Embed Size (px)
Citation preview
September 2014 47 Volume 13 • Issue 9
Copyright © 2014 ORIGINAL ARTICLES Journal of Drugs in Dermatology
SPECIAL TOPIC
A Randomized, Split-Face, Histomorphologic Study Comparing a Volumetric Calcium Hydroxylapatite
and a Hyaluronic Acid-Based Dermal Filler Yana Yutskovskaya MD,a Evgenjia Kogan MD,b and Eugene Leshunov MDa
aDepartment of Cosmetology, Pacific State Medical University, Moscow, Russia bDepartment of Pathology and Department of National Scientific Center of Obstetrics, Gynecology and
Perinatology of Russian Federation, First Moscow State Medical University, Moscow, Russia
Background: Soft-tissue augmentation with fillers is an aesthetic procedure for restoring age-related volume loss.Objective: To compare neocollagenesis and elastin production stimulated by Radiesse® (calcium hydroxylapatite; CaHA, Merz Pharma-ceuticals GmbH) and a hyaluronic acid-based filler (HA; Juvéderm® VOLUMA®).Methods: Twenty-four women, aged 35–45, participated in this split-face, comparative study. Punch biopsies were taken 4 and 9 months after supraperiostal injection of each filler into the ipsilateral or contralateral postauricular area. Samples were analyzed for collagens type I and III, elastin, Ki-67, and inflammatory and angiogenic markers. Results: At month 4, collagen type III was greater with CaHA vs HA (P=0.0052). By month 9, type I staining was higher with CaHA vs HA (P=0.0135), whereas type III was lower with CaHA than HA (P=0.0019). Staining for elastin, Ki-67 and angiogenesis was greatest with CaHA at both timepoints. Inflammatory markers increased most with HA treatment.Conclusions: CaHA resulted in more active, physiologic remodeling of the extracellular matrix than HA by stimulating a two-step process whereby collagen type I gradually replaced type III. Increased elastin stimulated by CaHA also indicates active remodeling. The results of this study suggest that, in the first 9 months after treatment, by reconstituting tissue homeostasis without inducing inflammation suggests CaHA has more desirable characteristics for a dermal filler than HA.
J Drugs Dermatol. 2014;13(9):xxx-xxx.
ABSTRACT
INTRODUCTION
Soft-tissue augmentation with dermal fillers is a popu-lar, minimally invasive aesthetic procedure.1 In 2012, in the USA, most non-surgical augmentation treatments
performed with a dermal filler used a product based on hyaluronic acid (HA), with the second most popular type be-ing the calcium hydroxylapatite (CaHA)-based filler, Radiesse®
(Merz Pharmaceuticals GmbH, Frankfurt, Germany), hereafter referred to as CaHA gel matrix.2
Several HA-based fillers are available, including the product Juvéderm® VOLUMA® (Allergan Inc., Irvine, CA), hereafter referred to as ‘HA gel’, an injectable cross-linked gel implant intended to restore the volume of the face. It is a member of a family of HA-based fillers that differ with respect to their degree of cross-linking and HA concentration.3,4 The CaHA gel matrix is formulated to immediately augment volume and, subsequently, to stimulate collagen production.5 As a sub-dermal implant, CaHA gel matrix is indicated for plastic and reconstructive surgery of the facial area, including the correc-tion of moderate-to-severe facial wrinkles and folds, such as nasolabial folds (NLF) and restoration and/or correction of the signs of facial fat loss (lipoatrophy) in people with human im-munodeficiency virus (HIV) infection.6
Studies have shown that the HA gel, which is a combination of a low (<1 mDa) and high (>1 mDa) molecular weight HA (20 mg/mL), is effective and well-tolerated in restoration of facial volume loss.4,7 Similarly, the porous CaHA gel matrix has well-established tolerability,8 having been used in re-constructive and orthopedic surgery and dentistry for over 20 years.9 The CaHA gel matrix has been studied in many clini-cal trials for volume augmentation in facial aesthetics and has demonstrated efficacy, safety, and good tolerability in the cor-rection of NLF,10-12 as well as the volume loss associated with HIV infection.13 In one direct comparison study of CaHA gel matrix and another HA gel product (Juvéderm® 24; HA 24; 24 mg/mL HA; Allergan Inc.) for the improvement of NLF, CaHA gel matrix was more efficacious and longer-lasting than HA 24.14
The CaHA gel matrix has also been shown to stimulate an increase in the production of collagen within the injected re-gion.15 Collagen and elastin are components of the extracellular matrix (ECM) that confer important biomechanic properties to the skin.16 Dermal collagen in adult skin accounts for 77% of the fat-free dry weight of the skin, and is primarily composed of col-lagen types I and III. These collagen subtypes provide the skin with its tensile strength and structural support, and are known
JDD PROOFS

48
Journal of Drugs in DermatologySeptember 2014 • Volume 13 • Issue 9
Y. Yutskovskaya, E. Kogan, E. Leshunov
Study TreatmentParticipants received injections of both CaHA gel matrix and HA gel. The CaHA gel matrix injections were given in a single dose (maximum 0.1 mL) by supraperiostal administration to the postauricular area on the left side. HA gel injections were also given in a single dose (maximum 0.1 mL), administered to the same area on the right side.
Visits and AssessmentsTreatment was performed at visit 1 (day 1). There were two sub-sequent evaluation visits at months 4 (±2 weeks) and 9 (±2 weeks) after treatment. At both visits, punch biopsies of the postauricular area (3–4 mm diameter) were obtained for histomorphologic and immunohistochemical analysis of collagen types I and III, elastin, and also Ki-67 and angiogenesis (morphometry data: for fibers, %/mm2; for cells, number of positive cells/mm2). Micropho-tography was performed using an Olympus BX41 microscope (Olympus America Inc., Melville, NY). Ultrasound scanning was performed at a frequency of 45 MHz using a SkinScanner DUB 22–75 MHz (taberna pro medicum GmbH, Lüneburg, Germany).
Punch biopsies (96 biopsies from 24 participants) were fixed in 10% neutral formalin and embedded in paraffin according to standard protocols. Serial 4 μm paraffin sections were prepared and stained with hematoxylin-eosin (H&E). Tissue samples extracted through punch biopsies at months 4 and 9 after treat-ment were analyzed by both qualitative and quantitative measures for collagen types I and III and elastin expression. Qualitative and quantitative measures of Ki-67, lymphohistiocytic infiltration and angiogenesis were also taken at these timepoints.
For immunohistochemistry, sections were stained after anti-gen unmasking in retriever solution, according to standard protocols. Monoclonal antibodies against collagen type I (Sig-ma-Aldrich Corporation, St. Louis, MO; used at 1:4000 dilution), collagen type III (Sigma Aldrich Corporation; used at 1:8000 di-lution), elastin (Novacastra Leica Biosystems, Newcastle upon Tyne, UK; used at 1:200 dilution) and Ki-67 (RTU DaKo, Glos-trup, Denmark; used at 1:100 dilution) were used.
A semi-quantitative method was used to analyze the immuno-histochemistry results, with 10 fields of vision studied at high magnification (x400) in two sections, according to the standard scale. Staining intensity was scored as weak (2 points), moderate (4 points), strong (6 points) or hyperexpression (8 points). Epider-mal expression of Ki-67 was evaluated by the mean percentage of positively-stained cell nuclei among a sample of 300 epithelial cells. Angiogenesis was measured by counting the number of capillary-type vessels per 10 fields of vision in dermal tissue slides stained with H&E, viewed at high magnification (x400). The sign-rank test of Wilcoxon was used for the comparison of the CaHA gel matrix and HA gel collagen type I, collagen type III, and Ki-67 quantification and the elastin data in this paired design.
to participate in the process of ECM remodeling.16,17 Indeed, as the most abundant structural protein in the dermal ECM, type I collagen has a pivotal role in providing the skin with strength and resilience.18 In contrast, elastin is a distinct protein character-ized by long-range extensibility, giving skin elasticity.16 During the ageing process there is a progressive loss of dermal collagen and elastin fibers19 that contributes to the formation of wrinkles by altering the biomechanic properties of the skin.20 As such, the potential of treatments such as CaHA gel matrix to stimu-late production of these important ECM components represents an interesting line of investigation, particularly in the context of previous work indicating that CaHA gel matrix can stimulate neo-collagenesis (the production of new collagen type I).15
A further role for dermal fillers in maintaining the structural integ-rity of the dermal ECM has been documented through the positive impact of HA on dermal cell proliferation, as shown through increased Ki-67 (a marker of cell proliferation and, therefore, an index of ECM remodeling in the injected skin) immunostaining.21
The aim of this study was to compare the CaHA gel matrix with HA gel for their ability to stimulate neocollagenesis follow-ing single-dose administration, as determined by qualitative and quantitative histomorphologic/immunohistochemical analysis at 4 and 9 months after treatment. An additional aim was to examine the effects of both fillers on levels of dermal elastin, lymphohistiocytic infiltration (a measure of inflamma-tory response in the injected region) and Ki-67. To the authors’ knowledge, this is the first head-to-head study of the histomor-phologic effects of two dermal fillers on neocollagenesis and elastin production in the region of the implant, while it is also the first to extend follow-up to 9 months.
METHODSStudy DesignThis was a randomized, split-face, comparative, clinical study and immunohistochemical investigation in healthy female volunteers, 35–45 years of age. Recruitment of participants occurred from one site in Moscow between November 2012 and February 2013. Writ-ten informed consent from all participants and ethical approval for the study were obtained. The study was conducted in accordance with the ethical principles laid down in the Declaration of Helsinki.
ParticipantsParticipants in the study had symmetric NLF as an indicator of facial symmetry, and scored 3–4 on the validated Merz 5-point scale for NLF at rest.22 Participants were excluded if they were pregnant or breastfeeding, had significant facial asymmetry, had applied any resorbable and permanent fillers, HAs or botu-linum toxin type A to the face in the previous 12 months (any previous administration of permanent materials in the lower third of the face, including polylactic acid, polymethyl methac-rylate and silicone) or had a history of facial nerve palsy.
JDD PROOFS

49
Journal of Drugs in DermatologySeptember 2014 • Volume 13 • Issue 9
Y. Yutskovskaya, E. Kogan, E. Leshunov
months 4 and 9 after treatment with CaHA gel matrix compared with HA gel (P<0.0002 and P<0.0001, respectively; Figure 4). Grade of lymphohistiocytic infiltration was significantly lower with CaHA gel matrix at months 4 and 9 after treatment com-pared with HA gel (P=0.0108 and P<0.0001, respectively) and grade of mucoid edema was significantly lower with CaHA gel matrix compared with HA gel at month 4 (P<0.0001). By month 9, the grades were negligible for both treatments (Figure 4).
Effect on Epidermal and Dermal StructureUltrasound scanning (a routine method for assessing dermal structure in the practice of cosmetology) showed that, prior to treatment with CaHA gel matrix, the structure of the epider-mis was neither homogenous nor clearly separated from the dermis. The dermis was not structurally uniform; fibers in the superficial layer were arranged densely and linearly, while the
SafetySafety and tolerability were monitored throughout the study and for a further month after study completion. Safety infor-mation was gathered from questionnaires given to participants and from face-to-face interviews prior to treatment. At each vis-it, subjects were asked about adverse events (AEs) and serious AEs, and details of concomitant medications were recorded.
RESULTSParticipant DemographicsA total of 24 healthy women (age range, 35–45 years) took part in this study.
Analysis of Collagen Expression at Month 4At month 4, collagen type I formation was found to be higher with CaHA (mean staining intensity: 4.0±1.44) than with HA gel (mean staining intensity: 3.65±1.65), nearing a level of statisti-cal significance (P=0.0679). At this timepoint, the mean staining intensity of collagen type III was significantly greater with CaHA gel matrix than HA gel (5.2±1.67 vs 4.2±1.44, respectively; P=0.0052).
Analysis of Collagen Expression at Month 9At month 9, the mean staining intensity for collagen type I was significantly greater after treatment with CaHA gel matrix than with HA gel (6.58±1.1 vs 4.8±1.86, respectively; P=0.0135; Figure 1). This difference in staining intensity was also dem-onstrated by the more widespread brown staining (indicating collagen type I expression) seen with CaHA gel matrix vs HA gel, (Figure 2). The staining intensity for collagen type III was significantly lower at month 9 after treatment with CaHA gel ma-trix compared with HA gel (3.7±1.09 vs 6.02±0.82, respectively; P=0.0019). This difference in staining intensity was also support-ed by the less intense brown staining (indicating collagen type III expression) seen with CaHA gel matrix vs HA gel at month 9.
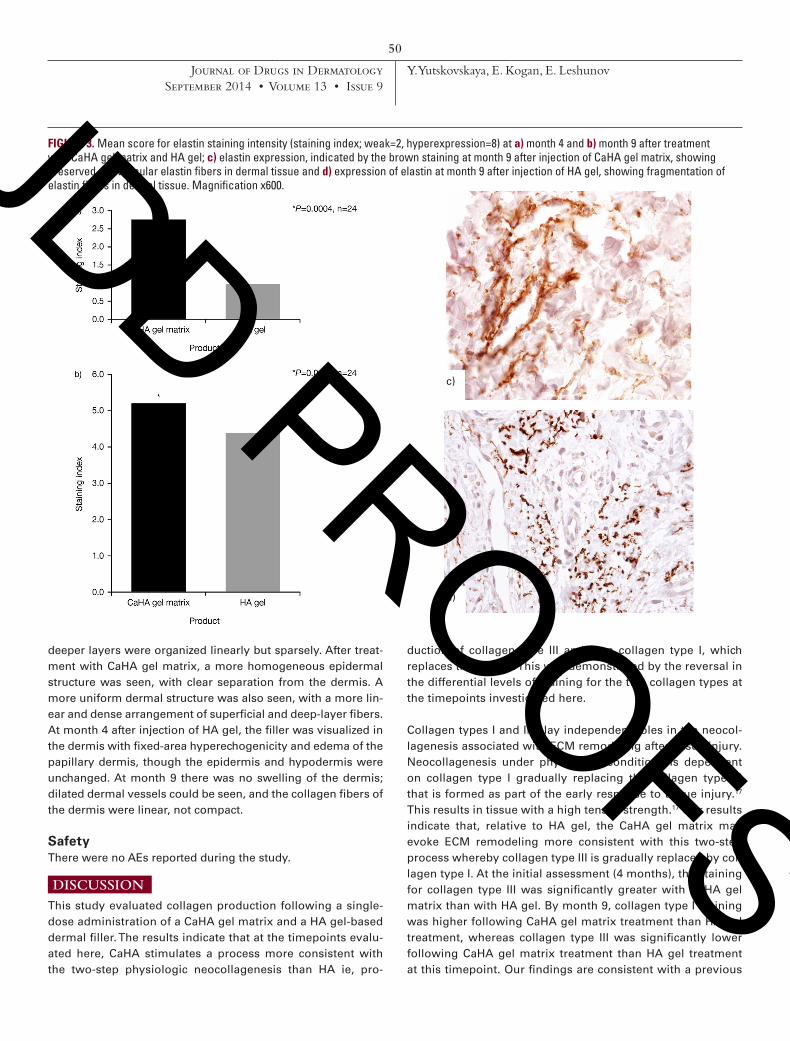
Analysis of Elastin Expression, Ki-67 Staining, Angiogenesis, Lymphohistiocytic Infiltration, and Mucoid EdemaElastin staining intensity was significantly higher after treat-ment with CaHA gel matrix vs HA gel, both at month 4 (2.8±2.3 vs 1.0±1.15, respectively; P=0.0004) and month 9 (5.2±1.22 vs 4.33±1.27; P=0.0186) (Figure 3). The pattern of elastin staining was also very different with CaHA gel matrix compared with HA gel; preserved perivascular elastin fibers were evident at 9 months after treatment with the former, but fragmentation of elastin fibers was observed at the same timepoint after treatment with HA gel (Figure 3). Ki-67 staining was similar with the CaHA gel matrix and HA gel at month 4 (3.4%±2.08% vs 3.3%±2.4%, respectively; P=0.2013) but was significantly greater with the CaHA gel than HA gel at month 9 after treatment (6.2%±2.2% vs 4.5%±1.79%, respectively; P=0.0011). Significantly more angio-genesis was evident in the dermis from H&E-stained sections at
FIGURE 1. Mean scores for collagen type I staining intensity (stain-ing index; weak=2, hyperexpression=8) 9 months after treatment with CaHA gel matrix or HA gel.
FIGURE 2. Microphotographs showing collagen type I expression, as indicated by the brown staining, at month 9 after treatment with a) CaHA gel matrix and b) HA gel. Deposition of collagen type I is indicated with the red arrows. Magnification x600.
JDD PROOFS
50
Journal of Drugs in DermatologySeptember 2014 • Volume 13 • Issue 9
Y. Yutskovskaya, E. Kogan, E. Leshunov
duction of collagen type III and then collagen type I, which replaces the former. This was demonstrated by the reversal in the differential levels of staining for the two collagen types at the timepoints investigated here.
Collagen types I and III play independent roles in the neocol-lagenesis associated with ECM remodeling after tissue injury. Neocollagenesis under physiologic conditions is dependent on collagen type I gradually replacing the collagen type III that is formed as part of the early response to tissue injury.17 This results in tissue with a high tensile strength.17 Our results indicate that, relative to HA gel, the CaHA gel matrix may evoke ECM remodeling more consistent with this two-step process whereby collagen type III is gradually replaced by col-lagen type I. At the initial assessment (4 months), the staining for collagen type III was significantly greater with CaHA gel matrix than with HA gel. By month 9, collagen type I staining was higher following CaHA gel matrix treatment than HA gel treatment, whereas collagen type III was significantly lower following CaHA gel matrix treatment than HA gel treatment at this timepoint. Our findings are consistent with a previous
FIGURE 3. Mean score for elastin staining intensity (staining index; weak=2, hyperexpression=8) at a) month 4 and b) month 9 after treatment with CaHA gel matrix and HA gel; c) elastin expression, indicated by the brown staining at month 9 after injection of CaHA gel matrix, showing preserved perivascular elastin fibers in dermal tissue and d) expression of elastin at month 9 after injection of HA gel, showing fragmentation of elastin fibers in dermal tissue. Magnification x600.
c)
d)
deeper layers were organized linearly but sparsely. After treat-ment with CaHA gel matrix, a more homogeneous epidermal structure was seen, with clear separation from the dermis. A more uniform dermal structure was also seen, with a more lin-ear and dense arrangement of superficial and deep-layer fibers. At month 4 after injection of HA gel, the filler was visualized in the dermis with fixed-area hyperechogenicity and edema of the papillary dermis, though the epidermis and hypodermis were unchanged. At month 9 there was no swelling of the dermis; dilated dermal vessels could be seen, and the collagen fibers of the dermis were linear, not compact.
SafetyThere were no AEs reported during the study.
DISCUSSIONThis study evaluated collagen production following a single-dose administration of a CaHA gel matrix and a HA gel-based dermal filler. The results indicate that at the timepoints evalu-ated here, CaHA stimulates a process more consistent with the two-step physiologic neocollagenesis than HA ie, pro-
JDD PROOFS

51
Journal of Drugs in DermatologySeptember 2014 • Volume 13 • Issue 9
Y. Yutskovskaya, E. Kogan, E. Leshunov
study that found that at 6 months post-treatment with CaHA gel matrix, collagen type I infiltration and deposition were stimulated.15 However, the previous study by Berlin et al only used a single timepoint at 6 months and, therefore, did not observe the change in infiltration pattern shown here.
The dominance of collagen type III at the later timepoint evalu-ated here, 9 months following HA gel administration, may be of concern owing to the involvement of collagen type III in fibrosis; it has been observed that the scar tissue that can persist after wound healing contains a higher concentration of collagen type III than is found in normal adult dermal tissue.23
However, it would be interesting to investigate whether the pro-cess of ECM remodeling is delayed following HA gel treatment compared with CaHA treatment and if the levels of collagens are more similar between the two products at later timepoints.
CaHA gel matrix also stimulated cell proliferation signifi-cantly more than HA gel, as reflected by a relative increase in Ki-67 staining with the former at month 9, which may support the observed increase in collagen production by stimulating proliferation of collagen-producing cells. This is consistent with previous work showing the presence of fibroblasts and macrophages 6 months after injection of CaHA gel matrix.5,15 Treatment with CaHA gel matrix also stimulated neoangio-genesis at both 4 and 9 months, suggesting that blood flow
and, therefore, nutrient delivery to the skin was improved with CaHA gel matrix compared with HA gel. Moreover, the increase in angiogenesis correlates with, and may result in, the early synthesis of collagen type III.
This study was the first known examination of the effect of der-mal fillers on elastin levels. It found that CaHA gel matrix also stimulated remodeling of the ECM by increasing elastin levels to a significantly greater extent than HA gel. Elastin provides skin with the ability to recoil after deforming stresses have been applied. Therefore, unlike HA gel, the CaHA gel matrix appears to have the potential to improve not only the structural strength of skin via collagen remodeling, but also its elasticity, proper-ties that are known to decline in ageing skin in parallel with the loss of both collagen and elastin fibers.19,20
Lymphohistiocytic infiltration is suggestive of inflamma-tory changes in the tissue. Observations at both timepoints showed that HA caused significantly more lymphohistiocytic infiltration, suggesting that it has a more pronounced effect on the inflammatory process than CaHA gel matrix. In addi-tion, the lymphohistiocytic infiltration may result in elastin lysis and fragmentation; this could account for the significant-ly lower levels of elastin following HA gel injection compared with CaHA gel matrix.
There were a number of limitations to this study that merit discussion. First, the study was performed in a relatively small number of participants. While the area chosen for treat-ment was the postauricular region rather than areas such as NLF, which are typically treated with dermal fillers, it was felt that this was a suitable sample point given the similarity between the skin of the postauricular region and areas that are commonly injected with dermal fillers. Furthermore, treating the postauricular region means that any temporary unsightliness caused by the biopsy can be easily hidden. Only two post-treatment timepoints were evaluated in the present study as this was deemed appropriate to show the process of neocollagenesis being stimulated. However, as mentioned above, we cannot rule out further changes in terms of colla-gen or elastin staining by either product beyond the 9-month timepoint and, thus, longer term monitoring of these pro-cesses should be the subject of further study.
In conclusion, CaHA gel matrix produced an instant volume enhancement, but with a longer reconstructive process brought about through collagen neogenesis. At the timepoints evaluated here, CaHA gel matrix treatment resulted in a pro-cess indicative of more active, physiologic remodeling of the ECM in comparison with HA gel. The CaHA gel matrix stimu-lated the production of collagen type III and type I in a two-step process whereby collagen type I gradually replaced collagen type III, consistent with the process of remodeling and collagen
FIGURE 4. Histomorphologic characteristics at (a) month 4 and (b) month 9 after treatment with CaHA gel matrix and HA gel. JDD PROOFS
52
Journal of Drugs in DermatologySeptember 2014 • Volume 13 • Issue 9
Y. Yutskovskaya, E. Kogan, E. Leshunov
production under physiologic conditions. The increase in elastin fibers stimulated by CaHA gel matrix treatment also indicates active remodeling; indeed, by reconstituting tissue homeosta-sis without inducing inflammation. Taken together, the results indicate that CaHA gel matrix evokes a process consistent with physiologic remodeling of the ECM and thus displays fa-vorable properties for a dermal filler.
ACKNOWLEDGMENTSFinancial and scientific support was provided by Merz Pharmaceu-ticals GmbH. Editorial assistance, funded by Merz Pharmaceuticals GmbH, was provided by Ogilvy 4D, Oxford, UK.
DISCLOSURESYana Yutskovskaya has no conflicts of interest to disclose. Evgenjia Kogan has no conflicts of interest to disclose. Eugene Leshunov has no conflicts of interest to disclose. This study was supported by Merz Pharmaceuticals GmbH, Frankfurt, Ger-many. All authors had full access to all the data in the study and had final responsibility for the decision to submit for pub-lication. Editorial assistance, funded by Merz Pharmaceuticals GmbH, was provided by Ogilvy 4D, Oxford, UK.
REFERENCES1. Carruthers J, Cohen SR, Joseph JH, et al. The science and art of dermal fill-
ers for soft-tissue augmentation. J Drugs Dermatol. 2009;8:335–50.2. ASAPS. The American Society for Aesthetic Plastic Surgery Statistics 2012. Avail-
able at: http://www.surgery.org/media/statistics. Accessed February 10, 2014.3. Bogdan Allemann I, Baumann L. Hyaluronic acid gel (Juvéderm) preparations
in the treatment of facial wrinkles and folds. Clin Interv Aging. 2008;3:629–34.4. Hoffmann K, Juvéderm Voluma Study Investigators Group. Volumizing ef-
fects of a smooth, highly cohesive, viscous 20-mg/mL hyaluronic acid volu-mizing filler: prospective European study. BMC Dermatol. 2009;9:9.
5. Marmur ES, Phelps R, Goldberg DJ. Clinical, histologic and electron micro-scopic findings after injection of a calcium hydroxylapatite filler. J Cosmet Laser Ther. 2004;6:223–6.
6. Jacovella PF. Use of calcium hydroxylapatite (Radiesse) for facial augmenta-tion. Clin Interv Aging. 2008;3:161–74.
7. Callan P, Goodman GJ, Carlisle I, et al. Efficacy and safety of a hyaluronic acid filler in subjects treated for correction of midface volume deficiency: a 24 month study. Clin Cosmet Investig Dermatol. 2013;6:81–9.
8. Pavicic T. Calcium hydroxylapatite filler: an overview of safety and tolerability. J Drugs Dermatol. 2013;12:996–1002.
9. Berlin A, Cohen JL, Goldberg DJ. Calcium hydroxylapatite for facial rejuvena-tion. Semin Cutan Med Surg. 2006;25:132–37.
10. Smith S, Busso M, McClaren M, Bass LS. A randomized, bilateral, prospective comparison of calcium hydroxylapatite microspheres versus human-based col-lagen for the correction of nasolabial folds. Dermatol Surg. 2007;33:S112–21.
11. Bass LS, Smith S, Busso M, McClaren M. Calcium hydroxylapatite (Radiesse) for treatment of nasolabial folds: long-term safety and efficacy results. Aes-thet Surg J. 2010;30:235–8.
12. Graivier MH, Bass LS, Busso M, et al. Calcium hydroxylapatite (Radiesse) for correction of the mid- and lower face: consensus recommendations. Plast Reconstr Surg. 2007;120:55S–66S.
13. Silvers SL, Eviatar JA, Echavez MI, Pappas AL. Prospective, open-label, 18-month trial of calcium hydroxylapatite (Radiesse) for facial soft-tissue augmentation in patients with human immunodeficiency virus-associated lipoatrophy: one-year durability. Plast Reconstr Surg. 2006;118:34S–45S.
14. Moers-Carpi M, Vogt S, Santos BM, et al. A multicenter, randomized trial comparing calcium hydroxylapatite to two hyaluronic acids for treatment of nasolabial folds. Dermatol Surg. 2007;33:S144–51.
15. Berlin AL, Hussain M, Goldberg DJ. Calcium hydroxylapatite filler for facial rejuvenation: a histologic and immunohistochemical analysis. Dermatol
Surg. 2008;34:S64–7.16. Hussain SH, Limthongkul B, Humphreys TR. The biomechanical properties of
the skin. Dermatol Surg. 2013;39:193–203.17. Williamson D, Harding K. Wound healing. Medicine. 2004;32:4–7.18. Fisher GJ, Varani J, Voorhees JJ. Looking older: fibroblast collapse and thera-
peutic implications. Arch Dermatol. 2008;144:666–72.19. Montagna W, Carlisle K. Structural changes in ageing skin. Br J Dermatol.
1990;122 Suppl 35:61–70.20. Friedman O. Changes associated with the aging face. Facial Plast Surg Clin
North Am. 2005;13:371–80.21. Quan T, Wang F, Shao Y, et al. Enhancing structural support of the dermal
microenvironment activates fibroblasts, endothelial cells, and keratinocytes in aged human skin in vivo. J Invest Dermatol. 2013;133:658–67.
22. Narins RS, Carruthers J, Flynn TC, et al. Validated assessment scales for the lower face. Dermatol Surg. 2012;38:333–42.
23. de Rigal J, Escoffier C, Querleux B, et al. Assessment of aging of the human skin by in vivo ultrasonic imaging. J Invest Dermatol. 1989;93:621–5.
24. Bailey AJ, Bazin S, Sims TJ, et al. Characterization of the collagen of human hypertrophic and normal scars. Biochim Biophys Acta. 1975;405:412–21.
AUTHOR CORRESPONDENCE
Yana Yutskovskaya MDE-mail:................…….................................................. [email protected]
JDD PROOFS




























