Embed Size (px)
Citation preview
Gluten Sensitive Enteropathy
Mary Grace Brignac
HHP 637
“Celiac Disease”
Overview
• What is it?
• Pathophysiology
• Epidemiology
• Etiology
• Symptoms
• Clinical Manifestations
• Medical Diagnosis
• Treatment
• Nutrition Care Process
What is Gluten Sensitive Enteropathy?• Gluten Sensitive Enteropathy is a T-cell mediated
autoimmune disease of malabsorption and abnormal reaction to gluten
• Those with this disease cannot tolerate gluten
• It is induced by ingestion of the gluten, but mainly the peptide strand gliadin in gluten
• Gliadin is found in wheat, barley, and rye
What is Gluten Sensitive Enteropathy?
• When gluten is ingested, the immune system responds by damaging the lining of the GI tract
• This response affects the body’s ability to absorb nutrients normally
• Disease originates from genetic, environmental, and autoimmune triggers by the body’s abnormal response to gluten
Additional Names
• Celiac Disease
• Celiac Sprue
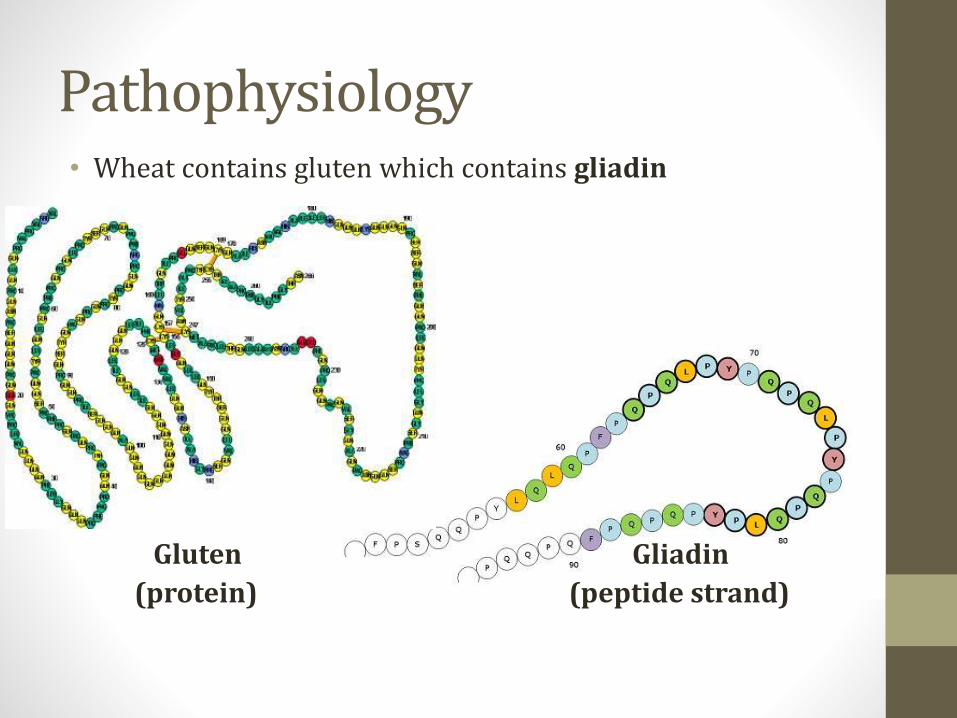
Pathophysiology• Wheat contains gluten which contains gliadin
Gluten Gliadin
(protein) (peptide strand)
Pathophysiology
• Gliadin
• Toxic effects to intestinal barrier
• Severely damages intestinal lining
• Difficult to digest
• Longer gliadin is left undigested, the greater amount of damage it can cause
• Undigested gliadin stimulates macrophages to release IL-8
• IL-8 activates innate immune system which triggers gut inflammation
• Antigens then attacked
• Inflammatory response is triggered
Pathophysiology
• Enterocytes and Tight Junctions
• Enterocytes are intestinal absorptive cells
• Tight junctions controlled by many signals
• Zonulin
• Protein that controls opening and closing of tight junctions
• Responsible for preventing paracellular absorptions of antigens

Pathophysiology• Gliadin-Zonulin interaction
• Gliadin causes zonulin levels to increase in people with this disease
• As zonulin increases, tight junctions function abnormally by opening wider
• This loosens the protective barrier of the gut wall
• Wider gut opening allows larger particles into enterocytes that shouldn’t be there
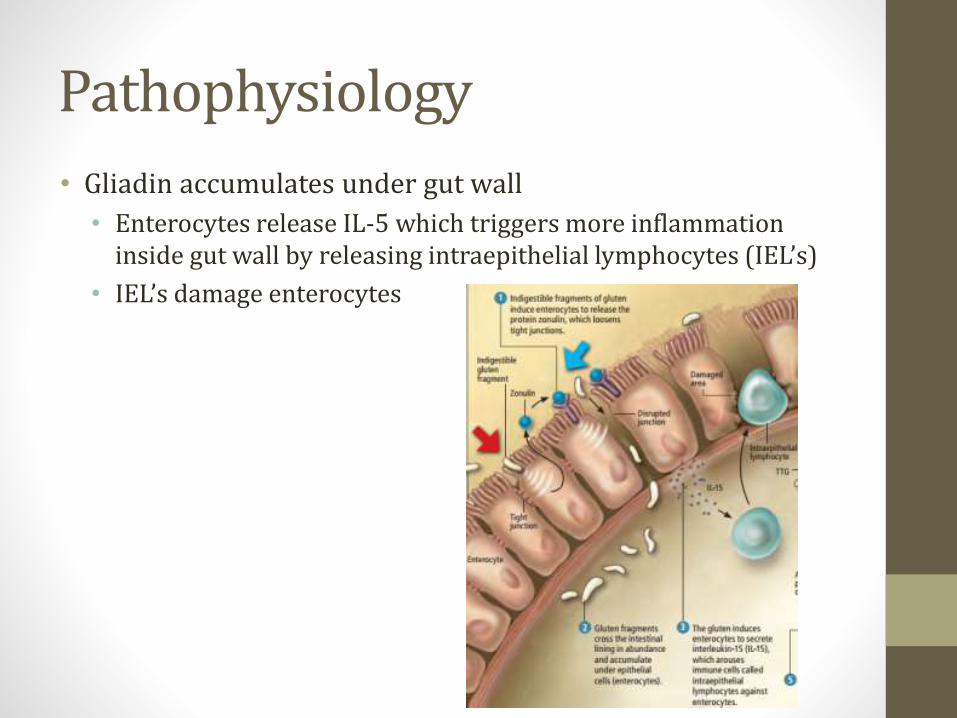
Pathophysiology
• Gliadin accumulates under gut wall
• Enterocytes release IL-5 which triggers more inflammation inside gut wall by releasing intraepithelial lymphocytes (IEL’s)
• IEL’s damage enterocytes
Pathophysiology
• Leaky Gut Syndrome
• Can be contracted depending on severity of enterocyte damage
• As gliadin accumulates behind gut wall, it crosslinks with the enzyme, tissue transglutaminase (tTG)
• tTG is released to repair damaged enterocyte cells
• tTG-gliadin crosslinkage mistakenly attacks enterocyte cells that produce tTG
• Triggers autoimmune response (body attacks itself)
• Microvilli eventually destroyed
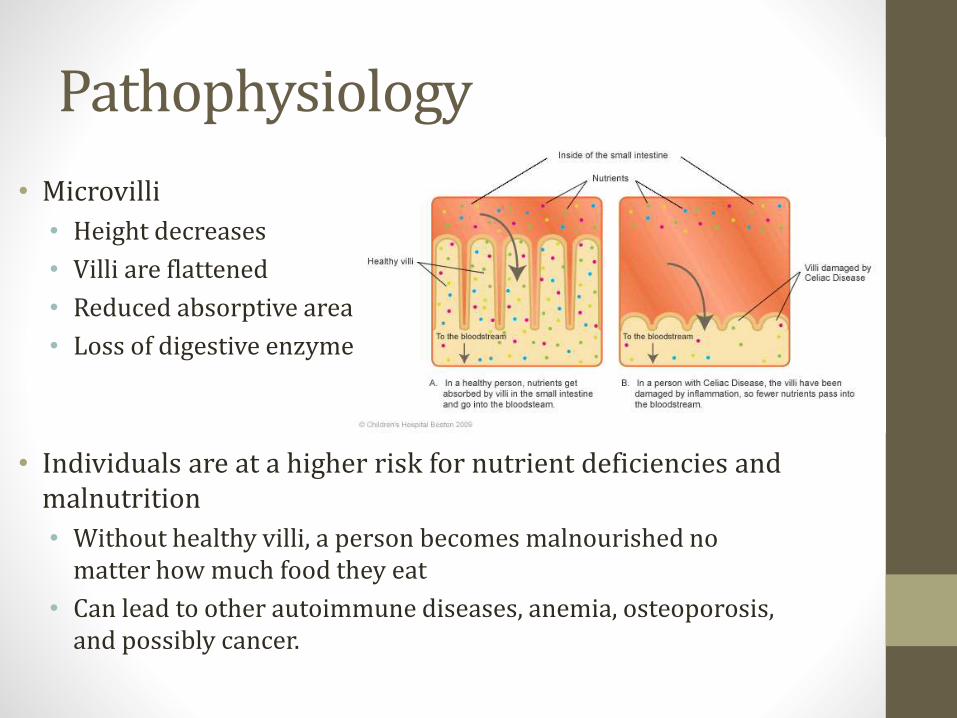
Pathophysiology
• Microvilli
• Height decreases
• Villi are flattened
• Reduced absorptive area
• Loss of digestive enzymes
• Individuals are at a higher risk for nutrient deficiencies and malnutrition
• Without healthy villi, a person becomes malnourished no matter how much food they eat
• Can lead to other autoimmune diseases, anemia, osteoporosis, and possibly cancer.
Epidemiology
• Affects 1 out of 250 people
• Likelihood of contracting the disease increases when a first-degree relative has it
• Associated with other autoimmune syndromes
• More commonly seen in these populations by a 5-10% increase
• Type 1 Diabetes Mellitus
• IgA deficiency
• Hyper-and hypothyroidism
• Turner and Down Syndromes
Epidemiology
• Women comprise 75% of newly diagnosed adult cases
• Genetics beginning to be identified as contributing factors in the cause of CD
• Several genes found to be present in 95% of all patients
• Sometimes triggered after surgery, pregnancy, childbirth, viral infections, or severe emotional distress
Etiology
• Damage to intestinal mucosa is accompanied by an inflammatory response in which WBC’s enter the mucosa
• Disease has an autoimmune nature
• Essentially the body attacks itself every time gluten is ingested
Etiology
• Environmental factors that appear to increase risk:
• Introducing gluten at a younger age
• Shorter length of breastfeeding time
• Amount of gluten containing foods
• Viral infections during infancy
• Symptoms vary based on age and degree of damage to the small intestine
• Many have this disease for a decade before being diagnosed
• The longer a person goes undiagnosed and untreated, the greater the chance of developing long-term complications
• Left untreated it can cause anemia, osteoporosis, or cancer
Symptoms
• In infants
• Impaired growth, diarrhea, abdominal distention
• In older children
• Short stature, pubertal delays, rickets, dental enamel defects,
behavioral disturbances and poor school performance
Symptoms
• In adults
• GI system: diarrhea, abdominal pain, cramping, bloating, gas
production
• Nervous System: seizures, tingling or numbness in hands/feet
• Skeletal system: bone pain, arthritis
• Psychiatric: depression and anxiety
• Miscellaneous: infertility, alopecia, hypoglycemia and weight loss
Clinical Manifestations
• Dermatitis Herpetiformis
• >10% of adults with CD
• Extremely itchy, chronic rash made of bumps and blisters
• On elbows, knees, back and buttocks
• Histological change in small intestine with mild or no GI
symptoms
• Treated with an antibiotic or strict gluten-free diet
• More likely to develop thyroid disease and certain cancers of the
intestines

Clinical Manifestations
• Dermatitis Herpetiformis
Clinical Manifestations
• Iron-Deficiency Anemia
• 50% of patients with CD are anemic
• Iron is absorbed in proximal small intestine where celiac
manifestations are most prominent
• Causes iron malabsorption
• Most common manifestation of CD
• Less commonly,
• Vitamin B12 deficiency, folate deficiency
Abnormal Lab Findings
• Decreased albumin
• malnutrition
• Elevated calcium, decreased phosphate
• Vitamin D deficiency, secondary hyperparathyroidism
• Low HDL and LDL
• Decreased fat absorption
• Coagulopathy
• Decreased vitamin K absorption
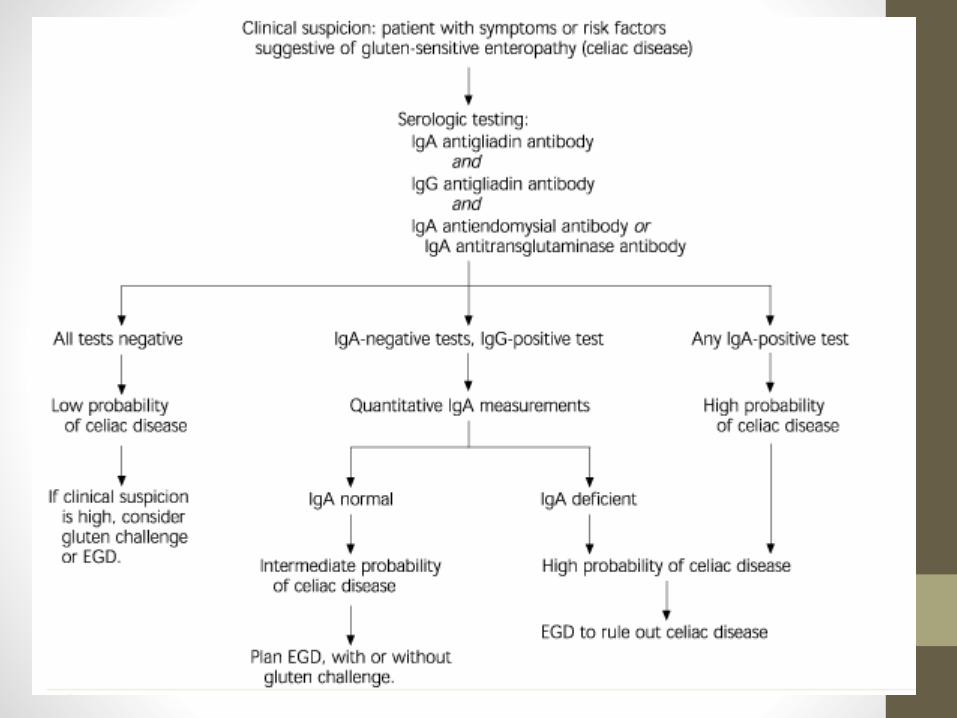
Medical Diagnosis
• Positive serologic test
• IgA anti-endomysial antibodies
• Measured using direct immunofluorescence
• IgA transglutaminase antibodies
• Measured using ELISA (assay)
• IgG and IgA anti-gliadin antibodies
• Measured using ELISA (assay)
• Presence of antibodies correlates to intestinal damage
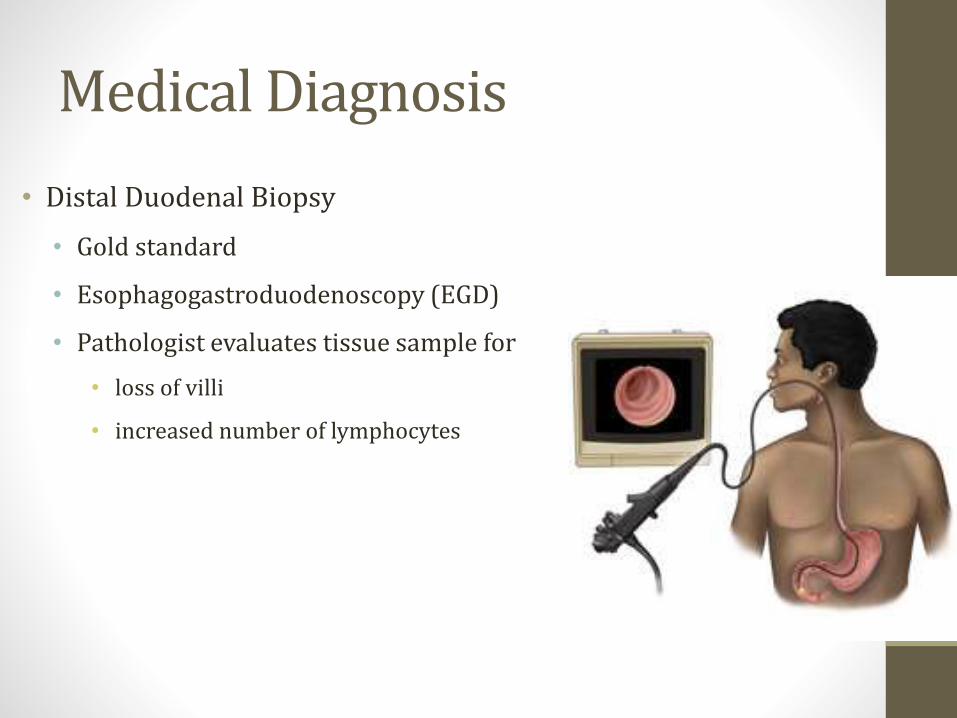
Medical Diagnosis
• Distal Duodenal Biopsy
• Gold standard
• Esophagogastroduodenoscopy (EGD)
• Pathologist evaluates tissue sample for
• loss of villi
• increased number of lymphocytes
4 Main Categories
• Classical Celiac Disease
• Symptoms of GI malabsorption
• Diagnosis by serological testing and intestinal biopsy
• Symptom improvement with gluten free diet
• Celiac Disease with Atypical Symptoms
• Few to no GI symptoms
• Diagnosis by serological testing and intestinal biopsy
• Symptom improvement with gluten free diet
4 Main Categories
• Silent Celiac Disease
• Asymptomatic individuals
• positive serological and biopsy tests
• Detected via screening of high-risk individuals
• Latent Celiac Disease
• Positive serological test
• no villous atrophy on biopsy
• Asymptomatic at first but may develop symptoms later
Treatment
• Exclusion of dietary gluten results in
• healing of mucosa
• resolution of malabsorptive state
• reversal of most effects of the disease
• People with CD can still eat a well-balanced diet with a
variety of foods
• plain meats, fish, rice, fruits, and vegetables.

• Gluten-free products are
increasing in mainstream stores.
Treatment
• Doctor will prescribe a gluten free diet and a consult with a
RD
• No wheat, barley, rye and sometimes oats
• Foods to avoid:
• Breaded foods• breads• bagels• cakes• donuts• most cereals • cold cuts• hot dogs
• crackers,• potato chips• gravy• pizza• most soups• beer• some candies• communion
• croutons• marinades• Sauces• some salad
dressings
Treatment
• What to eat
• Alternative grains rice, buckwheat, tapioca, potato or corn
flours
• Potatoes, rice flax, millet
• Legumes, nuts, seeds and cassava
• Oats are subject of controversy
• By themselves are nontoxic in limited quantities
• Commercial oat products are often contaminated with wheat
• Consult RD and doctor if seeking advice
Nutrition Care Process
I. Assessment
II. Diagnosis
III. Intervention
IV. Monitoring and Evaluation
Nutrition Care Process: Assessment• Assess food and nutrient intake
• Diet hx
• Macronutrient and micronutrient intake
• Calcium, Iron, B vitamins, vitamin D
• Knowledge/beliefs/attitudes
• Behavior
• Factors affecting access to food
• Food intake assessment is necessary to determine nutrition dx and plan intervention.
Nutrition Care Process: Assessment• Assess biochemical data
• GI profile• Intestinal biopsy• Celiac antibodies
• Nutritional anemias (iron deficiency anemia common)• Folate• Ferritin• B12
• Vitamin profile• Thiamin• Vitamin B6• 25-hydroxy vitamin D
• Mineral profile• Copper• Zinc
• Lipid profile• Electrolyte and renal profile
• Biochemical assessment is necessary because CD results in damage to the intestinal villi, leading to malabsorption.
Nutrition Care Process: Assessment• Bone density screening
• Recommended within the first year of diagnosis
• Studies and trials show reduced bone mineral content and density in adults with untreated CD
• Factors affecting quality of life
• Medical hx
• Any possible GI, immune, neurological, or psychological issues
• Social hx
• Socioeconomic factors, religion, social and medical support, stress level
• Individuals with CD may not have the same quality of life as people around them due to the inconveniences that go with following a gluten-free diet.
Nutrition Care Process: Assessment• GI symptoms
• Frequency and volume of BM
• Abdominal pain and bloating
• Nausea and vomiting
• Reduced gut motility
• Delayed gastric emptying
• People with CD, both treated and untreated, experience more GI symptoms.
Nutrition Care Process: Assessment• Other disease states
• Thyroid conditions
• Autoimmune disorders
• Endocrine disorders
• Diabetes
• RD needs to consider other disease states when implementing interventions
Nutrition Care Process: Diagnosis
• RD cannot diagnose CD• IDNT Nutrition Diagnostic Terminology
• Intake• Increased nutrient needs (specify) NI-5.1
• Iron• B12• Vitamin D• Calcium
• Clinical• Functional
• Altered GI function NC-1.4
• Biochemical• Impaired nutrient utilization NC-2.1
• Behavioral• Knowledge and Beliefs
• Food and nutrition knowledge related deficit NB-1.1• Not ready for diet/lifestyle change NB-1.3• Limited adherence to nutrient-related recommendations NB-1.6• Undesirable food choices NB-1.7
Nutrition Care Process: Intervention• Gluten-free diet
• Long-term compliance required
• Will improve villous atrophy, GI symptoms, bone density, iron deficiency anemia, pregnancy outcomes, and quality of life
• Lactose-free diet
• Secondary lactase deficiency common with CD
• Damage to villi and impaired enzyme secretion
• As villi heal, lactose can be added back to diet
• Usually not required long-term
Nutrition Care Process: Intervention• Consumption of whole/enriched gluten-free grains and
products
• Still need a source of CHO and fiber, but must be gluten-free
• Rice, wild rice, buckwheat, quinoa, amaranth, millet, oats*
• Oats Controversy
• Oats and oat products are sometimes contaminated with wheat, barley, or rye
• Nutrition practice guidelines say up to 50mg of oats/day is safe and generally tolerated.
• Individuals can tolerate oats as long as oats are from a pure, uncontaminated source
Nutrition Care Process: Intervention• Inclusion of a multivitamin and mineral supplement
• Gluten-free diet may result in low consumption of iron, folate, niacin, B12, calcium, phosphorous, and zinc
• If diet shoes inadequacy, multivitamin supplement is recommended
• Gluten-free
• Age and gender appropriate
• Calcium and vitamin D
• Gluten-free diet may improve but not normalize bone mineral density
• Individuals may have low levels of 25-hydroxy vitamin D
• Increase consumption of calcium and vitamin D
• Through food or supplements
Nutrition Care Process: Intervention• Iron supplementation
• For iron deficiency anemia
• Supplementation to achieve normal levels
• Other measures aimed to increase iron absorption can also be recommended
• Intake of heme-iron
• Intake of iron with ascorbic acid
• Avoiding tannin containing items
Nutrition Care Process: Intervention
• Education on label reading• How to review ingredients on food labels and supplements in order to
avoid sources of gluten • Wheat, rye, barley, malt, oats*
• Education on food cross-contamination• Patient needs to be aware of possible cross contamination of foods with
gluten in manufacturing plants, restaurant, and at home
• Coordination of care• RD may refer patient to another clinical professional based on
coexisting conditions• Gastroenterologists• Endocrinologists• Allergists• Dermatologists• Hepatologists• Pharmacists• Social workers
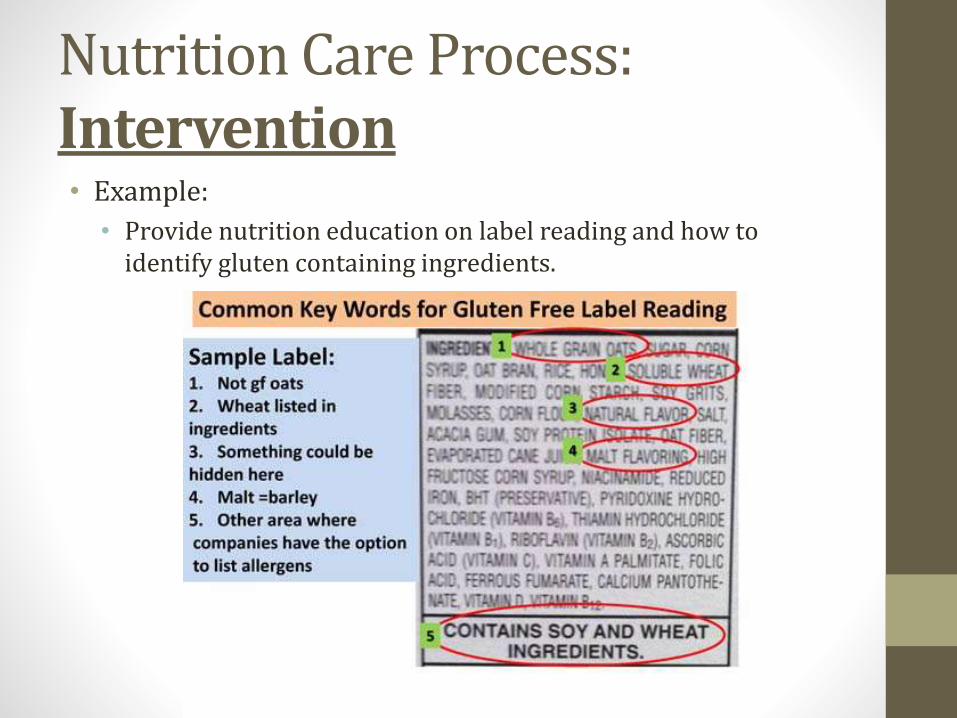
Nutrition Care Process:Intervention• Example:
• Provide nutrition education on label reading and how to identify gluten containing ingredients.
Nutrition Care Process: Intervention
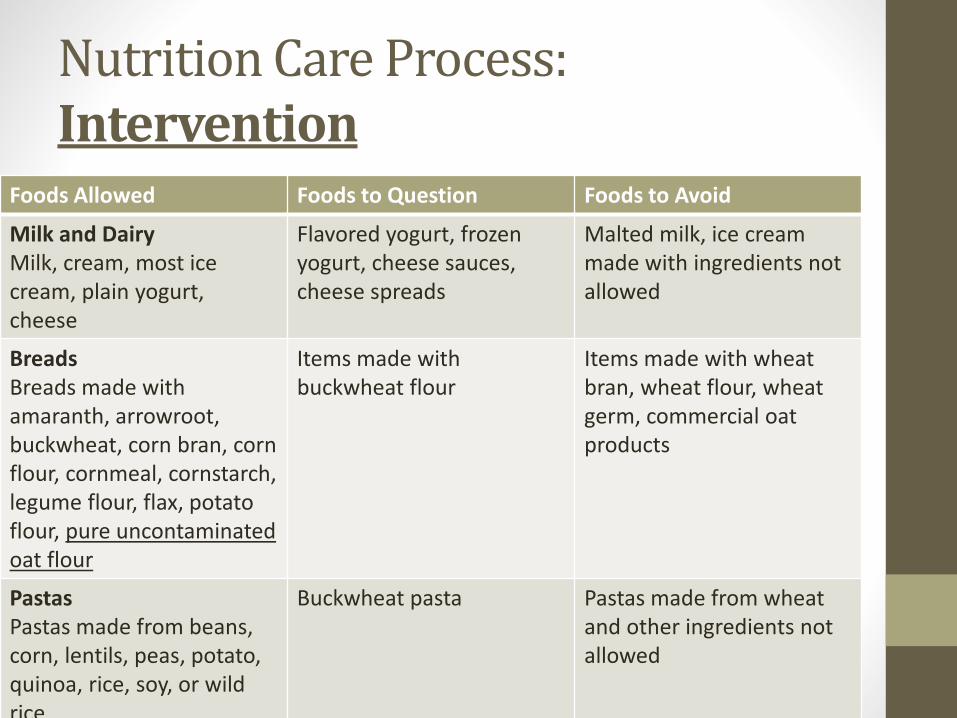
Foods Allowed Foods to Question Foods to Avoid
Milk and DairyMilk, cream, most ice cream, plain yogurt, cheese
Flavored yogurt, frozen yogurt, cheese sauces, cheese spreads
Malted milk, ice cream made with ingredients not allowed
BreadsBreads made with amaranth, arrowroot, buckwheat, corn bran, corn flour, cornmeal, cornstarch, legume flour, flax, potato flour, pure uncontaminated oat flour
Items made with buckwheat flour
Items made with wheat bran, wheat flour, wheat germ, commercial oat products
PastasPastas made from beans, corn, lentils, peas, potato, quinoa, rice, soy, or wild rice
Buckwheat pasta Pastas made from wheatand other ingredients not allowed
Nutrition Care Process: Intervention
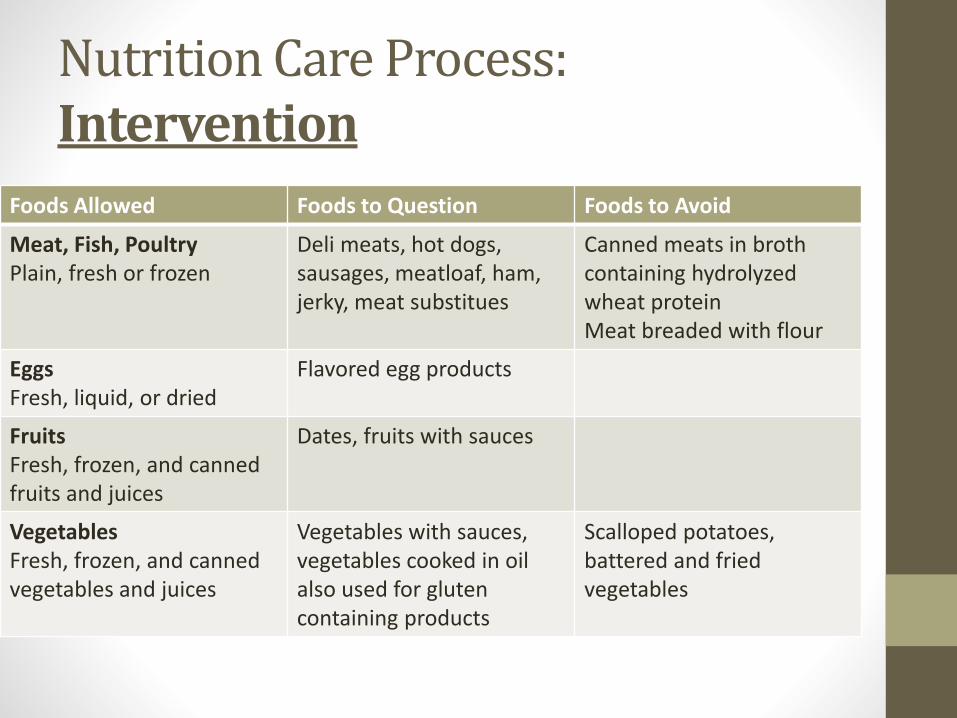
Foods Allowed Foods to Question Foods to Avoid
Meat, Fish, PoultryPlain, fresh or frozen
Deli meats, hot dogs, sausages, meatloaf, ham, jerky, meat substitues
Canned meats in brothcontaining hydrolyzed wheat proteinMeat breaded with flour
EggsFresh, liquid, or dried
Flavored egg products
FruitsFresh, frozen, and canned fruits and juices
Dates, fruits with sauces
VegetablesFresh, frozen, and canned vegetables and juices
Vegetables with sauces, vegetables cooked in oilalso used for gluten containing products
Scalloped potatoes, battered and fried vegetables
Nutrition Care Process: Monitoring and Evaluation• Dietary compliance
• RD needs to monitor • Gluten-free diet
• Antibody levels
• Any exposure to cross contamination
• Any hidden sources of gluten in foods, medications, and supplements
• Monitoring the above is necessary to evaluate dietary compliance
• Factors affecting quality of life• Changes in medical status
• GI, immune, neurological, psychological symptoms
• Changes in social status• Socioeconomic factors, religion, social support, medical support, stress levels
• GI symptoms• Bloating, gas, constipation, diarrhea
• Lactose intolerance
• Infections
• Related cancers
• Gluten-free diet reduces but may not always eliminate symptoms

Sources• 1. Gheller-Rigoni AI, Yale SH, Abdulkarim AS. Celiac disease: celiac sprue, gluten-sensitive enteropathy. Clinical
Medicine and Research. 2004 February;2(1):71-72. Available at: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1069074/. Accessed on October 31, 2014
• 2. Dugdale DC, Longstreth GF, Zieve D. Celiac disease- nutritional considerations- food sources. University of Maryland Medican Center Medical Reference Encyclopedia. 2010. Availble at: http://www.umm.edu/ency/article/002443fod.htm. Accessed on October 31, 2014.
• 3. Nelsen DA. Gluten-sensitive enteropathy (celiac disease): more common than you think. American Family Physician. 2002;66(12):2259-2266. Available at: http://www.aafp.org/afp/2002/1215/p2259.html. Accessed on October 31, 2014.
• 4. Nelms, M., Sucher, K., Lacey, K., et al. Nutrition Therapy and Pathophysiology. 2nd ed. Belmont, CA: Wadsworth/ Cengage Learning; 2011.
• 5. Biagi, F., Corazza, G. R., Clinical features of coeliac disease. Digestive and Liver Disease Journal. 2002 March; 34 (3): 225-228. Available at http://www.sciencedirect.com.libezp.lib.lsu.edu/science/article/pii/S1590865802801979#. Accessed 29 October 2014.
• 6. US Department of Health and Human Services: National Digestive Diseases Information Clearinghouse. Celiac disease. Celiac Disease Awareness Campaign. 2012. Available at: http://digestive.niddk.nih.gov/ddiseases/pubs/celiac/. Accessed on November 2, 2014.
• 7. Academy of Nutrition and Dietetics Evidence Analysis Library. "Celiac Disease Evidence Analysis Project." Academy of Nutrition and Dietetics, Accessed 24 October 2012, http://andevidencelibrary.com/topic.cfm?cat=3726
Sources• 8. Academy of Nutrition and Dietetics Evidence Analysis Library. "Celiac Disease Evidence Analysis Project."
Academy of Nutrition and Dietetics, Accessed 24 October 2012, Available at: http://andevidencelibrary.com/topic.cfm?cat=2826
• 9. Branski, D., Fasano, A., Troncone, R., Latest developments in the pathogenesis and treatment of celiac disease. The Journal of Pediatrics [serial online]. 2006;149(3):295-300. Available at http://www.sciencedirect.com/science/article/pii/S0022347606004975. Accessed November 14, 2014.
• 10. Fasano, A., Zonulin and its regulation of intestinal barrier function:The biological door to inflammation, autoimmunity, and cancer. J Physiological Reviews [serial online]. 2011; 91(1):151-175. Available at http://physrev.physiology.org/content/91/1/151.full. Accessed November 14, 2014.
• 11. Visser, J., Rosing, J., Sapone, A., Lammers, K., Fasano, A., Tight Junctions, Intestinal Permeability, and Autoimmunity Celiac Disease and Type 1 Diabetes Paradigms. NIHPA Author Manuscripts [serial online]. 2009; 1165:195-205. Available at http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2886850/. Accessed November 14, 2014.
• 12. Van Heel, D., Interleukin 15:its role in intestinal inflammation., GUT: An International Journal of Gastroenterology and Hepatology [serial online]. 2006; 55(4):445-445. Available at http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1856192/. Accessed November 14, 2014.
• 13. Fasano, A., Shea-Donohue, T., Mechanisms of Disease: the role of intestinal barrier function in the pathogenesis of gastrointestinal autoimmune diseases. Nature Clinical Practice Gastroenterology and Hepatology [serial online]. 2005; 2(9): 416-422. Available at http://www.elisaact.com/test/pdfs/EAB-Autoimmunity-Intestinal-Barrier.pdf. Accessed November 15, 2014.
















