Embed Size (px)
Citation preview

WELCOME
Anaesthetic Management of a Patient with HELLP Syndrome

Amenorrhea for 32 weeks H/O convulsion twice Headache for 01 day
Chief Complaints
The patient was admitted to CMH Jessore on 28 July 2016 with the complaints of amenorrhea for 32 weeks with severe headache and convulsions. She was diagnosed as a case of 32 weeks pregnancy with severe IUGR with eclampsia. Since, it was a case of IUGR with serious complications like convulsions developed within 32nd week; hence, it was decided to terminate the pregnancy as the safer option for the mother in an earlier opportunity. After achieving a handsome medical control over convulsions, trials of medical inductions were tried, but unfortunately failed.
History of Present Illness

Subsequently, the patient developed newer complications like scanty of micturition, breathing difficulties and she was found icteric. Since, the patient developed multiple medical problems along with her existing ailment; so, it was decided to shift her to CMH Dhaka by helicopter for advanced management. On 4 Aug 2016, she arrived in CMH Dhaka at about 1330 hrs. Here, she was detected to have developed the HELLP syndrome along with her pregnancy and was decided to undergo emergency Caesarean section under general anaesthesia.
H/O Present Illness (cont..)

She had no previous history of Hypertension, Diabetes Mellitus, Bronchial Asthma or Kidney disease.
She had no ante-natal check up.
Her father was a known case of HTN.
Family History
History of Past Illness
Personal History
Termination of pregnancy was tried at CMH Jessore, but failed. She was managed there with following medications – Tab Alpha-methyl dopa (250 mg, 2 tab 6 hourly) Tab Labetalol (200 mg,1 tab 12 hourly) Tab Misoprostole (100 mcg, 6 hourly) Inj magnesium sulphate (IV @ 6 drops/min for 24
hours) Inj Labetalol (10 mg 8 hourly) Inj Oxytocin (10 units) Inj Dexamethasone (5 mg)
Treatment History
Married for one and half yearsGravida - 01Para - nilLMP – 16 Dec 2015EDD – 23 Sep 2016
Obstetric History
Appearance - Anxious & restless Jaundice - ++ Anaemia - +++ Oedema - Generalized +++ Pulse - 110 beats/min BP - 160/100 mmHg RR - 28 breaths/min Temp - 98.4 F⁰
General Examination
Cardio Vascular System: Pulse rate - 110 beats/min, regular BP - 160/100 mmHg Respiratory System: Vesicular breath sound RR - 28 breaths/min
Breath sound - diminished on left lower zone Percussion note - stony dull on left lower
zone No added sound Central Nervous System: No abnormality detected
Systemic Examination
Abdominal Examination: Symphysio-fundal height
was corresponding to 24 weeks of pregnancy
Foetal heart sound- not audible
Foetal movement was absent
Systemic Examination (cont…)
Primi Gravida of 32 weeks of pregnancy with eclampsia with IUGR and HELLP syndrome
Provisional Diagnosis
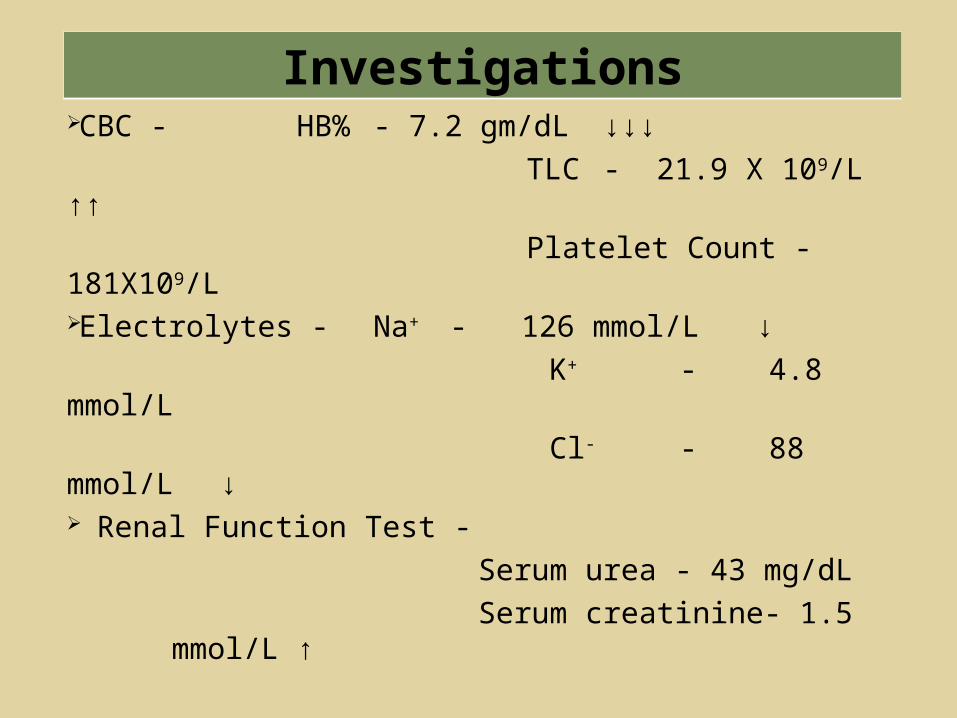
CBC - HB% - 7.2 gm/dL ↓↓↓ TLC - 21.9 X 109/L ↑↑ Platelet Count - 181X109/LElectrolytes - Na+ - 126 mmol/L ↓ K+ - 4.8 mmol/L Cl- - 88 mmol/L ↓ Renal Function Test -
Serum urea - 43 mg/dL Serum creatinine- 1.5 mmol/L ↑
Investigations
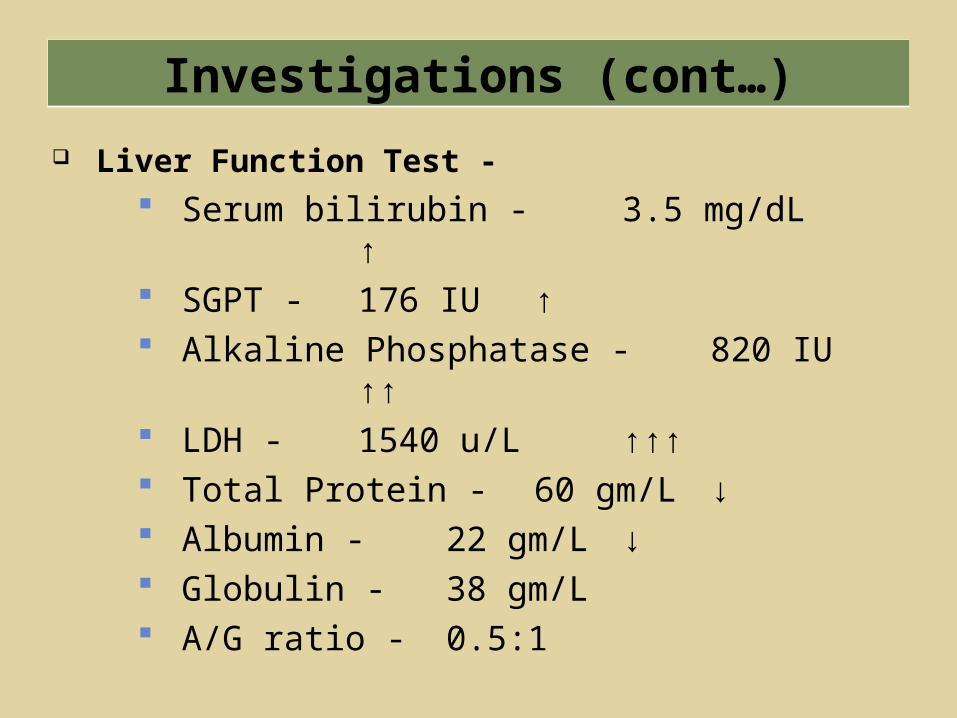
Liver Function Test - Serum bilirubin - 3.5 mg/dL ↑ SGPT - 176 IU ↑ Alkaline Phosphatase - 820 IU ↑↑ LDH - 1540 u/L ↑↑↑ Total Protein - 60 gm/L ↓ Albumin - 22 gm/L ↓ Globulin - 38 gm/L A/G ratio - 0.5:1
Investigations (cont…)
Coagulation profile - APTT - Patient 48 sec Control 28 sec PT - Patient 16 sec Control 12 sec Index - 75.60 Ratio - 1.33 INR - 1.34
Investigations (cont…)

Urine routine examination - Appearance – Turbid Reaction – Acidic Albumin - + RBC – Numerous WBC – 2-3 / HPA Epithelial cell - 8-10 / HPA
Investigations (cont…)
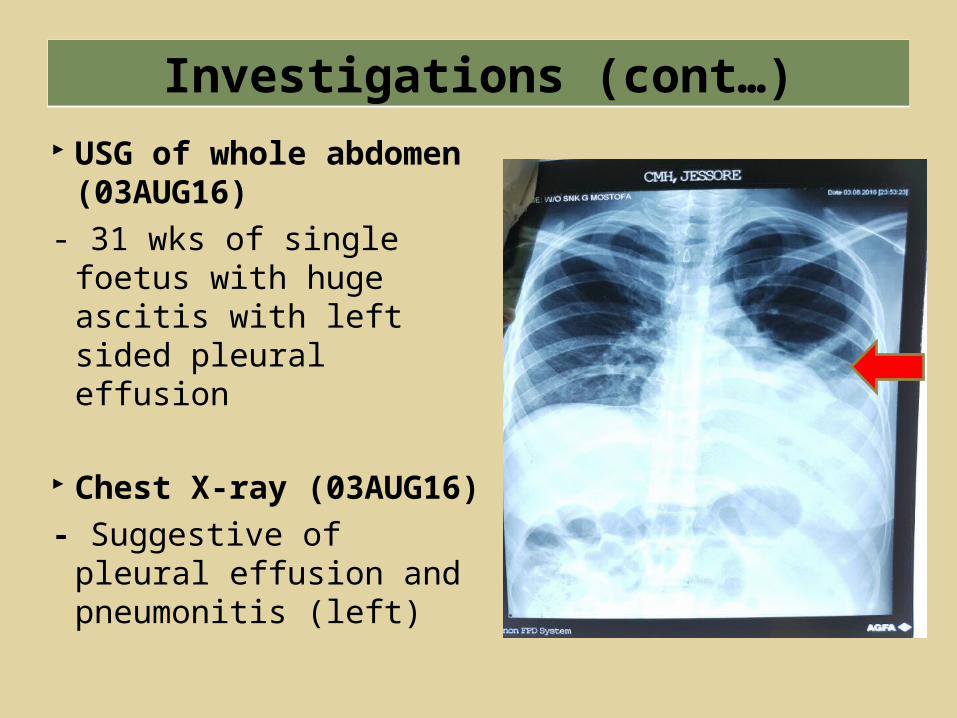
USG of whole abdomen (03AUG16)
- 31 wks of single foetus with huge ascitis with left sided pleural effusion
Chest X-ray (03AUG16)- Suggestive of pleural
effusion and pneumonitis (left)
Investigations (cont…)
A 20-year-old female (Wife of a Snk) got admitted at CMH Jessore on 28 Jul 2016 with the complaints of amenorrhea for 32 weeks, headache and convulsion. She was diagnosed as a case of 32 weeks pregnancy with eclampsia with IUGR associated with anaemia, ascites and jaundice. Subsequently, the patient developed dyspnoea and oliguria. Pharmacological termination of pregnancy was tried there, but failed. On 4 Aug 2016, she was evacuated to CMH Dhaka by helicopter at 1330 hours.
Salient Features
The patient was received at E & C of CMH Dhaka with dyspnoea, severe anaemia, jaundice, generalised oedema and raised blood pressure. On examination, there was diminished breath sound and stony dull on percussion over the lower zone of the left lung. Her abdominal examination revealed severe IUGR with no foetal movement and heart sounds. Investigations showed significant reduction of hemoglobin, coagulation disorder, electrolyte imbalance and hepatic & renal dysfunction.
Salient Features (cont…)
32 weeks pregnancy with HELLP Syndrome with IUD and Acute Kidney Injury
Final Diagnosis
ANAESTHETIC MANAGEMENT

The patient was severely anaemic and having altered coagulation profile.
She was moderately icteric and having very high liver enzyme levels & low serum protein.
Patient developed AKI. She developed pleural effusion and having
respiratory distress. Patient was accepted as ASA grade III (E) for
general anesthesia.
Pre-anaesthetic Assessment
Central venous catheter & an arterial line were established for invasive haemodynamic monitoring.
Catheterization of the urinary bladder was also done.
The patient was connected with multi parameter monitor.
Inj Metoclopromide 10 mg, Inj Ranitidine 50 mg IV was administered.
Pre-operative Preparation
Rapid Sequence Induction (RSI) protocol was followed.
Thiopental sodium (5 mg/kg) Fentanyl (1.5 mcg/kg) Suxamethonium 100 mg
was given and patient was intubated under direct laryngoscopic view and was put on controlled ventilation.
Induction and Intubation
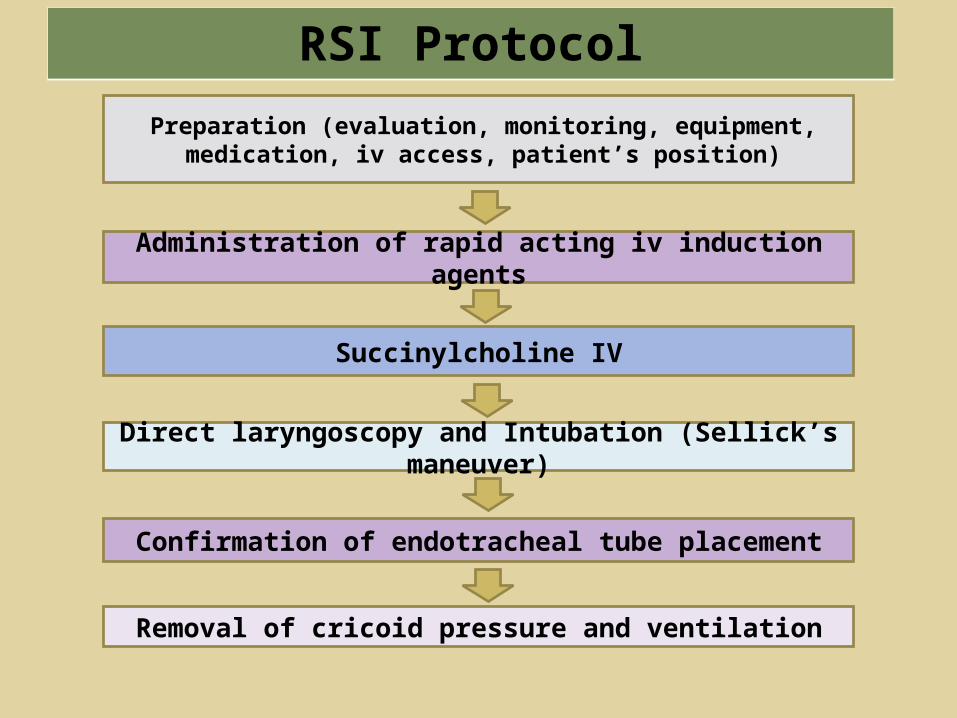
Preparation (evaluation, monitoring, equipment, medication, iv access, patient’s position)
Direct laryngoscopy and Intubation (Sellick’s maneuver)
Administration of rapid acting iv induction agents
Succinylcholine IV
Confirmation of endotracheal tube placement
Removal of cricoid pressure and ventilation
RSI Protocol
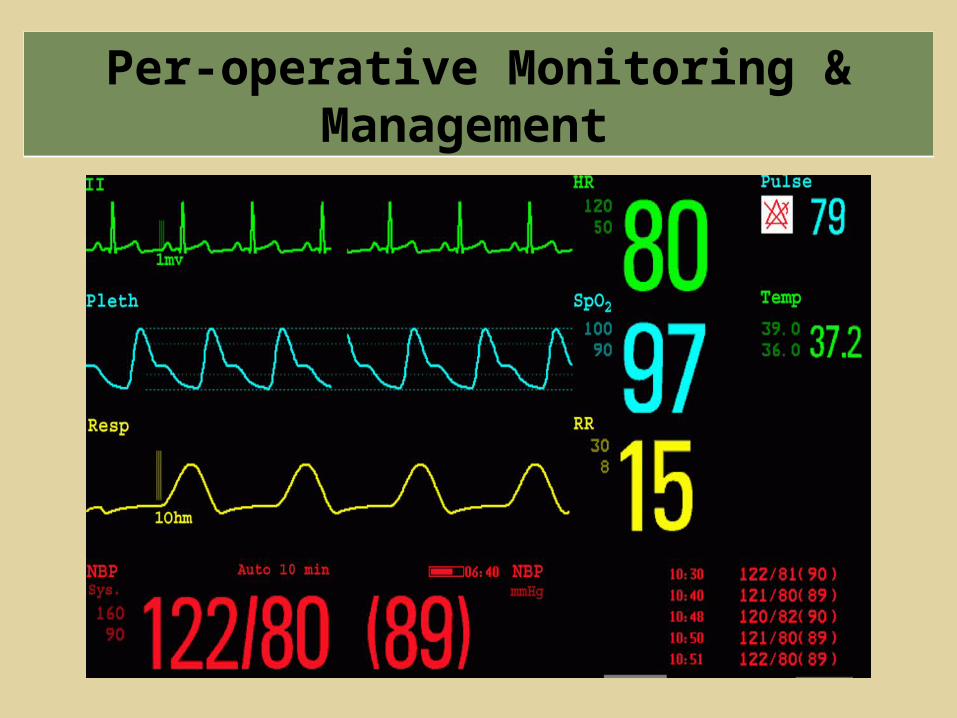
Per-operative Monitoring & Management

Anaesthesia was maintained with Inj Atracurium, Oxygen and nitrous oxide.
Analgesia was provided by using Fentanyl. Inj GTN and Inj Labetalol were used to control
BP. Duration of Operation: 1 hour 30 min
Per-operative Management Input Output
Hartman’s solution-1500 ml Blood loss - 1000 ml
5% Dextrose in Aqua-500 ml Urine output – 145 ml
Whole blood- 2 units
As the patient had multi-organ dysfunction, unstable haemodynamic condition and loss of significant amount of blood with pre-existing severe anaemia along with massive volume replacement.So, considering her critical clinical state and impending instabilities…Elective post-operative ventilation was planned and the patient was shifted to critical care centre (CCC).
Reversal and Extubation

Patient was severely anaemic and having altered coagulation profile.
She was moderately icteric and having very high liver enzyme levels & low serum protein
Patient developed AKI She developed pleural effusion and having
respiratory distress She was not kept NPO Having severe metabolic acidosis (pH 6.9) She was carrying a dead baby
Anaesthetic Challenges (for 1st Op)

On 04 Aug 1600 hours, the patient’s condition was - On ventilator (PSIMV mode)Pulse - 90 bpmBP - 150/90 mmHg (Labetolol & Dobutamine infusion)Abdominal girth were increased (10 cm).Massive HaematuriaUSG of whole abdomen revealed moderate intra-peritoneal collectionAn urgent Medical Board was held and decided to perform Emergency Laparotomy at 2100 hrs.
Re-Laparotomy (2nd operation)

Investigation findings: Hb% - 10.5 gm/dLPlatelet count - 185X109/LSerum urea - 43.48 mg/dlSerum creatinine - 2.10 mg/dlSerum bilirubin - 4.04 mg/dLALT - 118 u/LAST - 230 u/LALP - 599 u/LLDH - 1726 u/LD-dimer - PositiveINR - 2.36
VBG at 1820 hours:pH - 6.8PCO2- 45.4
PO2 - 85.4HCO3
- - 7.6 mmol/lBE - 28 mmol/lNa+ - 129.7 mmol/lK+ - 4.97 mmol/lCl- - 95.4 mmol/lLactate - 5.0 mmol/lSvO2 -81 %
Re-Laparotomy (2nd operation)
Considering the aforementioned critical findings, the patient was accepted as ASA Grade- III(E) for exploratory re-laparotomy.
She was prepared & managed by the Senior anaesthesiologists.
CVP and Invasive BP were monitored continuously. Anaesthesia was maintained by Inj Fentanyl, Inj
Vecuronium, Oxygen, Nitrous oxide. Duration of Operation: 2100-2200 (1 hour) After operation, elective post-operative ventilation
was planned and the patient was shifted to CCC.
Re-Laparotomy (2nd operation)
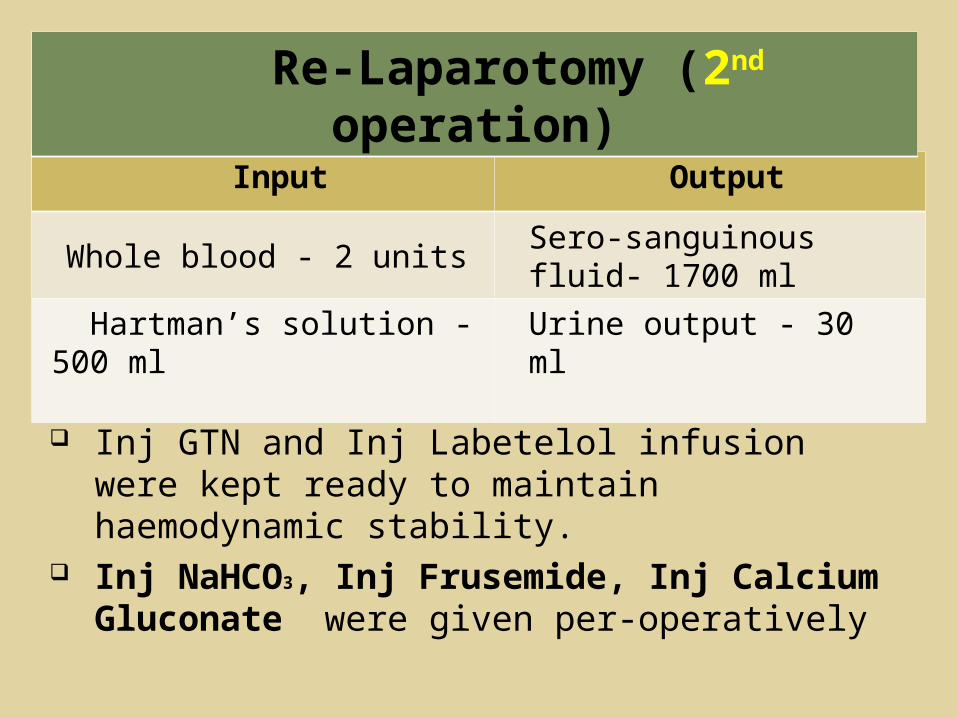
Inj GTN and Inj Labetelol infusion were kept ready to maintain haemodynamic stability.
Inj NaHCO3, Inj Frusemide, Inj Calcium Gluconate were given per-operatively
Input Output
Whole blood - 2 units Sero-sanguinous fluid- 1700 ml
Hartman’s solution - 500 ml Urine output - 30 ml
Re-Laparotomy (2nd operation)
Anaesthetic challengesA critical patient was undergoing 2nd operation 5 hours after the 1st one. The patient was in severely metabolic acidosis state.Her serum creatinine was high and having severe hematuria.Her serum electrolytes and coagulation profile were deranged.Her liver function tests were deranged.
Re-Laparotomy (2nd operation)
On 05 Aug 16, the patient’s condition was –On ventilator (PSIMV mode)Pulse - 90 beats/minBP - 130/80 mmHgHaemodialysis was done at 0100 hours (by SLED) [Sustained Low Efficiency Dialysis]
Re-Laparotomy 3rd Operation
The patient received… Packed Cell - 2 units FFP - 2 units
Drain bag collection was - 1200 ml of blood. At 1900 hours, her Hb% decreased to 4.6 gm/dl. So, an emergency Medical Board was held and
decided to perform re-laparotomy. Re-laparotomy and exploration of peritoneal
cavity was done at 2130 hrs on 1st POD.
Re-Laparotomy 3rd Operation
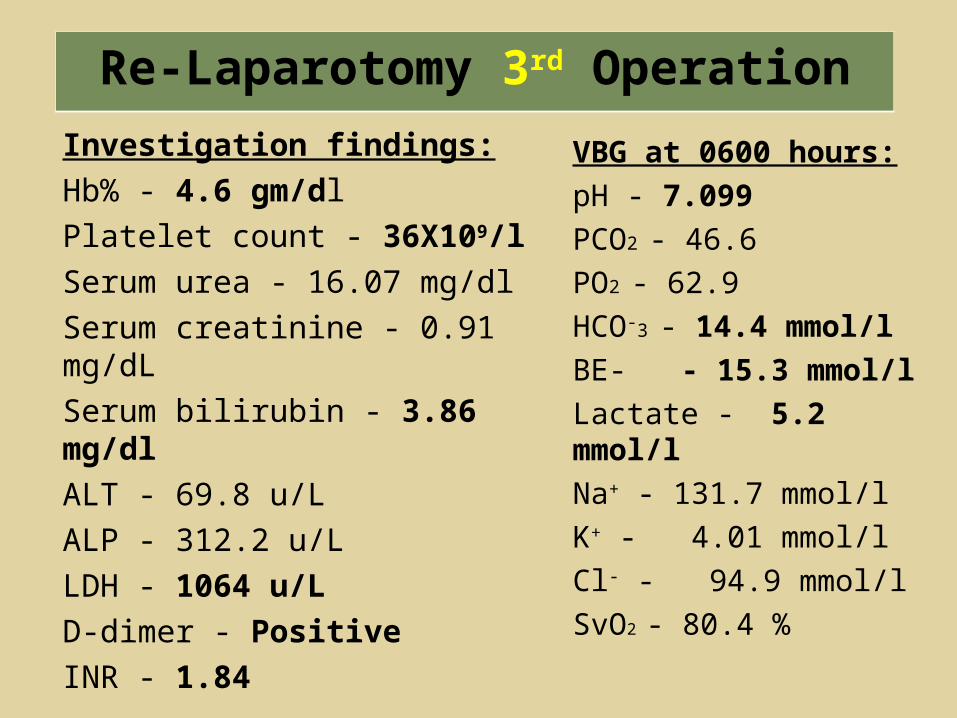
Investigation findings:Hb% - 4.6 gm/dlPlatelet count - 36X109/lSerum urea - 16.07 mg/dlSerum creatinine - 0.91 mg/dLSerum bilirubin - 3.86 mg/dlALT - 69.8 u/LALP - 312.2 u/LLDH - 1064 u/LD-dimer - PositiveINR - 1.84
VBG at 0600 hours:pH - 7.099PCO2 - 46.6PO2 - 62.9HCO-3 - 14.4 mmol/lBE- - 15.3 mmol/lLactate - 5.2 mmol/lNa+ - 131.7 mmol/lK+ - 4.01 mmol/lCl- - 94.9 mmol/lSvO2 - 80.4 %
Re-Laparotomy 3rd Operation
The patient was labeled as ASA Grade- IV(E) for exploratory re-re-laparotomy.
Patient was prepared and managed by the Senior anaesthesiologists.
An arterial line was re-established to monitor Invasive BP and central venous pressure was monitored continuously.
Re-Laparotomy 3rd Operation
Input Output
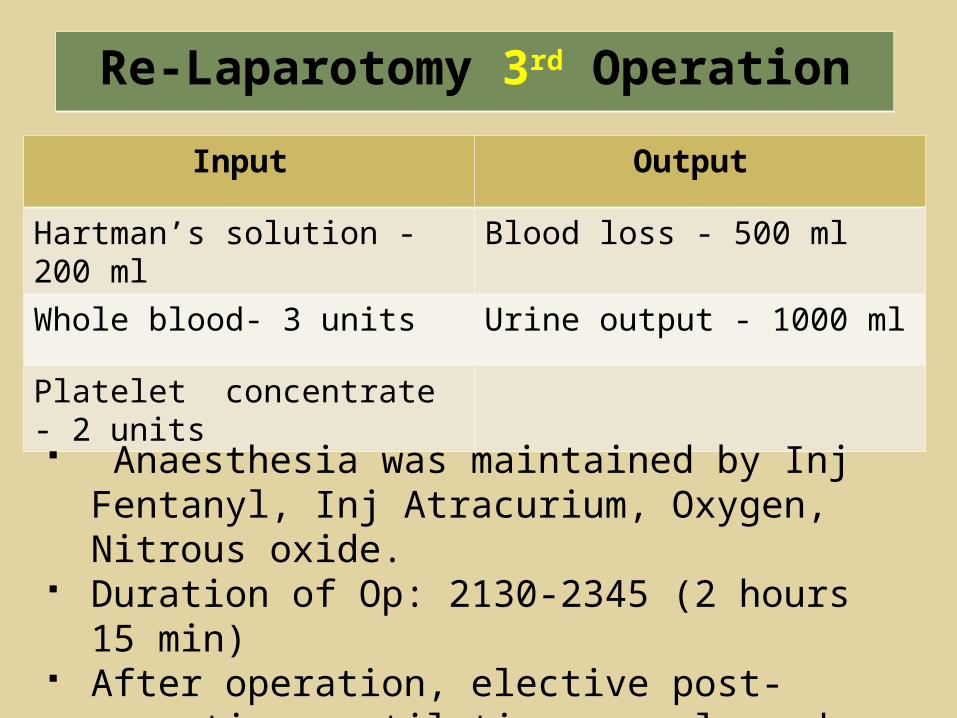
Hartman’s solution - 200 ml Blood loss - 500 ml
Whole blood- 3 units Urine output - 1000 ml
Platelet concentrate - 2 units
Anaesthesia was maintained by Inj Fentanyl, Inj Atracurium, Oxygen, Nitrous oxide.
Duration of Op: 2130-2345 (2 hours 15 min) After operation, elective post-operative ventilation
was planned and patient shifted to CCC.
Re-Laparotomy 3rd Operation
Anaesthetic challengesA moribund patient was undergoing 3rd operation on the 1st PODSeverely anaemic (Hb% - 4.6 gm/l) Patient was in severely metabolic acidotic state (pH - 7.099).Her renal function was impaired and having severe haematuria.Her electrolytes and Coagulation profile (platelet-36X109) were deranged.Her liver function test was deranged.
Re-Laparotomy 3rd Operation

At CCC, the patient remained on mechanical ventilation with multiple supports.
After getting advanced intensive care, she was extubated on 13 Aug 2016 (8th POD).
Post-operative Management
Discussion
The acronym HELLP was coined by Weinstein in 1982 to describe a syndrome consisting of Hemolysis, Elevated Liver enzymes, and Low Platelet count.
It is a syndrome that is characterized by hepatic endothelial disruption followed by platelet activation, aggregation and consumption, ultimately resulting in ischemia and hepatocyte death.
Introduction
HELLP syndrome is a life-threatening obstetric complication usually considered to be a variant of pre-eclampsia. Both conditions usually occur during the later stages of pregnancy or sometimes after childbirth.
Incidence: 0.2% to 0.6% of all pregnancy and the maternal mortality rate is 25%.
Introduction
The elevated liver enzymes are thought to be secondary to obstruction of hepatic blood flow by fibrin deposition in the sinusoids.
This obstruction leads to peri-portal necrosis and in severe cases intra-hepatic haemorrhage, subcapsular haematoma formation or hepatic rupture.
Pathophysiology
Haemolysis is due to microangiopathic haemolytic anaemia. Red cells become fragmented as they pass through small vessels with endothelial damage and fibrin deposits, results in increase in bilirubin levels and LDH.
Decreased platelet count is due to their increased consumption. Platelets are activated, and adhere to damaged vascular endothelial cells, resulting in increased platelet turnover with shorter lifespan.
Pathophysiology (cont..)
Placental abruption Pulmonary edema Disseminated intravascular coagulation (DIC) Adult Respiratory distress syndrome Ruptured liver hematoma Acute renal failure Intrauterine Growth retardation (IUGR) Cerebral oedema and hemorrhage
Complications of HELLP syndrome
Special Considerations for Anaesthetic Management
Coagulopathy: Platelet count <1,00,000/mm3 – regional procedures are to be avoided.
RSI – when GA is considered. Attenuation of Sympathetic responses to
endotracheal intubation. Availability of difficult intubation cart and drugs Compulsory Invasive monitoring Proactive management of haemodynamic
alterations by vasodilators &/or vasopressors (whenever necessary)
Special Considerations for Anaesthetic Management
Meticulous management of volume losses In time replacement of Blood and Plasma Prevention of Cerebral oedema/haemorage Renal protection Prevention of further hepatic injuries Last, but not the least…
It’s an issue of two lives, both of whom are seriously endangered and compromised.
It demands urgent management – always.
Special Considerations for Anaesthetic Management (cont..)
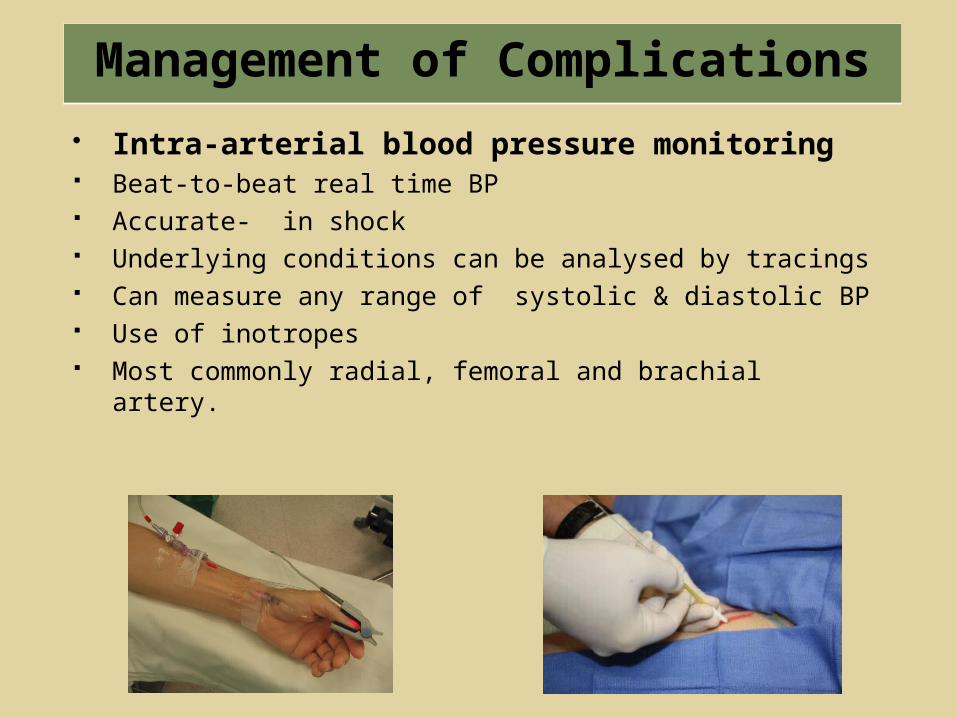
Intra-arterial blood pressure monitoring Beat-to-beat real time BP Accurate- in shock Underlying conditions can be analysed by tracings Can measure any range of systolic & diastolic BP Use of inotropes Most commonly radial, femoral and brachial artery.
Management of Complications

Management of Complications ( cont..)
Mechanism of Intra-arterial blood pressure monitoring
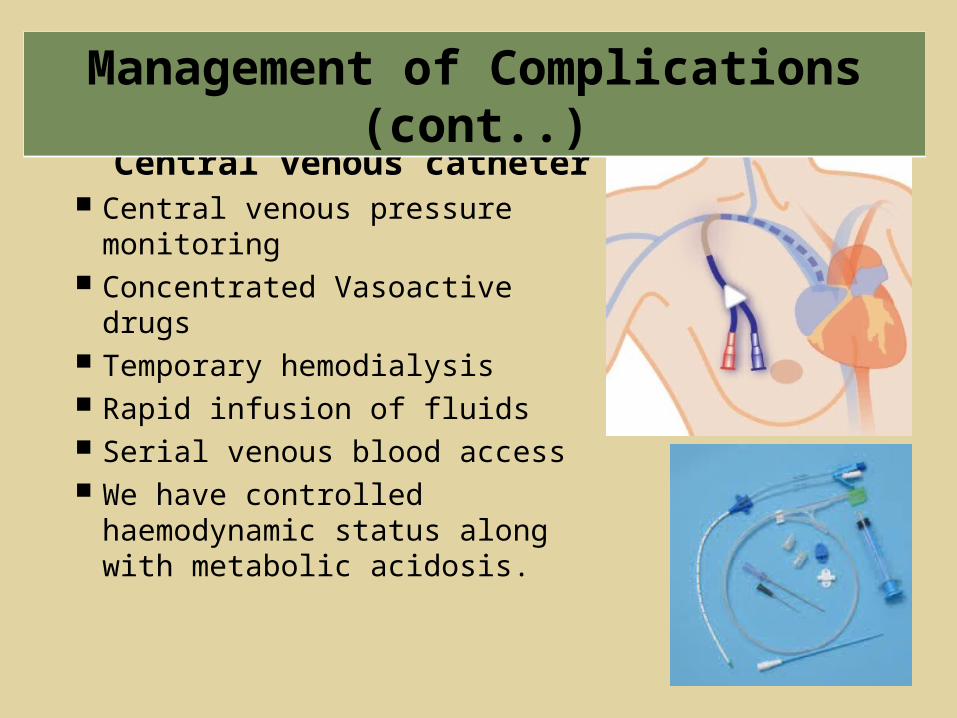
Central venous catheter Central venous pressure
monitoring Concentrated Vasoactive drugs Temporary hemodialysis Rapid infusion of fluids Serial venous blood access We have controlled
haemodynamic status along with metabolic acidosis.
Management of Complications (cont..)

Acute renal failure Intake- output was maintained srtictly Diuretics (Frusemide), renal vasodilators (Dopamine)
were used. Haemodialysis was done by using modified SLED
Liver injury Hepatotoxic anaesthetic agents were avoided Drugs with properties of self-degradation were used
Management of Complications (cont..)
Choice of anaesthesia depends on… Expertise of anaesthesiologist Patients condition Foetal condition Urgency of the procedure Patients desire to be awake during the
procedure
Choice of Anaesthesia
Invasive monitoring and restoration of haemodynamical status of the patient
To manage metabolic acidosis state. Altered coagulation profile. Deranged liver function. Severe respiratory distress
General Anaesthesia

Subarachnoid block - for this case it was not chosen because it likely to have severe hypotension due to sympathetic blockade.
Epidural Block - this might be the choice for the patient but avoided due to the risk for epidural haematoma formation.
Regional Anaesthesia
HELLP syndrome can be an extremely serious and complex multisystem disorder involving much more than just eclampsia. Special considerations in obstetric and anaesthetic management are necessary, to minimize the morbidity and mortality are associated with this syndrome and its complications.
Conclusion
Questions