Embed Size (px)
Citation preview
�0�JBMS Journal of the Bahrain Medical Society, July 2008 Vol 20, No. 3
Designed & layout by:
Queen P.O. Box: �8663- Manama - Kingdom of Bahrain
e-mail: [email protected]
الخالصة
االهداف : لتقييم فعالية االسترشاد بجهاز االشعه ذو الصوره األكثر حده ومثقاب مفصل الورك الديناميكي (9مم) كطريقه جراحيه دنيا في استئصال الورم العظمي شبيه بالعظم عن طريق الجلد في االطراف السفليه عند االطفال والبالغين.
مكان الدراسه : قسم جراحة العظام في مستشفى الجامعه االردنيه - عمان
المواد والطرق : تم عالج 18 من االطفال والبالغين ( 11 ذكور، 7 اناث) عمرهم يتراوح بين 16-4 سنه ومتوسط اعمارهم 12.17 سنه في الفتره الواقعه مابين عام 1999 - 2006 . متوسط فترة المتابعه السريريه (35.37) شهر ( المدى 18-78 ) شهر. حاالت في عظم القصبه. 414 حاله كانت في عظم الفخذ كل المرضى تمت معالجتهم من قبل الباحث االول عن طريق
الجلد تحت المخدر العام باستخدام مثقاب مفصل الورك الديناميكي و جهاز االشعه ذو الصوره األكثر حده.
النتائج: دلت النتائج االوليه شفاء 16 مريض (%88.88) في االسبوع االول عن طريق الثقب مره واحده. احتاج مريضين (%11.11) الثقب مره اخرى بعد اسبوعين نتيجة فشل المثقاب االول أستهداف
موطن نشوء الورم العظمي شبيه بالعظم . المضاعفات تضمنت كسر في عظم القصبه وحالتين تضمنت خدوش جلديه في الساق نتيجة المثقاب. صنفت االستجابه السريريه جيده في كل المرضى اعتمادا” على المتابعه الطويله والمتوسطه.
االستنتاج : أستخدام جهاز االشعه ذو الصوره األكثر حده لتحديد موقع الورم العظمي شبيه بالعظم اثناء العمليه مع استخدام كبديل الطريقه استخدام هذه يمكن قليل. فقدان عظم أمينه وفعاله مع الديناميكي أعطى طريقة شافيه الورك مثقاب مفصل
للتقنيات المعياريه الزالة الورم العظمي شبيه بالعظم. استخدام هذه الطريقه للقصبه يمكن ان يؤدي الى مضاعفات اكثر.
مفتاح الكلمات : الورم العظمي شبيه بالعظم.
Ablation of Osteoid Osteoma of Lower Extremity using Dynamic Hip Screw Drill Freih Odeh Abu Hassan�, F.R.C.S (Eng), F.R.C.S M.B.,BCh. Tarek Nayef Altamimi�, M.B.,BCh,J.P.Orth
Abstract
Objectives: Evaluate the efficacy of Image Intensifier- guidance percutaneous ablation of osteoid osteoma of lower extremity in children and adolescents. using a dynamic hip-screw (DHS) drill pit (9- mm) as a minimally invasive therapy.
Setting: Orthopaedic department at Jordan University Hospital –Amman.
Methods: The Study Started from November 1999 October 2006, Treating 18 children, (eleven males and seven females), with a mean age of 12.17 years (range 4–16 years). The mean follow-up period was 35.37 months (range 18–78 months). There were fourteen lesions in the femur and four in the tibia. All patients were treated percutaneously under Image intensifier guidance by the first author under general anesthesia.
Results: Initial clinical success in the first week was achieved in 88.88% of children (16/18) from drilling once. Two patients 11.11% needed redrilling two weeks later after failure of the first drilling to target the nidus. Complications included one fractured tibia and two skin abrasions over the tibia. At long- and medium term follow-up, all patients were classified to have good clinical response.
Conclusion: The combination of intraoperative localization of osteoid osteoma by image intensifier, using a dynamic hip-screw (DHS) drill, resulted in an efficient, safe, and curative procedure with minimal bone loss. This method can be used as an alternative to the standard techniques for removal of osteoid osteoma. Using the technique for the tibia may be associated with higher incidence of complications
Keywords: Osteoid osteoma, Nidus, Image intensifier, Drilling, DHS drill.
1 Associate Professor of Orthopaedics and Paediatric Orthopaedic Surgery, Jordan University- Amman

�02 JBMS Journal of the Bahrain Medical Society, July 2008 Vol 20, No. 3
Introduction
Osteoid osteoma is a benign bone tumour consisting of an osteoid nidus in a highly vascular connective tissue stroma.1, 2 It accounts for approximately two-to-three per cent of all primary bone neoplasms with a predilection for the major long bones of patients younger than forty years.1,
2 These tumours are painful, and demonstrate characteristic clinical picture and radiographic features. Clinical diagnosis is made with the radiological appearance of a small radiolucent area, known as the nidus, equal to or less than 1.5 cms surrounded by a thick zone of sclerotic bone which is smooth, convex, and homogeneously dense, especially in the cortical bone.1 The traditional treatment of osteoid osteoma consists of surgical en bloc excision.2, 3 but it has a high complication rate.4 Treatment varies from conservative to surgical en bloc excision of the nidus .2, 3, 5 by percutaneous CT-guided excision, 6-8 destruction of the nidus using radiofrequency thermocoagulation, 9-11 or laser photocoagulation. 12, 13 These modalities have been shown
to have many advantages and fewer complications over the traditional en block excision. Most minimal invasive techniques require a special equipments, CT scan and facilities for general anaesthesia for the removal of osteoid osteoma. 2, 5, 7, 11, 13 These facilities are usually available in special centers. We selected to use the commonly available instruments. We have used a minimal invasive percutaneous technique using a dynamic hip-screw (DHS) drill (9 mm) successfully, with the aim of mechanical local destruction of the nidus through a one centimetre incision with minimal bone loss under direct visualization of the image intensifier.
Materials and methods
From November 1999 to Octobar 2006, eighteen consecutive children with osteoid osteoma were treated with an image intensifier-guided percutaneous drilling using a Dynamic Hip Screw drill pit (9-mm). There were eleven males and seven females, with a mean age of 12.17 years (range 4–16 years), and the mean follow-up period was 35.37 months (range 18–78 months).
(Table-1) All patients had typical clinical and radiographic findings of osteoid osteoma. Pre-operative clinical evaluation included detailed medical history, patients’ gender, age, location of the lesion, and thorough clinical examination, pain severity, the response to aspirin or anti-inflammatory drugs, the limitations of function, and daily or recreational activities.All patients had severe pain that usually worsened at night and had taken some analgesics or narcotic injections and at least one course of non-steroidal anti- inflammatory drugs for pain relief. Pre-operative imaging evaluation included standard radiographs, anterioposterior and lateral films.All patients
Figure-1: Plain radiograph of the hip showing well visualized radiolucent nidus in the basal neck of the femur with mild sclerosis
Patient No.
Age (years) Sex Site of the Lesion
Duration of symptoms (months)
Follow-up (months) Approach
1 10 F Femur neck 10 34 Lateral
2 13 M Femur neck 18 43 Lateral
3 10 F Femur neck 10 34 Lateral
4 14 F Femur neck 12 36 Lateral
5 16 M Femur neck 10 66 Lateral
6 16 M Femur neck 16 18 Lateral
7 12 M Femur neck 23 18 Medial
8 15 M Femur neck 13 20 Medial
9 13 F Trochanteric area 15 44 Lateral
10 15 M Trochanteric area 96 48 Lateral
11 5 M Subtrochanteric area 18 20 Medial
12 4 F Proximal third femur 6 22 Lateral
13 10 F Distal third femur 18 42 Medial
14 15 F Distal third femur 24 18 Lateral
15 11 F Proximal tibia 5 42 Anterior
16 14 M Proximal tibia 36 37 Anterior
17 14 M Shaft tibia 6 38 Medial
18 15 M Distal tibia 12 30 Anterior
Table-1 Clinical characteristics of the patients
Freih Odeh Abu Hassan, Tarek Nayef Altamimi
�03JBMS Journal of the Bahrain Medical Society, July 2008 Vol 20, No. 3
had computed axial tomography scans with positive nidus, which allowed precise assessment of its size and location. Six referred patients had bone Scintigraphy and Magnetic Resonance Imaging (MRI) inspite all lesions were very clear on a computed tomography (CT) scan.Follow-up evaluation included clinical examination and a questionnaire, and radiographic evaluation was conducted postoperatively at regular intervals.Three cases required postoperative CT-scans, two due to the persistence of their initial symptoms and one for parents’ request. The delay between referral to hospital and correct diagnosis varied from 5 to 96 months (mean 19.75 months).The diagnosis was clear on the plain radiographs by a well-visualized nidus in thirteenpatients (Figure -1).Three cases of tibial lesions needed a preoperative application of cross skin mark under CT-scan guidance due to excessively dense
bone. All cases had preoperative plan of the direction of the guide wire after proper study of their plain radiograph and CT-scan images for the exact location of the nidus.
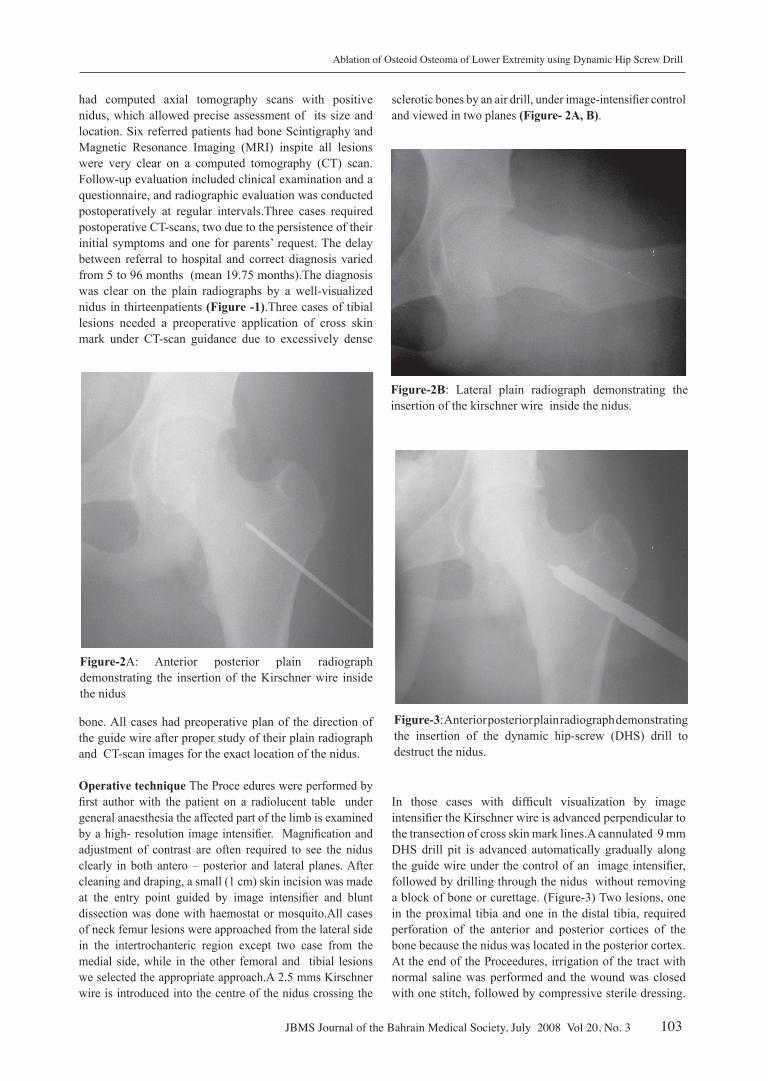
Operative technique The Proce edures were performed by first author with the patient on a radiolucent table under general anaesthesia the affected part of the limb is examined by a high- resolution image intensifier. Magnification and adjustment of contrast are often required to see the nidus clearly in both antero – posterior and lateral planes. After cleaning and draping, a small (1 cm) skin incision was made at the entry point guided by image intensifier and blunt dissection was done with haemostat or mosquito.All cases of neck femur lesions were approached from the lateral side in the intertrochanteric region except two case from the medial side, while in the other femoral and tibial lesions we selected the appropriate approach.A 2.5 mms Kirschner wire is introduced into the centre of the nidus crossing the
sclerotic bones by an air drill, under image-intensifier control and viewed in two planes (Figure- 2A, B).
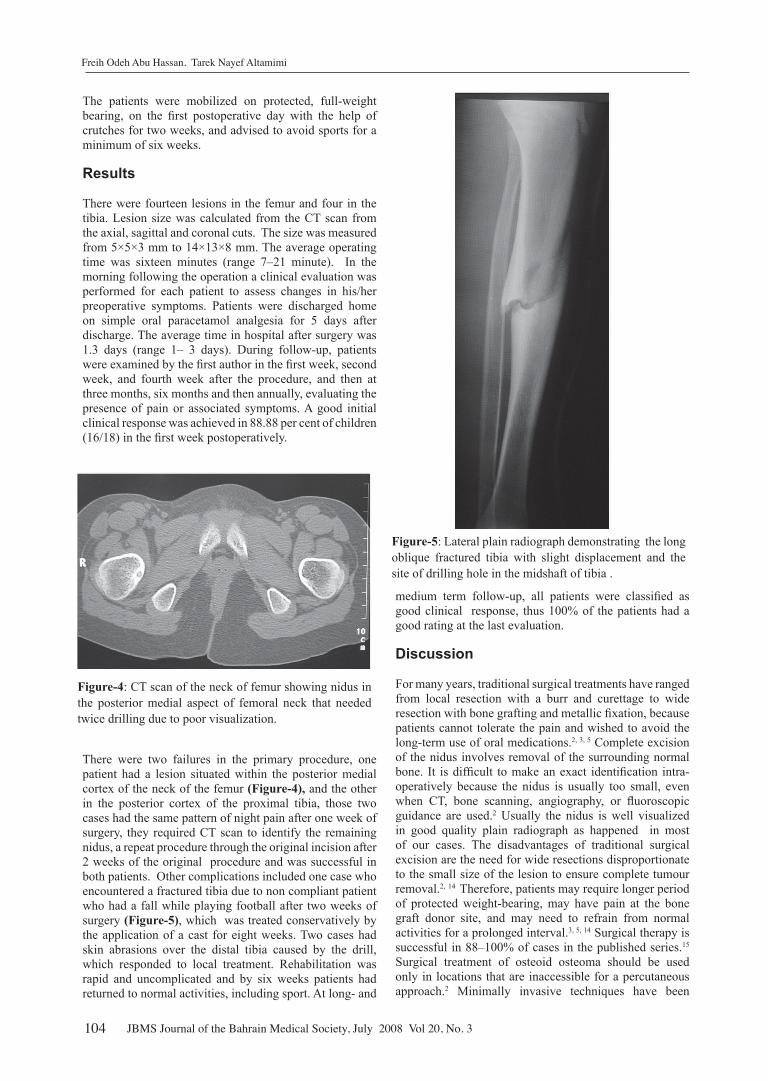
In those cases with difficult visualization by image intensifier the Kirschner wire is advanced perpendicular to the transection of cross skin mark lines.A cannulated 9 mm DHS drill pit is advanced automatically gradually along the guide wire under the control of an image intensifier, followed by drilling through the nidus without removing a block of bone or curettage. (Figure-3) Two lesions, one in the proximal tibia and one in the distal tibia, required perforation of the anterior and posterior cortices of the bone because the nidus was located in the posterior cortex. At the end of the Proceedures, irrigation of the tract with normal saline was performed and the wound was closed with one stitch, followed by compressive sterile dressing.
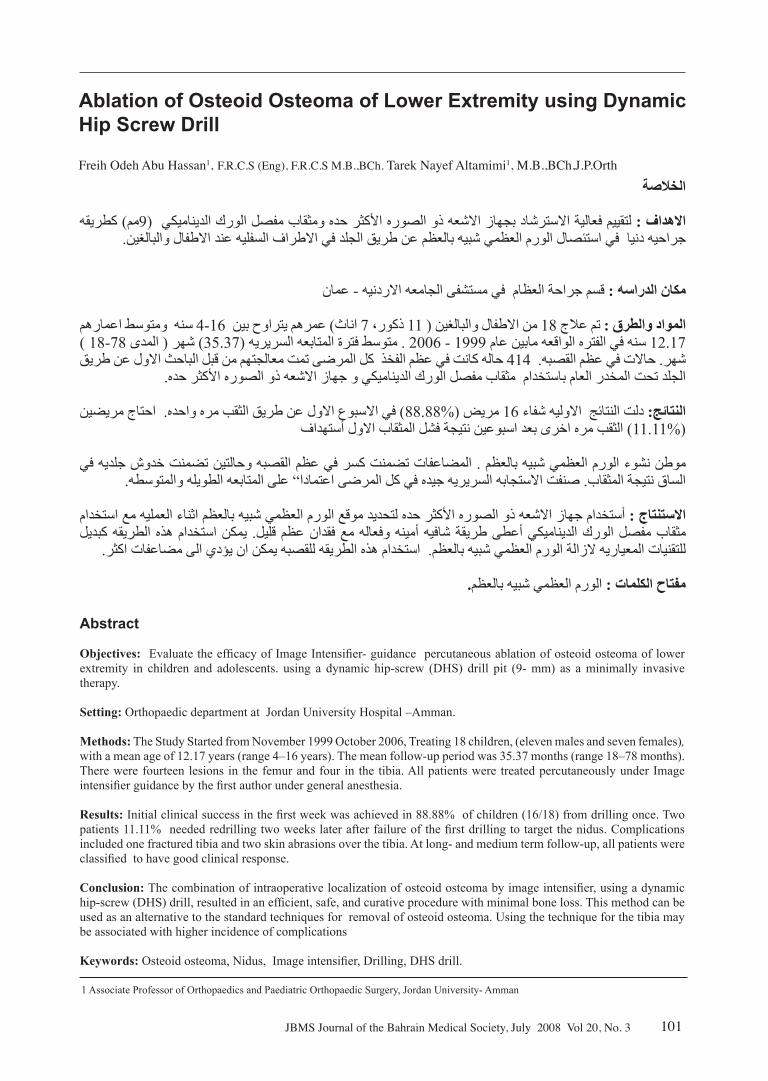
Figure-2A: Anterior posterior plain radiograph demonstrating the insertion of the Kirschner wire inside the nidus
Figure-2B: Lateral plain radiograph demonstrating the insertion of the kirschner wire inside the nidus.
Figure-3: Anterior posterior plain radiograph demonstrating the insertion of the dynamic hip-screw (DHS) drill to destruct the nidus.
Ablation of Osteoid Osteoma of Lower Extremity using Dynamic Hip Screw Drill
�04 JBMS Journal of the Bahrain Medical Society, July 2008 Vol 20, No. 3
The patients were mobilized on protected, full-weight bearing, on the first postoperative day with the help of crutches for two weeks, and advised to avoid sports for a minimum of six weeks. Results
There were fourteen lesions in the femur and four in the tibia. Lesion size was calculated from the CT scan from the axial, sagittal and coronal cuts. The size was measured from 5×5×3 mm to 14×13×8 mm. The average operating time was sixteen minutes (range 7–21 minute). In the morning following the operation a clinical evaluation was performed for each patient to assess changes in his/her preoperative symptoms. Patients were discharged home on simple oral paracetamol analgesia for 5 days after discharge. The average time in hospital after surgery was 1.3 days (range 1– 3 days). During follow-up, patients were examined by the first author in the first week, second week, and fourth week after the procedure, and then at three months, six months and then annually, evaluating the presence of pain or associated symptoms. A good initial clinical response was achieved in 88.88 per cent of children (16/18) in the first week postoperatively.
There were two failures in the primary procedure, one patient had a lesion situated within the posterior medial cortex of the neck of the femur (Figure-4), and the other in the posterior cortex of the proximal tibia, those two cases had the same pattern of night pain after one week of surgery, they required CT scan to identify the remaining nidus, a repeat procedure through the original incision after 2 weeks of the original procedure and was successful in both patients. Other complications included one case who encountered a fractured tibia due to non compliant patient who had a fall while playing football after two weeks of surgery (Figure-5), which was treated conservatively by the application of a cast for eight weeks. Two cases had skin abrasions over the distal tibia caused by the drill, which responded to local treatment. Rehabilitation was rapid and uncomplicated and by six weeks patients had returned to normal activities, including sport. At long- and
medium term follow-up, all patients were classified as good clinical response, thus 100% of the patients had a good rating at the last evaluation.
Discussion
For many years, traditional surgical treatments have ranged from local resection with a burr and curettage to wide resection with bone grafting and metallic fixation, because patients cannot tolerate the pain and wished to avoid the long-term use of oral medications.2, 3, 5 Complete excision of the nidus involves removal of the surrounding normal bone. It is difficult to make an exact identification intra-operatively because the nidus is usually too small, even when CT, bone scanning, angiography, or fluoroscopic guidance are used.2 Usually the nidus is well visualized in good quality plain radiograph as happened in most of our cases. The disadvantages of traditional surgical excision are the need for wide resections disproportionate to the small size of the lesion to ensure complete tumour removal.2, 14 Therefore, patients may require longer period of protected weight-bearing, may have pain at the bone graft donor site, and may need to refrain from normal activities for a prolonged interval.3, 5, 14 Surgical therapy is successful in 88–100% of cases in the published series.15 Surgical treatment of osteoid osteoma should be used only in locations that are inaccessible for a percutaneous approach.2 Minimally invasive techniques have been
Figure-4: CT scan of the neck of femur showing nidus in the posterior medial aspect of femoral neck that needed twice drilling due to poor visualization.
Figure-5: Lateral plain radiograph demonstrating the long oblique fractured tibia with slight displacement and the site of drilling hole in the midshaft of tibia .
Freih Odeh Abu Hassan, Tarek Nayef Altamimi

�05JBMS Journal of the Bahrain Medical Society, July 2008 Vol 20, No. 3
developed to match the tissue damage to the small size of the lesion. Different percutaneous techniques have been described as alternative therapeutic options: percutaneous resection under CT-guided radiofrequency ablation; and laser photocoagulation.6, 8, 9, 10, 12 The advantages of these minimally invasive techniques include the immediate verification of complete nidus removal and rapid relief of symptoms after nidus excision.7, 8, 11, 13 Many current minimally invasive methods needs special tools, instruments, anesthesia machine in the CT room and set up system, which may not be present in each hospital.
Our technique a part from being minimally invasive, simple and does not require special set up system, is performed by general orthopaedist. This technique has been effective, with a good clinical response in 88.23 per cent of cases from the first drilling, and 100 per cent from the second drilling. These results are comparable with other minimal invasive methods. 5, 7, 8, 11, 13 There was one fracture in our series due to non-compliance to strict non-sport activity for six weeks postoperatively. The main disadvantage of this technique is the lack of sufficient material for pathological examination but this disadvantage should not be viewed as a major insufficiency of the method, especially as this is even observed after surgical excision and other minimal invasive surgical procedures.3, 4, 8, 10, 12 On the other hand, histological confirmation with minimal-access techniques is not crucial as appropriate diagnosis can be made on clinical grounds reinforced by imaging techniques.3, 9, 16,17 Other disadvantages is the limitation of their use on the spine, and small-bone lesions owing to the risk of a large drill hole, difficult localization of the nidus under image intensifier and the risk of thermal injury to neural tissue and this is applicable to other percutaneous resection techniques.6-8 The patient needs to use crutches as a protective precaution for the first two weeks only, but this is not a real disadvantage as many other surgical procedures need the same.18 The advantages to the patient of a minimally invasive procedure, with small scars and rapid mobilization, brief hospitalization, and immediate protected, weight-bearing mobilization.We suggest that our method is more applicable for the well-visualized nidus through a plain radiograph by most orthopaedic surgeons. The use of the radiolucent table and the high- resolution image intensifier for anteroposterior and lateral radiographs is familiar to all orthopaedic doctors and the equipment of DHS reamer is widely available. The results of this study confirm the long- and medium term efficacy of this simple percutaneous technique of osteoid osteoma in children and adolescents. We think that our technique is a minimally invasive technique, simple, easy, safe, has minimal bone loss, easily tolerated by the patient, with shorter hospital stay, and a reliable procedure for well-visualized osteoid osteoma of large bones of the lower limbs if other expensive special tools are not available. However using the technique for the tibia is associated with more complications than with using it for the femoral neck.
References
1. Dahlin DC, Unni KK. Bone tumours: general aspects
and data on 8542 cases, 4th edn. Thomas, Springfield 1987, pp 88–101.
2. Gangi A. Treatment of osteoid osteomas: review of available therapeutic options: surgery, percutaneous resection, percutaneous alcohol ablation or thermocoagulation. J Radiol 1999; 80: 419–420.
3. Yildiz Y, Bayrakci K, Altay M, Saglik Y. Osteoid osteoma: the results of surgical treatment. Int Orthop 2001; 25: 119–122.
4. Bisbinas I, Georgiannos D, Karanasos T. Wide surgical excision for osteoid osteoma. Should it be the first-choice treatment? Eur J Orthop Surg Traumatol 2004; 14: 151–154
5. Kneisl JS, Simon MA. Medical management compared with operative treatment for osteoid-osteoma. J Bone Joint Surg (Am) 1992; 74: 179–185.
6. Assoun J, Jourlaud T, Chiavassu H, Bonnevialle P, Railhuc N, Giron J,etal . Osteoid osteoma: CT-guided percutaneous resection and follow-up in 38 patients. Radiology 1999; 212: 687–692.
7. Buhler M, Binkert C, Exner G. Osteoid osteoma: technique of computed tomography-controlled percutaneous resection using standard equipment available in most orthopaedic operation rooms. Arch.Orthop.Trauma Surg2001; 121: 458– 461.
8. Sierre S, Innocenti S, Lipsich J, Lanfranchi L, Questa H, Moguillansky S Percutaneous treatment of osteoid osteoma by CT-guided drilling resection in pediatric patients Pediatr Radiol 2006; 36: 115–118.
9. Barei DP, Moreau G, Scarborough MT, Neel MD. Percutaneous radiofrequency ablation of osteoid osteoma. Clin Orthop Relat Res 2000; 373:115–124.
10. Lindner NJ, Ozaki T, Roed R, Gosheger G, Winkelmann W, Wortler K. Percutaneous radiofrequency ablation in osteoid osteoma. J Bone Joint Surg Br 2001; 83: 391–396.
11. Torriani M, Rosenthal D. Percutaneous radiofrequency treatment of osteoid osteoma. Pediatr Radiol 2002; 32: 615–618.
12. Gangi A, Dietemann JL, Gasser B, et al. Interstitial laser photocoagulation of osteoid osteomas with use of CT-guidance. Radiology 1997; 203:843–848.
13. Witt JD, Hall-Cruggs MA, Ripley P, Cobb P, Bown SG. Interstitial laser photocoagulation for the treatment of osteoid osteoma. J Bone Joint Surg (Br) 2000; 82: 1125–1128
14. Campanacci M, Ruggieri P, Gasparini A, Ferrano A, Campanacci L. Osteoid osteoma. Direct visual identification and intralesional excision of the nidus with minimal removal of bone. J Bone Joint Surg (Br) 1999; 81: 814–820
15. Cantwell CP, O’Byrne J, Eustace S. Current trends in treatment of osteoid osteoma with an emphasis on radiofrequency ablation. Eur Radiol 2004; 14:607–617.
16. Rosenthal DI, Hornicek FJ, Torriani M, Gebhardt MC, Mankin HJ. Osteoid osteoma: percutaneous treatment with radiofrequency energy. Radiology 2003; 229:171–175.
17. Woertler K, Vestring T, Boettner F, Winkelmann W, Heindel W, Lindner N. Osteoid osteoma: CT-guided percutaneous radiofrequency ablation and follow-up in 47 patients. J Vasc Interv Radiol 2001; 12:717–722.
18. Sans N, Galy-Fourcade D, Assoun J, Jarlaud T, Chiavassa H, Bonnevialle P, et al. Osteoid osteoma: CT-guided percutaneous resection and follow-up in 38 patients. Radiology 1999; 212: 687–692.
Ablation of Osteoid Osteoma of Lower Extremity using Dynamic Hip Screw Drill





























