Embed Size (px)
Citation preview

Antiaggregazione per la prevenzione
secondaria dopo ictus ischemico:
mono o doppia?
Plinio Fabiani
Portoferraio
sabato 11 APRILE 2015
HOTEL VALDARNO - MONTEVARCHI (AR)
V° WORKSHOP DI
MEDICINA VASCOLARE
Precision Medicine
Precision Medicine
Tailored therapy
Sofisticata selezione per il trattamento endovascolare
nell’ictus acuto da acclusione prossimale del circolo
anteriore
(Escape, Extend-IA, SWIFT-Prime, Mr Clean)
Ruolo della doppia antiaggregazione nella
prevenzione secondaria dell’ictus
CARDIOEMBOLICONON
CARDIOEMBOLICO
www.escardio.org/guidelines
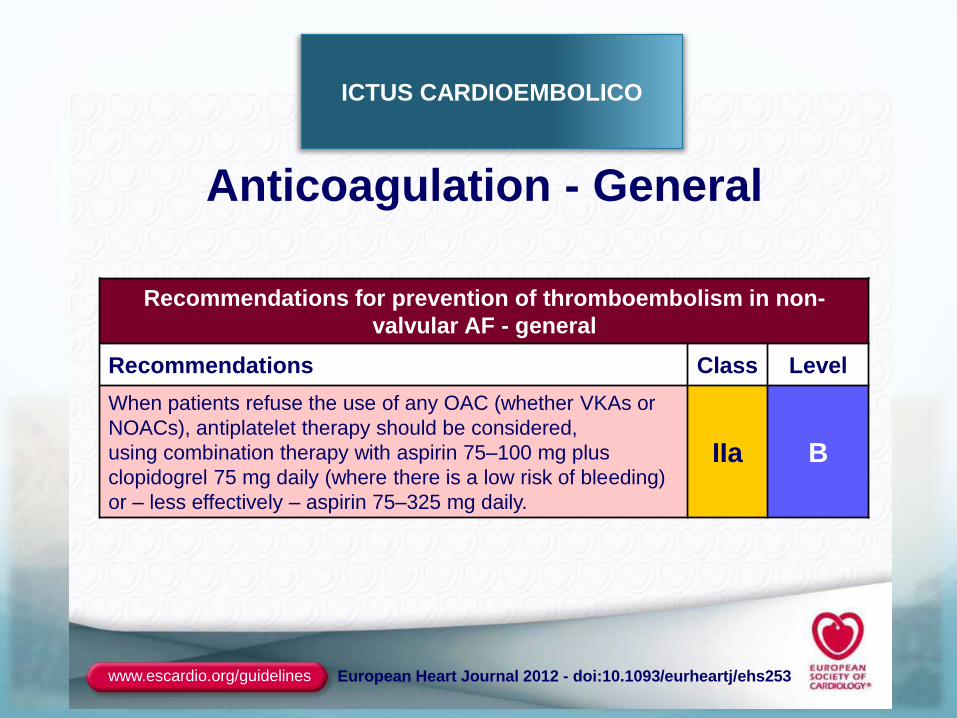
Anticoagulation - General
Recommendations for prevention of thromboembolism in non-
valvular AF - general
Recommendations Class Level
When patients refuse the use of any OAC (whether VKAs or
NOACs), antiplatelet therapy should be considered,
using combination therapy with aspirin 75–100 mg plus
clopidogrel 75 mg daily (where there is a low risk of bleeding)
or – less effectively – aspirin 75–325 mg daily.
IIa B
European Heart Journal 2012 - doi:10.1093/eurheartj/ehs253
ICTUS CARDIOEMBOLICO
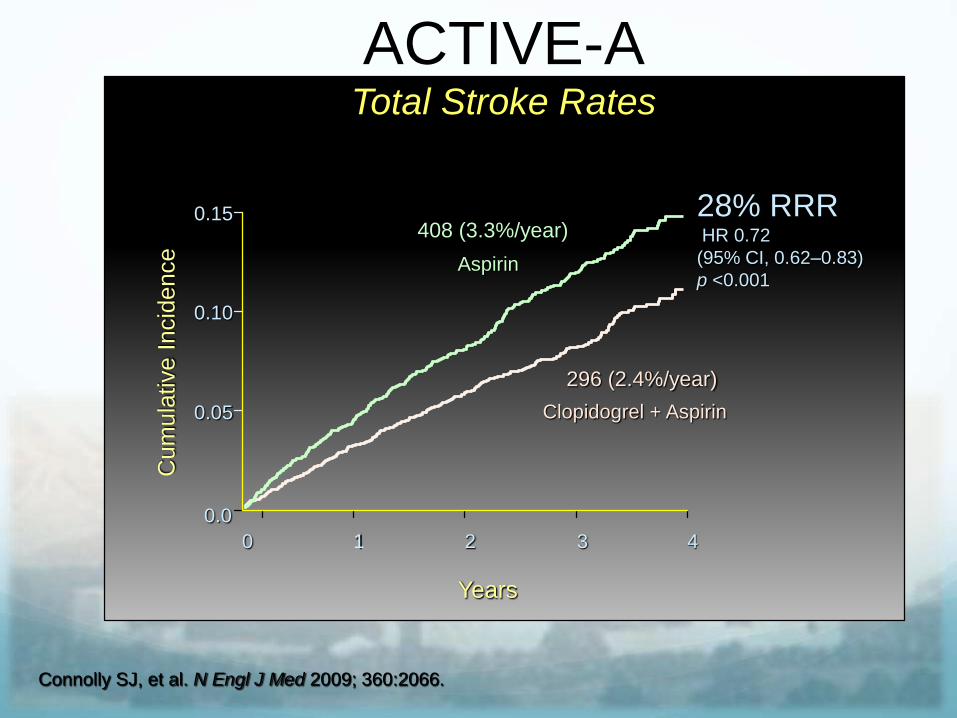
ACTIVE-ATotal Stroke Rates
296 (2.4%/year)
408 (3.3%/year)
Cum
ula
tive I
ncid
ence
28% RRRHR 0.72
(95% CI, 0.62–0.83)
p <0.001
0.0
0.05
0.10
0.15
0 1 2 3 4
Aspirin
Clopidogrel + Aspirin
Years
Connolly SJ, et al. N Engl J Med 2009; 360:2066.
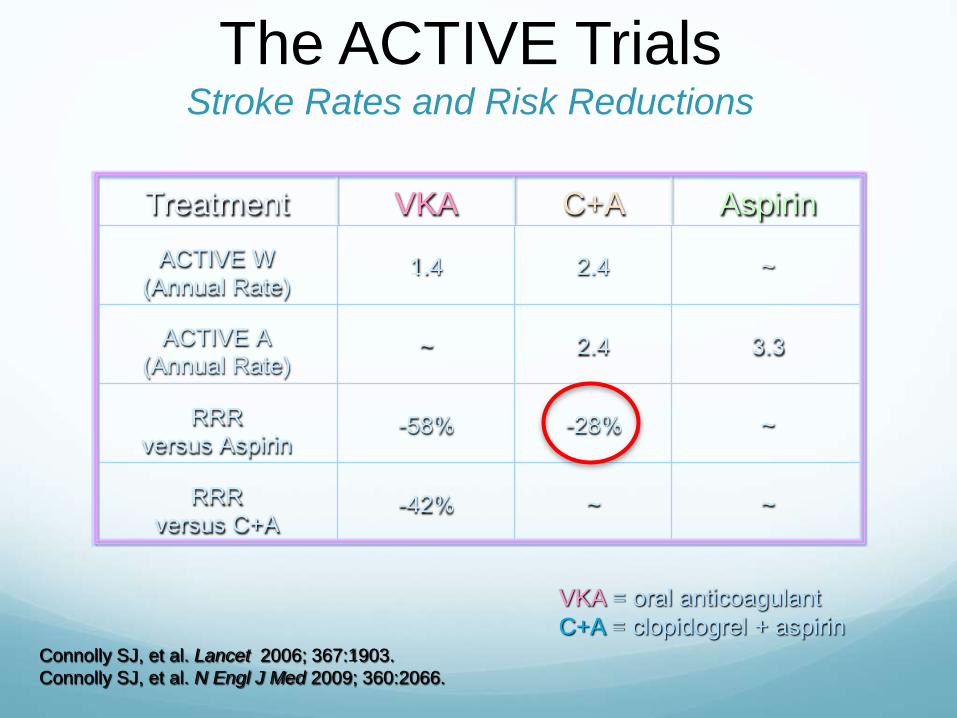
The ACTIVE TrialsStroke Rates and Risk Reductions
Connolly SJ, et al. Lancet 2006; 367:1903.
Connolly SJ, et al. N Engl J Med 2009; 360:2066.
VKA = oral anticoagulant
C+A = clopidogrel + aspirin
Treatment VKA C+A Aspirin
ACTIVE W (Annual Rate)
1.4 2.4 ~
ACTIVE A (Annual Rate)
~ 2.4 3.3
RRR versus Aspirin
-58% -28% ~
RRR versus C+A
-42% ~ ~
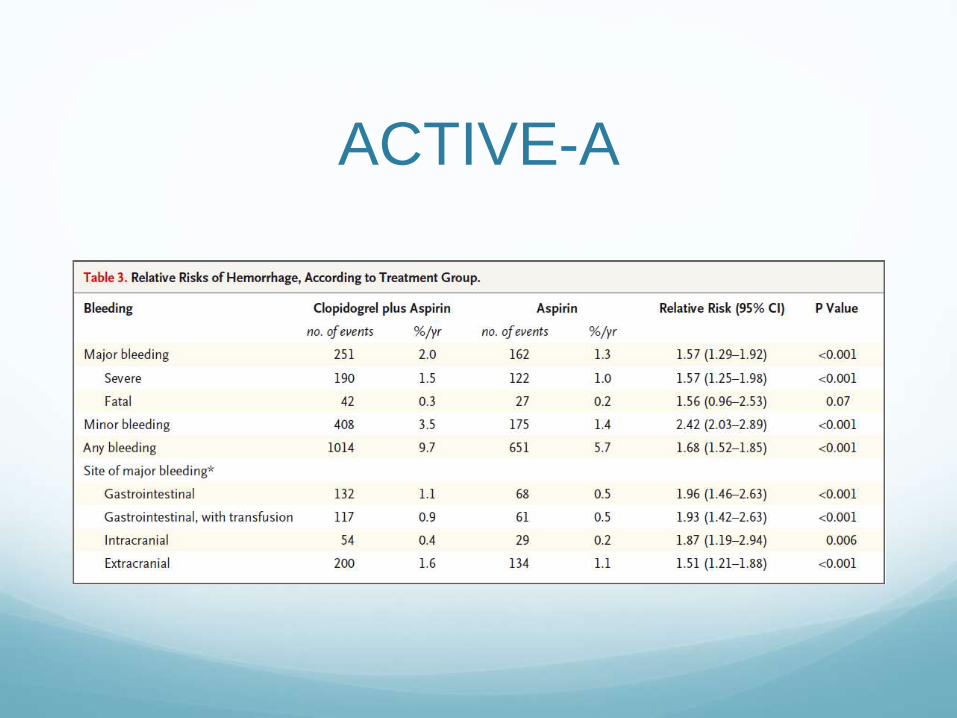
ACTIVE-A
ICTUS NON
CARDIOEMBOLICO
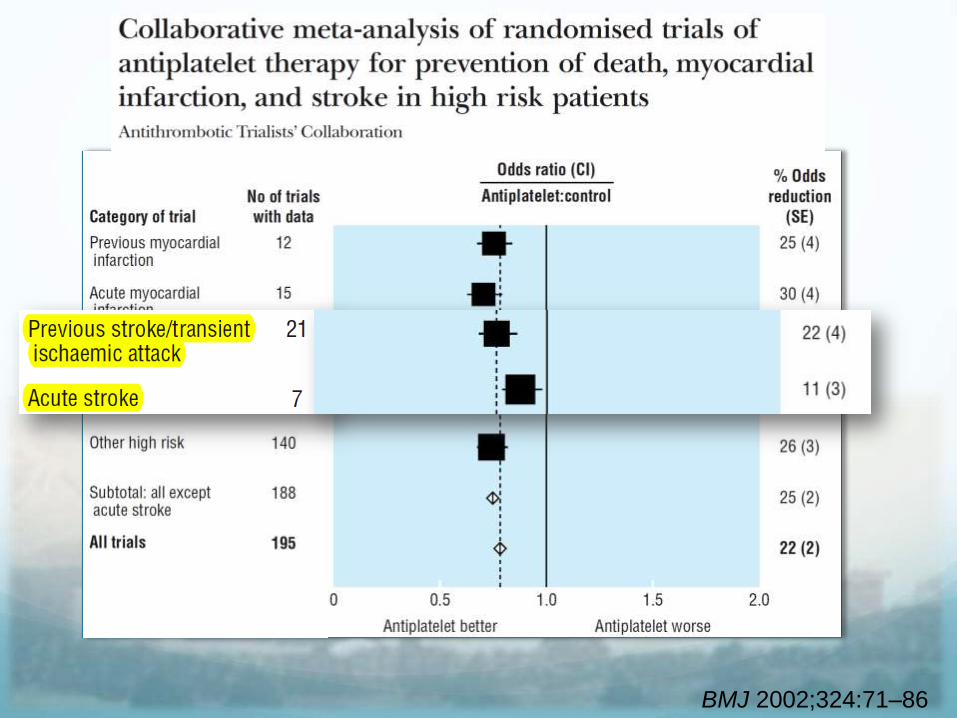
BMJ 2002;324:71–86
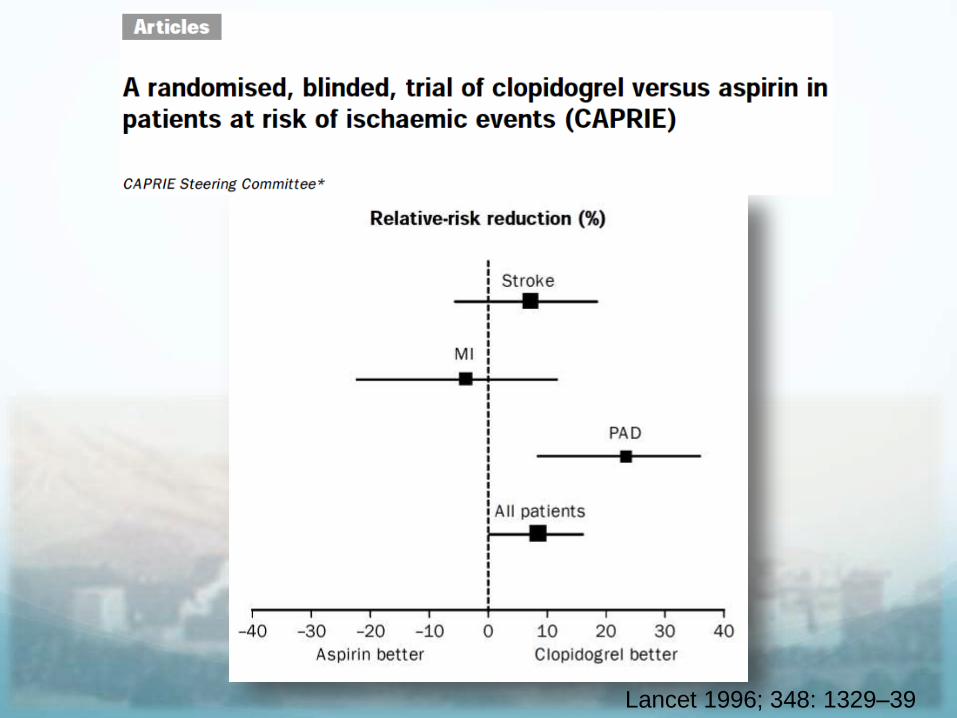
Lancet 1996; 348: 1329–39
1° Gruppo di studi Trial che hanno randomizzato pazienti a distanza
anche di diversi mesi dall’evento acuto valutando singola verso doppia antiaggregazione per periodi molto lunghi per circa 2,5-3 anni
ESPS2 1996 (Dipiridamolo+ASA Vs Dipirodamolo Vs ASA) 6.602 pts, FUP 2 anni
MATCH 2004 (Clopidogrel+ASA Vs Clopidogrel)
ESPRIT 2006 (Dipiridamolo + ASA Vs ASA)
CHARISMA 2006 (Clopidogrel and Aspirin versus Aspirin 1/3 dei pazienti su 12.000 circa 4000)
PRoFESS 2009 (Dipiridamolo+ASA Vs clopidogrel)
SPS3 2012 Clo+ASA vs ASA <180gg x 3,4 aa (ictus lacunare)
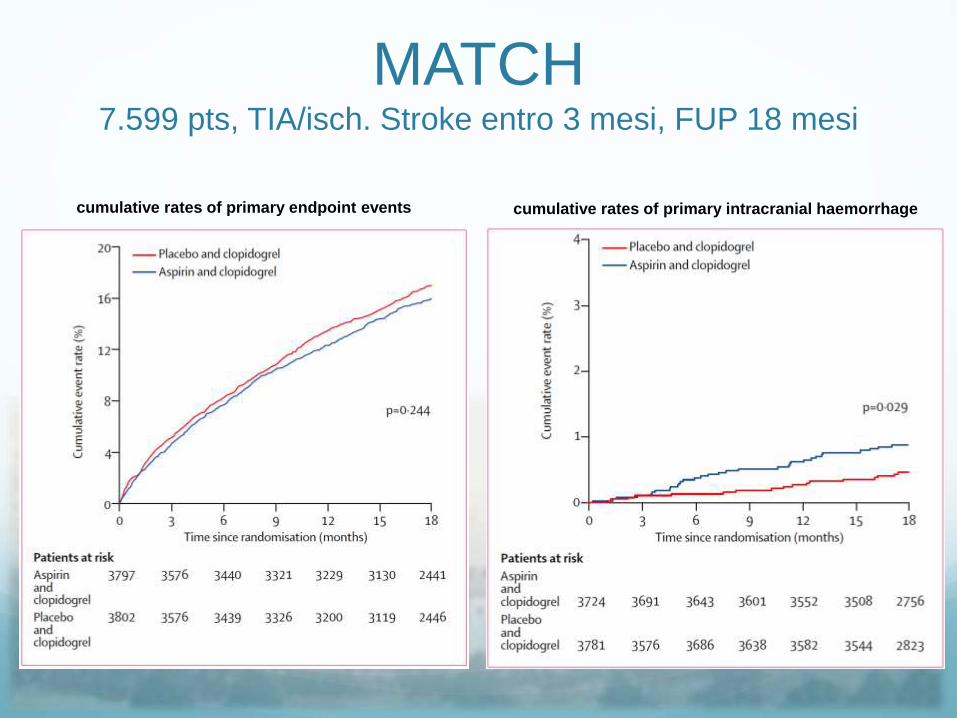
MATCH7.599 pts, TIA/isch. Stroke entro 3 mesi, FUP 18 mesi
cumulative rates of primary intracranial haemorrhagecumulative rates of primary endpoint events
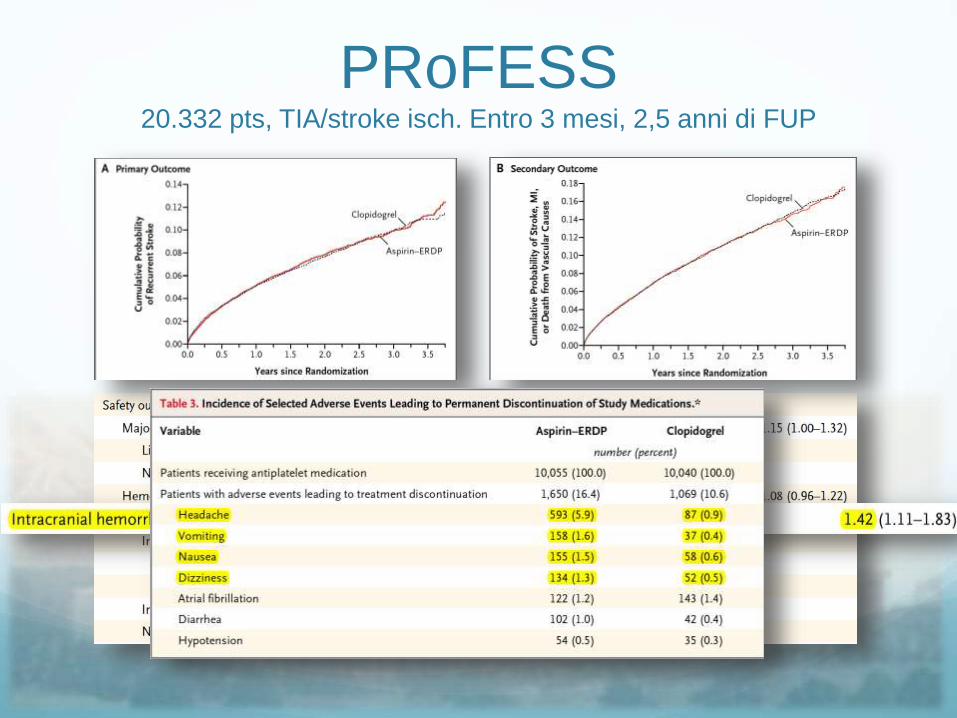
PRoFESS20.332 pts, TIA/stroke isch. Entro 3 mesi, 2,5 anni di FUP
2° Gruppo di studi Trial che hanno arruolato pazienti nella fase acuta ed hanno
trattato i pazienti per periodi molto più brevi come
CARESS (<3m x 7 gg) Clo+ASA vs ASA Circulation. 2005
CLAIR (<7 gg x 7 gg EP microemboli) Clo+ASA vs ASA Lancet Neurol 2010
FASTER (ASA+Clo vs ASA,<24h x 90 gg) Lancet Neurol 2007
EARLY (studio tedesco Dipiridamolo+ASA vs ASA DAPT <24h x 7 gg)
CHANCE (2013) 5.170 pts (il più interessante sia per i numeri che per i risultati della DAPT in fase precoce) < 24h x 21 gg
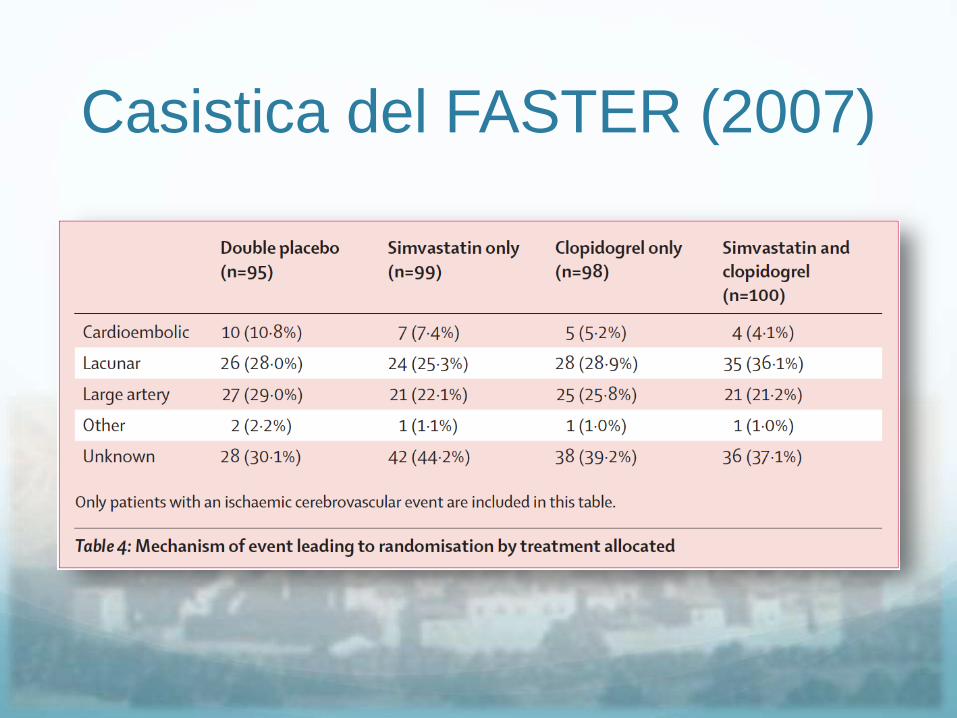
Casistica del FASTER (2007)
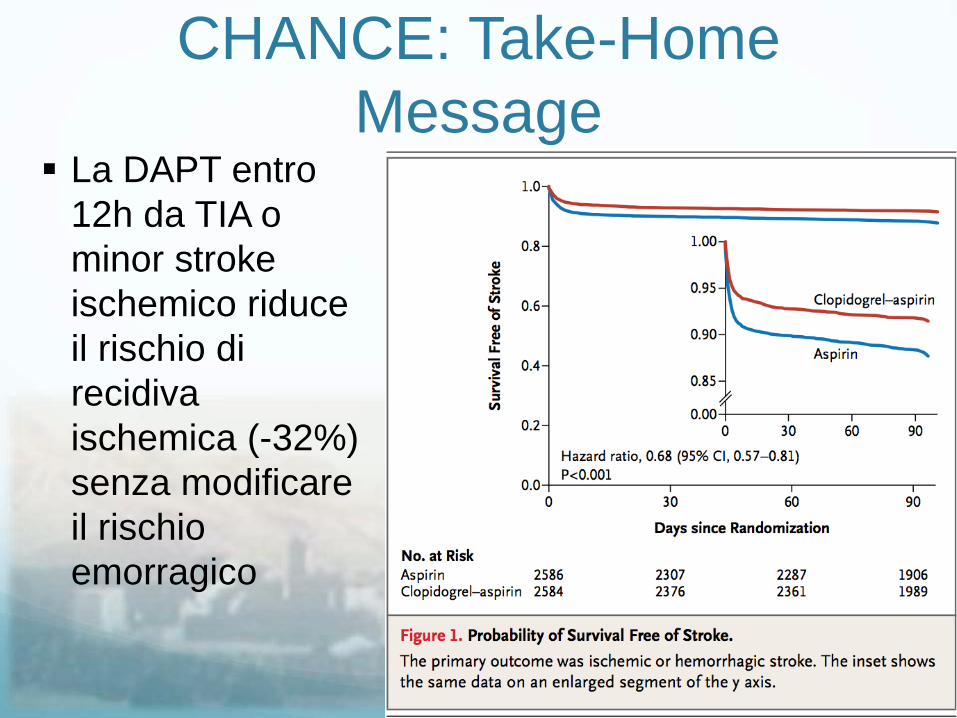
CHANCE: Take-Home
Message La DAPT entro
12h da TIA o
minor stroke
ischemico riduce
il rischio di
recidiva
ischemica (-32%)
senza modificare
il rischio
emorragico
Le Metanalisi hanno
esplorato:1. Intervallo di tempo fra esordio dei sintomi e
randomizzazione
Rischio di recidive
Rischio di eventi emorragici
2. Durata del trattamento
METANALISI Metanalisi di Wong
(Circulation. 2013;128:1656-1666.)
È stata focalizzata l’attenzione sui soli pazienti randomizzati entro 3 giorni
Caress, Chance, Clair ecc.
Charisma, ESPS2, Match, Esprit, PRoFESS (solo primi 3 gg)
Le durate dei trattamenti sono
molto brevi per Caress (7gg) , Chance (21gg), Clair (7gg )
Charisma (28m), ESPS2 (24m), Match (18m), Esprit (42m) PRoFESS(3 m)
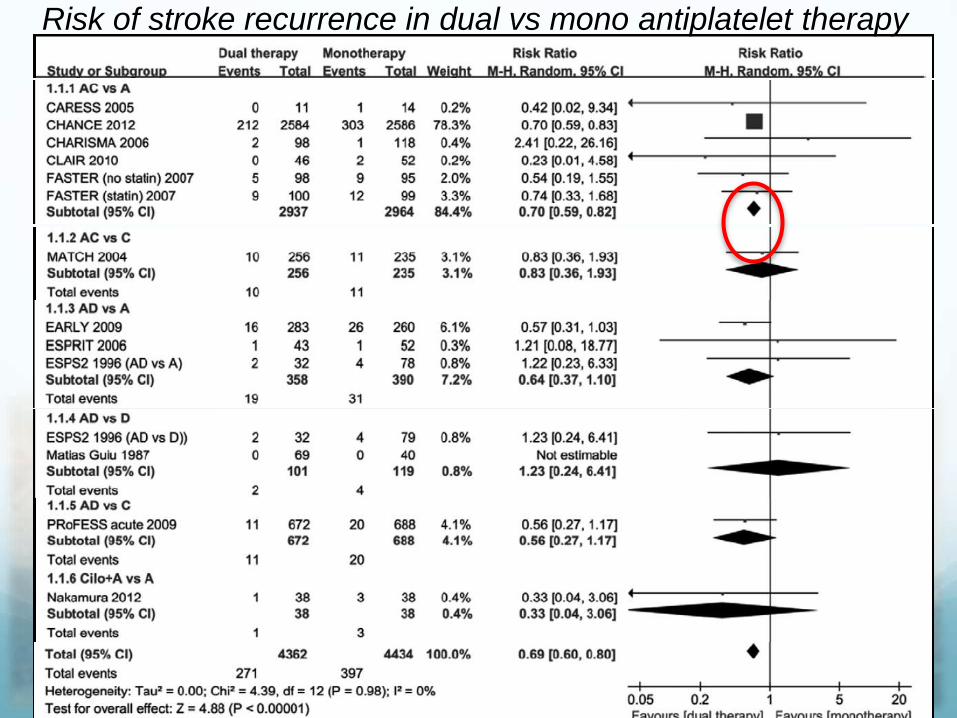
Risk of stroke recurrence in dual vs mono antiplatelet therapy
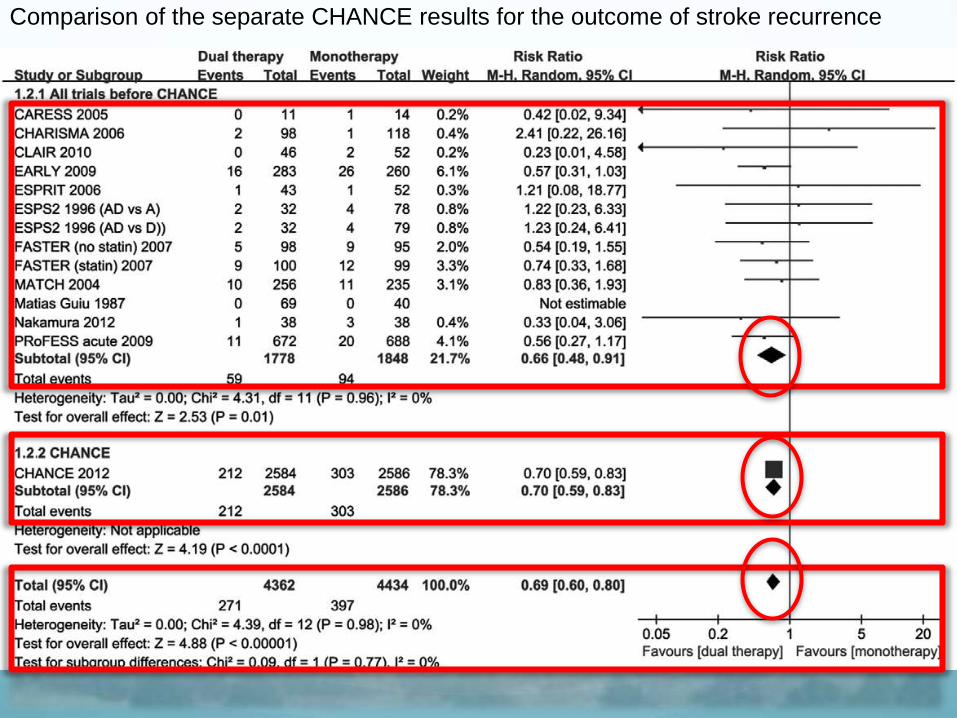
Comparison of the separate CHANCE results for the outcome of stroke recurrence
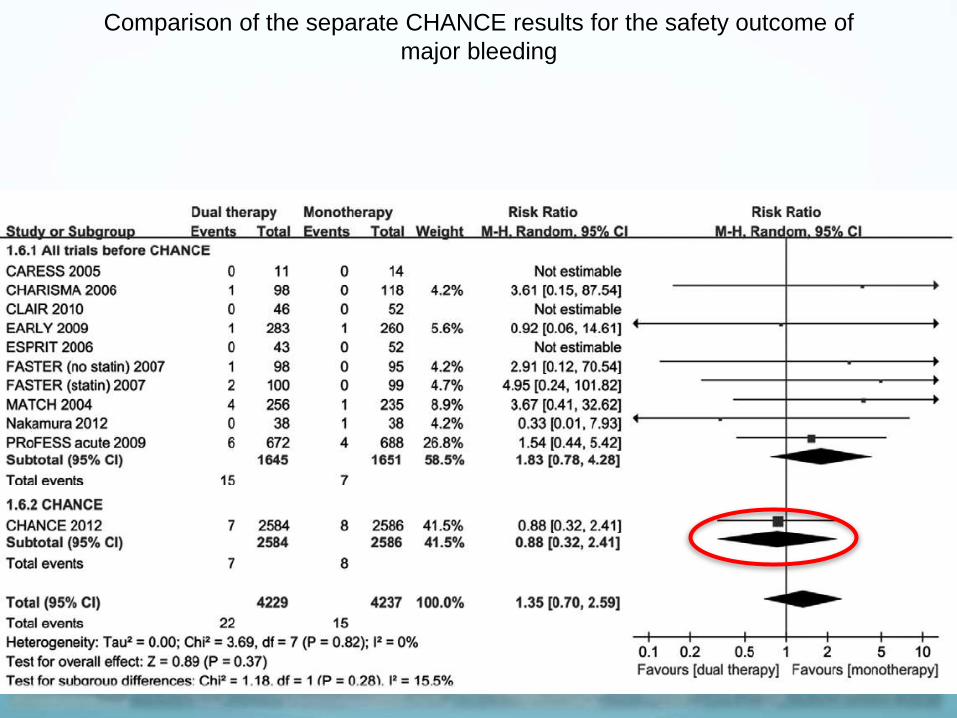
Comparison of the separate CHANCE results for the safety outcome of
major bleeding
METANALISI
PLoS One. 2014 Aug 11;9(8):e104402.
doi: 10.1371/journal.pone.0104402. eCollection 2014
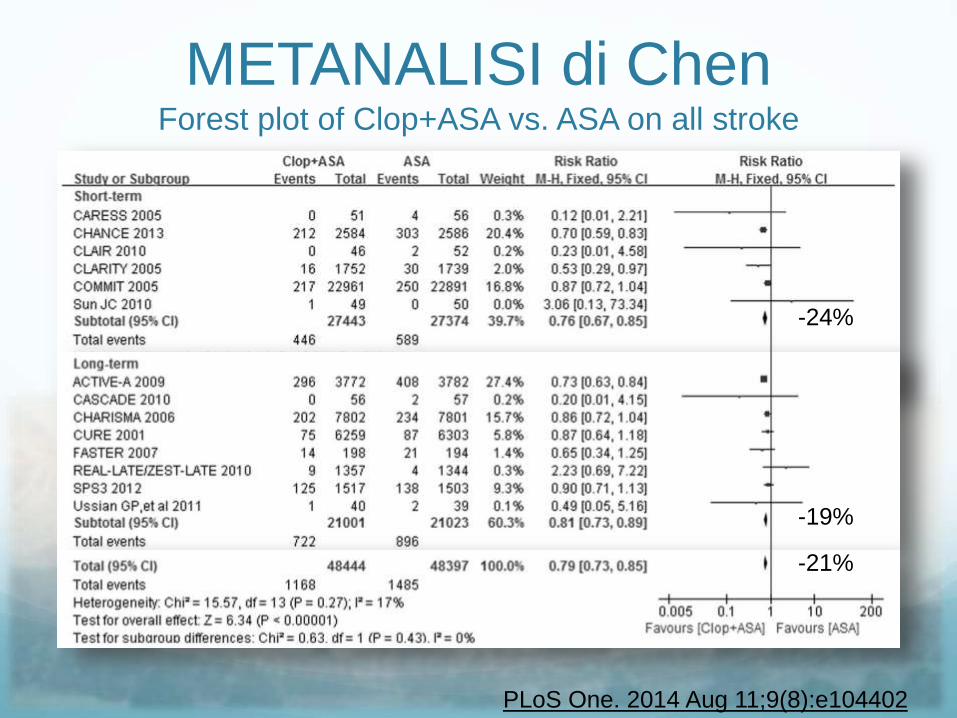
METANALISI di ChenForest plot of Clop+ASA vs. ASA on all stroke
PLoS One. 2014 Aug 11;9(8):e104402
-24%
-19%
-21%
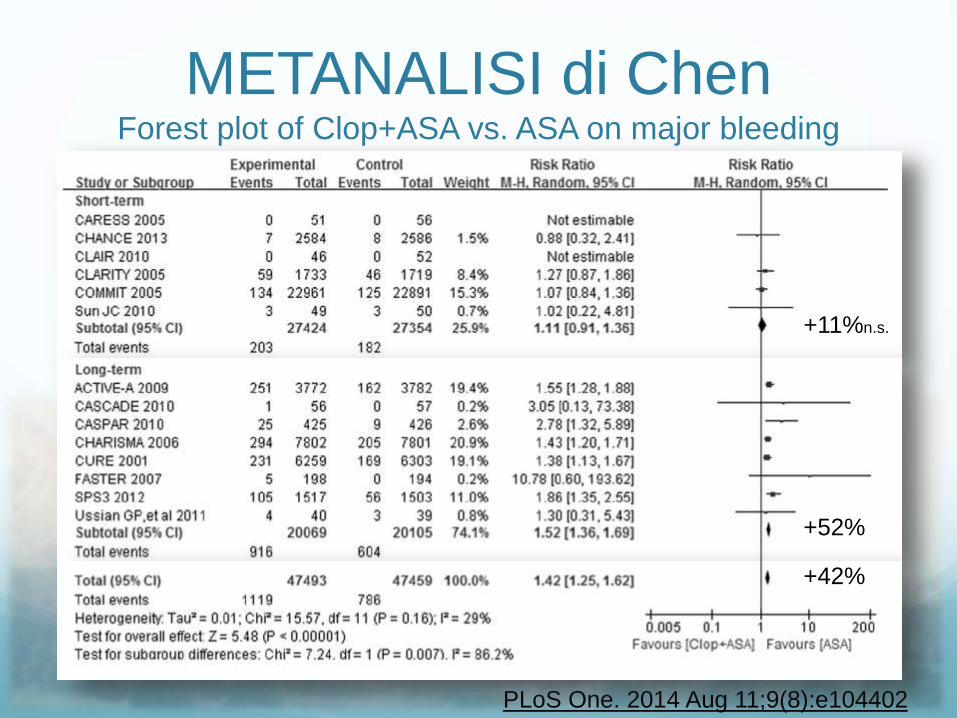
METANALISI di ChenForest plot of Clop+ASA vs. ASA on major bleeding
PLoS One. 2014 Aug 11;9(8):e104402
+11%n.s.
+52%
+42%
METANALISI di Zhang
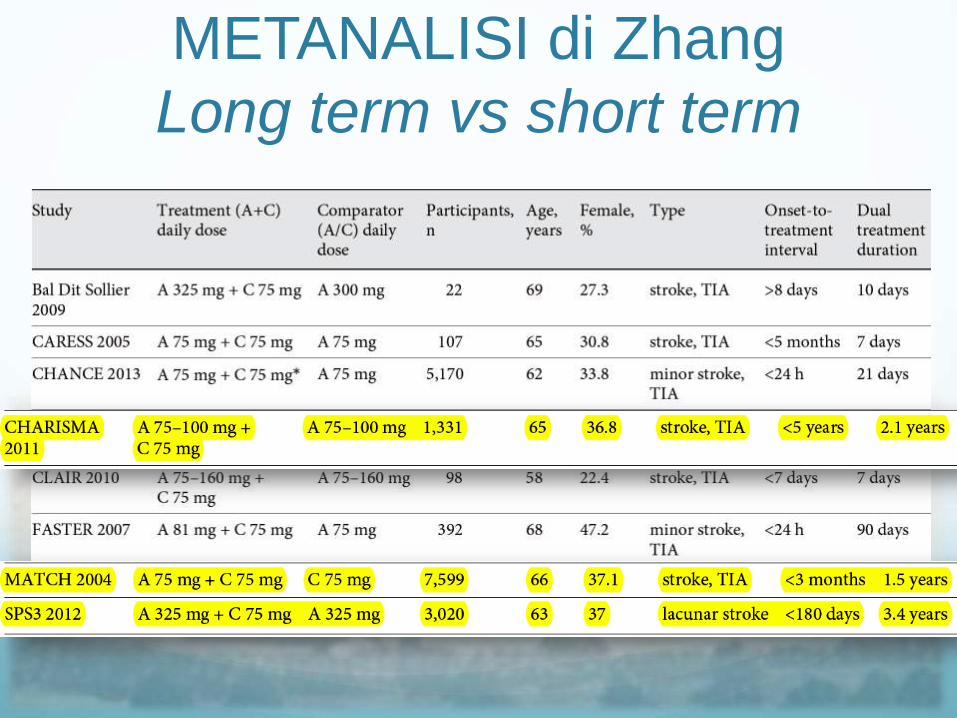
METANALISI di Zhang
Long term vs short term
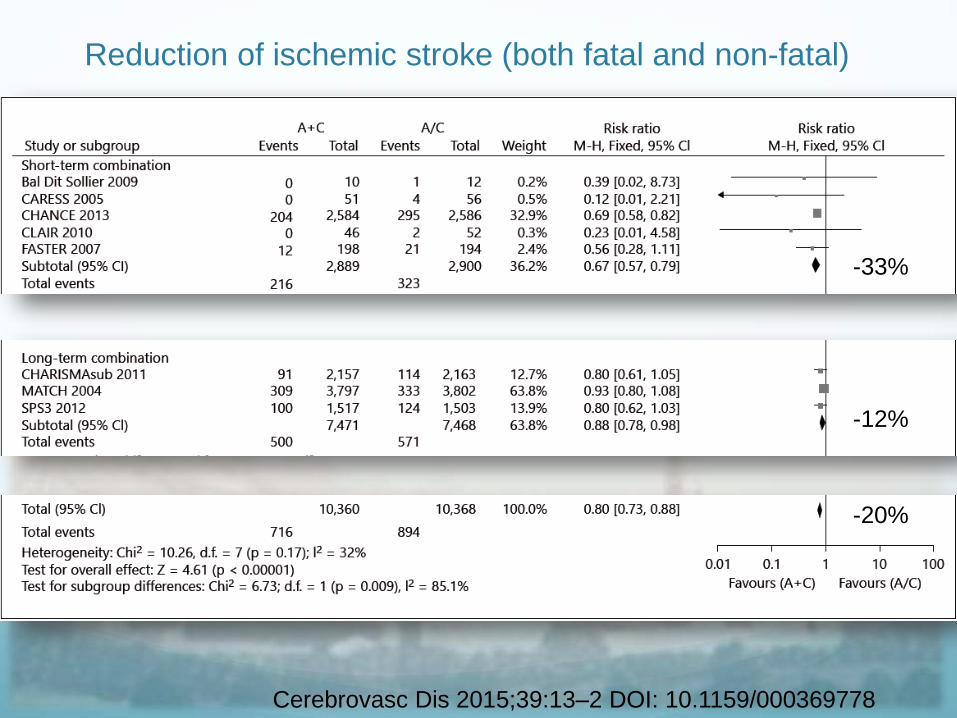
Reduction of ischemic stroke (both fatal and non-fatal)
Cerebrovasc Dis 2015;39:13–2 DOI: 10.1159/000369778
-33%
-12%
-20%
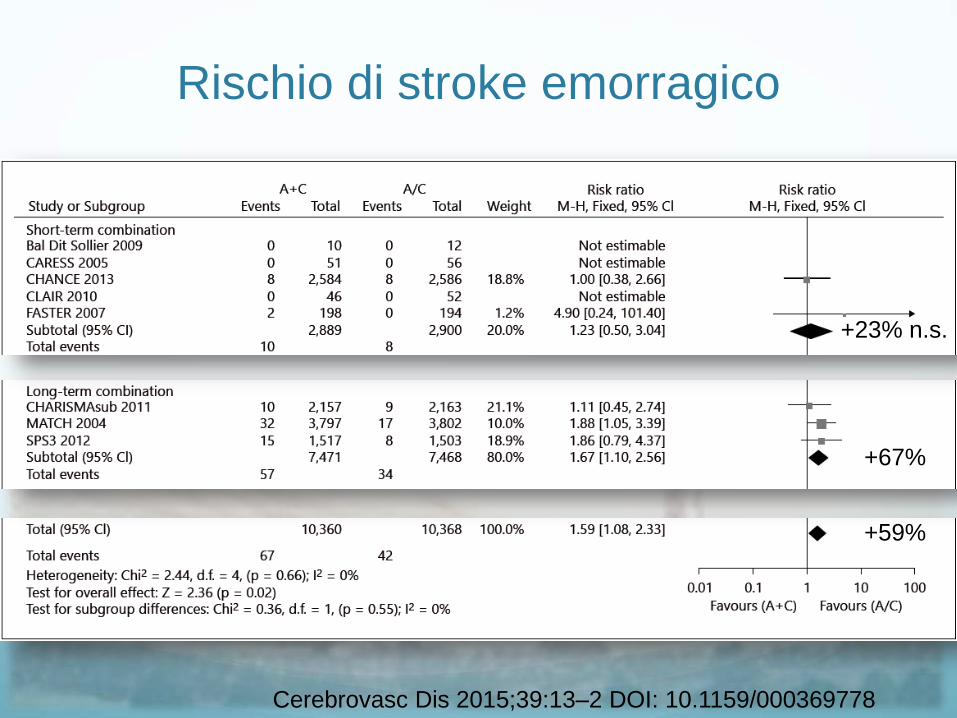
Rischio di stroke emorragico
Cerebrovasc Dis 2015;39:13–2 DOI: 10.1159/000369778
+59%
+67%
+23% n.s.
Timing
Tipo di evento ischemico
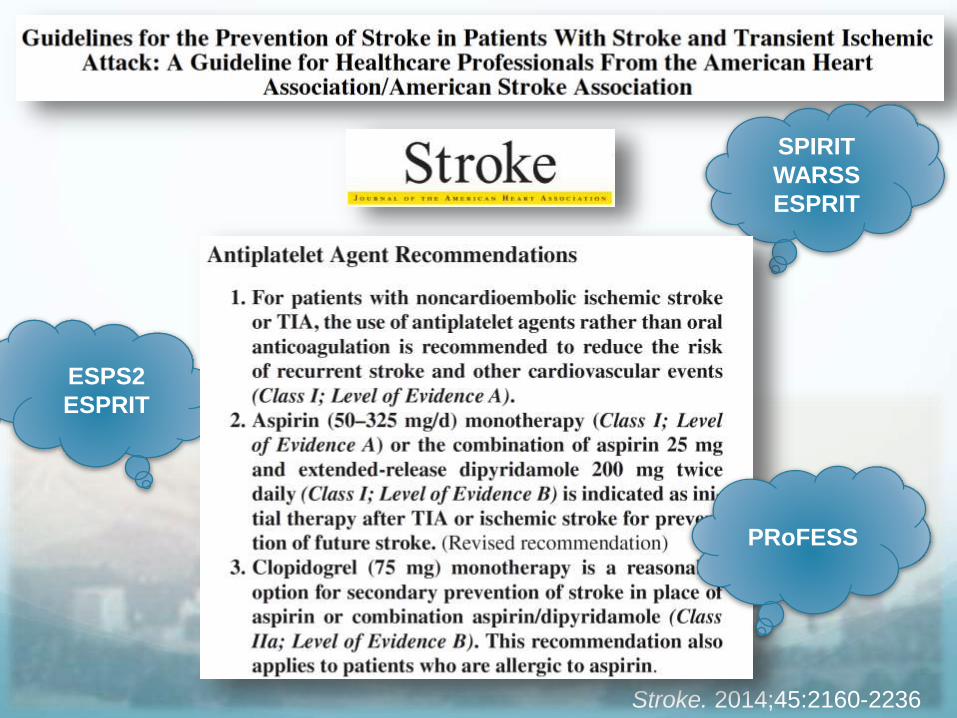
Stroke. 2014;45:2160-2236
SPIRIT
WARSS
ESPRIT
ESPS2
ESPRIT
PRoFESS
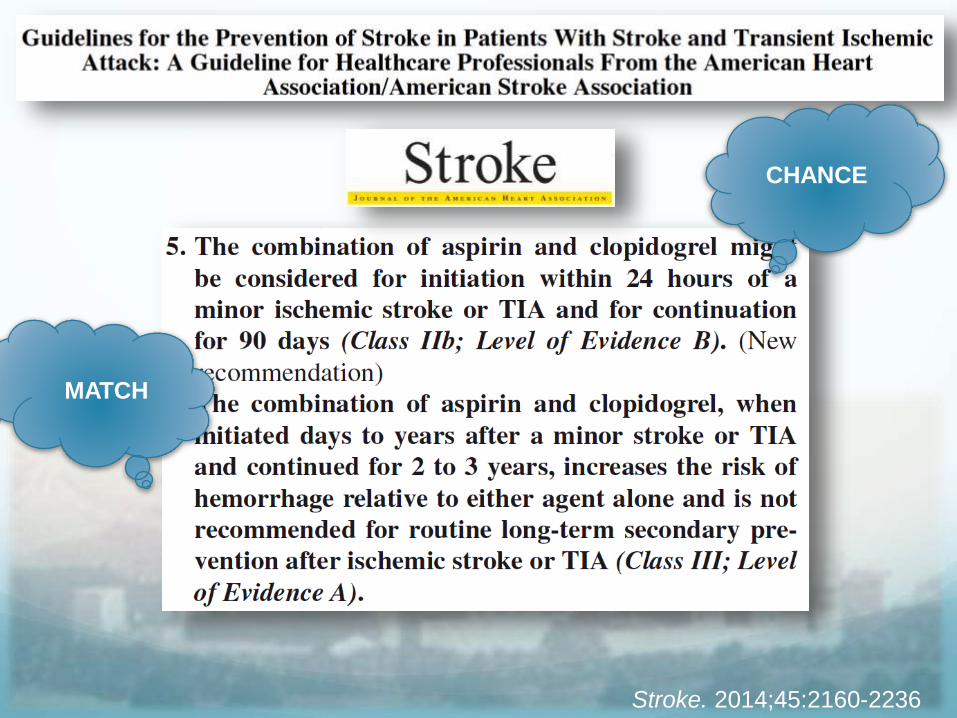
Stroke. 2014;45:2160-2236
CHANCE
MATCH
WASID Trial: Comparison of Warfarin and Aspirin for Symptomatic
Intracranial Arterial Stenosis
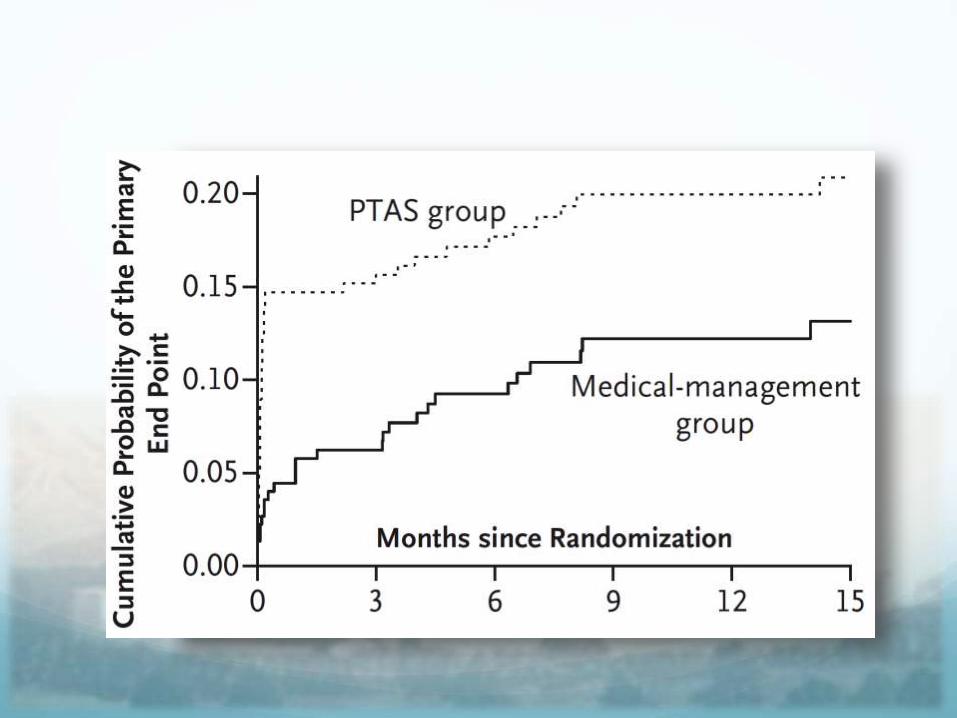
SAMMPRIS Trial:Stenting and Aggressive Medical Management
for Preventing Recurrent stroke in Intracranial
Stenosis
N Engl J Med 2011;365:993-1003
Occorre distinguere in sottogruppi!
Grazie per l’attenzione!





























