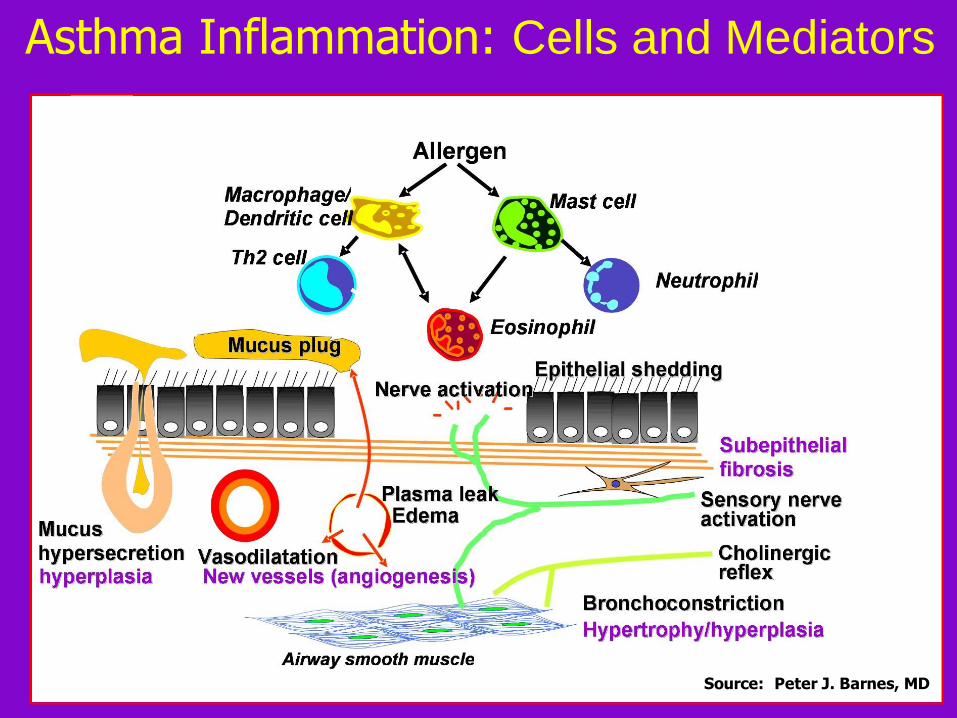
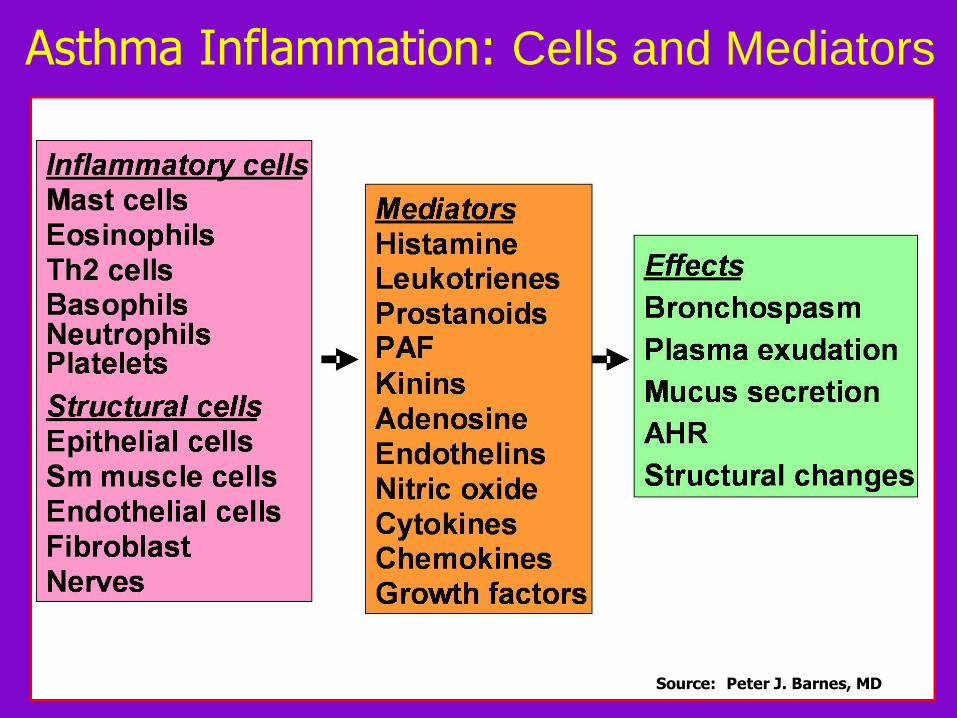
Asthma Inflammation: Cells and Mediators
Source: Peter J. Barnes, MD
Mechanisms: Asthma Inflammation
Source: Peter J. Barnes, MD
Asthma Inflammation: Cells and Mediators
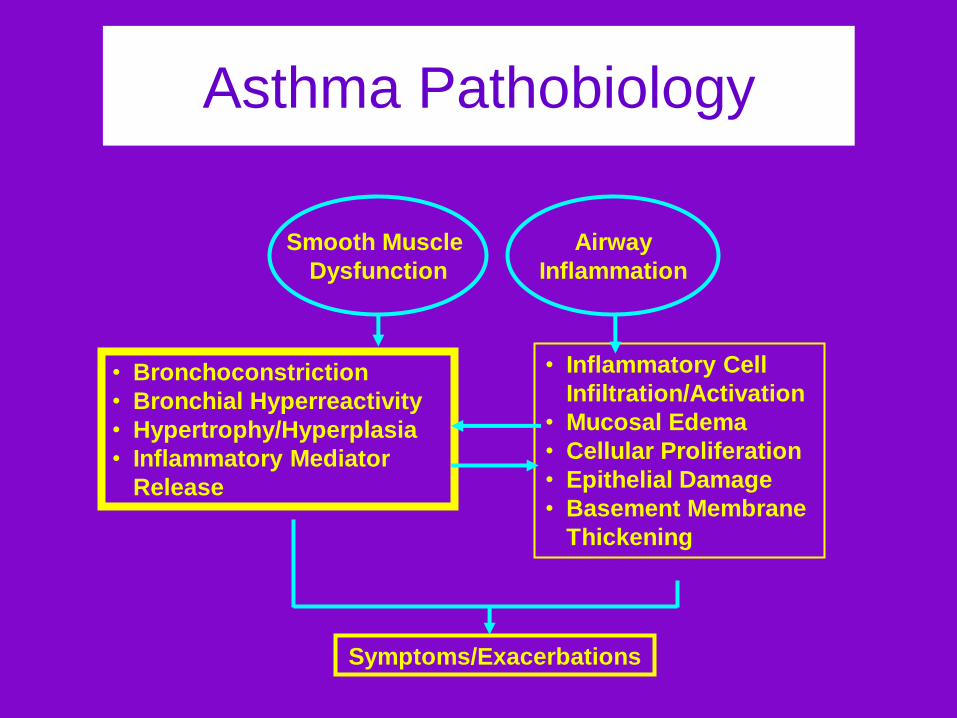
Smooth Muscle
Dysfunction
Airway
Inflammation
• Inflammatory Cell
Infiltration/Activation
• Mucosal Edema
• Cellular Proliferation
• Epithelial Damage
• Basement Membrane
Thickening
• Bronchoconstriction
• Bronchial Hyperreactivity
• Hypertrophy/Hyperplasia
• Inflammatory Mediator
Release
Symptoms/Exacerbations
Asthma Pathobiology
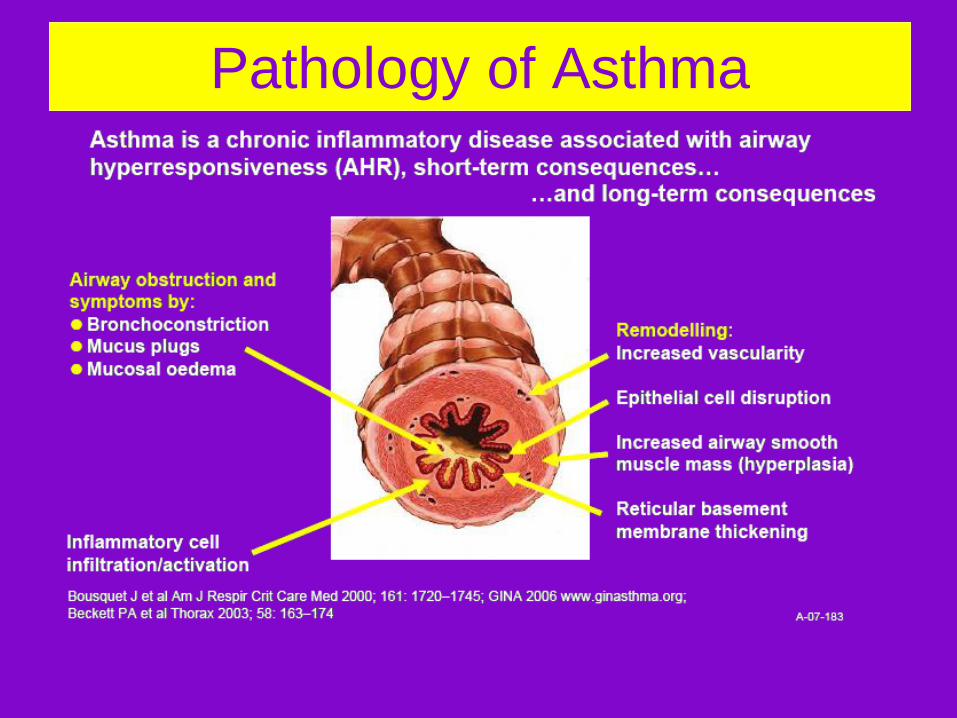
Pathology of Asthma
Factors that Exacerbate Asthma
Allergens
Respiratory infections
Exercise and hyperventilation
Weather changes
Sulfur dioxide
Food, additives, drugs
Factors that Influence Asthma
Development and Expression
Host Factors
Genetic
- Atopy
- Airway
hyperresponsiveness
Gender
Obesity
Environmental Factors
Indoor allergens
Outdoor allergens
Occupational sensitizers
Tobacco smoke
Air Pollution
Respiratory Infections
Diet
Is it Asthma?
Recurrent episodes of wheezing
Troublesome cough at night
Cough or wheeze after exercise
Cough, wheeze or chest tightness after exposure to airborne allergens or pollutants
Colds “go to the chest” or take more than 10 days to clear
90% of the asthma problem is not seen:
The inflammation!!!
Bronchospasm= 10%
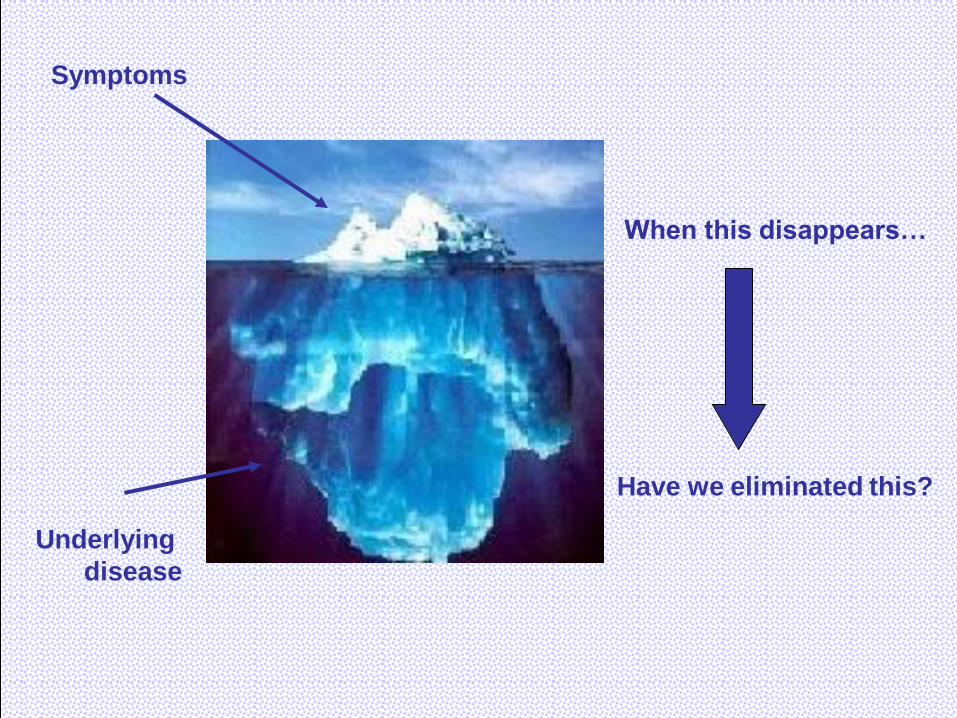
When this disappears…
Have we eliminated this?
Symptoms
Underlying
disease
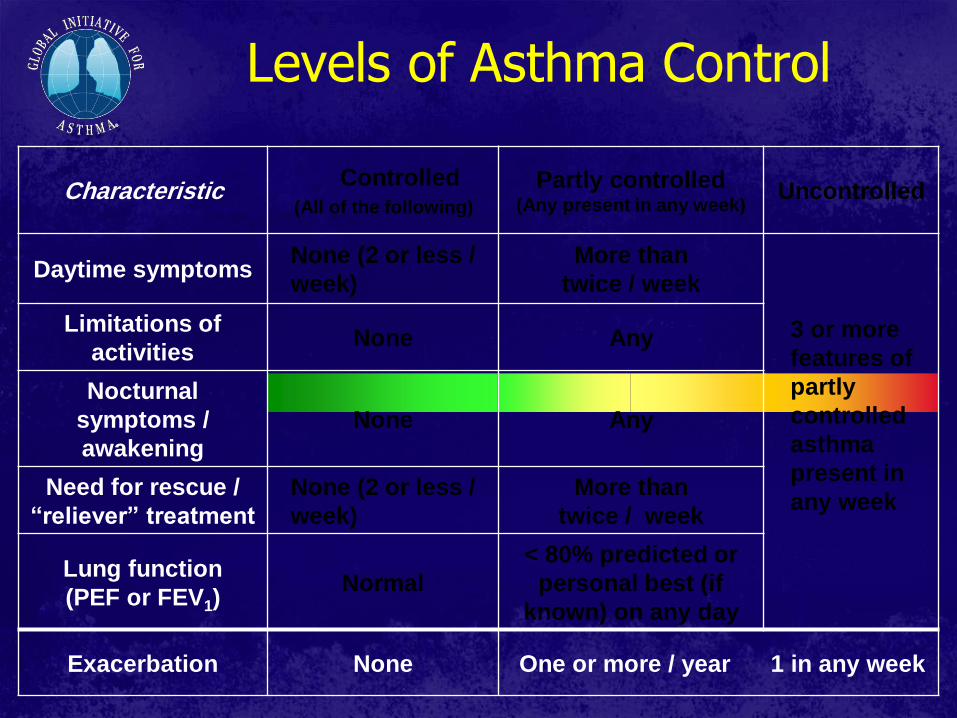
Levels of Asthma Control
Characteristic Controlled
(All of the following)
Partly controlled (Any present in any week)
Uncontrolled
Daytime symptoms None (2 or less /
week)
More than
twice / week
3 or more
features of
partly
controlled
asthma
present in
any week
Limitations of
activities None Any
Nocturnal
symptoms /
awakening
None Any
Need for rescue /
“reliever” treatment
None (2 or less /
week)
More than
twice / week
Lung function
(PEF or FEV1) Normal
< 80% predicted or
personal best (if
known) on any day
Exacerbation None One or more / year 1 in any week


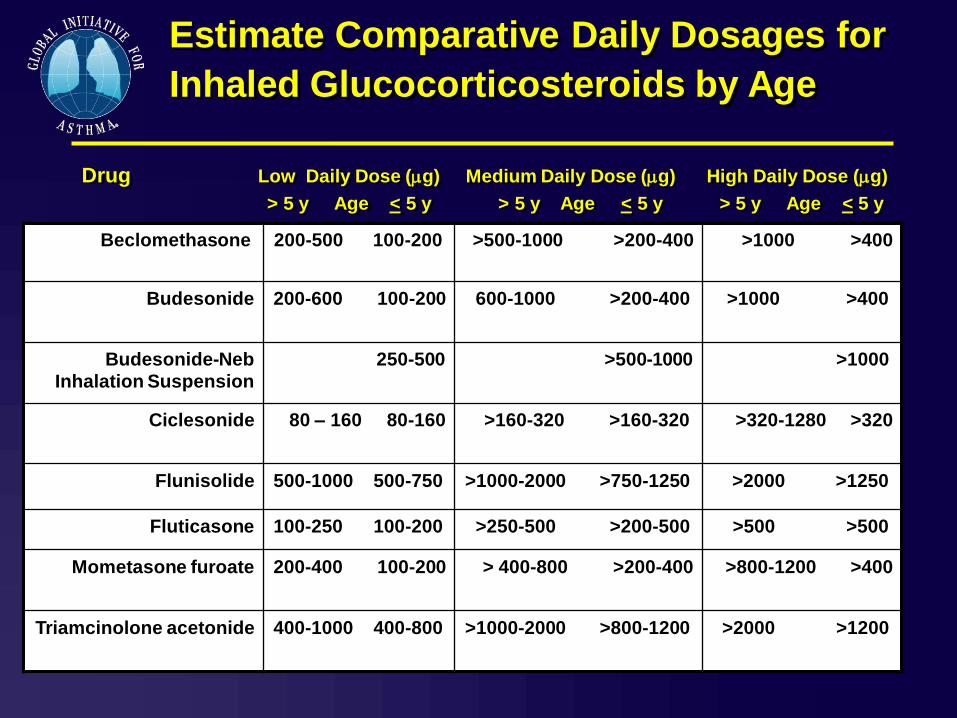
Estimate Comparative Daily Dosages for
Inhaled Glucocorticosteroids by Age
Drug Low Daily Dose (g) Medium Daily Dose (g) High Daily Dose (g)
> 5 y Age < 5 y > 5 y Age < 5 y > 5 y Age < 5 y
Beclomethasone 200-500 100-200 >500-1000 >200-400
>1000 >400
Budesonide
200-600 100-200
600-1000 >200-400 >1000 >400
Budesonide-Neb
Inhalation Suspension
250-500 >500-1000 >1000
Ciclesonide 80 – 160 80-160 >160-320 >160-320 >320-1280 >320
Flunisolide 500-1000 500-750 >1000-2000 >750-1250 >2000 >1250
Fluticasone 100-250 100-200 >250-500 >200-500 >500 >500
Mometasone furoate 200-400 100-200 > 400-800 >200-400 >800-1200 >400
Triamcinolone acetonide 400-1000 400-800 >1000-2000 >800-1200 >2000 >1200
Asthma is a complex disease or a syndrome that includes
several disease variants.
The term asthma, like „arthritis‟, equates to a definition of
grouped clinical and physiological characteristics. These
characteristics could identify syndromes, phenotypes or even
multiple diseases rather than a single disease.

For revealing the complexity and the heterogeneity of this
disease, asthma patients were grouped into subtypes called
phenotypes.
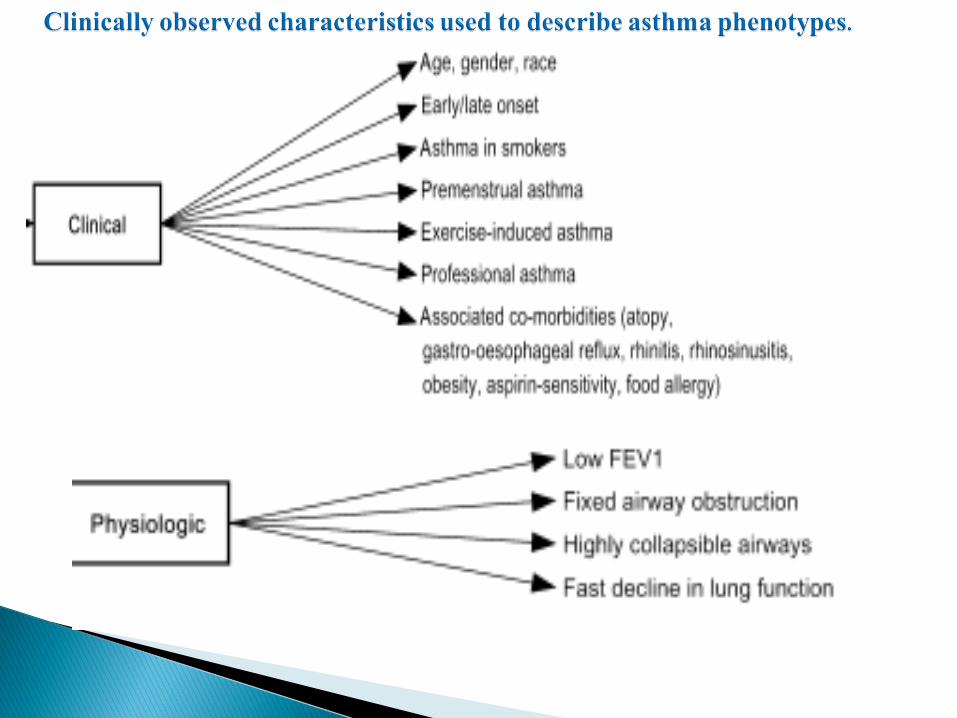
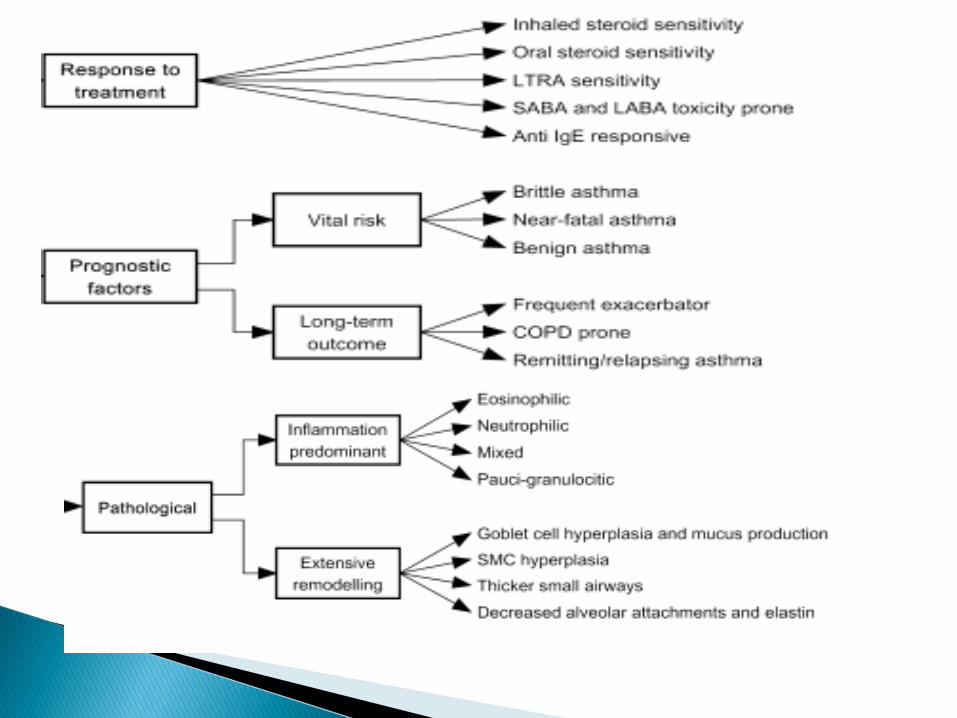
Term „phenotype‟ describes subtypes of asthma focused on
„clinically observable characteristics‟ of a disease.
Therefore, there are many „definitions‟ for asthma phenotypes, many of
which are related to differences in symptoms and severity rather than to
differences in underlying mechanisms. but this kind of subtyping does
little to help understand prognosis and target therapy.
When a link can be made between clinical characteristics and molecular
pathways, the term endotype can be introduced to describe distinct
subtypes with a defining etiology and consistent pathobiologic
mechanisms.
The definition of a true phenotype (or endotype) requires an
underlying pathobiology with identifiable biomarkers and
genetics .
Gene-expression profiling allows definition of expression
signatures to characterize patient subgroups, predict response
to treatment, and offer novel therapies.
By The study of wenzel ,et al 2013 Combining clinical, statistical
and molecular approaches two broad emerging “endotypes” have
been defined.
Traditionally asthma has been thought to be a Th2-associated
disease. There is strong evidence supporting a TH2-high phenotype
in up to 50% of people with asthma of any severity, yet 50% show
no evidence for this immune process.
These patients are characterized by atopy, eosinophilic
inflammation and favorable response to corticosteroids.
Early-onset allergic asthma
Late-onset persistent eosinophilic asthma
Exercise induced asthma
Clinical characteristics:
This group of asthmatic patients developed their disease in
childhood, and maintained their symptoms into adulthood. .
The majority of early-onset allergic asthma is mild but that an
increasing complexity of immune processes leads to greater
severity.
Most people with asthma are likely to have this phenotype.
Positive skin prick tests, specific IgE antibodies in serum,
eosinophilia in the peripheral blood .
Genetics:
Early-onset allergic patients commonly have a family history of
asthma, suggesting a genetic component.
Several Th2 cytokine SNPs
higher numbers of mutations in TH2-related genes (IL4, IL13,
IL4Rα ) associated with greater severity of disease.
Biomarkers:
Positive SPT, elevated IgE/elevated FeNO
Th2 cytokines IL-4 ,IL-5 , IL-9, IL-13, and periostin measured in
sputum, BAL, serum and bronchial biopsies.
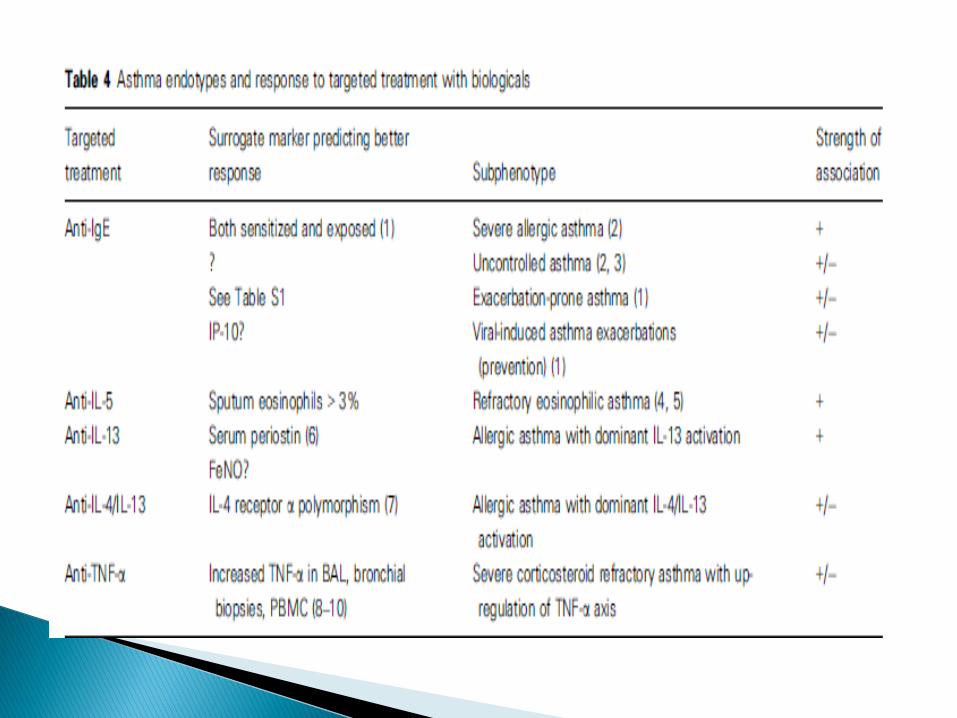
Treatment responses:
Corticosteroid-responsive.
Th2 Targeted therapy:
Anti IgE (omalizumab)in Severe allergic asthma.
Anti–IL-13( lebrikizumab) in Allergic asthma with dominant IL-13
activation Surrogate marker predicting better response is high
circulating levels of periostin. .
Inhaled IL-4Rα antagonist . Surrogate marker predicting
better response is IL-4 receptor a polymorphism.
Clinical characteristics:
The majority of this group develops disease in adult life,
often in the late 20s to 40s.
Severe from onset, Severe exacerbations with persistent
sputum eosinophilia (>2%), despite corticosteroid
therapy.
less clinical allergic responses( non atopic) than early-
onset asthma.
It is often associated with sinus disease.
Genetics:
Few patients in this group have a family history of asthma.
little is known regarding the genetics of adult onset persistent
asthma.
Biomarkers:
Lung eosinophilia. Persistent sputum eosinophilia (≥2%)
The lack of clinical allergy in this phenotype suggests that the TH2
process differs from and is probably more complex than the one
associated with the early-onset allergic phenotype but the presence
of IL-13 and IL-5 in the lower airways confirm Th2 pathway.
Some individuals show sputum neutrophilia intermixed with their
eosinophilic process. This mixed inflammatory process implies that
there are interactions of additional immune pathways with TH2
immunity, including activation of pathways related to IL-33 and IL-
17 .
Elevations in FeNO
Treatment responses:
persistent eosinophilia in late-onset disease inspite of ICS implies that the
TH2 process in this type of asthma is refractory to corticosteroids but high
systemic doses of corticosteroids are generally able to overcome this
refractoriness in late-onset asthma.
IL-5 targeted therapy may show much better efficacy in this endotype,
compared in early-onset allergic asthma patients, as IL-5 dependent
eosinophilia may be more important in this potential endotype.
(decreasing exacerbations and systemic corticosteroid requirements)
L-4 and IL-13 targeted therapy pathway.
AERD is probably a subendotype or a similar endotype. It is an
acquired condition on top of an intrinsic or less frequently
allergic asthma and thus, despite its peculiar sensitivity to
NSAIDs, still has major overlap with these conditions.
Clinical characteristics :
AERD is frequently progressive severe asthma starts late in
life and is associated with eosinophilia and sinus disease
Polyposis.
Response to aspirin challenge
Genetics :
LT-related gene polymorphisms.
Gene-expression study identified upregulation of periostin a
potent regulator of fibrosis and collagen deposition has also
been identified in polyps of and in airway epithelial cells of
patients with AIA.
Overexpression of periostin has been associated with
accelerated cell growth and angiogenesis(subtype).
Biomarkers:
high cysteinyl leukotriene level.
Treatment responses :
Many patients require systemic corticosteroids to control their
sinusitis and asthma.
Leukotriene modifiers especially 5-LO inhibitors can have a
robust impact on the AERD subset.
Downregulation of periostin after treatment of asthmatic
patients with corticosteroids suggests that normalization of
periostin expression is a part of the therapeutic effects of
corticosteroids. This opens a possibility of specifically
targeting periostin in future therapies for nasal polyps and
asthma
Clinical characteristics:
Exercise induced asthma refers to asthma whose symptoms are
experienced primarily after exercise. EIA is a milder form of
TH2 asthma.
Consistent with a relationship to TH2 processes, EIA common
in atopic athletes and high percentages of eosinophils and
mast cells and their mediators .
Biomarkers:
Th2 cytokines and cysteinyl leukotriene
Genetics:
No distinct genetic factors .
Treatment responses:
Leukotriene modifiers high LTE4/FENO ratio is Surrogate
marker predicting better response.
IL-9 targeted therapy has been shown effective on patients of
this group, which implies that Th2 immunity is involved in the
pathophysiology of EIA.
The lack of efficacy of Th2 targeted therapy suggests that a
subgroup of asthma develops in the absence of Th2 immunity .
Little is understood about the non Th2 asthma and its related
molecular elements.
Obesity-related asthma
Neutrophilic asthma
Smoking asthma
Whether obesity is a driving component in asthma development
or a mere confounder or comorbidity of its presence remains
controversial.
It is likely that obesity differentially impacts asthma that
develops early in life, as compared to later in life, being a more
prominent independent contributor in later onset disease.
So a distinct obesity-related asthma phenotype seems to occur
only in non-TH2 asthma.
, ..
Clinical characteristics :
Patients in this group are commonly women, obese, late onset
(mid-40s), less allergic (obesity is neither a risk factor for atopy
nor a risk factor for allergic asthma).with a high burden of
symptoms.
Biomarkers:
High expression of non Th2 mediators such as tumor
necrosis factor (TNF)-a, IL-6 .
Hormones of obesity, such as adiponectin, leptin, and resistin
either alone or in association with increased oxidative stress.
Elevations in an endogenous inhibitor of iNOS, asymmetric
dimethyl arginine (ADMA).
lower amounts of FeNO, fewer eosinophils.
Treatment responses:
Patients of this subgroup usually respond poorly to corticosteroids.
Bariatric surgery induced weight loss was associated with profound
improvements in lung function and symptoms in obese asthma.
However, the effect of weight loss on bronchial hyper responsiveness
was only shown in late-onset, nonallergic (non-Th2) asthma patient,
consistent with late onset obese asthma being a separate endotype. This
is further supported by the increase in ADMA in association with
worsening severity and control in late onset obese asthma only.
Clinical characteristics and biomarkers:
It remains controversial whether neutrophilia is an independent driving
component, a synergistic factor with eosinophilia or just a consequence of
corticosteroid therapy.
Still unclear whether this represents a unique form of asthma or just a
different stage of severity or persistent bacterial colonization or infection of
the airways on the background of a previously eosinophilic asthma.
Airway pathophysiology in neutrophilic asthma is characterized by (fixed)
airflow limitation more trapping of air, thicker airway walls (as
measured by CT) .
Novel mechanisms implicated in the pathogenesis of
noneosinophilic asthma involve the activation of innate immune
responses with a possible role of bacteria, viruses.
Neutrophilia can also co-exist with eosinophilia, and this identifies
the people with the most severe asthma and emphasizes the
complexity of the immunobiology of severe asthma in which
multiple different innate and adaptive immune pathways and cells
may have roles.
Impaired nuclear recruitment of histone deacetylase (HDAC).
The role of TH17 immunity
Biomarkers:
IL-8, IL-17A, LTB4, and possibly IL-32.
IL-1 and TNF-α pathways are upregulated and associated with
neutrophilic inflammation in a sputum gene-expression study.
low levels of FeNO.
Treatment responses:
Corticosteroids are less effective in patients of this subgroup.
Macrolide antibiotics may have some efficacy on neutrophilic
asthma, By modulating the innate immune response in the
lung, by reducing the expression of neutrophilic markers .
Restoration of HDAC 2 nuclear recruitment with theophylline.
Anti-TNF-α responsive( infliximab )
The efficacy of IL-17 targeted therapy in this subtype of
asthma awaits evidence from ongoing clinical trials.
Smoking has a complex relationship with asthma. It is
associated with deteriorating lung function and resistance to
corticosteroids.
Smoking asthma has been associated with neutrophilia in lung
tissue.
It is unknown if smoking asthma is a subtype of neutrophilic
asthma or an independent endotype . Since not all smoking
asthma is accompanied by neutrophilia, it is more likely that
there is only a partial overlap between neutrophilic asthma and
smoking asthma.
Some reports have suggested that smoking is associated with
elevated total IgE and that active smoking may increase the risk of
sensitization to workplace allergens.
However, little is understood regarding the role of genetics,
biomarkers or pathobiology.
FeNO levels are decreased by smoking and could help to
differentiate asthmatic subjects from non-asthmatic subjects.
Treatment responses
Quitting smoking
Restoration of HDAC 2 nuclear recruitment with theophylline.
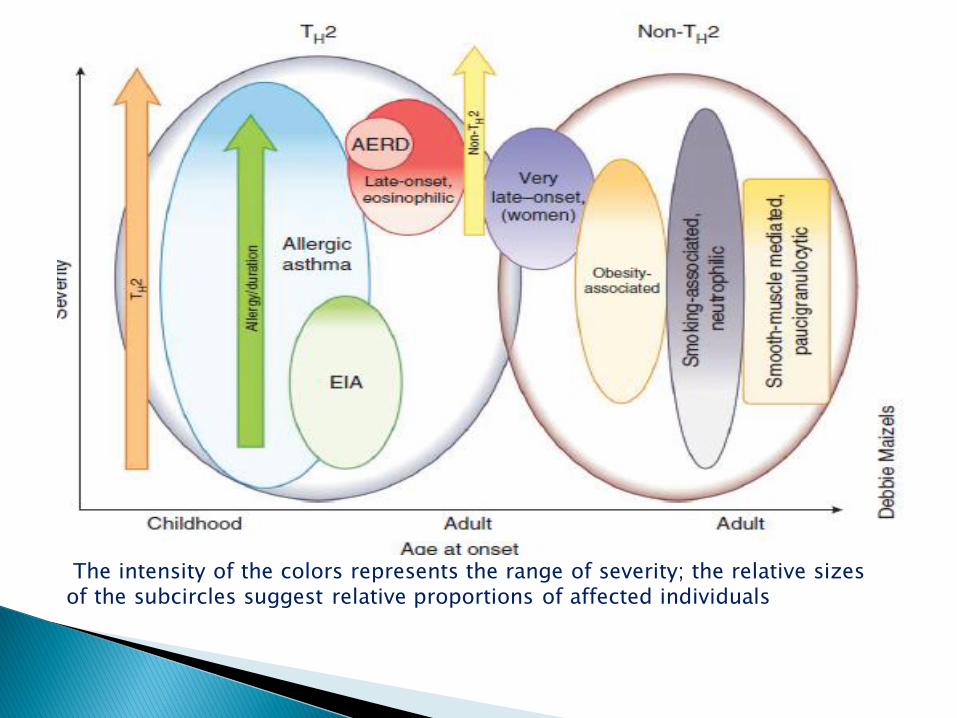
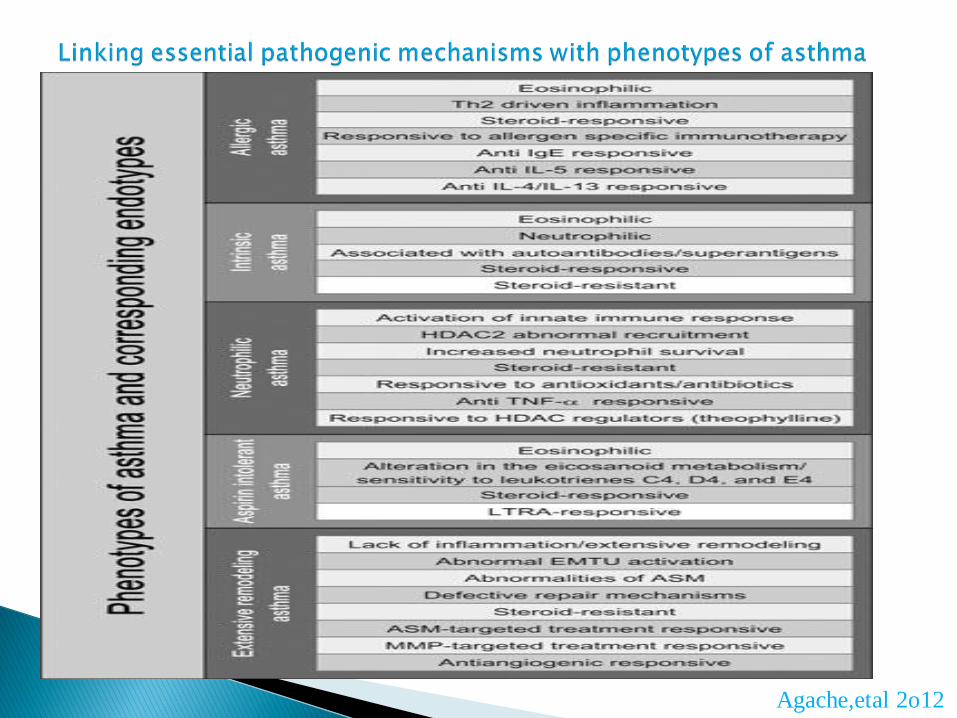
The intensity of the colors represents the range of severity; the relative sizes of the subcircles suggest relative proportions of affected individuals
Lötvall et al.2011 proposed endotyping asthma into six classes
depending on several parameters used to define an endotype.
Aspirin sensitive asthma
Allergic asthma (adults)
Severe late-onset hypereosinophilic
ABPM
API-positive preschool wheezer
Asthma in cross country skiers
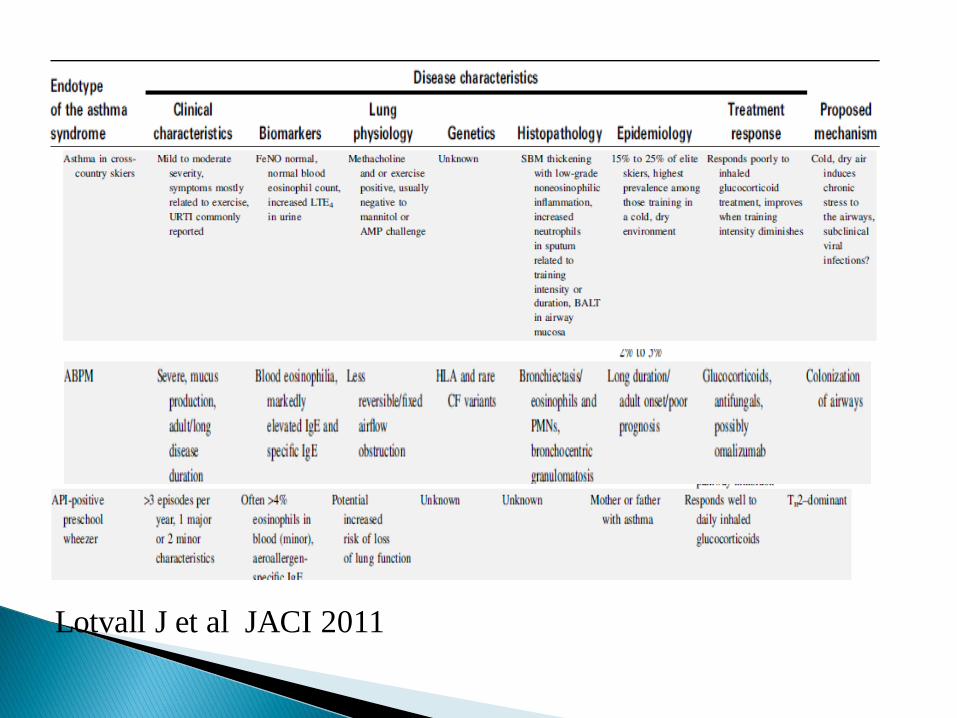
Lotvall J et al JACI 2011
Agache,etal 2o12
The principle of personalized or individualized medicine is to
'bring the right drug to the right patient at the right dose', such
that therapeutic efficacy is maximized and the side effects are
kept to a minimum.
The consideration of disease endotypes in treatment design
should be able to bridge the present era of treating asthma
based on family history, patient characteristics and laboratory
test, to the future era of personalized medicine where
treatment scheme will be based on individual biological data
such as genomic, proteomic and metabolic profiles.
This study present video-assisted thoracoscopic biopsy
findings from 10 patients, previously diagnosed with severe
asthma and meeting criteria for asthma. Pathobiologically,
these patients have evidence for asthmatic small airway
inflammation and infrequent nonnecrotizing granulomas with
interstitial inflammation. This distinct pathobiology in addition
to their response to cytotoxic agents suggests that these
patients represent a newly described disease, which we term
asthmatic granulomatosis.
Sally E. Wenzel1, Catherine A. Vitari1, Manisha Shende2, Diane C. Strollo3,
Allyson Larkin4, and Samuel A. Yousem5 Am J Respir Crit Care Med Vol 186, Iss. 6, pp 501–507, Sep 15, 2012
Asthmatic Granulomatosis A Novel Disease with Asthmatic and
Granulomatous Features
The Asthma–Chronic Obstructive
Pulmonary Disease Overlap
Syndrome (ACOS)
The Spanish COPD guidelines propose
four COPD phenotypes that determine
differential treatment: nonexacerbator
with emphysema or chronic bronchitis,
mixed COPD–asthma, exacerbator with
emphysema and exacerbator with
chronic bronchitis
ACOS
ACOS
The mixed COPD–asthma phenotype was
defined as an airflow obstruction that is not
completely reversible accompanied by
symptoms or signs of an increased
reversibility of the obstruction.[7] In other
guidelines, these patients are described as
'patients with COPD and prominent asthmatic
component' or as asthma that complicates
COPD.
ACOS
*Two major criteria (FEV1 >15% and >400 ml
after bronchodilator or sputum eosinophils or
history of asthma) and
*Two minor criteria (elevated total IgE or
history of atopy or FEV1 >12% and >200 ml
after bronchodilator) are recommended.
ACOS
*Asthma with partially reversible airflow obstruction
– that is, based on change in FEV1 with
bronchodilators – with or without emphysema or
reduced carbon monoxide diffusing capacity (DLco)
to <80% predicted;
*COPD with emphysema accompanied by
reversible or partially reversible airflow obstruction,
with or without environmental allergies or reduced
DLco.
ACOS
The following major criteria for ACOS:
a physician diagnosis of asthma and COPD in the
same patient, history or evidence of atopy, for
example, hay fever, elevated total IgE, age 40 years
or more, smoking >10 pack-years,
postbronchodilator FEV1 <80% predicted and
FEV1/FVC <70%.
Minor criteria:
A ≥15% increase in FEV1 or ≥12% and ≥200 ml
increase in FEV1 postbronchodilator treatment with
albuterol .
Do oral Beta Blockers Really
Exacerbate Asthma?
Recent investigations suggest BB therapy may actually improve asthma. A 2002 meta-analysis found no significant adverse effects of beta-blocker therapy in people with mild-to-moderate asthma, and in fact, bronchodilator response increased with chronic beta-blocker treatment. Thorax 2011;66:502-507.
72
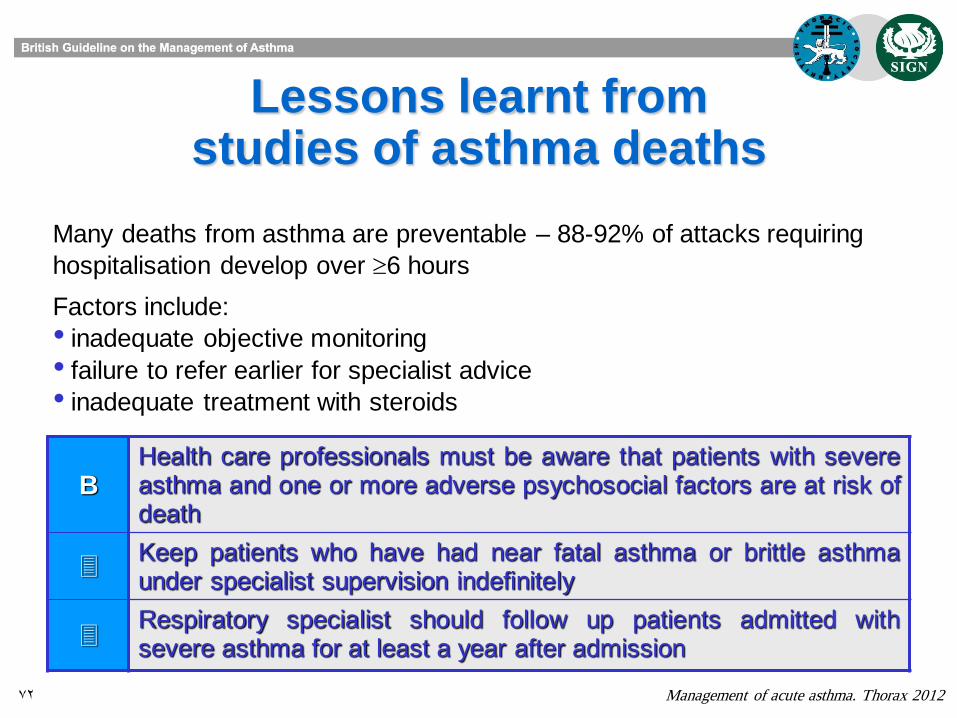
Lessons learnt from studies of asthma deaths
Management of acute asthma. Thorax 2012
B Health care professionals must be aware that patients with severe asthma and one or more adverse psychosocial factors are at risk of death
Keep patients who have had near fatal asthma or brittle asthma under specialist supervision indefinitely
Respiratory specialist should follow up patients admitted with severe asthma for at least a year after admission
Many deaths from asthma are preventable – 88-92% of attacks requiring
hospitalisation develop over 6 hours
Factors include:
• inadequate objective monitoring
• failure to refer earlier for specialist advice
• inadequate treatment with steroids
73
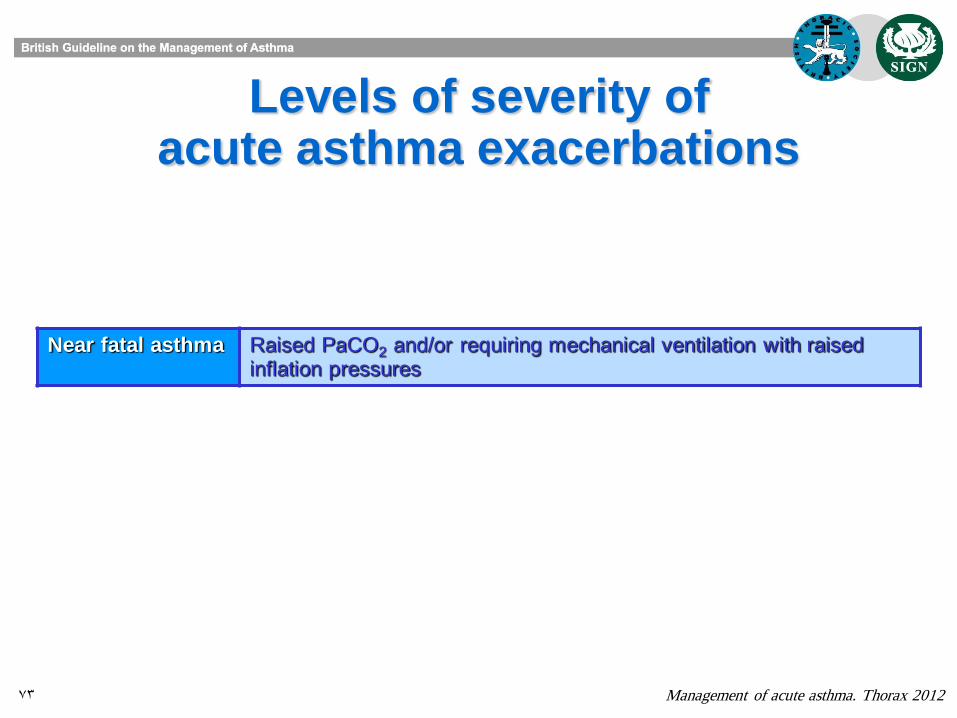
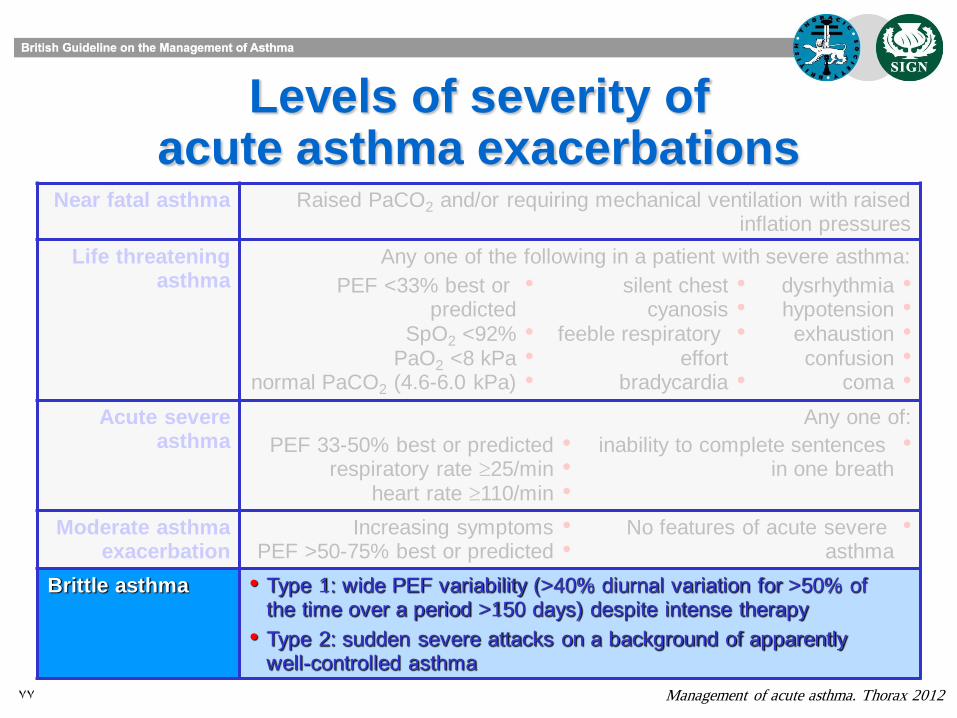
Levels of severity of acute asthma exacerbations
Management of acute asthma. Thorax 2012
Near fatal asthma Raised PaCO2 and/or requiring mechanical ventilation with raised inflation pressures
74
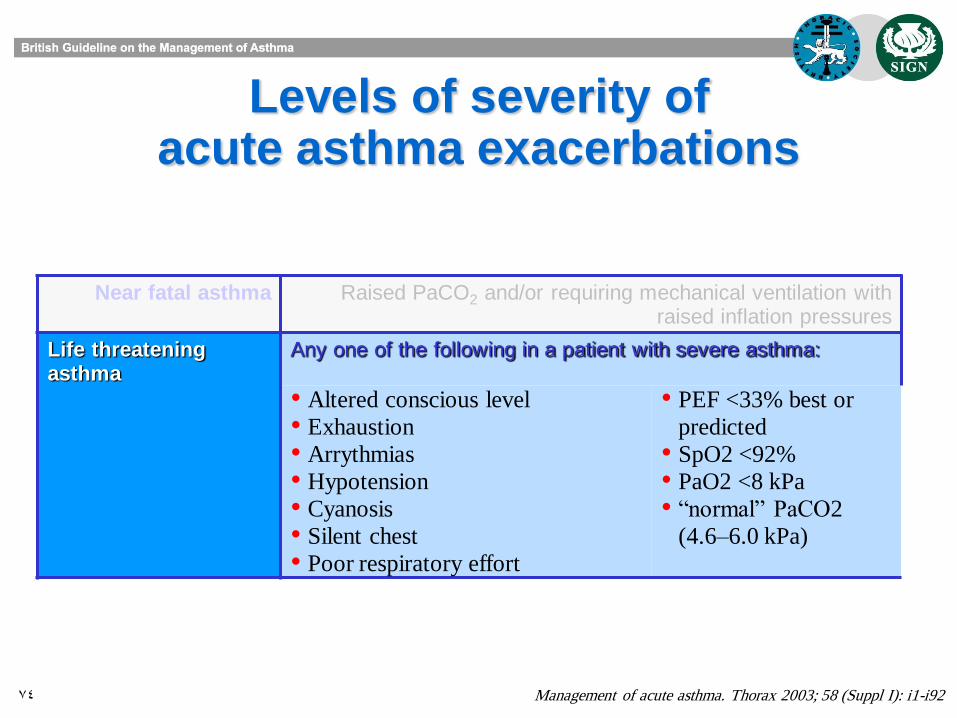
Levels of severity of acute asthma exacerbations
Management of acute asthma. Thorax 2003; 58 (Suppl I): i1-i92
Near fatal asthma Raised PaCO2 and/or requiring mechanical ventilation with raised inflation pressures
Life threatening asthma
Any one of the following in a patient with severe asthma:
• Altered conscious level
• Exhaustion
• Arrythmias
• Hypotension
• Cyanosis
• Silent chest
• Poor respiratory effort
• PEF <33% best or
predicted
• SpO2 <92%
• PaO2 <8 kPa • “normal” PaCO2
(4.6–6.0 kPa)
75
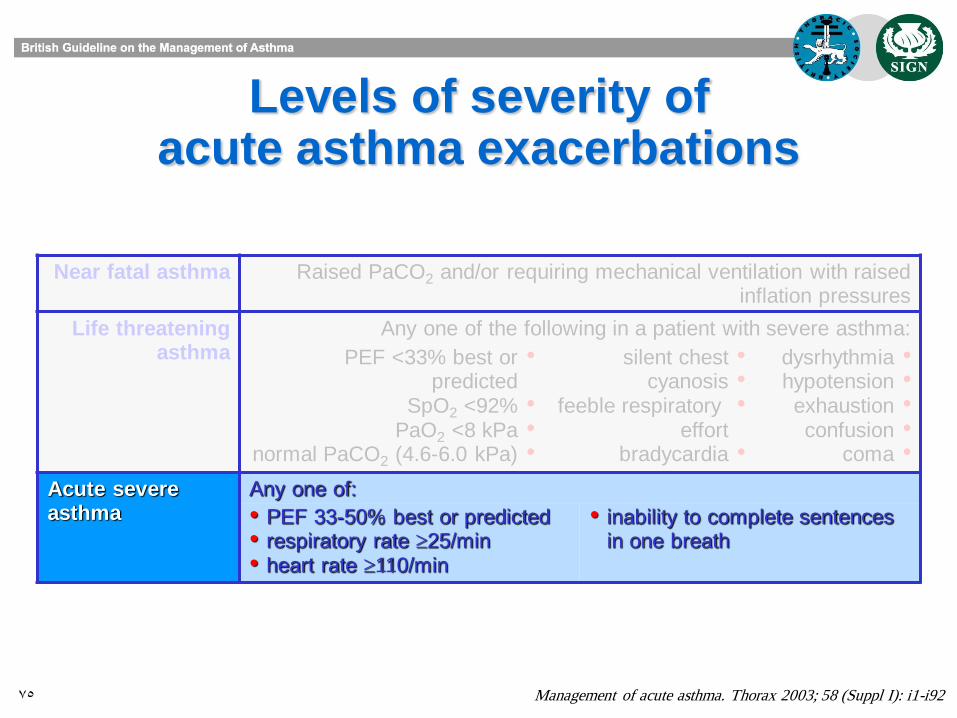
Levels of severity of acute asthma exacerbations
Management of acute asthma. Thorax 2003; 58 (Suppl I): i1-i92
Near fatal asthma Raised PaCO2 and/or requiring mechanical ventilation with raised inflation pressures
Life threatening asthma
Any one of the following in a patient with severe asthma:
•PEF <33% best or predicted
•SpO2 <92% •PaO2 <8 kPa •normal PaCO2 (4.6-6.0 kPa)
•silent chest •cyanosis •feeble respiratory
effort •bradycardia
•dysrhythmia •hypotension •exhaustion •confusion •coma
Acute severe asthma
Any one of:
• PEF 33-50% best or predicted • respiratory rate 25/min • heart rate 110/min
• inability to complete sentences in one breath
76
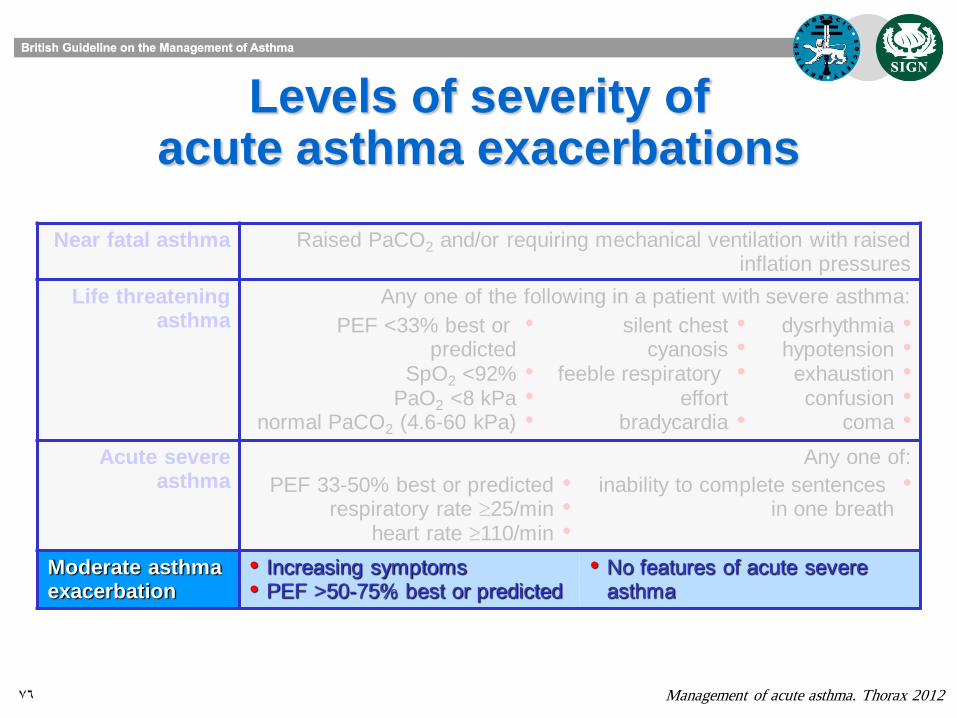
Levels of severity of acute asthma exacerbations
Management of acute asthma. Thorax 2012
Near fatal asthma Raised PaCO2 and/or requiring mechanical ventilation with raised inflation pressures
Life threatening asthma
Any one of the following in a patient with severe asthma:
•PEF <33% best or predicted
•SpO2 <92% •PaO2 <8 kPa •normal PaCO2 (4.6-60 kPa)
•silent chest •cyanosis •feeble respiratory
effort •bradycardia
•dysrhythmia •hypotension •exhaustion •confusion •coma
Acute severe asthma
Any one of:
•PEF 33-50% best or predicted •respiratory rate 25/min •heart rate 110/min
•inability to complete sentences in one breath
Moderate asthma exacerbation
• Increasing symptoms • PEF >50-75% best or predicted
• No features of acute severe asthma
77
Levels of severity of acute asthma exacerbations
Management of acute asthma. Thorax 2012
Near fatal asthma Raised PaCO2 and/or requiring mechanical ventilation with raised inflation pressures
Life threatening asthma
Any one of the following in a patient with severe asthma:
•PEF <33% best or predicted
•SpO2 <92% •PaO2 <8 kPa •normal PaCO2 (4.6-6.0 kPa)
•silent chest •cyanosis •feeble respiratory
effort •bradycardia
•dysrhythmia •hypotension •exhaustion •confusion •coma
Acute severe asthma
Any one of:
•PEF 33-50% best or predicted •respiratory rate 25/min •heart rate 110/min
•inability to complete sentences in one breath
Moderate asthma exacerbation
•Increasing symptoms •PEF >50-75% best or predicted
•No features of acute severe asthma
Brittle asthma • Type 1: wide PEF variability (>40% diurnal variation for >50% of the time over a period >150 days) despite intense therapy
• Type 2: sudden severe attacks on a background of apparently well-controlled asthma
78
Initial assessment – the role of symptoms, signs and measurements
Management of acute asthma. Thorax 2012
Clinical features Clinical features can identify some patients with severe asthma,
eg severe breathlessness (including too breathless to complete
sentences in one breath), tachypnea, tachycardia, silent chest,
cyanosis, accessory muscle use, altered consciousness or
collapse.
None of these singly or together is specific. Their absence does not
exclude a severe attack.
79
Initial assessment – the role of symptoms, signs and measurements
Management of acute asthma. Thorax 2003; 58 (Suppl I): i1-i92
Clinical features Clinical features, symptoms and respiratory and cardiovascular signs helpful in recognising severe asthma, but none specific, and their absence
does not exclude a severe attack
PEF or FEV1 Measurements of airway caliber improve recognition of the
degree of severity, the appropriateness or intensity of therapy, and
decisions about management in hospital or at home.
PEF or FEV1 are useful and valid measures of airway caliber. PEF is
more convenient in the acute situation.
PEF expressed as a percentage of the patient‟s previous best value
is most useful clinically. PEF as a percentage of predicted gives
a rough guide in the absence of a known previous best value.
Different peak flow meters give different readings. Where possible
the same or similar type of peak flow meter should be used.
80
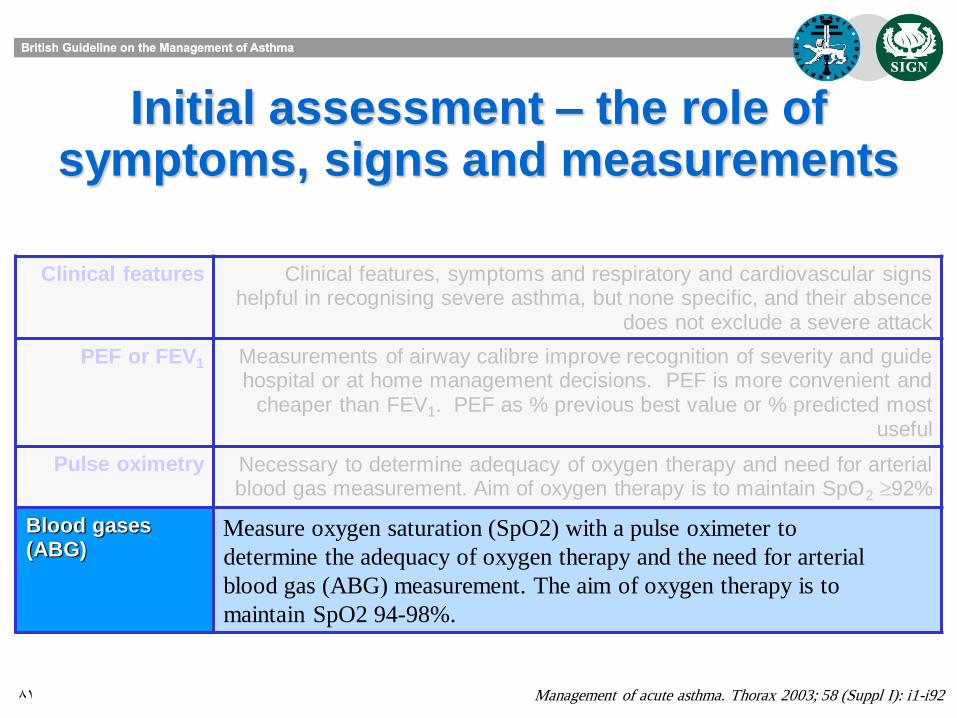
Initial assessment – the role of symptoms, signs and measurements
Management of acute asthma. Thorax 2012
Clinical features Clinical features, symptoms and respiratory and cardiovascular signs helpful in recognising severe asthma, but none specific, and their absence
does not exclude a severe attack
PEF or FEV1 Measurements of airway calibre improve recognition of severity and guide hospital or at home management decisions. PEF is more convenient and
cheaper than FEV1. PEF as % previous best value or % predicted most useful
Pulse oximetry Measure oxygen saturation (SpO2) with a pulse oximeter to
determine the adequacy of oxygen therapy and the need for arterial
blood gas (ABG) measurement. The aim of oxygen therapy is to
maintain SpO2 94-98%.
81
Initial assessment – the role of symptoms, signs and measurements
Management of acute asthma. Thorax 2003; 58 (Suppl I): i1-i92
Clinical features Clinical features, symptoms and respiratory and cardiovascular signs helpful in recognising severe asthma, but none specific, and their absence
does not exclude a severe attack
PEF or FEV1 Measurements of airway calibre improve recognition of severity and guide hospital or at home management decisions. PEF is more convenient and
cheaper than FEV1. PEF as % previous best value or % predicted most useful
Pulse oximetry Necessary to determine adequacy of oxygen therapy and need for arterial blood gas measurement. Aim of oxygen therapy is to maintain SpO2 92%
Blood gases (ABG)
Measure oxygen saturation (SpO2) with a pulse oximeter to
determine the adequacy of oxygen therapy and the need for arterial
blood gas (ABG) measurement. The aim of oxygen therapy is to
maintain SpO2 94-98%.
82
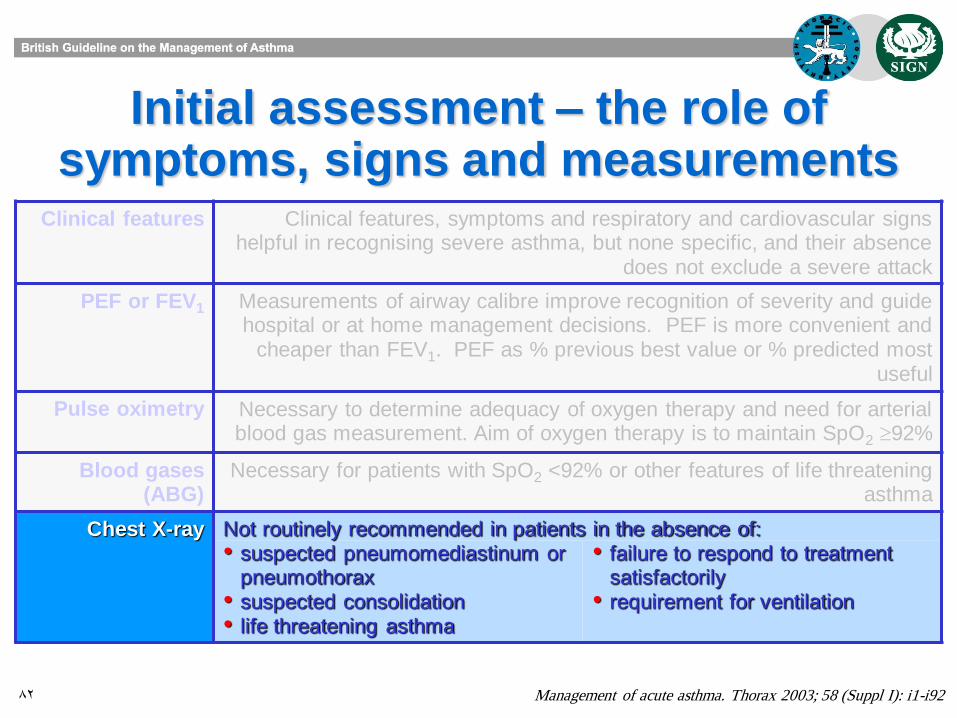
Initial assessment – the role of symptoms, signs and measurements
Management of acute asthma. Thorax 2003; 58 (Suppl I): i1-i92
Clinical features Clinical features, symptoms and respiratory and cardiovascular signs helpful in recognising severe asthma, but none specific, and their absence
does not exclude a severe attack
PEF or FEV1 Measurements of airway calibre improve recognition of severity and guide hospital or at home management decisions. PEF is more convenient and
cheaper than FEV1. PEF as % previous best value or % predicted most useful
Pulse oximetry Necessary to determine adequacy of oxygen therapy and need for arterial blood gas measurement. Aim of oxygen therapy is to maintain SpO2 92%
Blood gases (ABG)
Necessary for patients with SpO2 <92% or other features of life threatening asthma
Chest X-ray Not routinely recommended in patients in the absence of: • suspected pneumomediastinum or
pneumothorax • suspected consolidation • life threatening asthma
• failure to respond to treatment satisfactorily
• requirement for ventilation
83
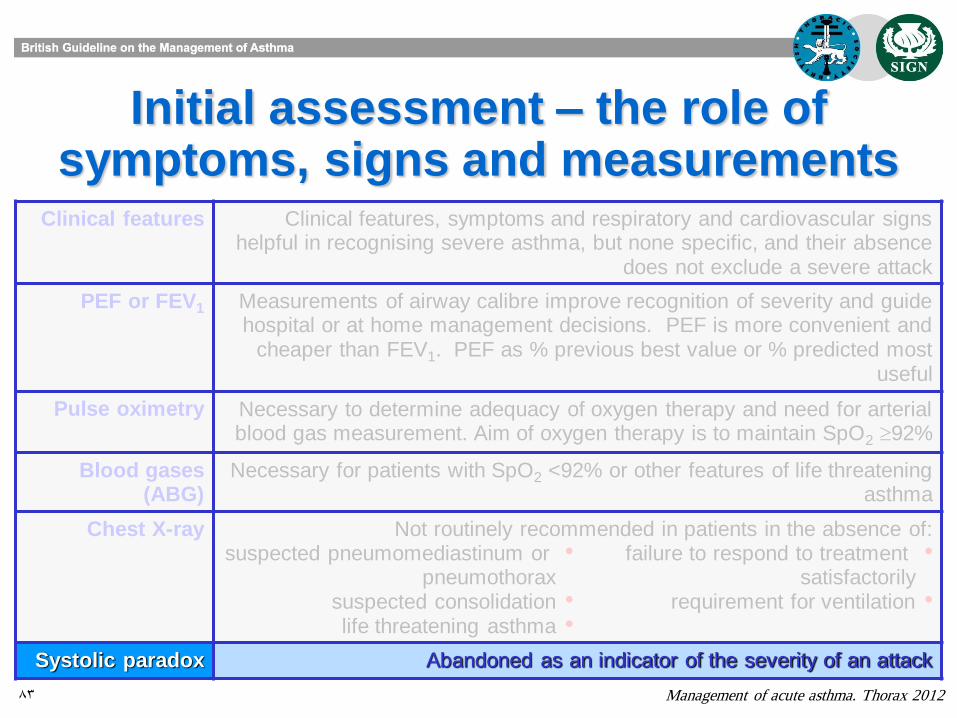
Initial assessment – the role of symptoms, signs and measurements
Management of acute asthma. Thorax 2012
Clinical features Clinical features, symptoms and respiratory and cardiovascular signs helpful in recognising severe asthma, but none specific, and their absence
does not exclude a severe attack
PEF or FEV1 Measurements of airway calibre improve recognition of severity and guide hospital or at home management decisions. PEF is more convenient and
cheaper than FEV1. PEF as % previous best value or % predicted most useful
Pulse oximetry Necessary to determine adequacy of oxygen therapy and need for arterial blood gas measurement. Aim of oxygen therapy is to maintain SpO2 92%
Blood gases (ABG)
Necessary for patients with SpO2 <92% or other features of life threatening asthma
Chest X-ray Not routinely recommended in patients in the absence of: •suspected pneumomediastinum or
pneumothorax •suspected consolidation •life threatening asthma
•failure to respond to treatment satisfactorily
•requirement for ventilation
Systolic paradox Abandoned as an indicator of the severity of an attack
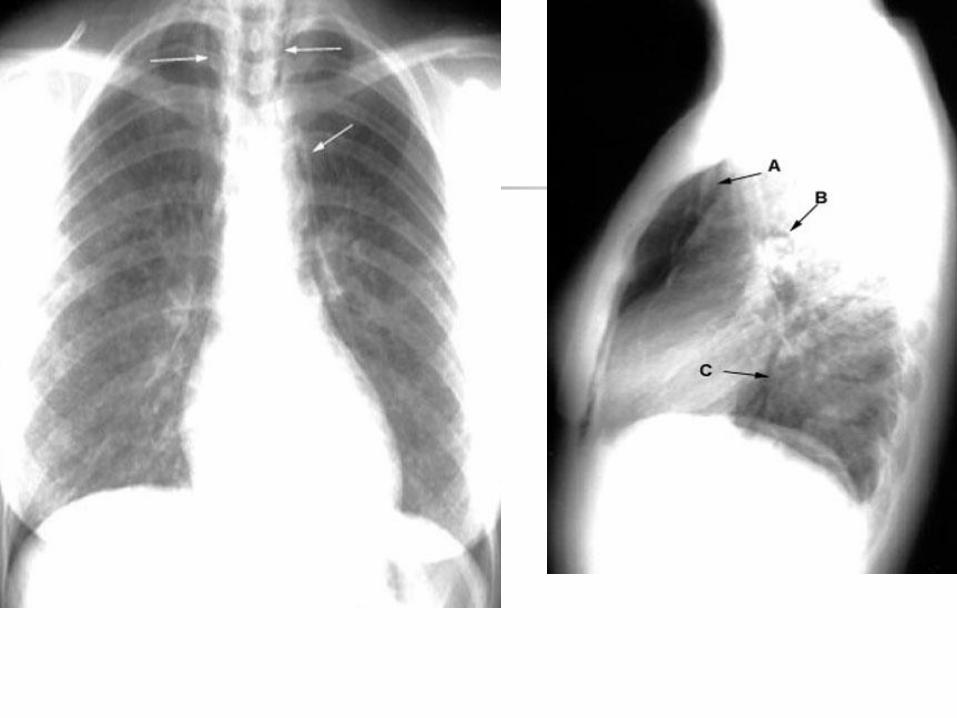
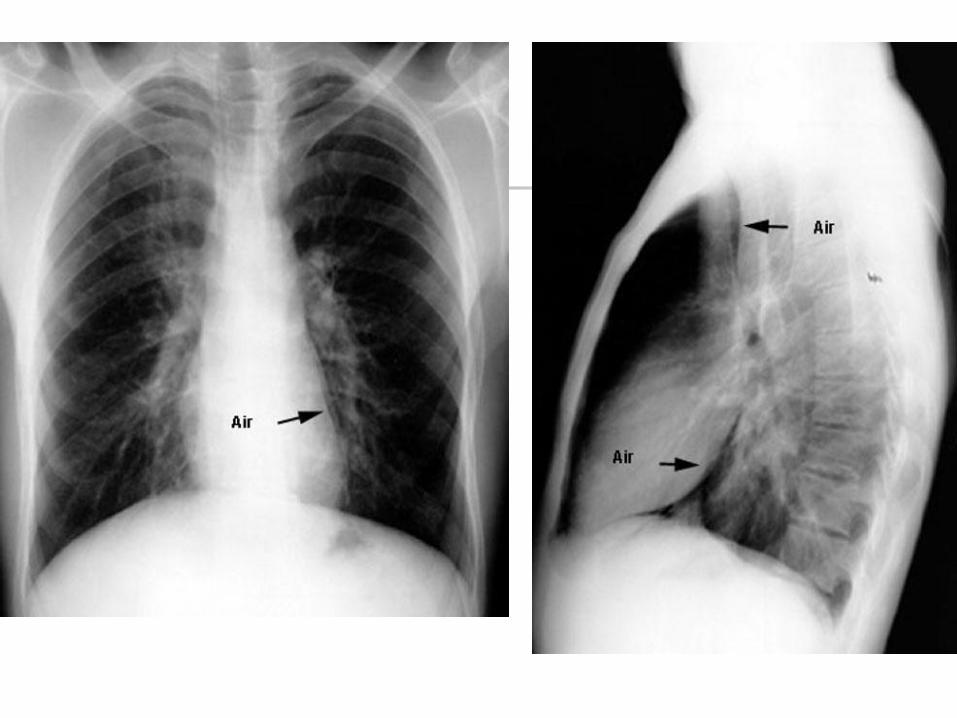
Radiographic Signs of Pneumomediastinum
Subcutaneous emphysema
Thymic sail sign
Pneumoprecardium
Ring around the artery sign
Tubular artery sign
Double bronchial wall sign
Continuous diaphragm sign
Extrapleural sign
Air in the pulmonary ligament


Pediatric Asthma Not all wheezing is asthma
Wheezing occurrences in children:
- single episode in 30% to 50% of children
before 5 yr of age
- 40% who wheeze before 3 yr of age continue
at 6 yr (“persistent wheezers”)
- 50% of infants who wheeze once will wheeze
again within several months
Wheezing in Children - Phenotypes
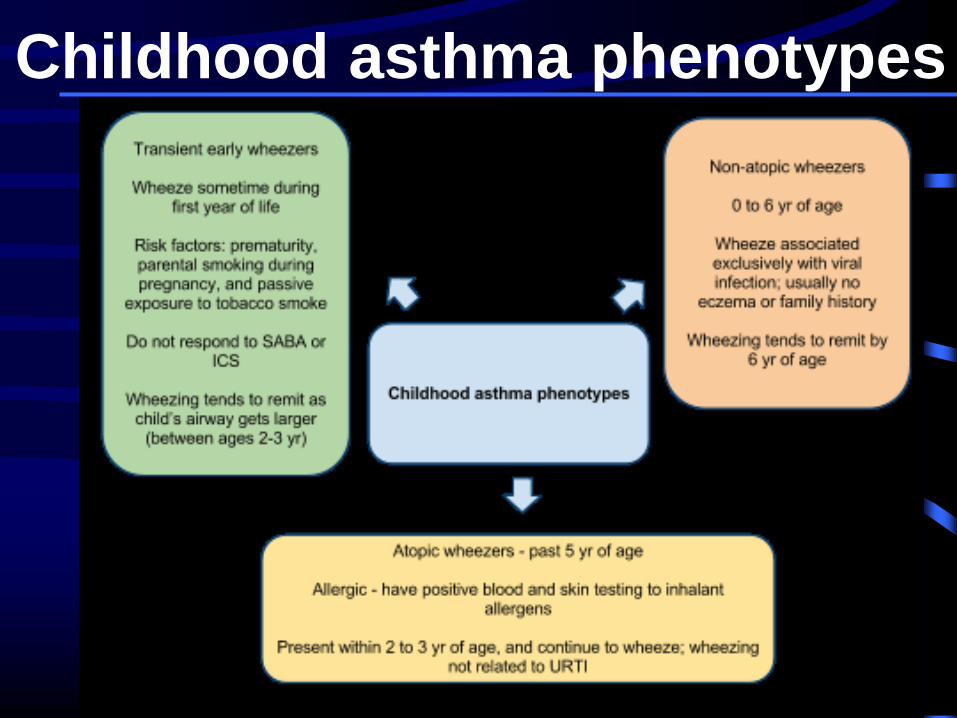
Childhood asthma phenotypes
Childhood asthma phenotypes
*A 2012 study described 2 "new" phenotypes for
young children with wheezing: "boys atopic
multiple-trigger" and "girls nonatopic uncontrolled
wheeze". JACI, 2012.
*Toward a definition of asthma phenotypes in
childhood: early viral wheezers, multitrigger
wheezers (MTWs), and nonatopic uncontrolled
wheezers (NAUWs). Some children have “allergic
bronchitis” rather than “asthma”. JACI, 2012.
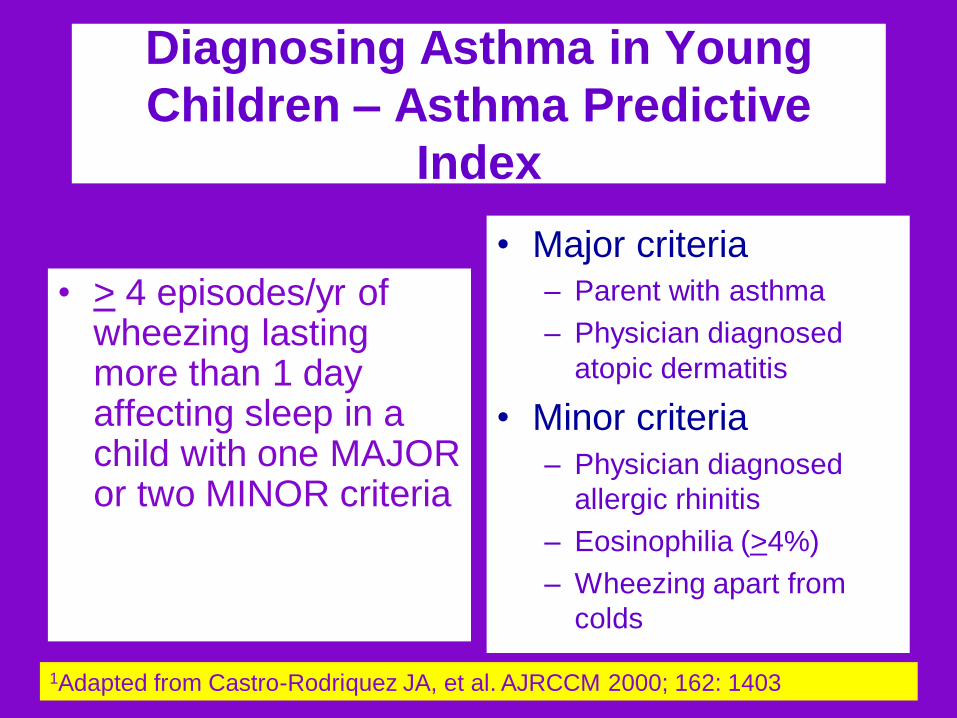
Diagnosing Asthma in Young
Children – Asthma Predictive
Index
• > 4 episodes/yr of wheezing lasting more than 1 day affecting sleep in a child with one MAJOR or two MINOR criteria
• Major criteria – Parent with asthma
– Physician diagnosed
atopic dermatitis
• Minor criteria
– Physician diagnosed
allergic rhinitis
– Eosinophilia (>4%)
– Wheezing apart from
colds
1Adapted from Castro-Rodriquez JA, et al. AJRCCM 2000; 162: 1403
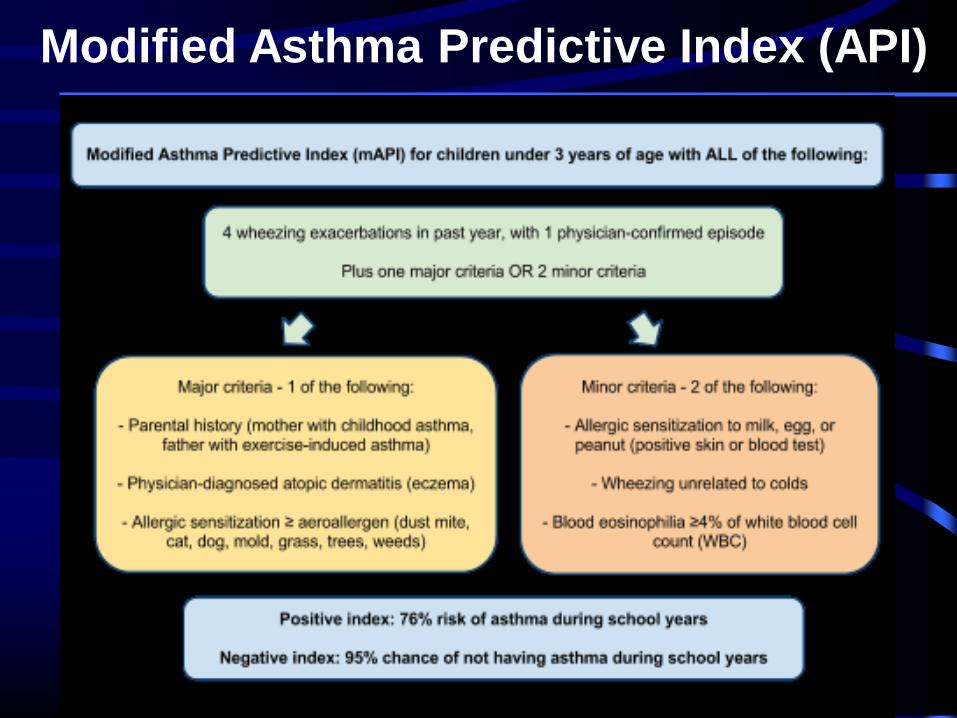
Modified Asthma Predictive Index (API)
Cough-variant asthma
Cough-variant asthma presents as dry
cough at night. It worsens with exercise
(EIA) and nonspecific triggers (cold air).
Cough-variant asthma responds to asthma
therapy with ICS.
Cough-variant asthma is diagnosed with
pulmonary function testing (PFTs) with
response to bronchodilator. The most
common cause of chronic cough in children
is cough-variant asthma.
Guidelines National Heart, Lung, and Blood Institute (NHLBI) guidelines
for diagnosis and management of asthma
Key concepts: - severity dictates therapy
- - distinction between intermittent and persistent asthma
- - "rule of 2s”
- - 4 levels of asthma severity - intermittent; 3 sublevels of
persistent
- - inhaled corticosteroids (ICS) preferred for all levels of
persistent asthma
- - use of asthma action plans
- - spirometry recommended
Rule of 2s
- if symptoms are present for more than 2 days per
week or for more than 2 nights per month, asthma
categorized as persistent.
- Within this category, disease must be classified as
mild, moderate, or severe. However, as severity of
asthma not constant, must monitor patients for
changes; as severity changes, therapy should
change too.
- The category of “mild intermittent” asthma was
eliminated in the 2007 guidelines - now it is just called
“intermittent” asthma.
- impairment - refers to symptoms
- - risk - refers to likelihood that the patient will eventually
have exacerbation of asthma and present to emergency
department (ED) or hospital, or need course of oral
corticosteroids
- - control - refers to the level of patient’s asthma control
The concepts of “impairment”, “risk”, and “control” were
introduced in the 2007 guidelines:
Classification of asthma severity
- impairment domain - daytime and nighttime symptoms
(rule of 2's), use of short-acting beta-agonist (SABA),
interference with normal activities
- - risk domain - number of exacerbations per year (if more
than 2, daily controller medication is needed). Increased
risk is conferred by parental history of asthma or history of
eczema.
- Childhood Asthma Control Test (ACT) is validated down to
age 4 yr. Adult ACT questionnaire should be used for
teenagers (cutoff age is 11 years).
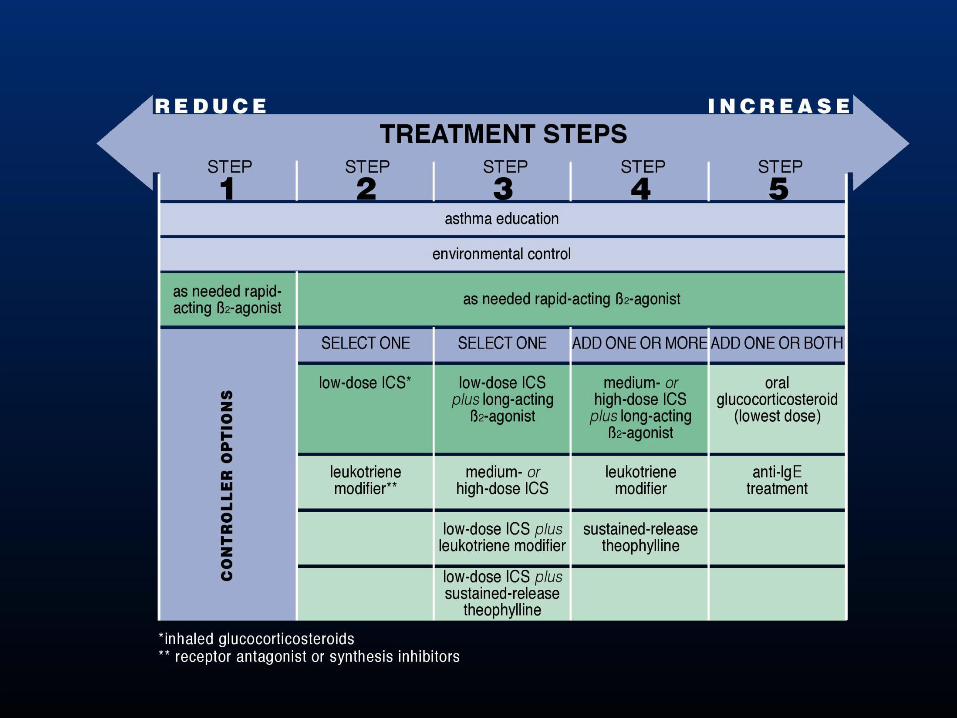
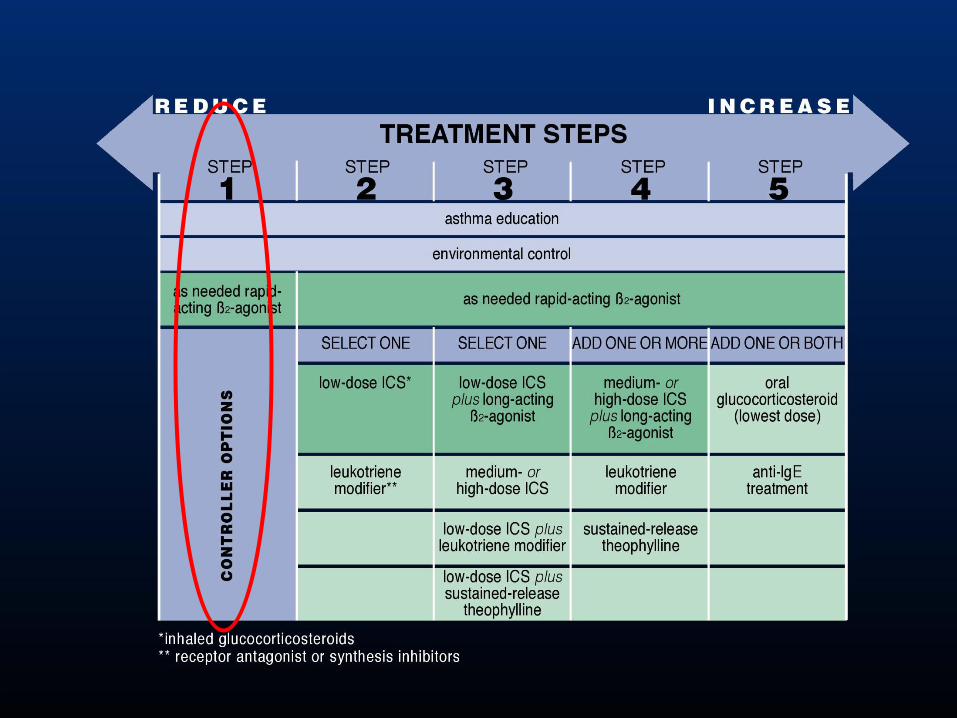
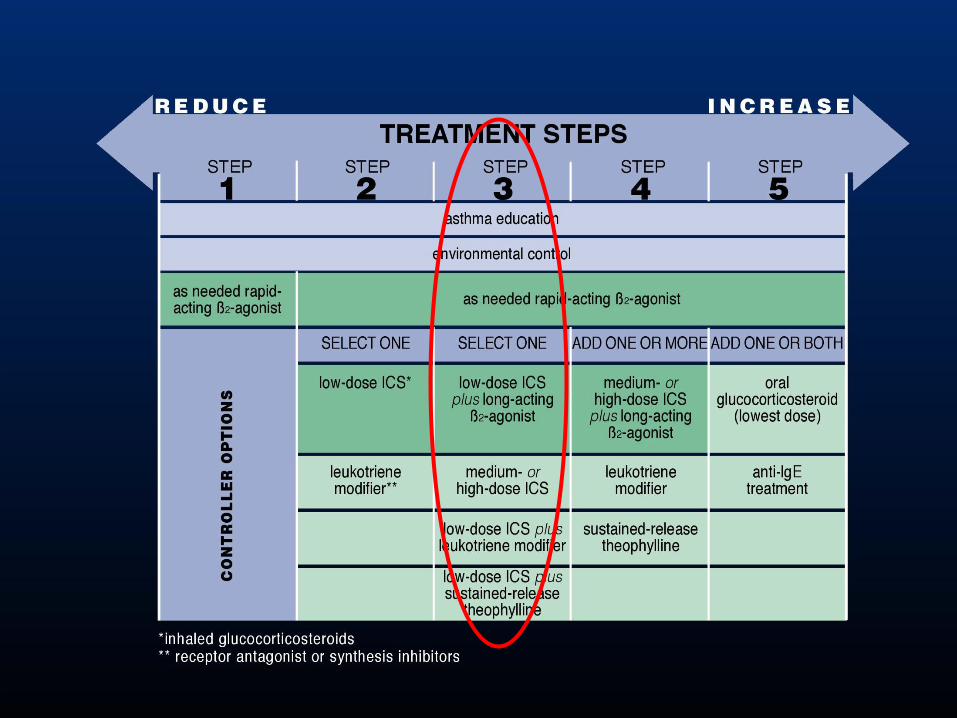
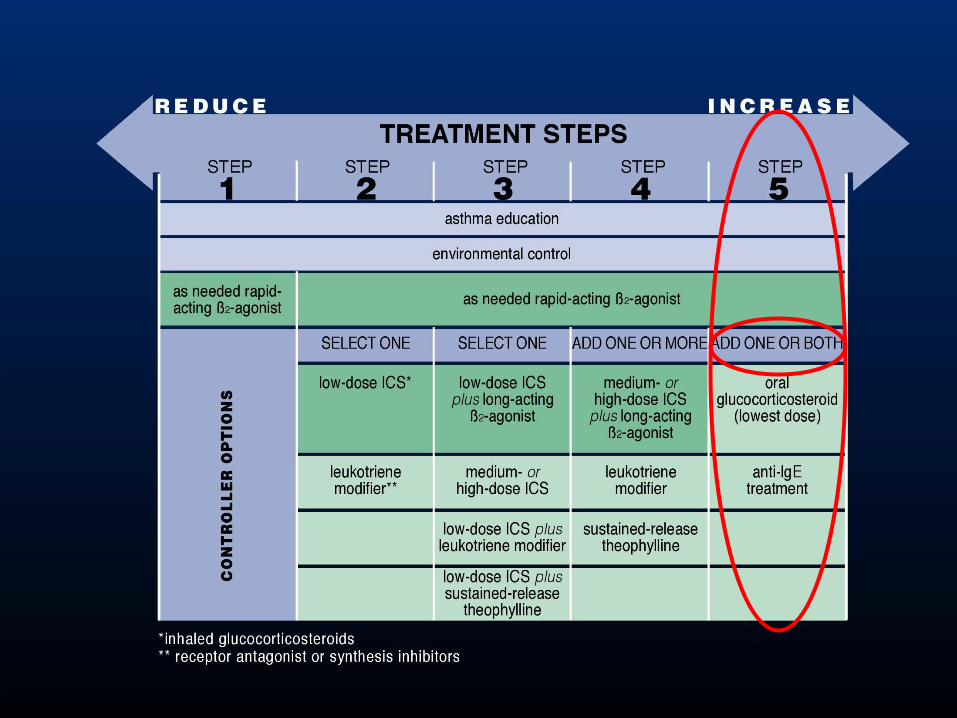
Treatment steps
- step 1 - SABA as needed –
- step 2 - low-dose ICS monotherapy vs. leukotriene receptor
antagonist (LTRA)
- - step 3 - low-to-medium dose ICS plus long-acting beta-
agonist (LABA)
- - step 4 - high-dose ICS therapy plus LABA and (if needed)
systemic corticosteroids. Omalizumab (Xolair; anti-IgE
antibody) is prescribed before placing patient on daily oral
corticosteroids.
“Rule of 2s” to determine level of control
- daytime symptoms more than 2 days/wk
- rescue β2 -agonist use more than 2 times per week
- nighttime symptoms more than 2 nights/mo
- more than 2 rescue β2-agonist canisters/yr

Step Down or Step Up
When to step down therapy? If patient is well-controlled for
3 mo, consider stepping down therapy.
When to step up therapy? If the patient is not well-
controlled, step up therapy and re-evaluate in 2 to 6 wk. If the
patient is very poorly controlled, step up therapy 2 steps,
consider short course of steroids, and reassess in 2 wk.
When to consider long-term ICS treatment
- positive API and more than 3 wheezing episodes in
previous 12 mo lasting more than 1 day and affecting
sleep
- consistent requirement for SABA treatment (more than
2 times/wk, on average, over 1-2 mo); 2 exacerbations in
6 mo requiring oral corticosteroids
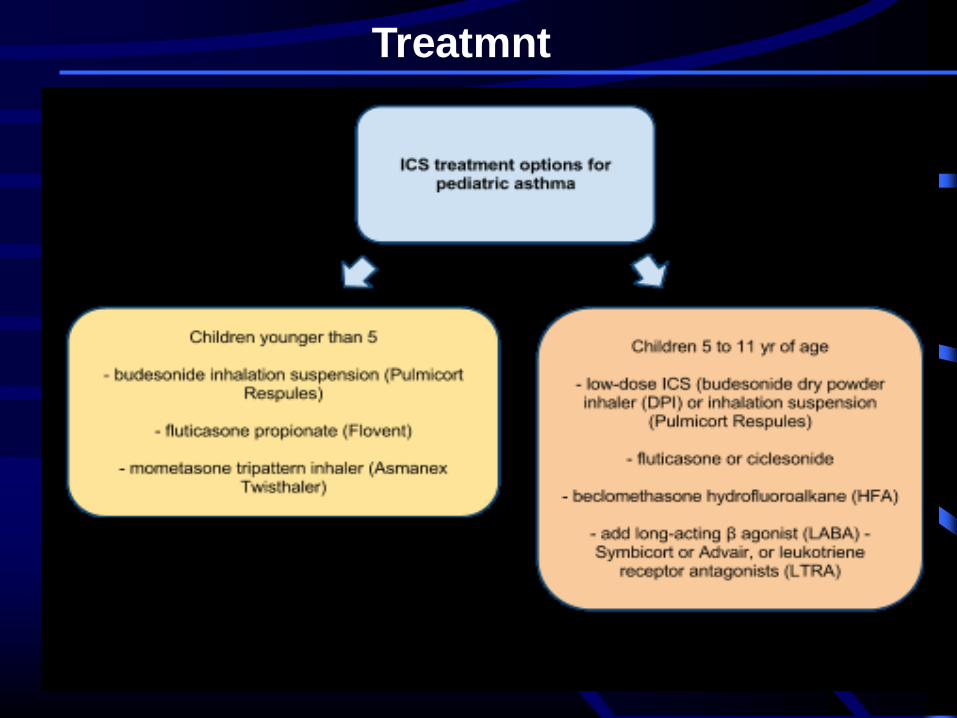
Treatmnt
Inhaled corticosteroid
Relative binding affinity for glucocorticoid receptor (GR):
mometasone = fluticasone > budesonide > triamcinolone.
Relative anti-inflammatory potency: mometasone =
fluticasone > budesonide = beclomethasone >
triamcinolone.
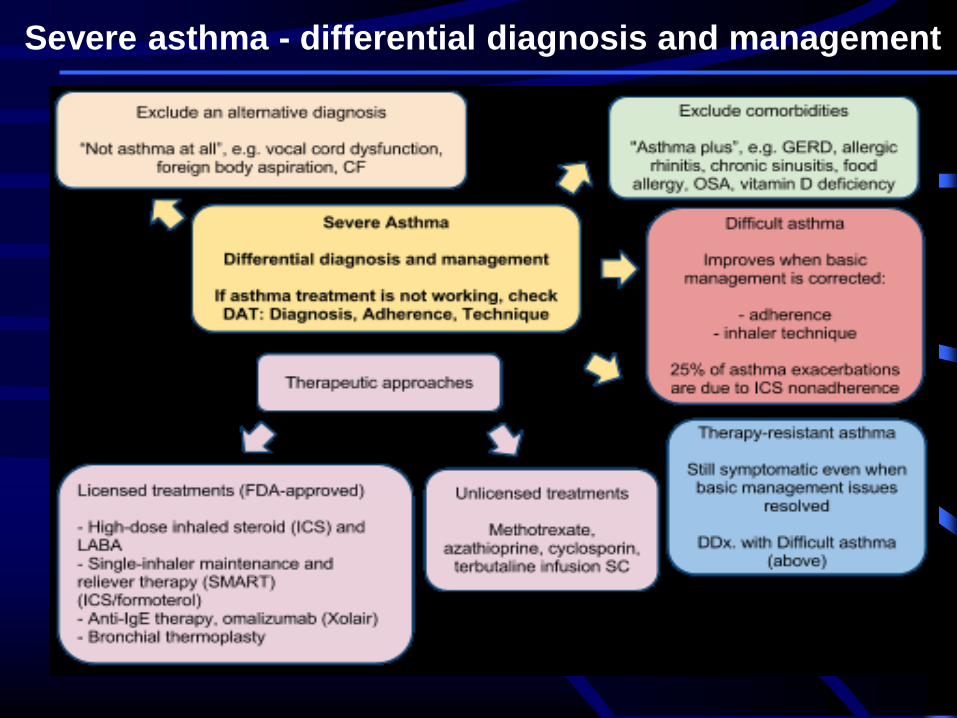
Severe asthma - differential diagnosis and management
Treating to Maintain Asthma Control
Stepping up treatment in response to loss of control
Use of a combination rapid and long-acting inhaled β2-agonist (e.g., formoterol) and an inhaled glucocorticosteroid (e.g., budesonide) in a single inhaler both as a controller and reliever is effecting in maintaining a high level of asthma control and reduces exacerbations (Evidence A)
Doubling the dose of inhaled glucocortico-steroids is not effective, and is not recommended (Evidence A)
Difficult Asthma
Other terminology
• Severe asthma
• Difficult to control asthma
• Difficult to treath asthma
• Refractory asthma
• Steroid resistant asthma
• Unstable asthma
• Life threatening asthma
• Definition
• Factors that could be preventing a
normal response to asthma medication
• Phenotypes
• Risk Factors
Severe - Difficult Asthma
Definition - ERS Task Force
• ‘failure to achieve asthma
control when maximally
recommended doses of
inhaled therapy are
prescribed for at least 6 -
12 months’
ERS Task Force: ERJ 1999;13:1198-6
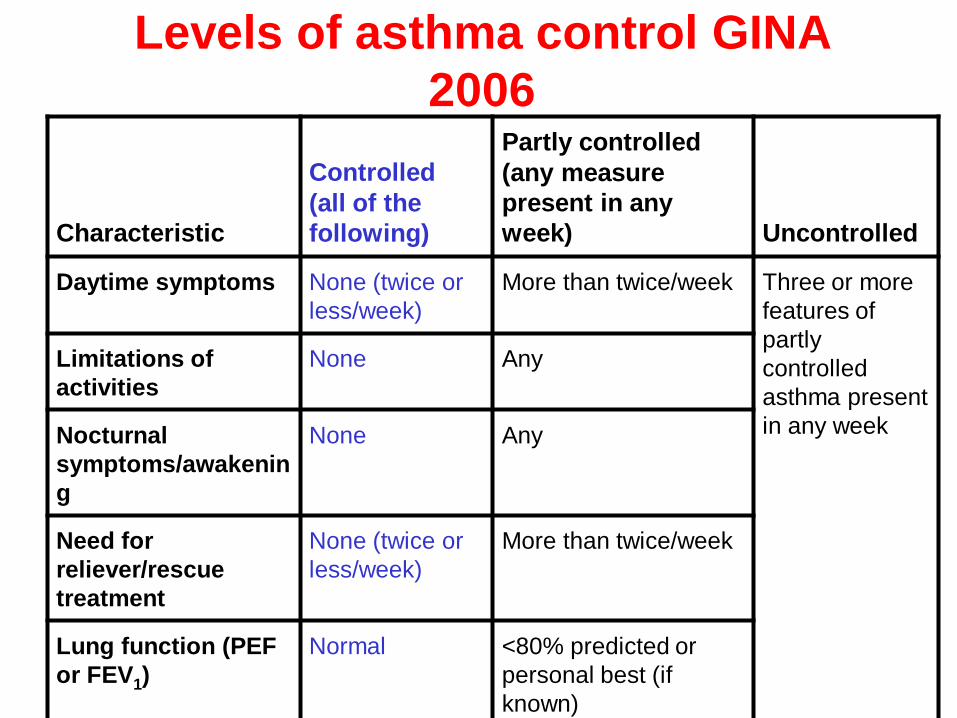
Levels of asthma control GINA
2006
Characteristic
Controlled
(all of the
following)
Partly controlled
(any measure
present in any
week) Uncontrolled
Daytime symptoms None (twice or
less/week)
More than twice/week Three or more
features of
partly
controlled
asthma present
in any week
Limitations of
activities
None Any
Nocturnal
symptoms/awakenin
g
None Any
Need for
reliever/rescue
treatment
None (twice or
less/week)
More than twice/week
Lung function (PEF
or FEV1)
Normal <80% predicted or
personal best (if
known)
Exacerbations None One or more/year One in any
week
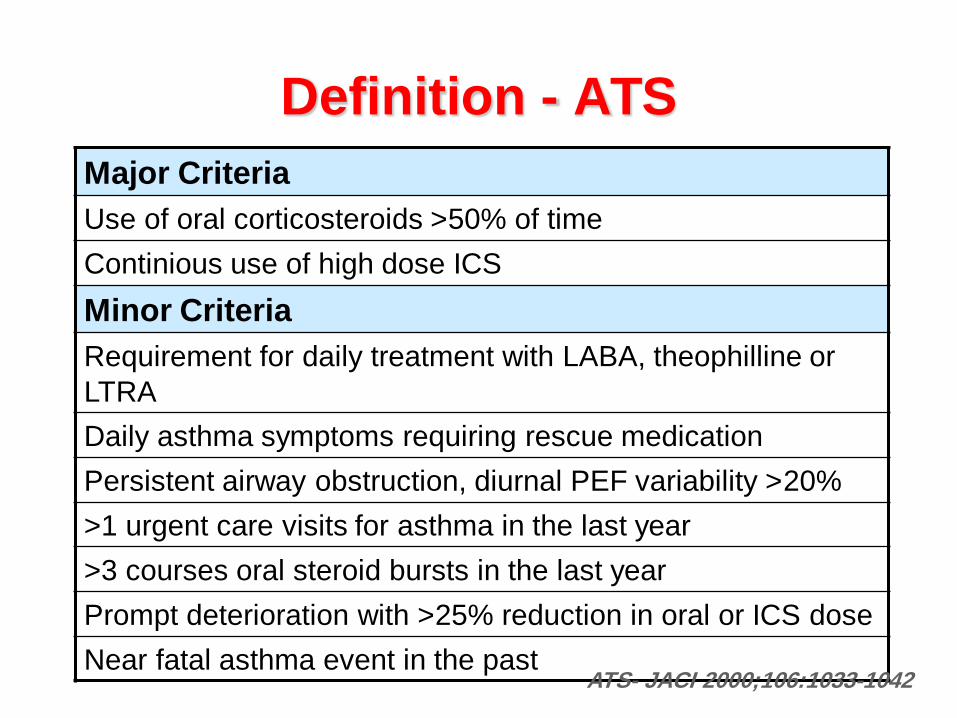
Definition - ATS
Major Criteria
Use of oral corticosteroids >50% of time
Continious use of high dose ICS
Minor Criteria
Requirement for daily treatment with LABA, theophilline or
LTRA
Daily asthma symptoms requiring rescue medication
Persistent airway obstruction, diurnal PEF variability >20%
>1 urgent care visits for asthma in the last year
>3 courses oral steroid bursts in the last year
Prompt deterioration with >25% reduction in oral or ICS dose
Near fatal asthma event in the past ATS- JACI 2000;106:1033-1042
• Definition
• Factors that could be preventing a
normal response to asthma medication
• Phenotypes
• Risk Factors
Severe - Difficult Asthma
Factors that could be preventing a
normal response to asthma
medication
• Incorrect diagnosis
• Continuing exposure to sensitising
agents
• Unrecognised aggravating
comorbidities
• Non-compliance with therapy
Incorrect Diagnosis -
Alternative Diagnoses
• COPD
• Congestive heart failure
• Central airway obstruction
– Foreign body, tumour, sarcoidosis, tracheobronchomalacia
• Cystic fibrosis
• Recurrent pulmonary embolism
• Obstructive bronchiolitis
• Recurrent aspiration
• Vocal cord disfunction
• Allergic bronchopulmonary aspergillosis
• Churg-Strauss syndrome
Bel EH. Breathe 2006; 3:2; 129-139
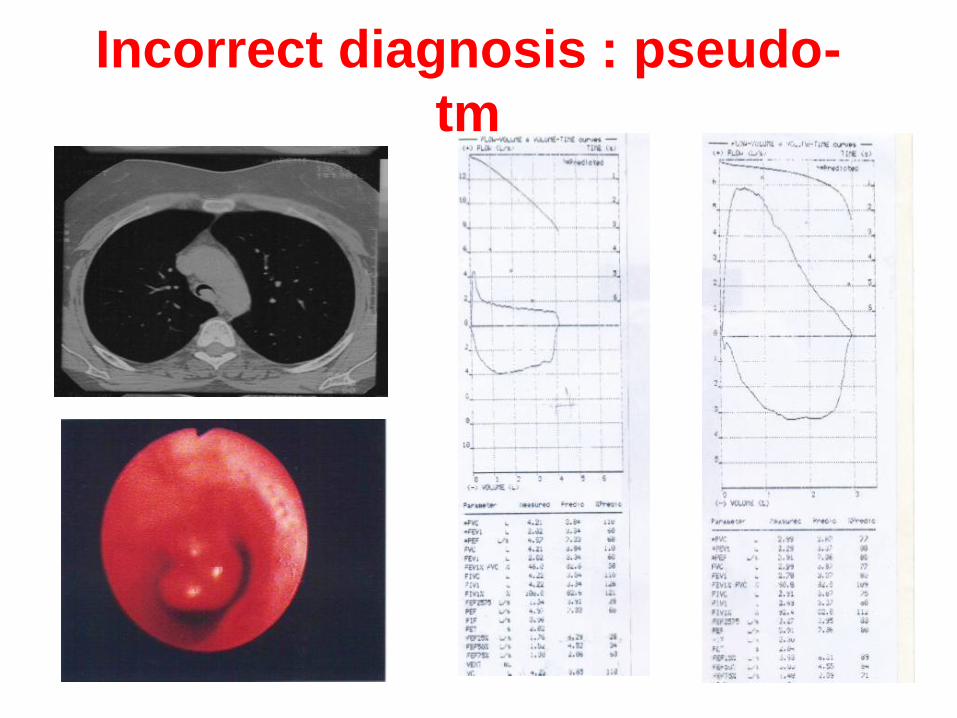
Incorrect diagnosis : pseudo-
tm
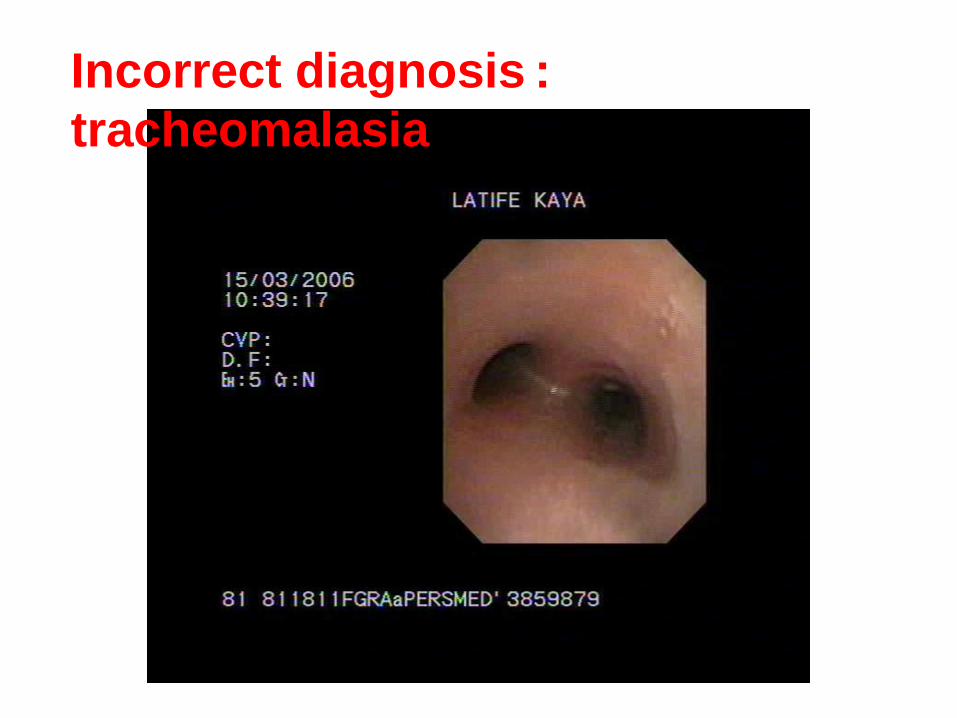
Incorrect diagnosis :
tracheomalasia
Strategy for the diagnosis-1
• History of asthma development
(age of onset, atopy, response to treatment, smoking)
• Severity of disease
(exacerbations, hospitalisations, ICU admissions)
• Exogenous aggravating factors
(allergens, occupationnal agents, drugs, foods..)
• Endogenous aggrating factors
(Rhinosinusitis, GER, OSA, influence of menstruation, psychiatric disease..)
• Miscellaneous
(adherence, advers effect, psychosocial circumstances)
• Physical examination (specific points of attention)
(Body mass index, Nasal polypes, cardiac failure, adverse effects of treatment)

Strategy for the diagnosis:
Laboratory tests
• Peripheral blood
(ESR, blood count, tIgE, sIgE, T3, T4, TSH)
• Lung function
(spirometry, flow-volume, PEF variability, challenge tests, arterial blood gases)
• Radiology
(chest radiography, thorax CT or HRCT, sinus CT scans)
• Additional tests for comorbidities and alternative diagnoses
(nasal endoscopy, oesophageal pH or PPI, polysomnography, broncoscopy, D-dimer, ANCA, IgG againts aspergllus fumigatus….)
Bel EH. Breathe 2006; 3:2; 129-139
Continuing exposure to
sensitising agents
• Allergen exposure at
home
• Allergen or
occupationnal exposure
at work
• Drugs
• Dietary factors
- metabisulphite, salicylate,
food allergens
• Smoking
Bel EH. Breathe 2006; 3:2; 129-139
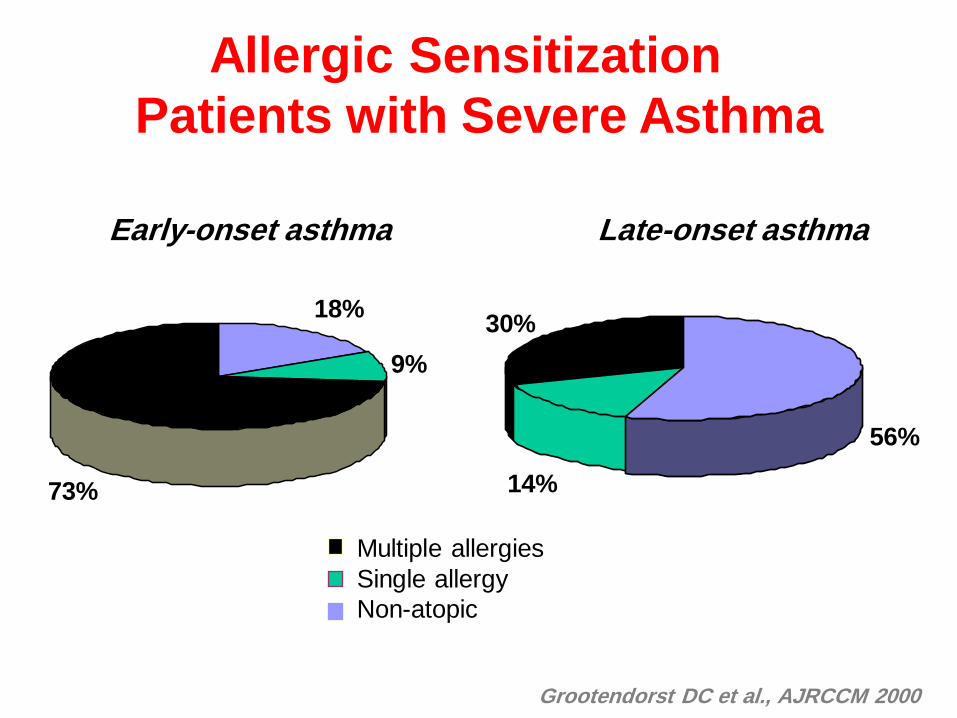
18%
73%
9%
56%
14%
30%
Allergic Sensitization
Patients with Severe Asthma
Grootendorst DC et al., AJRCCM 2000
Multiple allergies
Single allergy
Non-atopic
Early-onset asthma Late-onset asthma
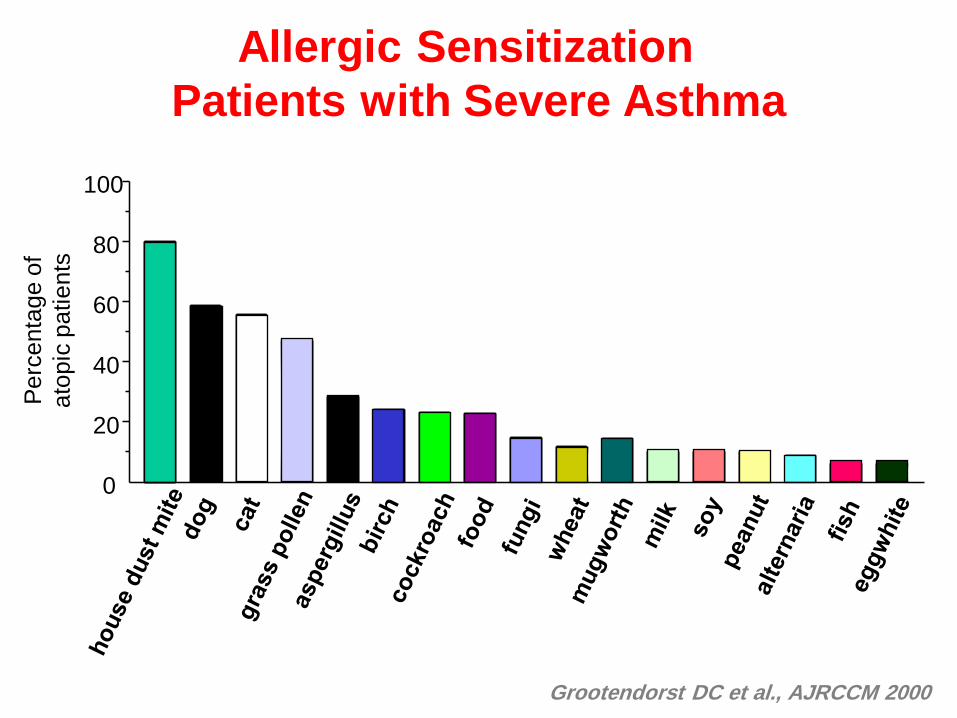
Allergic Sensitization
Patients with Severe Asthma
Grootendorst DC et al., AJRCCM 2000
0
20
40
60
80
100
Pe
rce
nta
ge
of
ato
pic
pa
tie
nts
• ß-Blockers
Exposure to sensitizing drugs
• Aspirin and NSAIDS
• ACE inhibitors
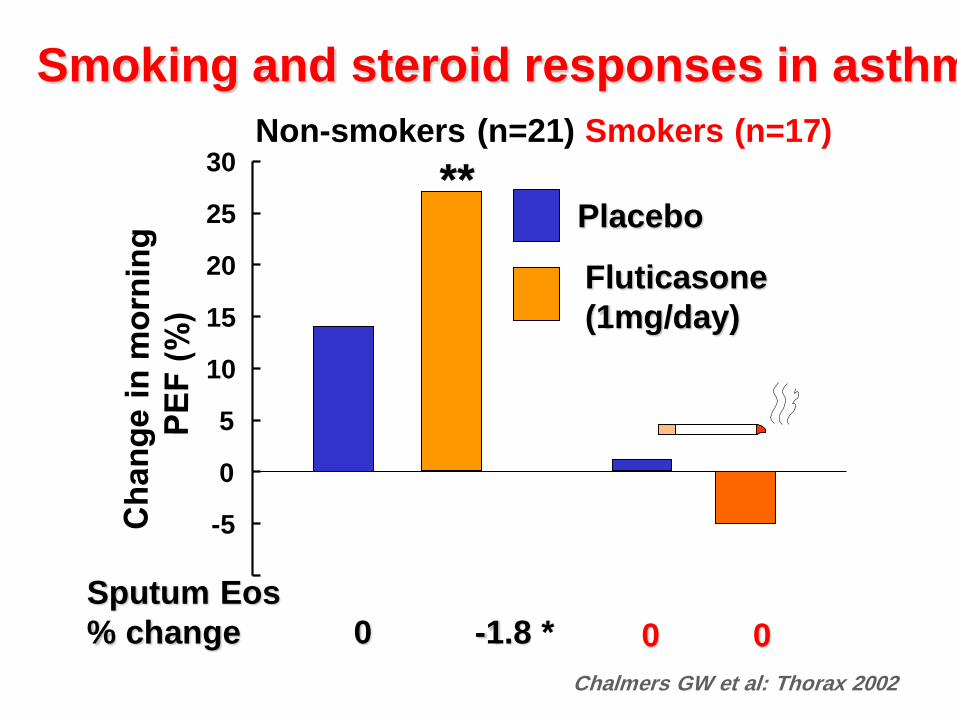
-5
0
5
10
15
20
25
30
Placebo
Fluticasone
(1mg/day)
Non-smokers (n=21)
Sputum Eos
% change 0 -1.8 *
**
Chalmers GW et al: Thorax 2002
Smoking and steroid responses in asthma
Smokers (n=17)
0 0
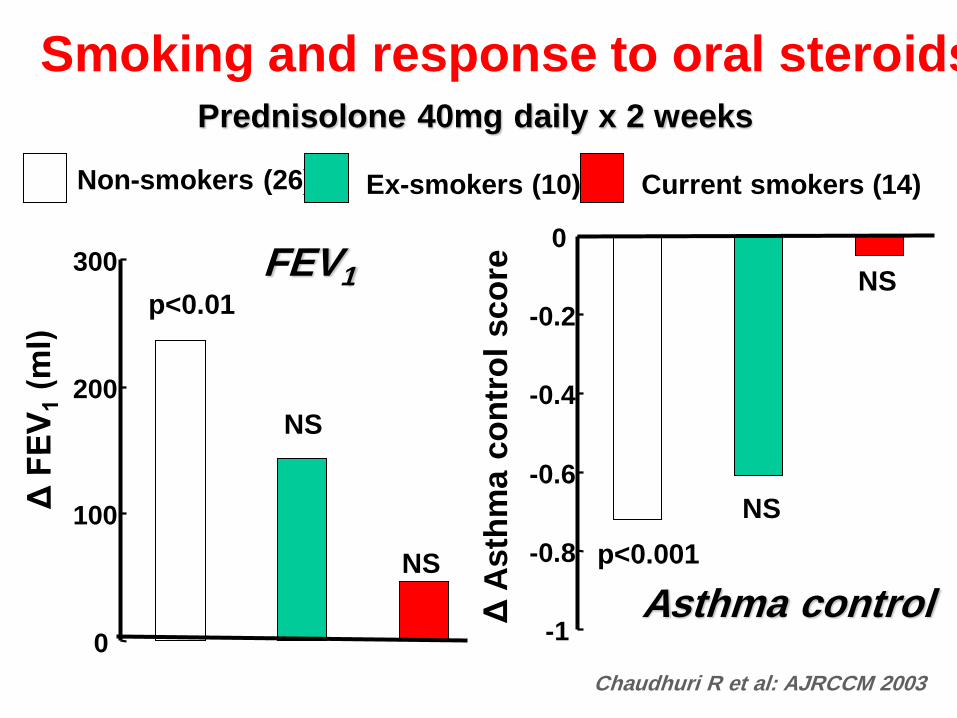
Smoking and response to oral steroids
Non-smokers (26) Ex-smokers (10) Current smokers (14)
0
100
200
300
p<0.01
NS
NS
Chaudhuri R et al: AJRCCM 2003
Prednisolone 40mg daily x 2 weeks
FEV1
-1
-0.8
-0.6
-0.4
-0.2
0
Δ A
sth
ma c
on
tro
l sco
re
NS
NS
p<0.001
Asthma control
Unrecognised aggravating
comorbidities
• Chronic rhinosinusitis
• Recurrent respiratory tract infections
• Gastro-oesophageal reflux
• Obstructive sleep apnea
• Psychological dysfunctioning
• Obesity
• Systemic diseases (thyrotoxicosis…)
Bel EH. Breathe 2006; 3:2; 129-139
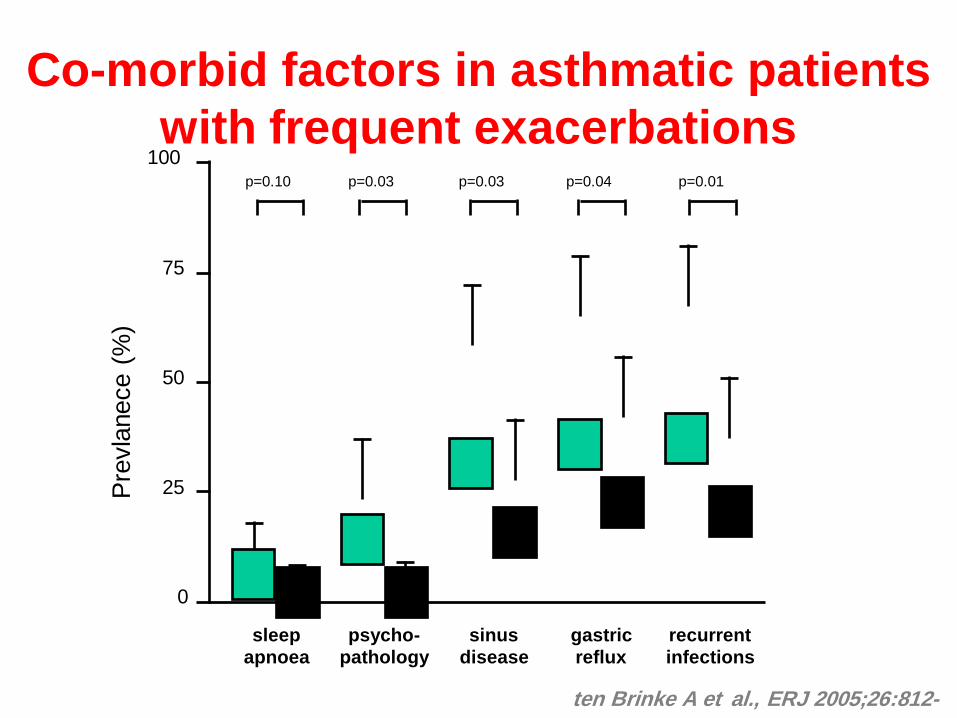
Co-morbid factors in asthmatic patients
with frequent exacerbations
sleep
apnoea
psycho-
pathology
sinus
disease
gastric
reflux
recurrent
infections
0
25
50
75
100
Pre
vla
nece (
%)
p=0.04 p=0.01 p=0.03 p=0.03 p=0.10
ten Brinke A et al., ERJ 2005;26:812-
8.
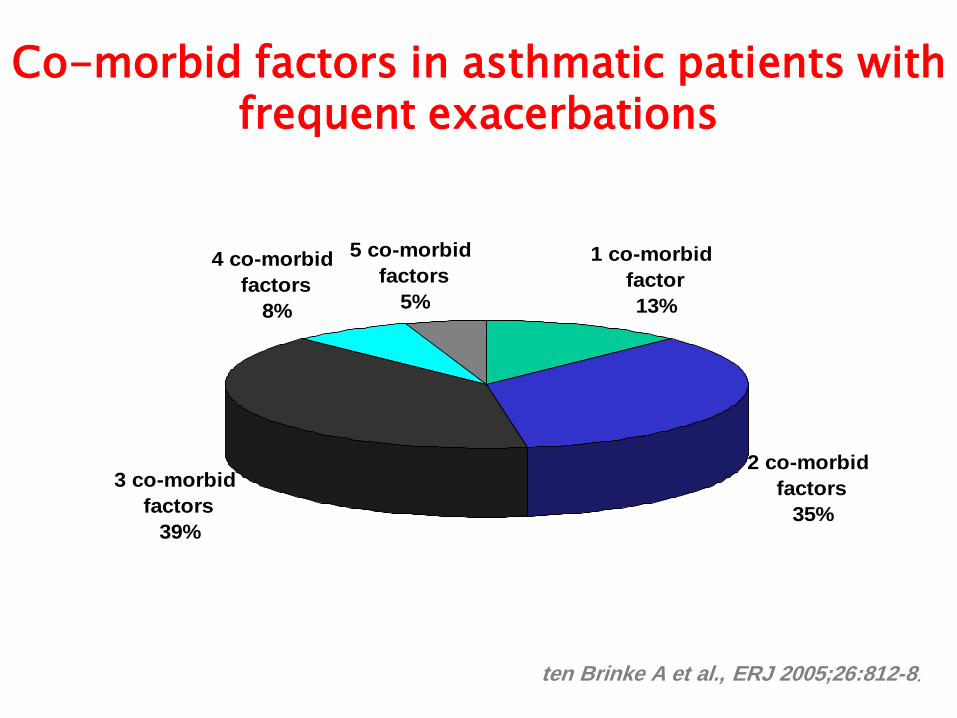
Co-morbid factors in asthmatic patients with frequent exacerbations
1 co-morbid
factor
13%
2 co-morbid
factors
35%
3 co-morbid
factors
39%
4 co-morbid
factors
8%
5 co-morbid
factors
5%
ten Brinke A et al., ERJ 2005;26:812-8.
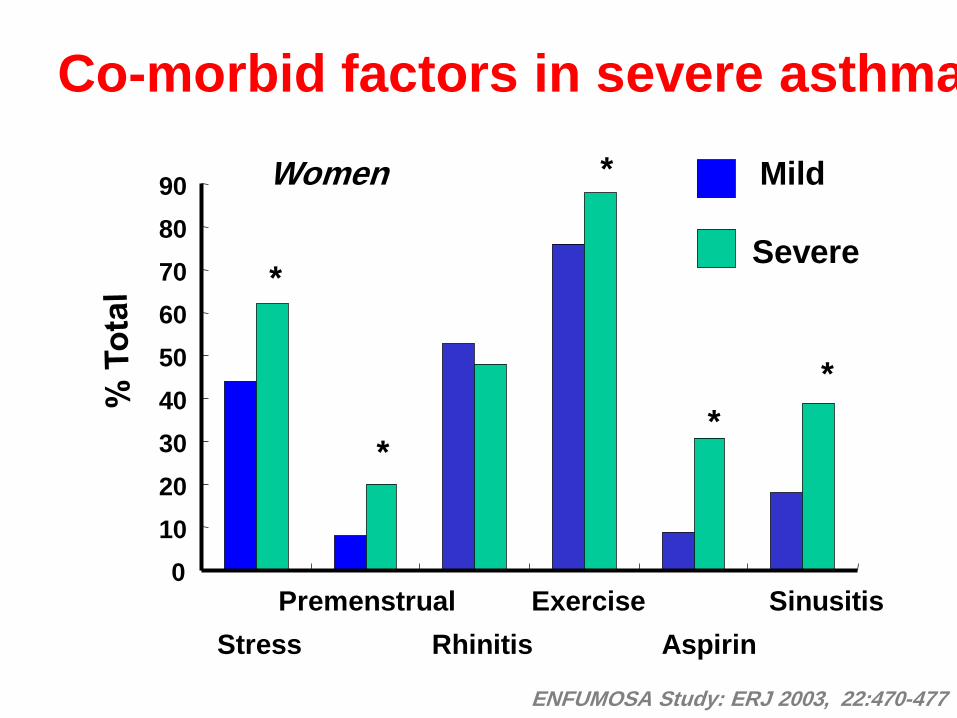
0
10
20
30
40
50
60
70
80
90
Premenstrual Exercise
Aspirin
Sinusitis
Rhinitis Stress
Mild
Severe *
*
*
*
*
Women
ENFUMOSA Study: ERJ 2003, 22:470-477
Co-morbid factors in severe asthma
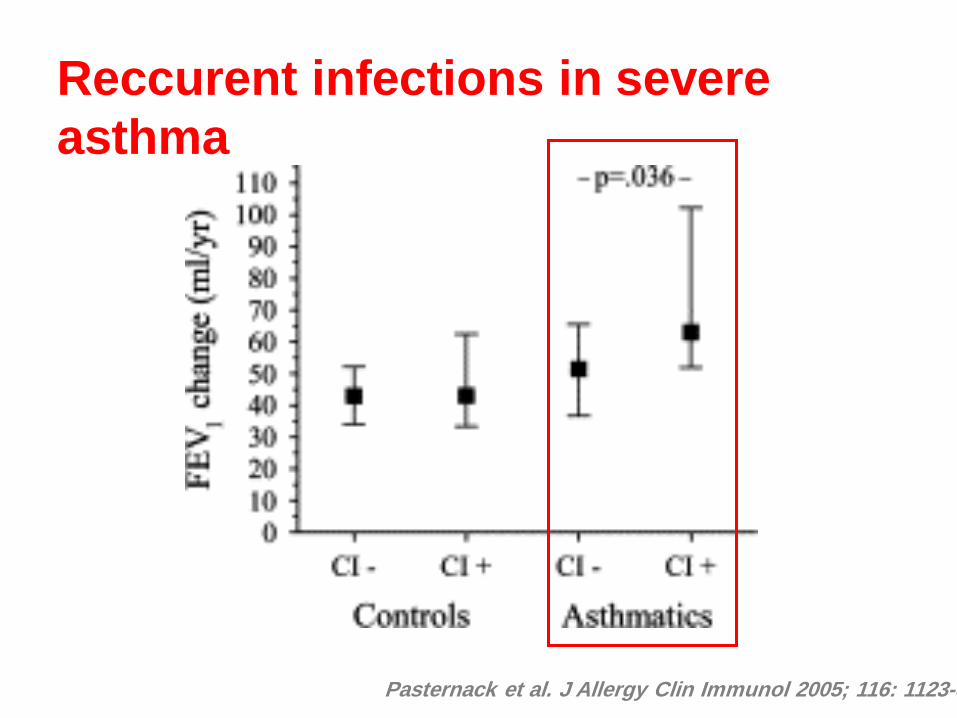
Pasternack et al. J Allergy Clin Immunol 2005; 116: 1123-8
Reccurent infections in severe
asthma
Pasternack et al. J Allergy Clin Immunol 2005; 116: 1123-8
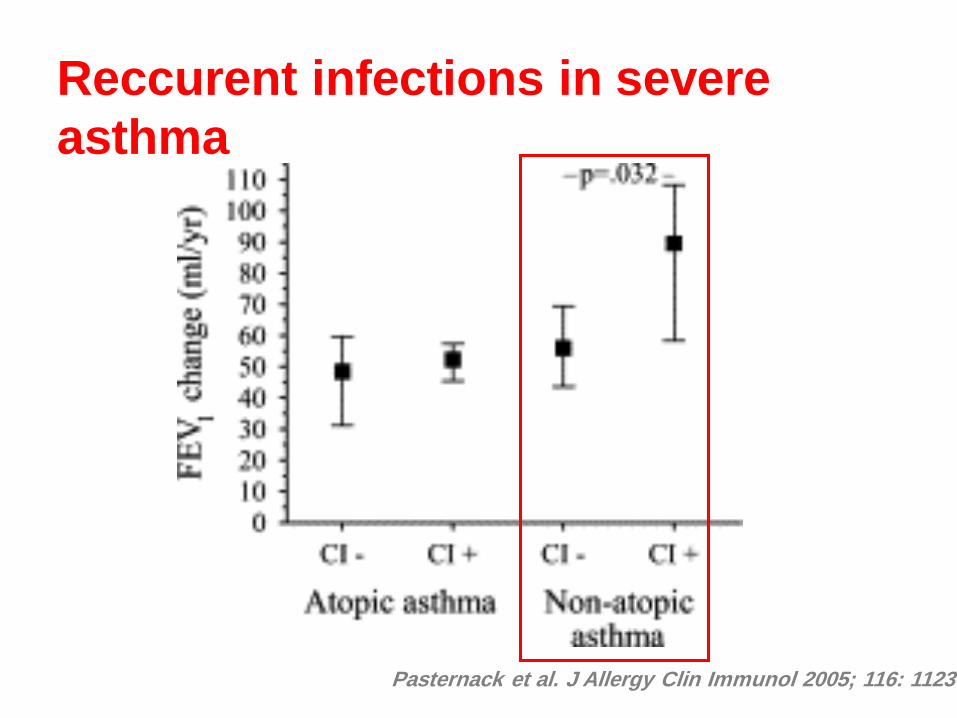
Reccurent infections in severe
asthma
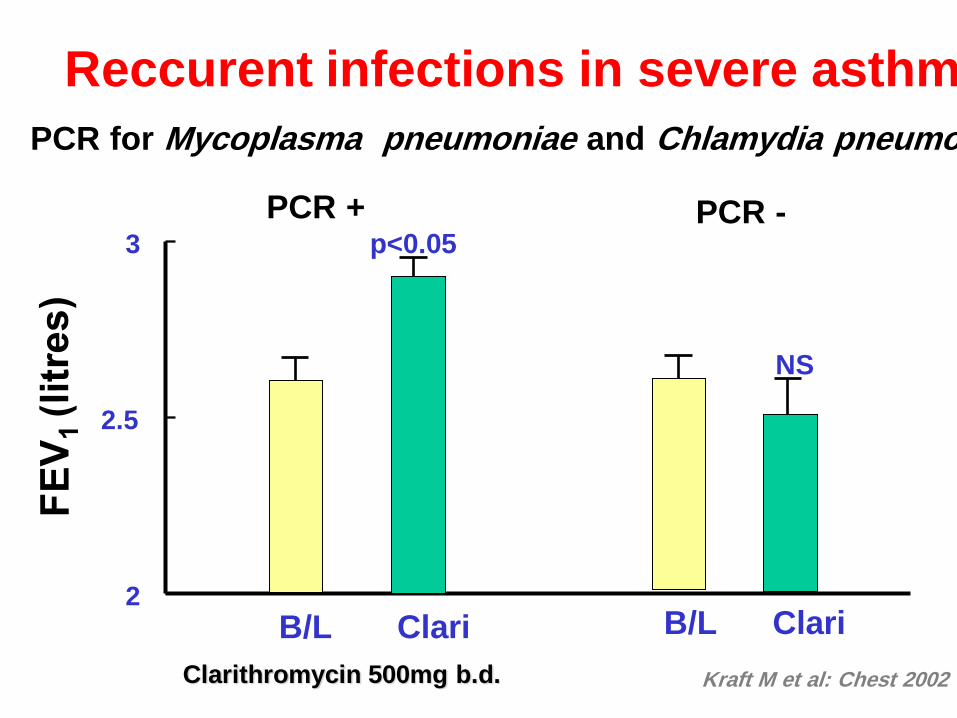
Reccurent infections in severe asthma
Kraft M et al: Chest 2002
2
2.5
3 p<0.05
B/L Clari
PCR +
NS
B/L Clari
PCR -
PCR for Mycoplasma pneumoniae and Chlamydia pneumoniae
Clarithromycin 500mg b.d.

Non- compliance with therapy
• Psychological problembs
• Missed appointments
• Complexity of treatement
• Lack of insight into illness
• Inhalation technique
Bel EH. Breathe 2006; 3:2; 129-139
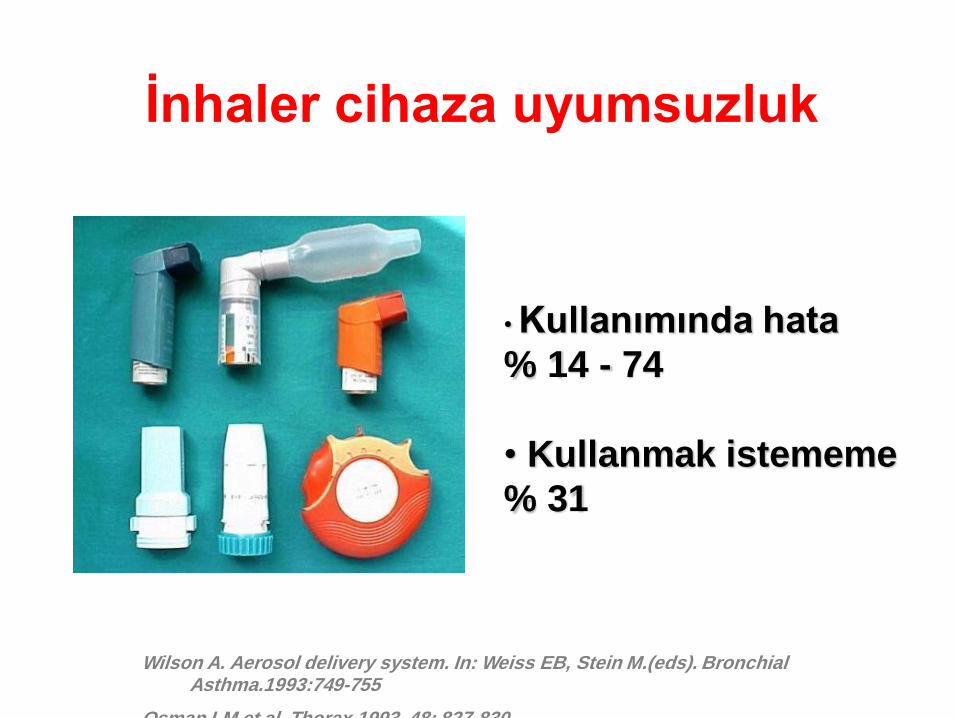
İnhaler cihaza uyumsuzluk
• Kullanımında hata
% 14 - 74
• Kullanmak istememe
% 31
Wilson A. Aerosol delivery system. In: Weiss EB, Stein M.(eds). Bronchial Asthma.1993:749-755
Osman LM et al. Thorax 1993, 48: 827-830
• Definition
• Factors that could be preventing a
normal response to asthma
medication
• Phenotypes
• Risk Factors
Severe - Difficult Asthma
Difficult asthma phenotypes
• Unstable asthma (Brittle, Nocturnal, Premenstrual)
• Poor response to treatment (Steroid-dependent asthma, Steroid-resistant asthma)
• “Fixed” asthma
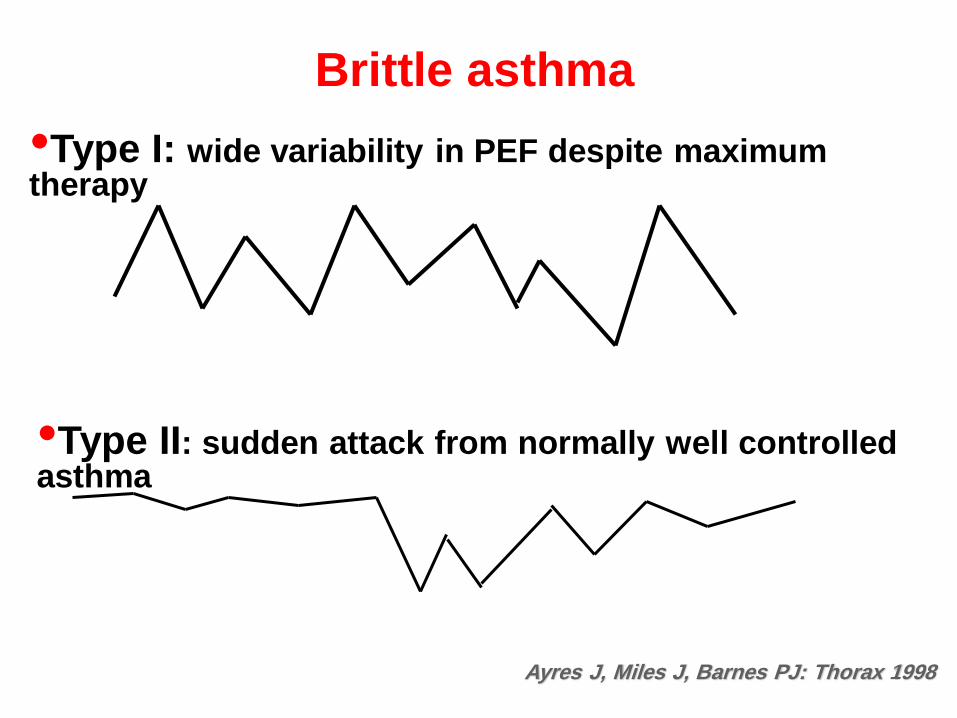
Brittle asthma
•Type I: wide variability in PEF despite maximum therapy
•Type II: sudden attack from normally well controlled asthma
Ayres J, Miles J, Barnes PJ: Thorax 1998
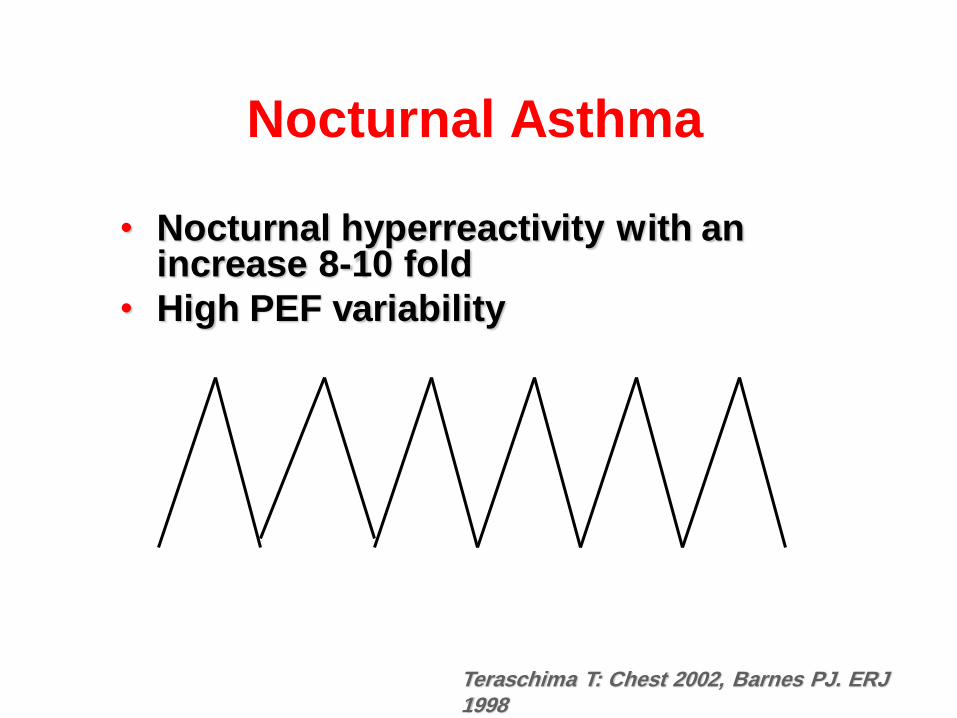
Nocturnal Asthma
• Nocturnal hyperreactivity with an increase 8-10 fold
• High PEF variability
Teraschima T: Chest 2002, Barnes PJ. ERJ 1998
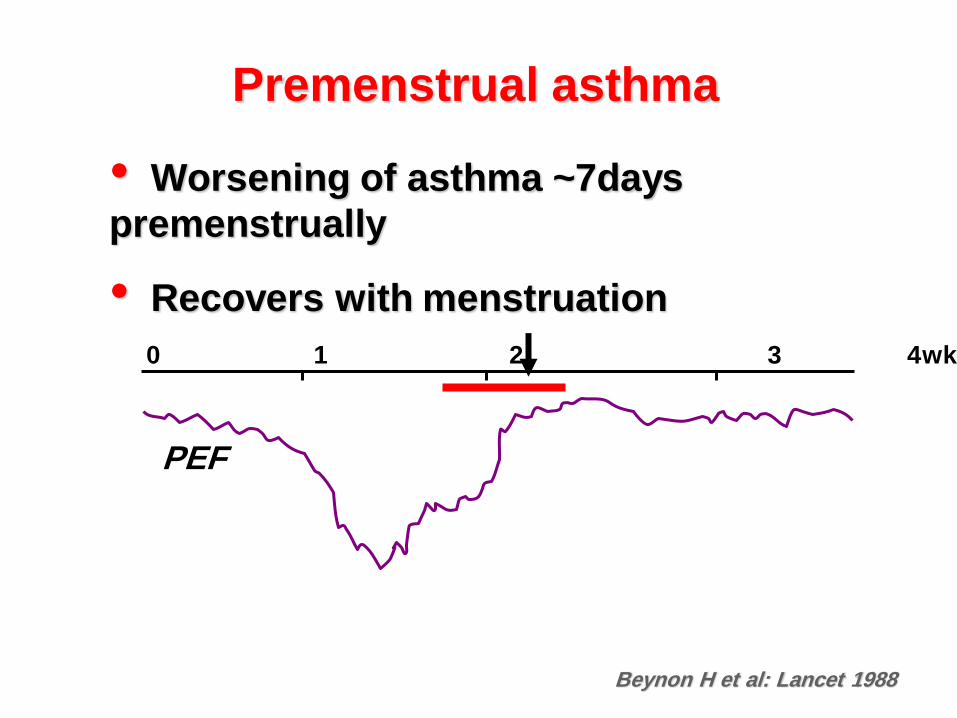
Premenstrual asthma
• Worsening of asthma ~7days
premenstrually
• Recovers with menstruation
0 1 2 3 4wk
PEF
Beynon H et al: Lancet 1988
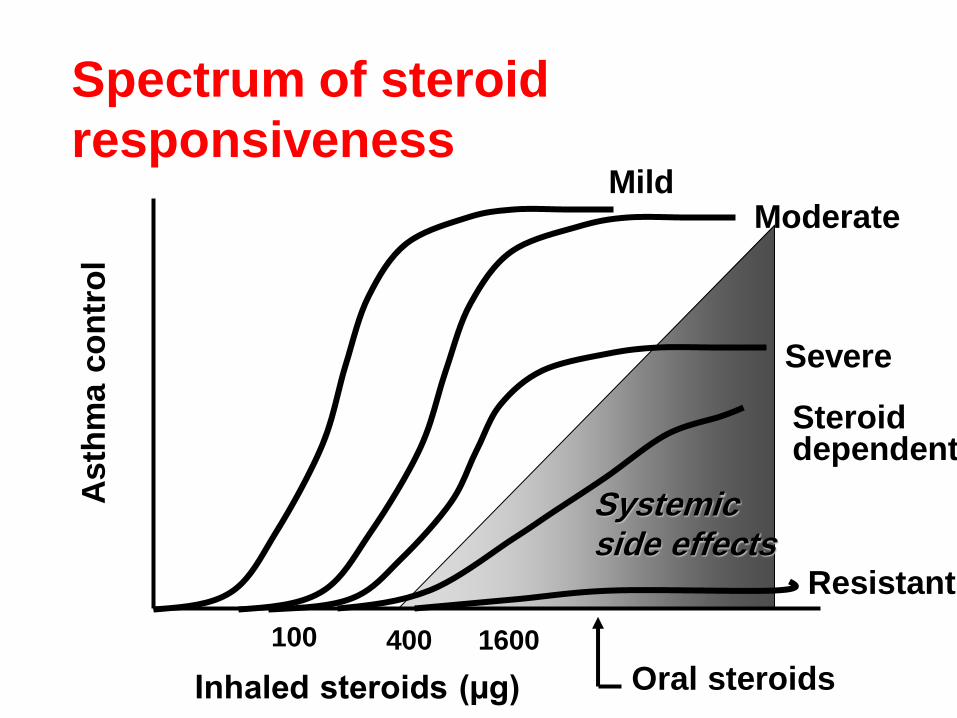
Systemic side effects
Mild Moderate
Severe
Inhaled steroids (µg)
100 400 1600
Resistant
Steroid dependent
Oral steroids
Asth
ma c
on
tro
l Spectrum of steroid
responsiveness
• Poor adherence
• Wrong diagnosis
• Dose too low
• Increased metabolism
(e.g. carbamazepine, rifampicin)
• Relative resistance / Complete
resistance
Poor response to corticosteroids
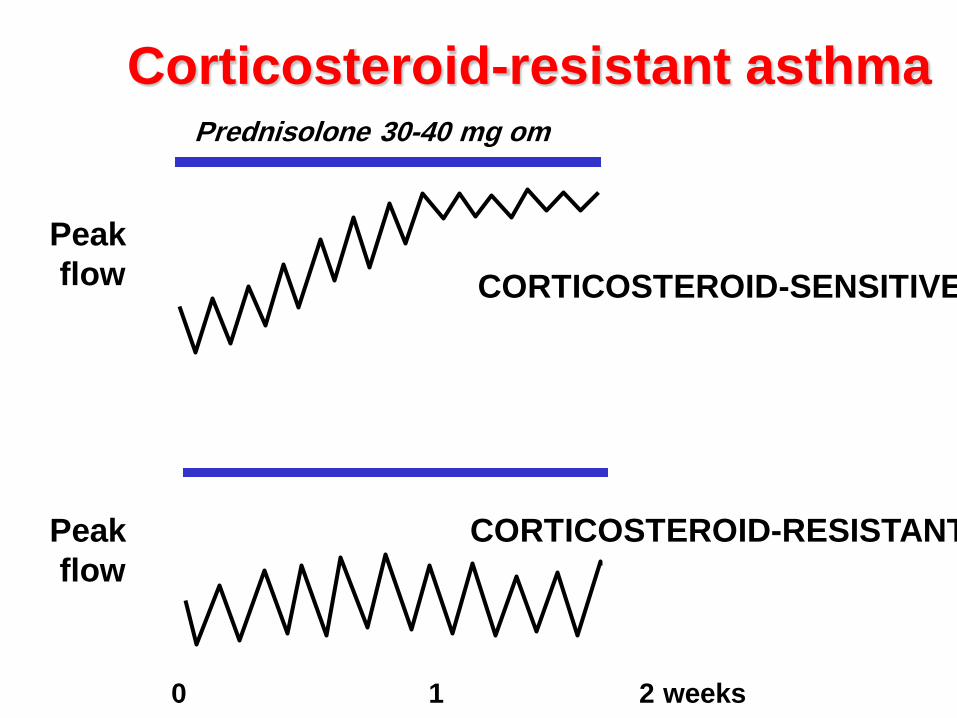
0 1 2 weeks
Peak
flow CORTICOSTEROID-SENSITIVE
Peak
flow
0 1 2 weeks
CORTICOSTEROID-RESISTANT
Prednisolone 30-40 mg om
Corticosteroid-resistant asthma
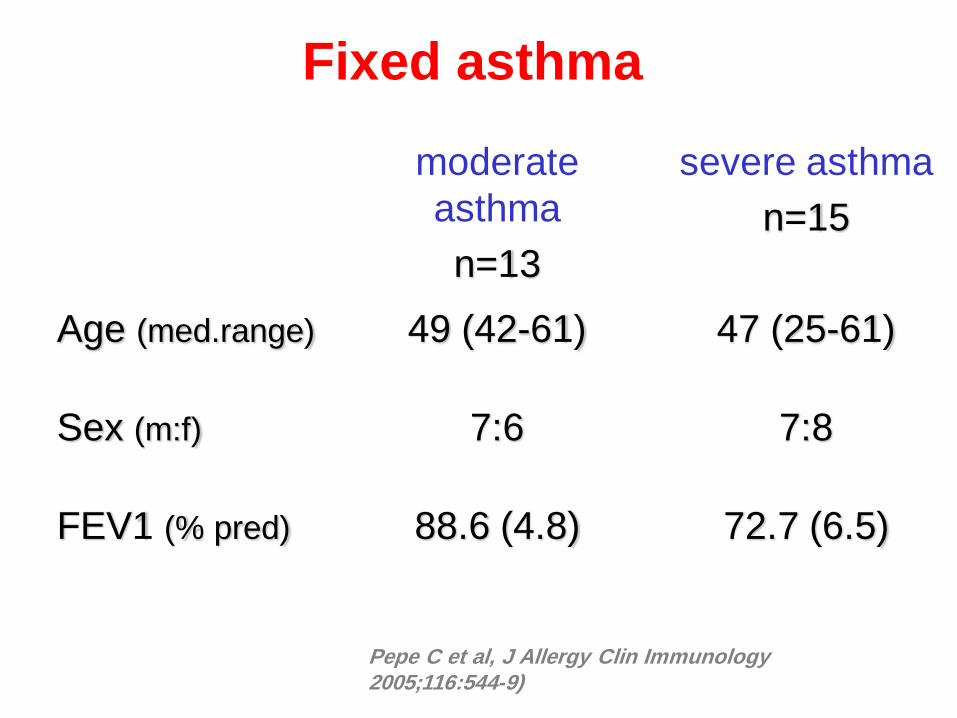
moderate
asthma
n=13
severe asthma
n=15
Age (med.range) 49 (42-61) 47 (25-61)
Sex (m:f) 7:6 7:8
FEV1 (% pred) 88.6 (4.8) 72.7 (6.5)
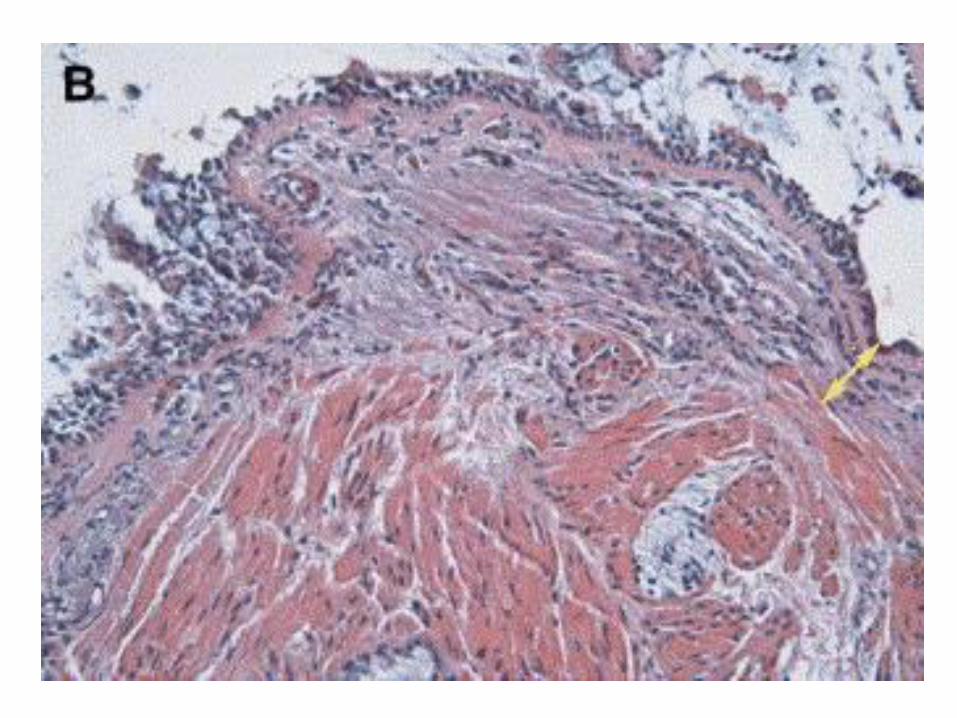
Pepe C et al, J Allergy Clin Immunology 2005;116:544-9)
Fixed asthma
Pepe C et al, J Allergy Clin Immunology 2005;116:544-9)
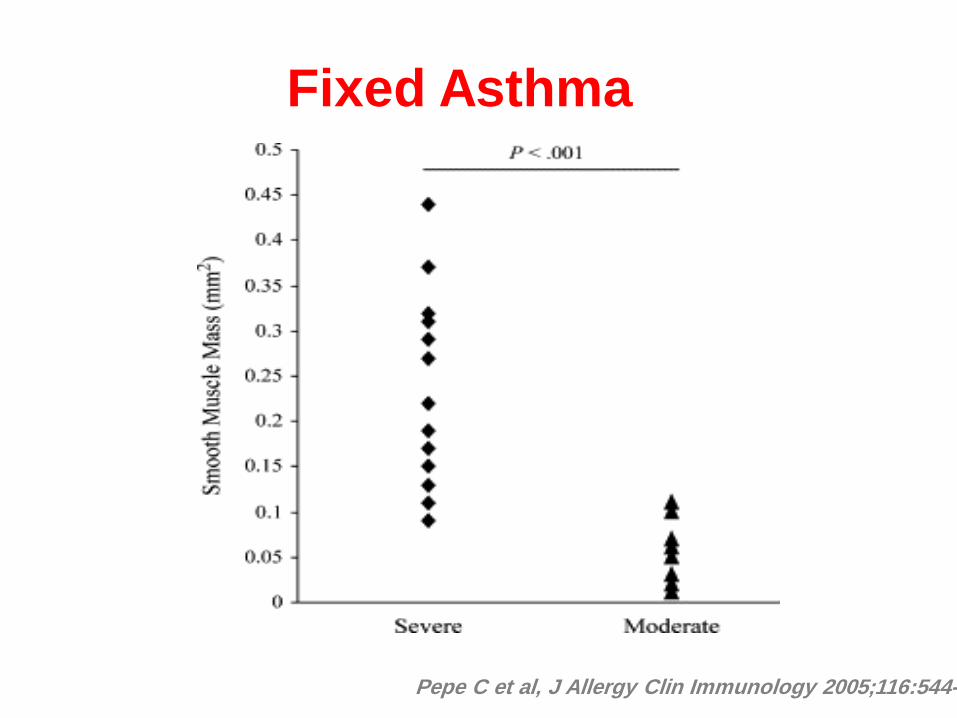
Fixed Asthma
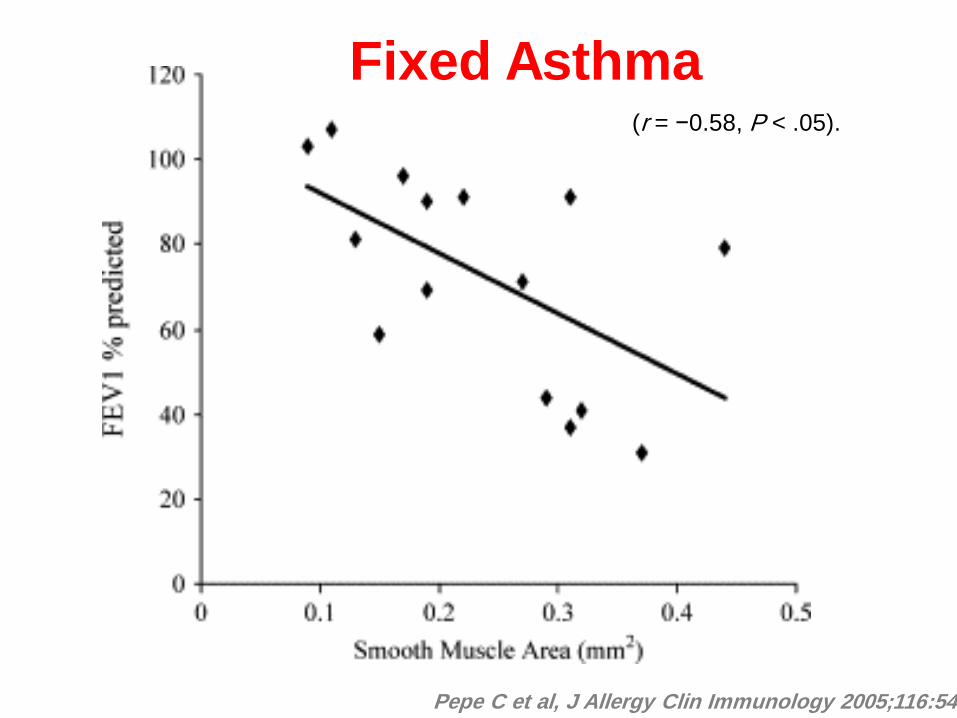
Pepe C et al, J Allergy Clin Immunology 2005;116:544-9)
(r = −0.58, P < .05).
Fixed Asthma
• Definition
• Factors that could be preventing a
normal response to asthma
medication
• Phenotypes
• Risk Factors
Severe - Difficult Asthma
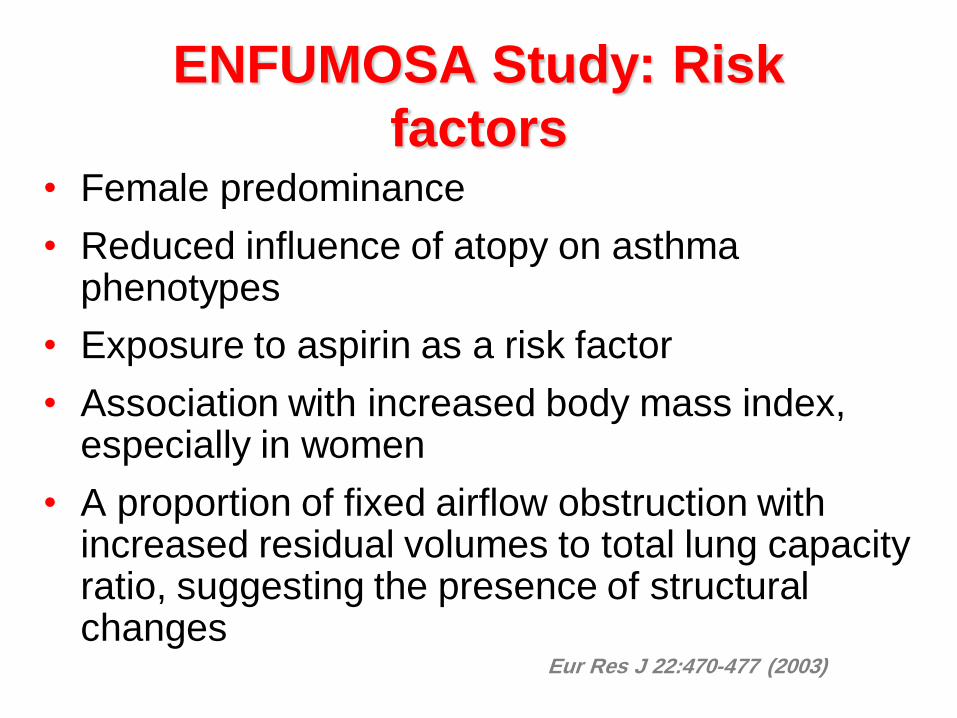
ENFUMOSA Study: Risk
factors • Female predominance
• Reduced influence of atopy on asthma phenotypes
• Exposure to aspirin as a risk factor
• Association with increased body mass index, especially in women
• A proportion of fixed airflow obstruction with increased residual volumes to total lung capacity ratio, suggesting the presence of structural changes
Eur Res J 22:470-477 (2003)
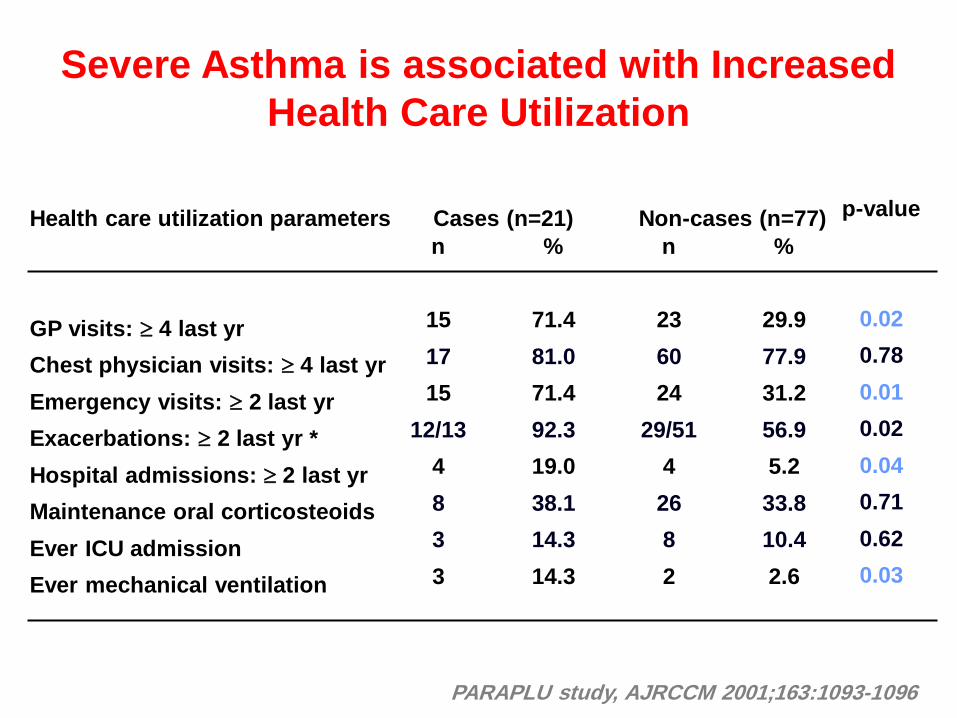
PARAPLU study, AJRCCM 2001;163:1093-1096
Severe Asthma is associated with Increased
Health Care Utilization
Health care utilization parameters
GP visits: 4 last yr
Chest physician visits: 4 last yr
Emergency visits: 2 last yr
Exacerbations: 2 last yr *
Hospital admissions: 2 last yr
Maintenance oral corticosteoids
Ever ICU admission
Ever mechanical ventilation
n
15
17
15
12/13
4
8
3
3
%
71.4
81.0
71.4
92.3
19.0
38.1
14.3
14.3
n
23
60
24
29/51
4
26
8
2
%
29.9
77.9
31.2
56.9
5.2
33.8
10.4
2.6
p-value
0.02
0.78
0.01
0.02
0.04
0.71
0.62
0.03
Cases (n=21) Non-cases (n=77)
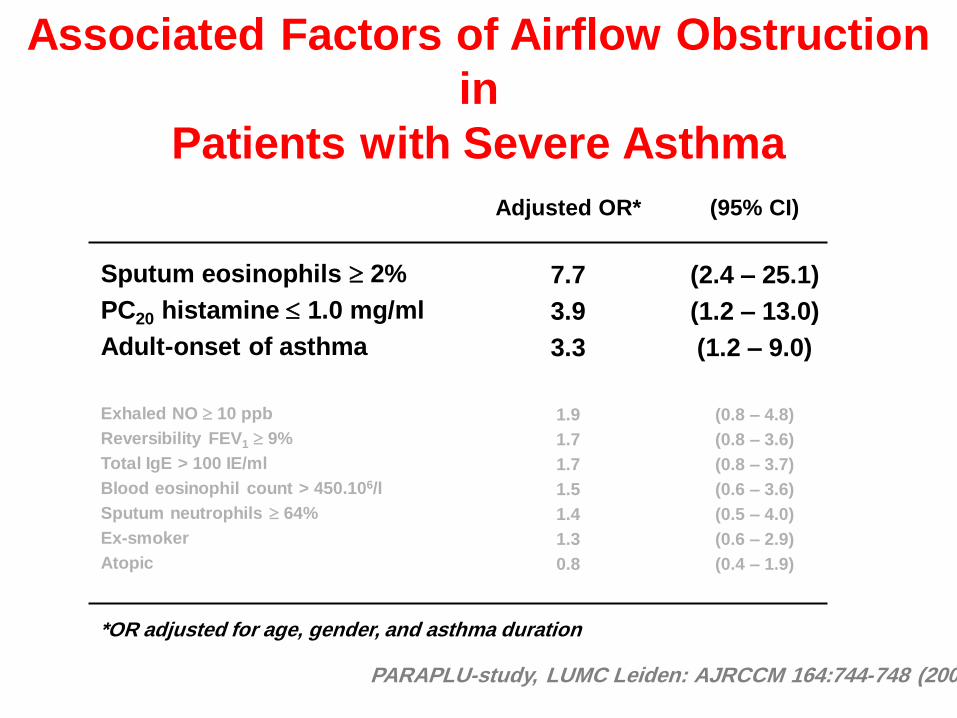
Associated Factors of Airflow Obstruction
in
Patients with Severe Asthma
Adjusted OR*
7.7
3.9
3.3
1.9
1.7
1.7
1.5
1.4
1.3
0.8
(95% CI)
(2.4 – 25.1)
(1.2 – 13.0)
(1.2 – 9.0)
(0.8 – 4.8)
(0.8 – 3.6)
(0.8 – 3.7)
(0.6 – 3.6)
(0.5 – 4.0)
(0.6 – 2.9)
(0.4 – 1.9)
Sputum eosinophils 2%
PC20 histamine 1.0 mg/ml
Adult-onset of asthma
Exhaled NO 10 ppb
Reversibility FEV1 9%
Total IgE > 100 IE/ml
Blood eosinophil count > 450.106/l
Sputum neutrophils 64%
Ex-smoker
Atopic
*OR adjusted for age, gender, and asthma duration
PARAPLU-study, LUMC Leiden: AJRCCM 164:744-748 (2001)
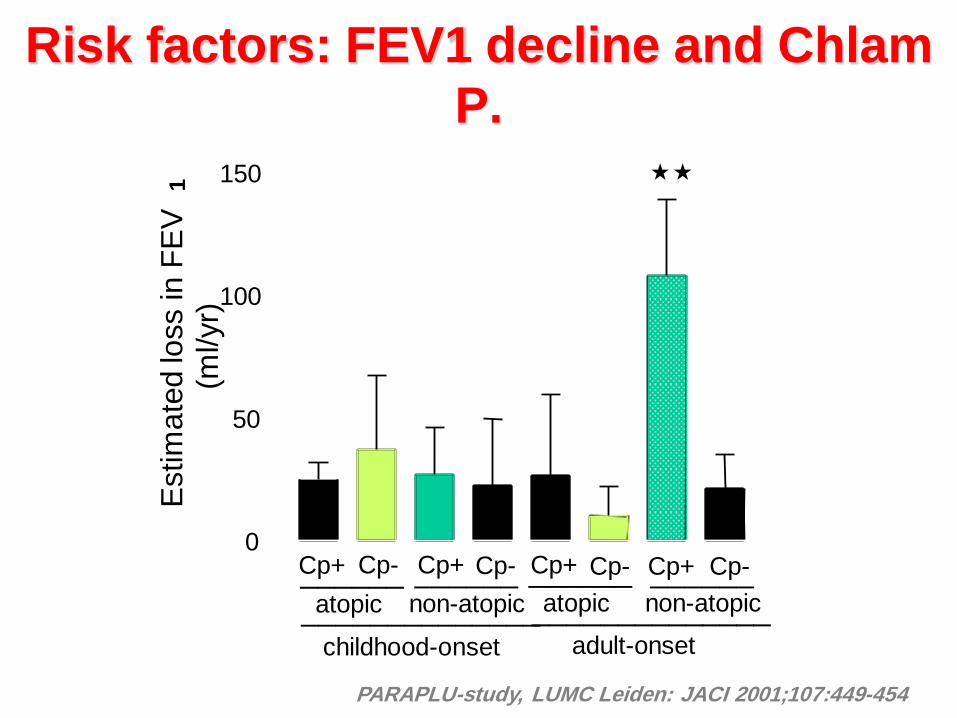
Risk factors: FEV1 decline and Chlam
P.
0
50
100
150
Cp+ Cp+ Cp- Cp- Cp+ Cp- Cp+ Cp-
atopic atopic non-atopic non-atopic ______ ______ ______ ______
______________ ______________ childhood-onset adult-onset
Estim
ate
d lo
ss in
FE
V
1
(ml/yr)
PARAPLU-study, LUMC Leiden: JACI 2001;107:449-454
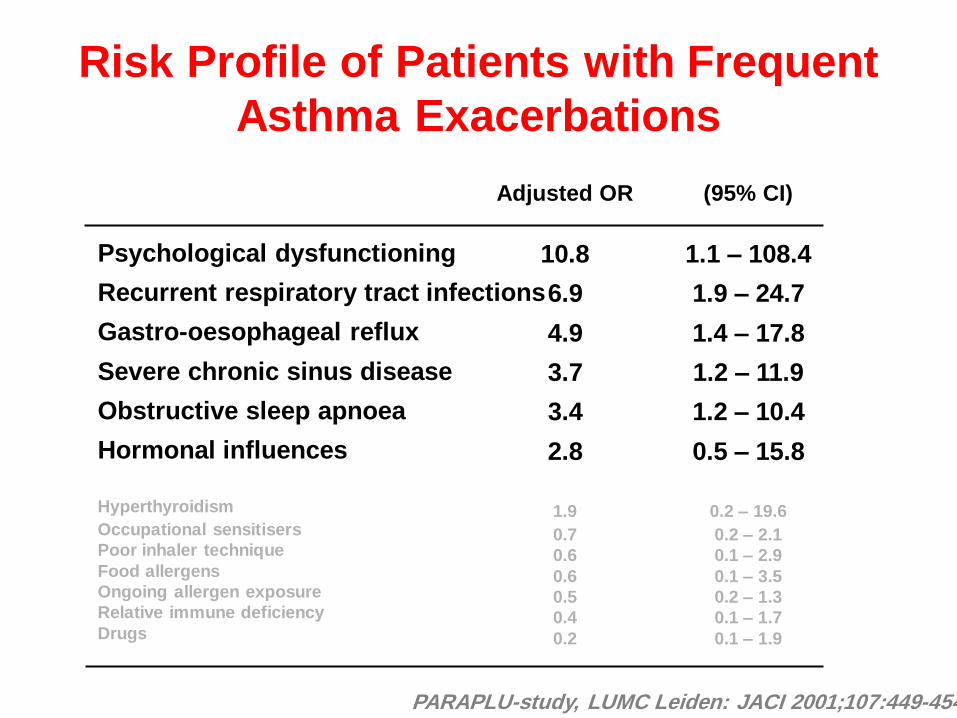
Risk Profile of Patients with Frequent
Asthma Exacerbations
Adjusted OR
10.8
6.9
4.9
3.7
3.4
2.8
1.9
0.7
0.6
0.6
0.5
0.4
0.2
(95% CI)
1.1 – 108.4
1.9 – 24.7
1.4 – 17.8
1.2 – 11.9
1.2 – 10.4
0.5 – 15.8
0.2 – 19.6
0.2 – 2.1
0.1 – 2.9
0.1 – 3.5
0.2 – 1.3
0.1 – 1.7
0.1 – 1.9
Psychological dysfunctioning
Recurrent respiratory tract infections
Gastro-oesophageal reflux
Severe chronic sinus disease
Obstructive sleep apnoea
Hormonal influences
Hyperthyroidism
Occupational sensitisers
Poor inhaler technique
Food allergens
Ongoing allergen exposure
Relative immune deficiency
Drugs
PARAPLU-study, LUMC Leiden: JACI 2001;107:449-454

154