Embed Size (px)
DESCRIPTION
website: http://www.am-medicine.com Facebook page : https://www.facebook.com/pages/Am-medicine/207726329406832 Facebook group: https://www.facebook.com/groups/1409138472653811/
Citation preview


MOB TCD
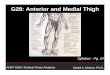
Anterior Thigh
Professor Emeritus Moira O’Brien
FRCPI, FFSEM, FFSEM (UK), FTCD
Trinity College
Dublin

Cutaneous Supply MOB TCD

Thigh
• Anterior muscle group: supplied by femoral nerve
• Sartorius• Quadriceps: rectus femoris, vastus
medialis, vastus intermedius and vastus lateralis
• Pectineus
MOB TCD

• Medial or adductor group: adductor longus, adductor brevis, adductor portion adductor magnus and gracillis are supplied by the obturator nerve
• Posterior group: hamstring, semimembranosus, semitendinosus, biceps femoris, adductor magnus, below femoral hiatus
• Supplied by sciatic nerve
Thigh MOB TCD

Femoral Sheath
• Anterior wall formed by transversalis fascia
• Posterior by fascia iliaca• Three compartments• Medial, short, is the femoral canal,
contains lymph gland • Opens into abdomen via femoral ring,
site of femoral hernia• Middle compartment contains femoral vein• Lateral, femoral artery and femoral branch of genito-
femoral nerve• Femoral nerve is outside sheath
MOB TCD

Quadriceps Femoris
• Rectus femoris• Vastus medialis• Vastus intermedius• Vastus lateralis• Forms the anterior portion of the
capsule of the knee joint• The largest muscle group in the body • Wastes rapidly if there is an effusion,
particularly the oblique portion of the vastus medialis
MOB TCD

Rectus Femoris
• Tendinous origin from the upper part of the anterior inferior iliac spine (epiphysis) and the groove above the acetabulum
• The most superficial portion of the quadriceps
• The most frequently strained • The only portion of the quadriceps
that crosses two joints • Flexes hip, extends knee• Femoral nerve
MOB TCD

Vastus Medialis
• Vastus medialis arises from the lower half of the trochanteric line
• The spiral line • The medial lip of the linea aspera• The oblique (horizontal) fibres arise
from the lower portion of the adductor magnus, helping to stabilise the patella
• Separate branch from femoral nerve
MOB TCD

• Arises from the upper half of the inter-trochanteric line
• The root of the greatertrochanter• The lateral lip of the gluteal
tuberosity• The lateral lip of the linea aspera • The oblique portion of the muscle
arises from the iliotibial band• Separate nerve supply• Helps to stabilise the patella• Lateralis is a common site for
muscle biopsies and for injections
Vastus Lateralis MOB TCD

Vastus Intermedius
• Arises from the upper two thirds of the anterior and lateral aspect of the shaft of the femur
• It is the deepest portion of the quadriceps and is a common site (with vastus lateralis) for myositis ossificans, after a direct blow to the thigh
• The articularis genu is inserted into the upper part of the suprapatellar bursa
MOB TCD

Quadriceps
• The rectus femoris forms the most superficial lamina of the quadriceps, passes anterior to the patella
• To form the anterior part of the patellar ligament
• The fibres of the medialis and the lateralis decussate cross in an X-shape and lie in a plane posterior to the rectus femoris
• Some of these fibres form the retinacular fibres • Their oblique portions are inserted into the sides of
the patella
MOB TCD

Quadriceps Femoris
• The vastus intermedius is the most posterior lamina, forms the main part of the patellar ligament
• It is the most powerful extensor • The patellar ligament is inserted into
the smooth upper portion of the tibial tuberosity
• The quadriceps are the extensors of the knee
• Only the rectus femoris portion arises above the hip joint, and therefore is also a flexor of the hip
MOB TCD

Weak Vastus Medialis Obliquus
• Lower most fibres of vastus medialis• Partly arise from the adductor
magnus• Straightens the pull on the quads
tendon and patella• Controls patella tracking during
flexion/extension of the knee • Fibres atrophy quickly after knee
injury (within 24 hours)• 10-15 ml of effusion inhibit VMO • VMO rehabilitation strength and
timing of contraction
MOB TCD

Abnormal Lower Limb Biomechanics
Anatomical anomalies• Femoral torsion• Genu valgum • Increased Q angle • High (Alta) patella• Tibial torsion• Overpronation• Q angles
males 140 and females 170
> 200 greater problems
MOB TCD

The Q-angle
• The Q-angle is the angle formed by a line drawn from the anterior superior iliac spine to the centre of the patella
• And a line drawn upwards from the attachment of the patellar ligament to the tibial tubercle passing through this point
MOB TCD

• Functionally, on standing, the normal angle is 10–15°
• With the knee at 90°of flexion, an angle of 6°is normal, while greater than 10°is abnormal
• Contraction of the quadriceps tends to displace the patella laterally in the femoral groove
• The oblique fibres of the vastus medialis and the bony prominence of the lateral femoral condyle resist this
The Q-angle MOB TCD

Osgood Schlatter
• In young athletes, the patellar ligament is stronger than the bone
• Which can lead to a traction apophysitis of the tibial tuberosity, Osgood Schlatter disease
• Jumpers’ knee is a lesion at the apex of the patella and the ligament
MOB TCD

Sartorius
• Sartorius arises from anterior superior illiac spine
• Forms lateral boundary of femoral triangle • Crosses adductor longus at apex• Lies anterior to femoral artery• Posterior to adductor longus lies the
profunda artery• Knife injury at apex can injury both arteries
and the main blood supply to lower limb• Sartorius lies on roof of subsartorial canal which
contains femoral artery
MOB TCD

• Inserted into upper third of medial surface of tibia
• Anterior to gracillis and semitendinosus, as part of the pes anserinum
• Separated by tibial intertendinous bursa
• Supplied by femoral nerve
Sartorius MOB TCD

Adductor Muscles
• Adductor longus • Adductor brevis • Portion of adductor
Magnus• Gracilis• Supplied by obturator
Nerve L2,3,4• Act with lower abdominals
to stabilise the pelvis
MOB TCD

Adductor Origins
lateral medial
inferior
MOB TCD

Adductor Longus
• Tendinous origin, pubic body, has a variable shape
• Inserted into medial lip of linea aspera
• Most frequently torn at proximal musculo-tendinous junction, which varies
• Or may tear at teno-periosteal junction
• Site of junction varies, medial or lateral, may be longer in some
• Anterior division obturator nerve
MOB TCD

Adductor Brevis
• Origin lower portion of body of pubis
• Inferior pubic ramus• Inserted into lower half of the
pectineal line • Upper half of the linea
aspera• Deep to adductor longus• Separates two divisions of
obturator nerve• Anterior division supplies it
MOB TCD

Adductor Magnus
• Triangular area of ischial tuberosity• Ramus of ischium and inferior
ramus of pubis• Inserted into medial lip of gluteal
tuberosity• Lateral lip of linea aspera• Medial supracondylar line• Adductor tubercle• Hiatus for popliteal vessels• Origin of oblique fibres of vastus medialis• Post division obturator nerve• Sciatic nerve below hiatus for femoral vessels
MOB TCD

Gracilis
• Gracilis is the weakest, most medial and superficial of the adductors
• Gracilis is the only one that crosses the knee joint
• It arises from a thin aponeurosis, lower half of the body and the inferior ramus of the pubis and part of the ramus of the ischium. It is strap like above
• It ends in a rounded tendon, inserted into the upper portion of the medial surface of the tibia between the sartorius and the semitendinosus
MOB TCD

• Gracilis is separated from sartorius and the semitendinosus by the tibial intertendinous bursa (pes anserinum)
• Gracilis is usually supplied by the anterior division of the obturator nerve, L2, 3, 4
• It adducts the hip and flexes and medially rotates the leg
Gracilis MOB TCD

The Tibial Intertendinous Bursa
• Inflammation of the tibial intertendinous bursa
• Must be differentiated from injury to the lower attachment of the medial collateral ligament of the knee
MOB TCD

Adductors
• The adductors adduct the femur and help to stabilise and counteract the rotation of the pelvis, particularly during the double support
• When the anterior limb is flexed and the posterior limb is extended
Carlsoo, 1972
MOB TCD

Adductor Muscle - Tendon StrainAdductor Muscle - Tendon Strain
Common in soccer is adductor muscle-tendon strain. Be aware of:
• Rectus Femoris• Sartorius• Rectus Abdominus• Pectineus• Adductor Magnus• Gracilis
MOB TCD

• If the hip is flexed, the adductors rotate the hip medially
• When the hip is extended the adductors can laterally rotate
• They can also flex the extended hip and extend the flexed hip
• At the beginning of the swing phase of walking they work synergistically with the iliopsoas
• At the end of the swing phase, they work with the hamstrings, which contract to prevent further hip flexion
Adductors MOB TCD

Pectineus
• The pectineus muscle is a short flat muscle, which forms part of the floor of the femoral triangle
• It arises from the anterior aspect of the superior ramus of the pubic bone and the fascia covering it
• It is inserted into the upper half of a line drawn from the lesser trochanter to the linea aspera and lies posterior to the femoral sheat
• It is supplied by a branch from the femoral nerve or the accessory obturator (L2, 3)
MOB TCD

• The pectineus is mainly a flexor of the thigh and a weak adductor
• There may occasionally be some fusion between the adductor longus and brevis or with the pectineus
• Doubling of the origin of the adductor longus or brevis may also take place
Pectineus MOB TCD

Psoas Major
Origin• Intervertebral discs, adjoining
bodies of T12-L5 vertebrae• Medial half, anterior aspect of five
lumbar transverse processes• Fibrous arches on the sides of the
bodies of the four upper four lumbar vertebrae, over four lumbar arteries
• Inserted into the lesser trochanter of femur
• Nerve L2,3,4
MOB TCD

Psoas Minor
• Minor • Origin • T12 –L1• Insertion• Arcuate line• Iliopubic eminence
MOB TCD

Psoas Major Muscle and Fascia
• The psoas is covered by fascia which is attached medially to the lumbar vertebrae
• To the fibrous arches • Medially along the brim of the
pelvis to the arcuate and pectineal lines
• Laterally, the fascia is attached to the transverse processes of the lumbar vertebrae
• Medial Arcuate Ligament is a thickening of fascia over the Psoas
MOB TCD

Psoas
• Flexes the hip when acting from above
• Lumbar plexus is formed inside the substance of psoas
• A strain of the psoas muscle may be the cause of chronic groin pain, and you must take care not to mistake it for an adductor strain
MOB TCD

Psoas bursa, between psoas and capsule of hip joint, may communicate with the synovial membrane of the joint
Psoas abscess will present in the groin
Psoas MOB TCD

The Iliopsoas
• The iliacus• Origin: iliac fossa and iliac crest• Inserted into the lateral aspect of the psoas
and into the femur below the lesser trochanter• Nerve L2,3 • The iliopsoas is an active postural or stabilising muscle
of the hip which helps to prevent hyperextension of the hip while standing
• Acting from above, the iliopsoas flexes the hip and may be either a medial or a lateral rotator; acting from below, psoas flexes spine
MOB TCD

• In walking, the iliopsoas is used to start swinging the leg forwards
• On level ground the leg moves forwards like a pendulum to complete the swing
• Stronger contraction of the iliopsoas is required when running or walking up a hill
• When climbing stairs, the iliopsoas lifts the leg and places the foot on the stair above
The Iliopsoas MOB TCD

• When preparing to stand from sitting, the iliopsoas pulls the trunk forwards as the femur is fixed
• The trunk leans forwards and, before standing upright, the centre of gravity of the trunk moves over the feet
• In sitting up from lying, the iliopsoas pulls on the pelvis and the lower vertebrae in order to pull the trunk up
Tyldesley & Grieve, 1989
The Iliopsoas MOB TCD

• Running with the legs lifted high, helps to develop the iliopsoas
• The iliopsoas is also used in the downbeat of freestyle swimming
• The iliopsoas is the main muscle involved in straight leg sit-ups
• These, however, should never be done as they put stress on the lumbar vertebrae and do nothing for the abdominal muscles
The Iliopsoas MOB TCD

“BMJ Publishing Group Limited (“BMJ Group”) 2012. All rights reserved.”