Embed Size (px)
Citation preview

Center for Preventive and Genomic Cardiology, Divisions of Cardiologyand Clinical Epidemiology, Department of Medicine, McGill
University Health Centre, Montreal, Canada.
Am J Cardiol 2014;113:168e172
INTRODUCTION • The rapid increase in energy drink (ED) consumption has
stimulated growing public concern with adverse events related to ED consumption.
• The US Substance Abuse Services and Mental Health Administration has reported that over a 4-year period from 2007 to 2011, emergency department visits related to EDs more than doubled to >20,000 visits annually.
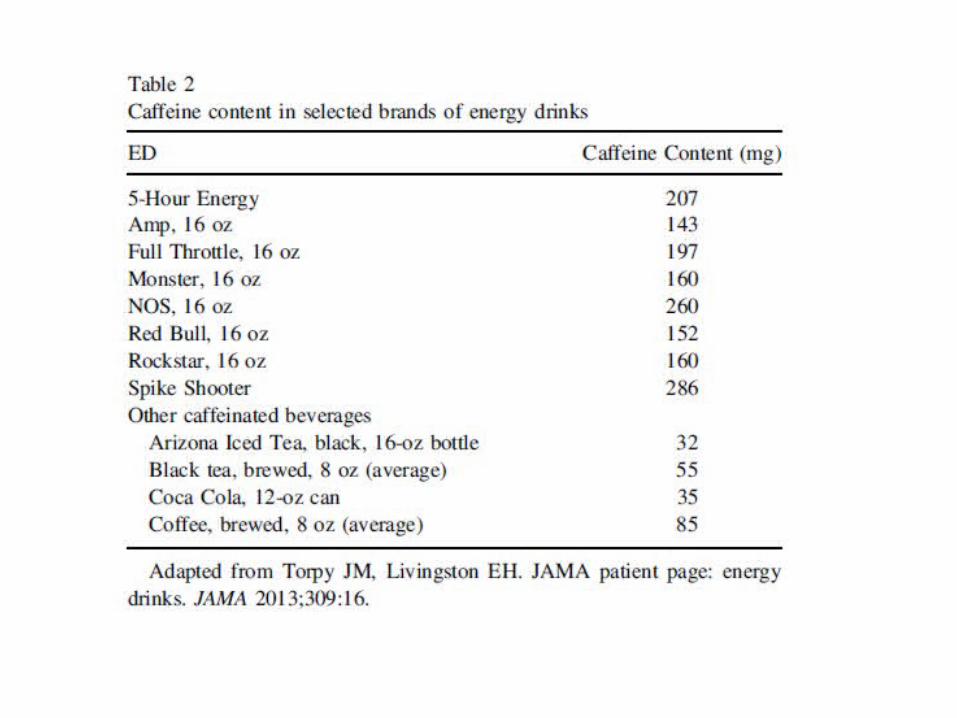
• Most of the adverse effects and toxicities associated with EDs have been attributed to the high caffeine content of EDs.
• In addition to the high caffeine content, EDs are frequently consumed by younger segments of the population who may be caffeine naive and more prone to consume large quantities, often mixed with alcohol and other substances, increasing the risk of adverse events.
• EDs also contain several other ingredients that may also increase these risks.
• Although the US FDA recently released a list of adverse
event reports allegedly related to EDs, extremely limited data (product name, symptoms, and outcome) regarding the clinical characteristics of these cases and their ED consumption profile have been made available to inform clinicians about this emerging health problem.
• Accordingly, we systematically reviewed the available literature for cases of cardiovascular (CV) events temporally related to ED consumption.
• We also included 2 additional cases from our institution of cardiac arrest after ED consumption.

METHODS• A systematic review of the Medline and Embase databases for peer-
reviewed articles published between January 1, 1980, and February 1, 2013, containing the search terms “energy drinks,” “adverse effects,” “myocardial infarction,” “cardiac arrest,” and “arrhythmia” in various combinations.

• From each eligible case, we extracted available data with regard to age and gender of the case, type of CV event, brand of ED consumed, estimated caffeine-dose ingested (as documented in the original report or calculated based on reported ED consumption and corresponding caffeine content disclosed on product labels) within 24 hours of event, co-ingestions with alcohol or other substances, preexisting CV disease, and results of CV investigations.
• We considered an estimated acute ingestion of 480 mg of caffeine within 8 hours as “acute heavy consumption” because this corresponds to drinking >3 cans or bottles (16 oz) of several popular EDs in a short time period.

• We also characterized “chronic heavy consumption” as 200 mg/ day of caffeine from EDs over 1 weeks.
• A serious CV event was defined as a cardiac
arrest, ventricular arrhythmia, or ST-segment elevation.

RESULTS
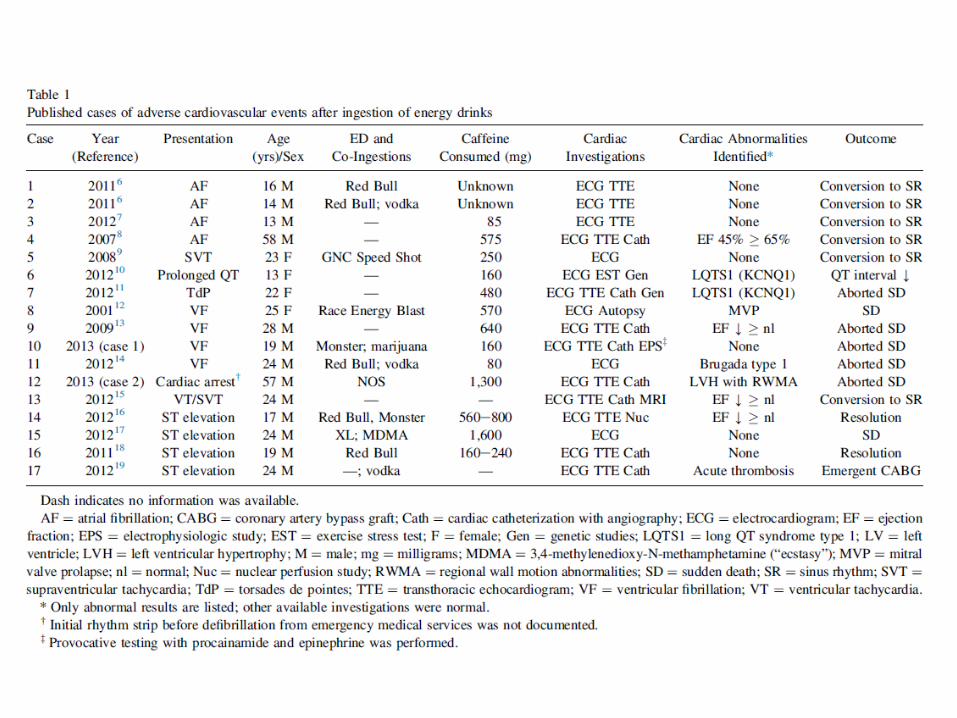
• Total 17 cases (15 cases from the literature and 2 cases from our institution).
DISCUSSION• Our case series of 17 cases represents the first systematic review of
the literature of ED-associated acute adverse CV events and adds to the growing number of adverse events related to EDs reported by the FDA and by health authorities in Canada.
• Despite the many adverse events reported to regulatory agencies, few data have been released regarding the clinical characteristics of these cases to help inform the CV community about these events.
• Our results, although prone to publication bias, show that the majority of affected cases involved teenagers and young adults, the largest demographic of ED consumers.
• On the basis of our series, we cannot conclude that any specific additive or brand appeared to be more frequently involved.

• However, we did find that heavy consumption of EDs was implicated in at least 7 cases, and 5 cases were associated with co ingestion of alcohol or other drugs.
• Of note, in all 4 reported cases of ST-elevation, the presenting symptom was severe chest pain.
• We also report that 11 cases presented with serious adverse events,
including cardiac arrest. Of these serious cases, the majority occurred either with acute heavy consumption of EDs or in combination with alcohol or other drugs.
• In at least 2 of these cases, EDs may have unmasked an underlying
channelopathy that predisposed the patient to ventricular arrhythmia.
• Importantly, in the remaining cases, no predisposing cardiac abnormality to explain the CV event was found (although the intensity of testing to uncover underlying cardiac abnormalities varied in each case).

• In 1 case of aborted SCD in a 19-year-old man from our institution (case 10), we performed detailed structural, functional (including echocardiography, magnetic resonance imaging, and coronary angiography) and electrophysiologic testing and could not identify any cardiac abnormality to explain the cardiac arrest
• There are several potential reasons EDs may predispose to acute adverse CV events.
• Caffeine, in doses that might be consumed in a beverage (250 mg), has been shown in normal subjects to increase levels of circulating catecholamines.
• EDs are also often consumed in an excessive or rapid manner, which may then lead to a surge in catecholamines.
• EDs have also been shown to increase platelet aggregation and worsen endothelial function, reduce myocardial blood flow when consumed before exercise, and significantly increase myocardial oxygen demand in experimental models, all of which could result in cardiac ischemia.
• Hypokalemia, which occurs in a caffeine dose-related manner, could contribute to ventricular arrhythmias and sudden death.
• EDs may also unmask channelopathies by prolonging the QT interval or suppressing sodium channel conduction.

• EDs are often coingested with other substances, such as alcohol and illicit drugs, which may potentiate the effects of caffeine.
• Chronic alcohol consumption has been shown to increase the half life of caffeine by up to 72%.
• Caffeine allows people to drink more alcohol without becoming excessively sedated, resulting in a higher likelihood of alcohol toxicity, which may include atrial fibrillation and ventricular arrhythmias.
• Ingredients in EDs other than caffeine, most of which have not been extensively studied, may also play a role in contributing to adverse CV events .

• Although the prevalence of heavy ED use in our case series (7 of 17 cases; 41%) is higher than the reported prevalence of heavy ED use from a control cohort of young military recruits (137 of 988; 14%), our findings neither imply nor rule out a causal relation between ED consumption and CV events.
• Given the increasing popularity of EDs, the increase in emergency department visits related to these drinks, the recent FDA report of several potentially related deaths, and the seriousness of many of the events in our series, ED-associated adverse events may represent an emerging public health problem.

• We acknowledge that the large number of consumers and the few reported events suggests that the risks related to EDs may, in fact, be small.
• However, because such adverse events are likely severely underreported, additional epidemiologic research is required to accurately estimate the magnitude of risks related to EDs, identify vulnerable populations (such as youth, patients with heart disease, and caffeine-naive consumers), and assess important interactions with additives in EDs, alcohol, and other co-ingestions

• Perhaps consideration of a nationwide registry for ED cases may assist in determining the true significance and the number of events.
• Until additional data become available, the general public and especially potentially vulnerable consumers such as youth and young adults, who make up the largest demographic of ED consumers, should be advised that caution is warranted when consuming these drinks (and consider avoiding them altogether in young adult/youth or caffeine-naive populations), specially in large quantities over short periods of time or mixed with alcohol or other drugs.

• The FDA has been actively investigating adverse events related to the consumption of EDs but has not yet further regulated EDs because of insufficient data.
• Health Canada, on the recommendations of an expert advisory panel, has recently reclassified EDs from “natural health product” to “food product”.
• Among the more stringent requirements, the new regulations involve limits on the amount of caffeine allowed per serving and mandatory labeling of caffeine content.
• Although the evidence for harm from EDs remains incomplete, given the
potential public health concern, reductions in caffeine content per serving to reduce the risk of caffeine intoxication, improved labeling that fully discloses total caffeine content from all sources (including natural) and advises against overconsumption, and warnings that certain vulnerable populations (e.g., youth, pregnant women, patients with cardiac conditions or caffeine sensitivity) should avoid EDs is recommended until additional evidence is available
LIMITATIONS• The rates of co-ingestions with EDs may be underestimated because
toxicology results were not always reported.
• Heavy consumption of EDs were temporally associated with these events and in many cases no alternative etiology could be identified, we cannot exclude that some of these cases are rare spontaneous CV events not directly related to ED consumption.
• we cannot accurately ascertain the prevalence of heavy ED use in a control group of healthy individuals.
• Although, we provide data from a US military cohort, the low numbers of cases in our series and potential selection bias limits our ability to make definitive claims regarding the risks of EDs.
CONCLUSION
• Several adverse CV events after consuming ED have been reported in the literature.
• Although causality cannot be inferred from our series, physicians should routinely inquire about ED consumption in relevant cases, and vulnerable consumers such as youth should be advised that caution is warranted with heavy consumption and/or with concomitant alcohol or drug ingestion





























