Embed Size (px)
Citation preview
Antiphospholipid Syndrome and Pregnancy
BY : Ali sarhan
Definition
• Antiphospholipid syndrome (APS) is an acquired autoimmune disorder that manifests clinically as recurrent venous or arterial thrombosis.
• laboratory abnormalities in APS include persistently elevated levels of antibodies directed against membrane anionic phospholipids.
• This disorder is associated with pregnancy complications, including preeclampsia, thrombosis, fetal growth restriction, and fetal loss.
Obstetric features of APS
1. Unexplained fetal death or stillbirth2. Recurrent pregnancy loss 3. Severe preeclampsia at less than 34
weeks’ gestation4. Unexplained severe fetal growth
restriction5. Chorea gravidarum
Nonobstetric features of APS
1. Nontraumatic thrombosis or thromboembolism (venous or arterial )
2. Stroke3. Unexplained transient ischemic attack 4. Unexplained amaurosis fugax5. Autoimmune thrombocytopenia6. Autoimmune hemolytic anemia7. Unexplained prolongation of a clotting
assay ( due to low platelets )
Classification
1. Primary APS : disease without other recognized autoimmune disease.
2. Secondary APS : is diagnosed in patients with other autoimmune disorders, such as systemic lupus erythematous (SLE).
Three antiphospholipid antibodies that have proven association with the diagnosis of APS:
1. lupus anticoagulant (LAC)2. anticardiolipin (aCL) antibody3. anti-beta-2glycoprotein I antibody.
Pathophysiology
• Biologic effects mediated by the human aPL antibodies include the following:1. Reactivity with endothelial structures that disturbs the balance
of prostaglandin E2/thromboxane production2. Interaction with platelet PLs upregulation of platelet
aggregation3. Interaction of aPL with phosphatidylserine exposed during
trophoblast syncytium formation, which raises the possibility of a more direct effect of these autoantibodies on placental structures
• Early histological studies demonstrated decidual vasculopathy and placental thrombosis. Displacement of annexin V from trophoblasts contributes to a procoagulant state through acceleration of coagulation reactions.
• More recently, direct trophoblastic damage by aPL, independent of mechanisms involving thrombosis and complement activation, has been demonstrated. Interaction of aPL with 2GPI, exposed during trophoblast syncytium formation, has been shown to cause inhibition of trophoblast invasiveness. This mechanism has been hypothesised to contribute to early pregnancy loss.
Mechanism
• Like other autoimmune disorders, APS does not have a known etiology , and its more common in women .
• The association between aPL antibodies and particular human leukocyte antigen (HLA) alleles and HLA-linked epitopes has been reported in studies of patients with lupus erythematous (eg, HLA-DR7, HLA-DR4).
Phospholipid release• PL molecules are present in the inner surface of the cell (ie, on the inner or outer
surface of the cell membrane or intracellular organelles) and in microorganisms. • Therefore, during infectious disease processes, including viral , bacterial , spirochetal
and parasitic infections, the disruption of cellular membranes may occur during cell damage, consequently PL released, stimulating aPL antibodies.
Some numbers !!
• In USA : – 80% of patients are females – The aPL antibodies are detected in approximately 2% of all patients with nontraumatic
venous thrombosis.– Approximately 22% of women with APS have had venous thrombosis , 24% of
thrombotic events have been found to occur during pregnancy or the postpartum period.
– women with recurrent pregnancy loss( 3 and more ) , 10–20% have detectable aPL.– women with documented APS should not take estrogen-progestin combination oral
contraceptives.– The rate of fetal loss may exceed 90% in untreated patients with APS.

• In IRAQ : – a research was done on 2012 , showing that of 200 women underwent the test
, 26.5% had anticardiolipin antibodies present, while 13.5% were positive for lupus anticoagulant.
– Clinically , those with antiphospholipids antibodies were found to have significantly higher prevalence of positive medical history of thrombosis (17.6%) and family history of recurrent abortions 19.1% .
– No significant differences were found in the prevalence of a positive history of still births, intrauterine death and congenital abnormalities between APA positive and negative groups respectively .
Presentation
History• The “international consensus statement for the diagnosis of
antiphospholipid syndrome,” was updated in 2006 to requires that the patient have at least 1 clinical and 1 laboratory criterion.
• Clinical criteria1. One or more clinical episodes of arterial, venous, or small-vessel thrombosis
anywhere . 2. One or more unexplained deaths of morphologically normal fetuses at or after 10
weeks’ gestation3. One or more premature births of morphologically normal fetuses at or before 34
weeks’ gestation because of eclampsia or severe preeclampsia or features consistent with placental insufficiency
4. Three or more consecutive, unexplained spontaneous abortions before 10 weeks’ gestation, with maternal anatomic or hormonal abnormalities and paternal and maternal chromosomal causes excluded
• Laboratory criteria1. Anticardiolipin antibodies (IgG or IgM ) present at moderate or high levels (ie, >40
*GPL or *MPL or >99th percentile) in the blood on 2 or more occasions at least 12 weeks apart
2. Lupus anticoagulant detected in the blood on 2 or more occasions at least 12 weeks apart.
3. Anti-beta2 -glycoprotein I antibodies IgG or IgM - In titers above the 99th percentile for normal as defined by the laboratory performing the test, on 2 or more occasions at least 12 weeks apart
*Note: 1 MPL unit is 1 microgram of IgM antibody , 1 GPL unit is 1 microgram of IgG antibody
Physical Examination• Patients with secondary APS are more likely to have
findings on physical examination, although some physical findings may be associated with primary APS.
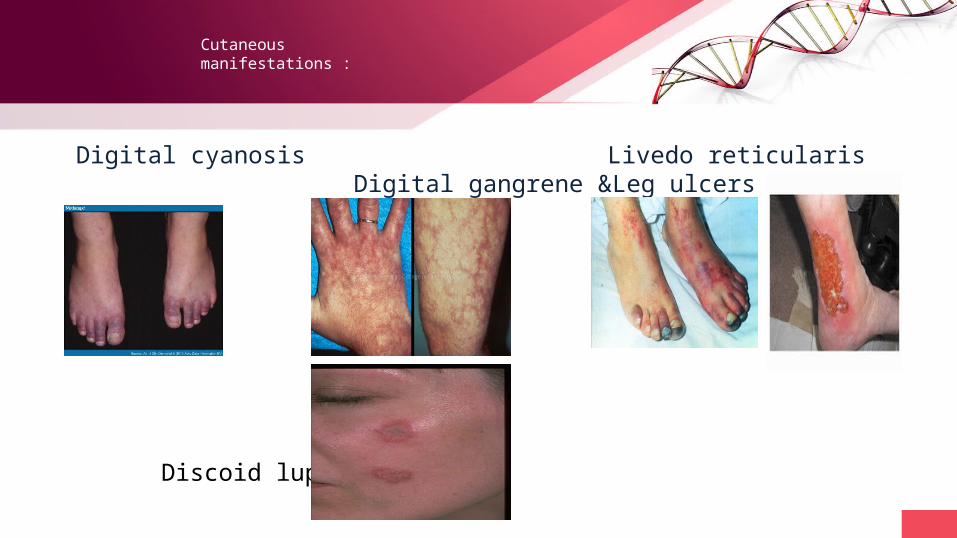
Cutaneous manifestations :
Digital cyanosis Livedo reticularis Digital gangrene &Leg ulcers
Discoid lupus
Catastrophic APSThis term defines a severe, accelerated form of APS resulting in multi-organ failure
from microvascular thrombosis its acute with involvement of at least three different organ systems over a period of days to weeks.
Postpartum syndromeThis is a rare syndrome characterised by pleuropulmonary disease, fevers and cardiac
manifestations due to extensive immunoglobulin IgG, IgM, IgA and C3 deposition.
Why APS not something else ?!!
• Some times the defect is secondary to autoimmune disorder , we suspect that if you had some of these finding :
1. Arthritis - nonerosive arthritis involving 2 or more peripheral joints.2. Serositis - pleuritis , pericarditis or effusion.3. Renal disorder - Proteinuria or cellular casts.4. Hematologic disorder
i. hemolytic anemia with reticulocytosisii. Leukopenia , lymphopenia iii. thrombocytopenia of less than 100,000 cells/µL
5. Skin lesions ( malar rash ) 6. Lymphadenopathy 7. Splenomegaly
Diagnosis
• For diagnosis , we depend on a set of criteria. These were updated in 2006 to reflect new insights into the disease.
• The diagnosis of APS is based primarily on clinical history and laboratory data.
Laboratory Studies
Antiphospholipid (aPL) antibodies are detected by enzyme-linked immunoassays(ELISA)
LAC is detected by phospholipid (PL)-dependent clotting assays, with prolongation in activated partial thromboplastin time (aPTT) , Kaolin clotting time and Plasma clotting time.
aCL or anti-beta2 -glycoprotein I antibodies, an IgG isotype greater than 12-20 GPL units is indicative(moderate and high levels ) .
• combining tests for LAC, anti-beta2 -glycoprotein I, and anti-phosphatidylserine/prothrombin (aPS/PT) antibodies provided greater diagnostic accuracy for APS than did other combinations of laboratory tests.
• The investigators also found that patients in whom all 3 tests were positive were at greater risk for clinical events, such as thrombosis or pregnancy loss, than were patients in whom only 1 or 2 of the tests were positive.
• Antiphospholipid antibodies are found in 3–5% in those without thrombosis or obstetric morbidity.
• All studies need to be repeated in at least 12 weeks for confirmation before the diagnosis of APS is appropriate.
• Thrombocytopenia is common, with platelet-specific antibodies distinct from aPL
• Positive direct Coombs test with occasional cases of clinical haemolytic anaemia.
• On histopathology , Decidua from women with antiphospholipid syndrome had more necrosis, acute and chronic inflammation, vascular thrombus , more infarction, intravascular fibrin deposition, syncytial knot formation, and fibrosis
DOPPLER STUDIES : increased impedance in the uterine arteries and umbilical arteries at 18–24 weeks of gestation provided useful prediction of both pre-eclampsia and intrauterine growth restriction .

Management
Keep In mind !
• Its considered a high-risk obstetrical patients
• Therapeutic abortion is NOT indicated in pregnant women with autoimmune disease.
• Low maternal platelets level makes the epidural anestheisa unfavorable .
• chloroquine and cytotoxic agents are not recommendcontraindicated during pregnancy; patients should stop taking these drugs several months prior to becoming pregnant.
• breastfeeding is not recommended if high doses of cytotoxic or immunosuppressive agents are required.
Obstetric Care
• Education about the signs or symptoms of thrombosis or thromboembolism, severe preeclampsia, or decreased fetal movement.
• Ultrasonography is recommended every 3-4 weeks starting at 18-20 weeks
• Human chorionic gonadotropin (hCG) level – doubling every 2 days in the first month of pregnancy indicates a successful outcome in 80-
90% of cases. – However, when the increases are abnormal (ie, slower), a poor outcome is predicted in 70-80%
of cases.
Anticoagulation therapy
• Low-molecular-weight heparin (LMWH) may be used in these patients.
• Heparin-induced osteoporosis occurs in 1-2% of cases, so Bone density studies should be done .This may be most important in women who have been treated in a previous pregnancy or are planning pregnancy.
• Warfarin may be substituted for heparin during the postpartum period to limit further risk of heparin-induced osteoporosis and bone fracture (its CI during pregnancy ) .
• Low-dose aspirin combined with prophylactic doses of heparin or LMWH appears to be superior to aspirin therapy alone or maternal steroids.
• APS with prior fetal death or recurrent pregnancy loss : low molecular weight Heparin with aspirin 75mg daily per oral with vitamin d and calicum supplement .
• APS without prior pregnancy loss or thrombosis : No treatment or daily treatment with low-dose aspirin .
• APS with prior venous or arterial thrombosis : heparin at intermediate or therapeutic dosage + aspirin
• Duration : the treatment should begin at early pregnancy , or even before the female conceives , then to be continued up to the end of the puerperium.
• Corticosteroids have not been proven effective for persons with primary APS, and they have been shown to increase maternal morbidity and fetal prematurity rates.
• unfractionated intravenous (IV) heparin and fractionated subcutaneous (SC) LMWH are the 2 choices for initial anticoagulation therapy.
• LMWHs are derived from unfractionated heparin but have smaller, more standard average masses than does unfractionated heparin.
• LMWHs have higher specificity for factor Xa and have fewer effects on platelet activity causeing less bleeding ,and less heparin-induced osteoporosis.
Heparin
• augments the activity of antithrombin III to Inactivates factor Xa and inhibits conversion of prothrombin to thrombin and prevents the conversion of fibrinogen to fibrin. Heparin does not actively lyse but is able to inhibit further thrombogenesis.
• 8000-10,000 units IV initially, THEN 50-70 units/kg (5000-10,000 units) q4-6hr.• Adverse Effects
1. Heparin-induced thrombocytopenia, possibly delayed (10-30% )2. Mild pain3. Hemorrhage 4. Injection site ulcer (after deep SC injection)5. Osteoporosis (long-term, high-dose use)6. Immune hypersensitivity reaction or Anaphylaxis
Antidote : protamine 1-1.5 mg per 100 units of heparin; not to exceed 50 mg
Enoxaparin (Lovenox) • Dose : 40 mg SC daily • SE : elevation in liver enzymes ,bleeding, Thrombocytopenia. ( 5 % )• Antidote : protamine 1 mg per mg enoxaparin
Dalteparin ( fragmin ) • Dose : 5000 iu daily• SE : Injection site hematoma (7-35%),Thrombocytopenia (10.9-13.6%, patients with
cancer ) ,Injection site pain (4.5-12%) ,Major hemorrhage (up to 4.6%) ,Increased liver function test (up to 4.3%) ,Wound hematoma ,Hematuria
• Antidote : protamine 1 mg protamine for 100 units dalteparin
Other choices
• plasma exchange and corticosteroids are generally used in the treatment of catastrophic type (CAPS) .
• Intravenous immunoglobulin or cyclophosphamide may also be considered in selected patients with CAPS.
• Rituximab has shown benefit in controlling severe thrombocytopenia, skin ulcers, and cognitive dysfunction that can be associated with APS.

Follow up
• In women with APS and 1 or more prior thrombotic events, lifelong anticoagulation with warfarin may be advisable to avoid recurrent thrombosis. An assessment by a rheumatologist or hematologist may also be helpful.
• Keep INR 2-3 • Initial dose: 2-5 mg PO/IV daily for 2 days• Check INR after 2 days and adjust dose according to results• Typical maintenance dose ranges between 2 and 10 mg/day
References
1. The American College of Obstetricians and Gynecologists. Antiphospholipid Syndrome. ACOG Practice Bulletin. January/2011. 118:1-8.
2. Antiphospholipid Antibodies in Iraqi Women with Recurrent Mid-Trimester Abortions , J Lab Physicians. 2012 Jul-Dec; 4(2): 78–82.
3. Review Diagnosis and management of antiphospholipid syndrome in pregnancy (Authors Bethan Myers / Sue Pavord)
4. Histologic features of placentas and abortion specimens from women with antiphospholipid and antiphospholipid-like syndromes. 2004 Aug;25(7):642-8
5. http://emedicine.medscape.com/article/261691-overview






























