Embed Size (px)
Citation preview
1
ARDS, Respiratory Failure
Dr. Manu Mohan K
Dept. of Pulmonary Medicine
ARDS
• Severe dyspnea of rapid onset
• Hypoxemia
• Diffuse pulmonary infiltrates
• Respiratory failure
2

Etiology
3Harrison’s Principles of Internal
Medicine 17th ed.
Clinical features
• Diagnostic criteria for ALI and ARDS• Oxygenation
ALI – PaO2/FiO2 < 300mm of Hg
ARDS - PaO2/FiO2 < 200mm of Hg• Onset
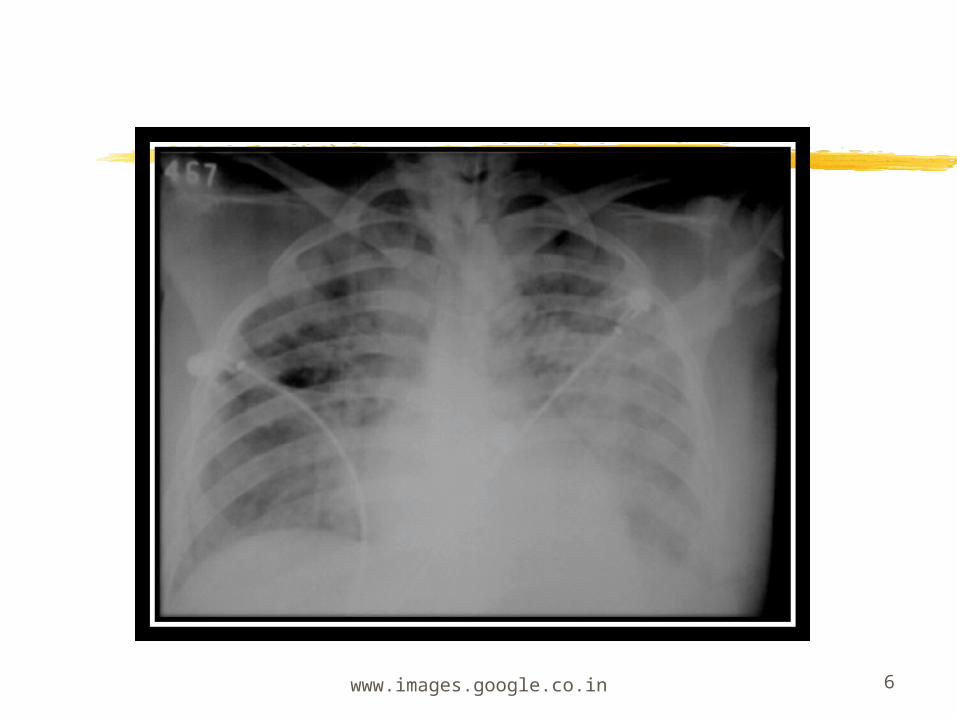
Acute• Chest radiograph
Bilateral alveolar or interstitial infiltrates
4Harrison’s Principles of Internal
Medicine 17th ed.
• Absence of left atrial hypertension
PCWP < 18 mm of Hg or no clinical evidence of increased left atrial pressure
Harrison’s Principles of Internal Medicine 17th ed. 5
www.images.google.co.in 6
http://radiology.rsna.org/content/213/2/545/F5.large.jpg 7
Clinical course and pathophysiology
• Exudative
• Proliferative
• Fibrotic
Harrison’s Principles of Internal Medicine 17th ed. 8
Exudative phase
• First 7 days
• Alveolar and interstitial edema
• Hyaline membrane whorls
• Atelectasis
• Decreased lung compliance
Harrison’s Principles of Internal Medicine 17th ed. 9
Proliferative Phase
• 7 to 21 days
• Early pulmonary fibrosis
• Proliferation of Type 2 pneumocytes
Harrison’s Principles of Internal Medicine 17th ed. 10
Fibrotic stage
• 3 to 4 weeks
• Extensive alveolar duct and interstitial fibrosis
• Emphysema and bullae
• Pulmonary hypertension
Harrison’s Principles of Internal Medicine 17th ed. 11
Treatment
• General
• Mechanical ventilation
Ventilator induced lung injury
Prevention of alveolar collapse
PEEP
Inverse ratio ventilation
Prone position ventilationHarrison’s Principles of Internal
Medicine 17th ed. 12
• Other strategies of mechanical ventilation
High frequency ventilation
Extracorporeal membrane oxygenation
Partial liquid ventilation
13
General support during ventilation
• Fluid management
Maintaining low left atrial filling pressure
• Glucocorticoids
• Other therapies
Surfactant replacement
Nitric oxide inhalation
14
Complications of Mechanical ventilation
• Pulmonary complications
• Barotrauma
• Nosocomial pneumonia
• Oxygen toxicity
• Tracheal stenosis
• Deconditioning of respiratory muscles
Harrison’s Principles of Internal Medicine 17th ed. 15
• Hypotension
• GI - Stress ulcer and mild cholestasis
16
Prognosis
• Mortality 41-65%
• >80 % deaths due to nonpulmonary complications
17
• Functional recovery
Recover maximum lung function in 6 months
18
Respiratory failure
19
20
Respiratory failure
• When lungs cannot fulfill their primary function of maintaining adequate gas exchange at rest, or during exercise
• This results in an inability to maintain normal blood gases, so that the Po2 (less than 60) is low with or without Hypercarbia (more than 50).
21
• Two types of respiratory failure
• Type I and Type II
• Type I - Hypoxemia without Hypercarbia
• Type II- Hypoxemia with Hypercarbia
• It can be acute or chronic
22
• Type I respiratory failure causes
• Chronic bronchitis and emphysema
• Pneumonia
• Pulmonary edema
• Pulmonary fibrosis
• Asthma
• Pneumothorax
• Pulmonary embolism
• Bronchiectasis
• Obesity
• ARDS
• Cyanotic heart disease
23
Type II Hypercarbic Respiratory failure causes
• COPD
• Asthma
• Drug overdose
• Poisoning
24
• Myasthenia Gravis• Polyneuropathy• Poliomyelitis• Sleep apnea syndrome• Pulmonary edema• ARDS• Tetanus• Foreign body
25
Mechanism
• Oxygenation failure and ventilatory failure
• Type I respiratory failure
Ventilation perfusion mismatch is marked
Control of ventilation is intact
So excess CO2 is exerted by normal areas of lung
26
27
• Type II
Ventilatory failure marked
PaCO2 rises due to alveolar hypoventilation, PaO2 falls.
Clinical features
• Clinical evidence of hypoxemia
• Central cyanosis best assessed by examining the oral mucous membrane.
• Not useful in anemia
28
29
• CNS effects- irritability impaired intellectual function and clouding of consciousness
• Progress to convulsion, coma and death
• Persistent hypoxemia can lead to secondary polycythemia
Clinical evidence of hypercapnia
• CNS effects- irritability, confusion, somnolence and coma, tremor, myoclonic jerks, asterixis, even seizures, headache, papilledema.
• Warm flushed skin with bounding pulse.
• Tachycardia and sweating
30
31
• Gastric dilatation, paralytic ileus
• Head ache on waking up common in chronic hypercapnia due to progressive increase in CO2retention during sleep.
32
DIAGNOSIS
• ABG• It is important to measure arterial pH and
assess degree on compensation. • In acute respiratory failure 10mm of Hg
increase in CO2 increases HCO3 by 1meq/L pH increase by 0.08 units. In Chronic 10mm Hg increase in CO2 increase pH by 0.03 and HCO3 by 3.5meq/L
33
Management
• Type I
• Treatment of primary cause
• Correction of arterial hypoxemia highest priority
• The goal should be to increase saturation of oxygen to at least 85-90% without risk of oxygen toxicity.
34
• High Fi02 for short period can be used. The use of PEEP, change in position, sedation and paralysis may help in lowering Fi02
• Fever, agitation, overfeeding, vigorous respiratory activity and sepsis increases the oxygen demand.
General indication of ventilation
• Inadequate oxygenation despite an increasing Fi02
• Increased PaCO2 associated with decreased mental status or increasing fatigue.
• Failure to control secretions
35
Methods
• Non invasive mechanical ventilation
• Mechanical ventilation
36
Mechanical ventilation• Indications
• PaO2 less than 60 mm Hg despite FiO2 > 0.6 with hypercapnia
• Rapid increase in CO2 causing uncompensated
• Respiratory acidosis
• Tachypnea > 35 breaths per minute
• Clinical judgment on impending exhaustion of the patient
37
Complications
• Barotrauma
• GIT bleeding
• Nosocomial Pneumonia
38
• LTOT - long term oxygen therapy
39

40