Embed Size (px)
Citation preview
RICHARD CHAMPLIN, MD
Houston, USA
• Professor and Chair of the Department of Stem Cell Transplantation and Cellular Therapy at the University of Texas MD Anderson Cancer Center
• Dr. Richard Champlin has over 30 years of experience in clinical and translational research involving hematopoietic stem cell transplantation. He has been the President of the American Society of Blood and Marrow Transplantation as well as the Center for International Center for Blood and Marrow Transplantation Research. He was also the board Member of the National Marrow Donor Program and is a current member of the HRSA Advisory Committee for Cord and Stem Cell Transplantation at the MD Anderson Cancer Center. Professor Champlin chairs the Working Committee on Alternative Donors and Cell Sources of the International Bone Marrow Transplant Registry.
Alternative Donors-Now Everyone Can Get a Transplant
Pros and Cons with available options
Richard Champlin, MD
Donor Selection
• Identical twin
• HLA matched sibling
• HLA matched unrelated donor (8 of 8 HLA A,B,C,DRB1 loci)
• Alternative Donors
– Unrelated donor (7 of 8)
– Cord Blood (4 or 5 of 6 HLA A, B, DRB1 loci)
– Haploidentical
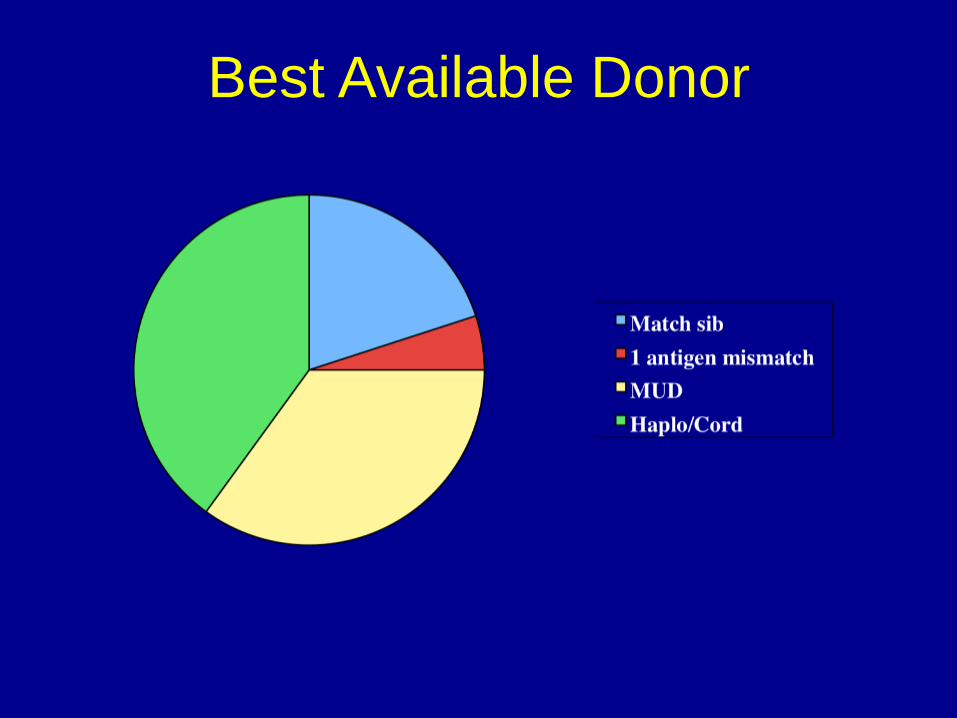
Best Available Donor
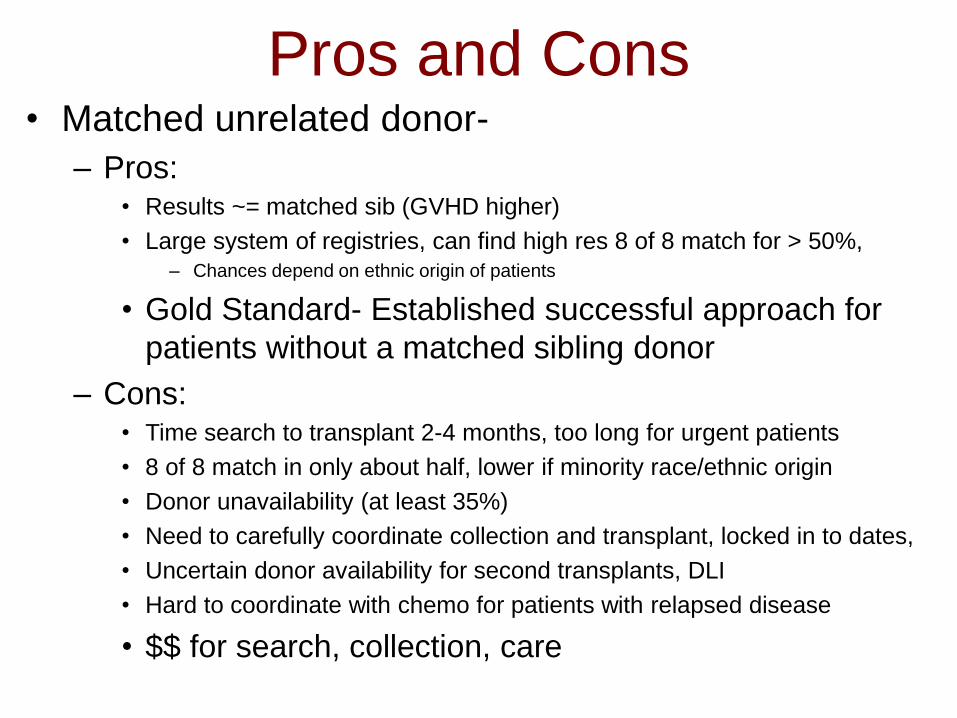
Pros and Cons• Matched unrelated donor-
– Pros: • Results ~= matched sib (GVHD higher)
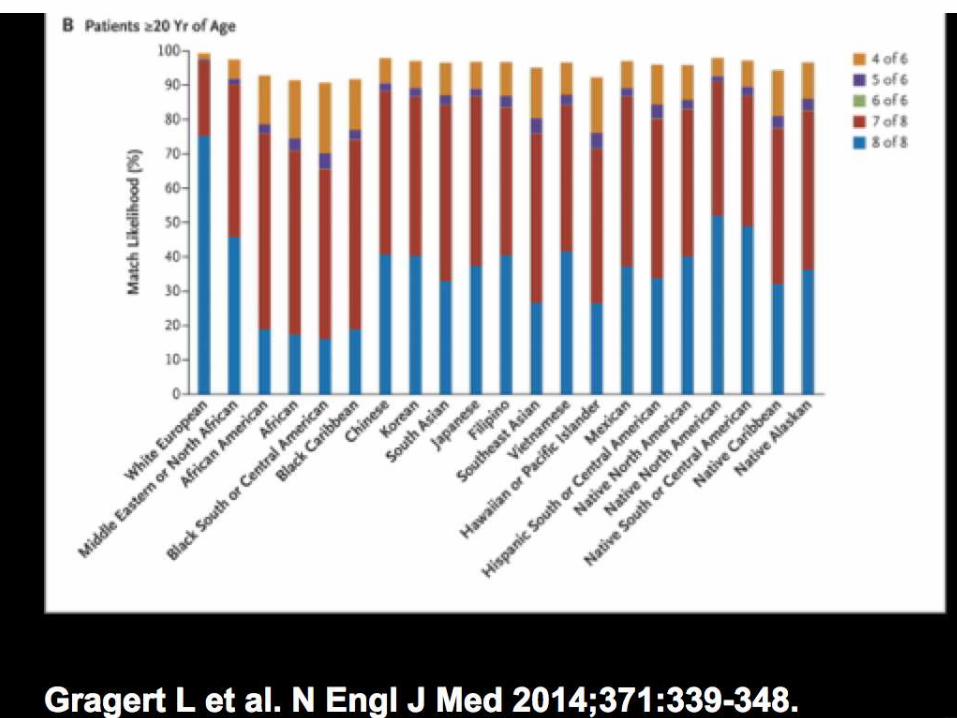
• Large system of registries, can find high res 8 of 8 match for > 50%,– Chances depend on ethnic origin of patients
• Gold Standard- Established successful approach for
patients without a matched sibling donor
– Cons: • Time search to transplant 2-4 months, too long for urgent patients
• 8 of 8 match in only about half, lower if minority race/ethnic origin
• Donor unavailability (at least 35%)
• Need to carefully coordinate collection and transplant, locked in to dates,
• Uncertain donor availability for second transplants, DLI
• Hard to coordinate with chemo for patients with relapsed disease
• $$ for search, collection, care
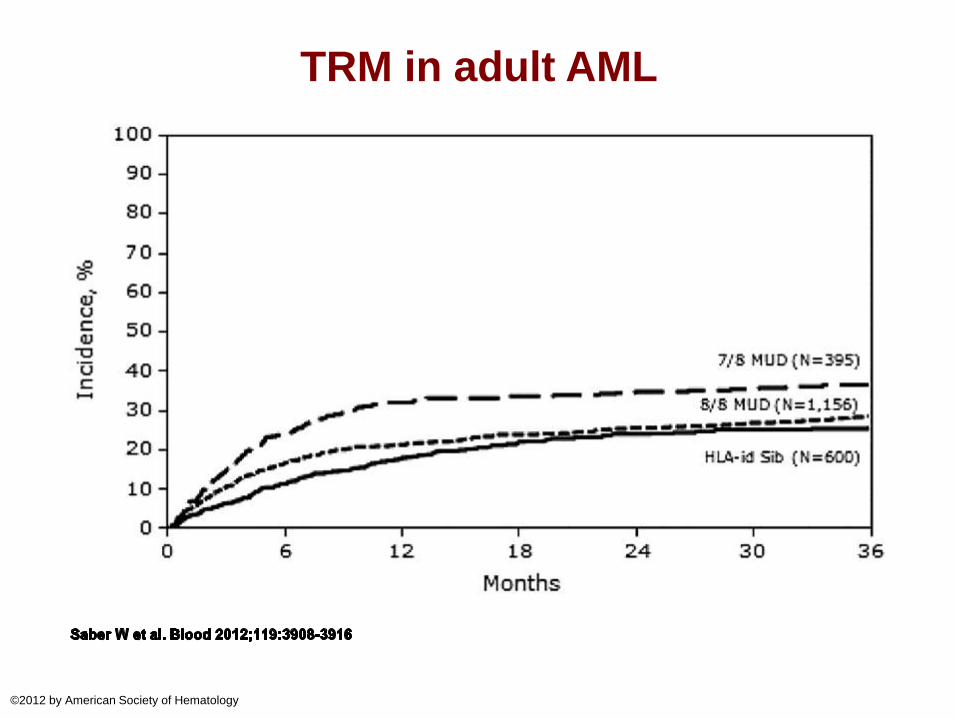
TRM in adult AML
©2012 by American Society of Hematology
Pros and Cons• Cord Blood
– Pros: • Immunologically immature- less prone to produce
GVHD
• Less risk of transmitting infection
• Immunologically naïve- no preexisting immunity
• Can successfully transplant across HLA mismatch
• Can identify 5 of 6 or 4 of 6 match for most patients
• Has potent GVL effect, ?better than BM
• Cells already collected, shorter time search to transplant
• Results improving, = MUD in some studies
• Low rate of chronic GVHD
Pros and Cons• Cord Blood
– Cons:
• Low cell dose, slow recovery hematopoiesis and
immunity,
• Survival depends on cell dose- double cord required for
most adults
• GVHD major problem (with 4 of 6 or 5 of 6 matched Tx)
• Relatively high TRM
• Can’t go back to the donor for more cells or DLI (?CLI)
• Resource intensive – Progress shortening time to
engraftment
– $$$ for cord(s) transplant care
• Need system of banks, cost for collection, QA, storage
Cu
mu
lative
In
cid
en
ce
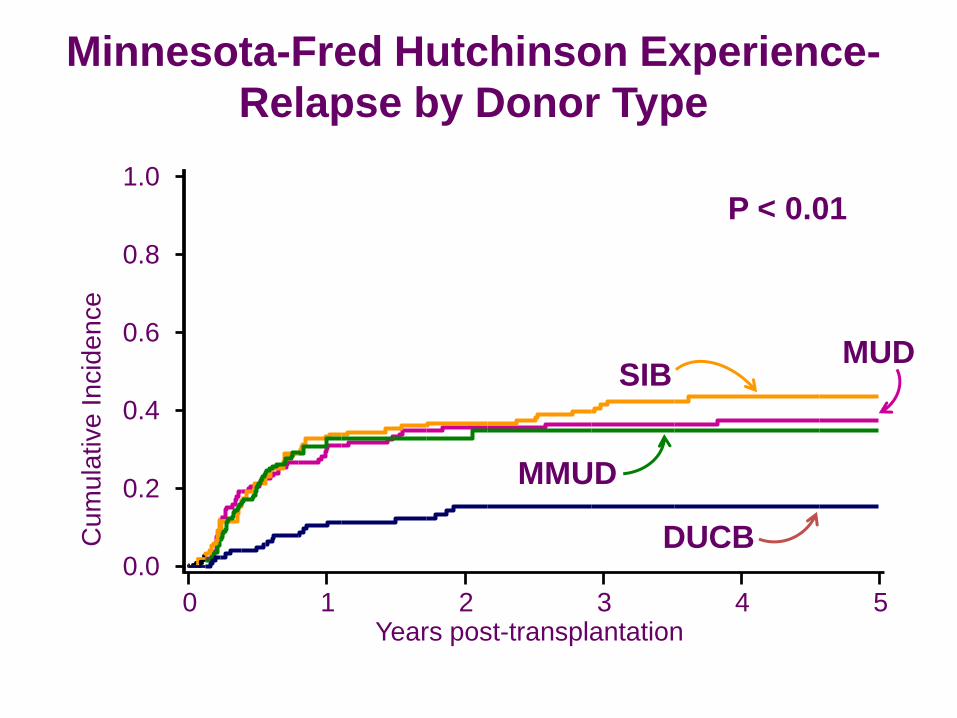
SIB
P < 0.01
MMUD
MUD
DUCB0.0
0.2
0.4
0.6
0.8
1.0
0 1 2 3 4 5Years post-transplantation
Minnesota-Fred Hutchinson Experience-
Relapse by Donor Type
Pros and Cons• Haploidentical related
– Pros:
• Most patients have a haplo match (parent, child,
half of siblings)
• Donor immediately available to transplant center,
allows close coordination with chemotherapy
• Don’t need a registry/ banks
– Major Progress
• T-cell depletion, particularly successful in children– Depletion of alpha/beta T-cells, addition of Tregs
• T-cell replete
• Post transplant cyclophosphamide, tacrolimus, MMF– Low rate of acute and chronic GVHD
Pros and Cons
• Haploidentical related
– Cons
• Ultimate challenge- most alloreactive transplant
• Historically, high rate rejection/GVHD/TRM
• T-cell depletion- slow immune recovery,
variable results, poorer results in adults
• Studies with post transplant cyclophosphamide-
short follow up, question if GVL will be reduced
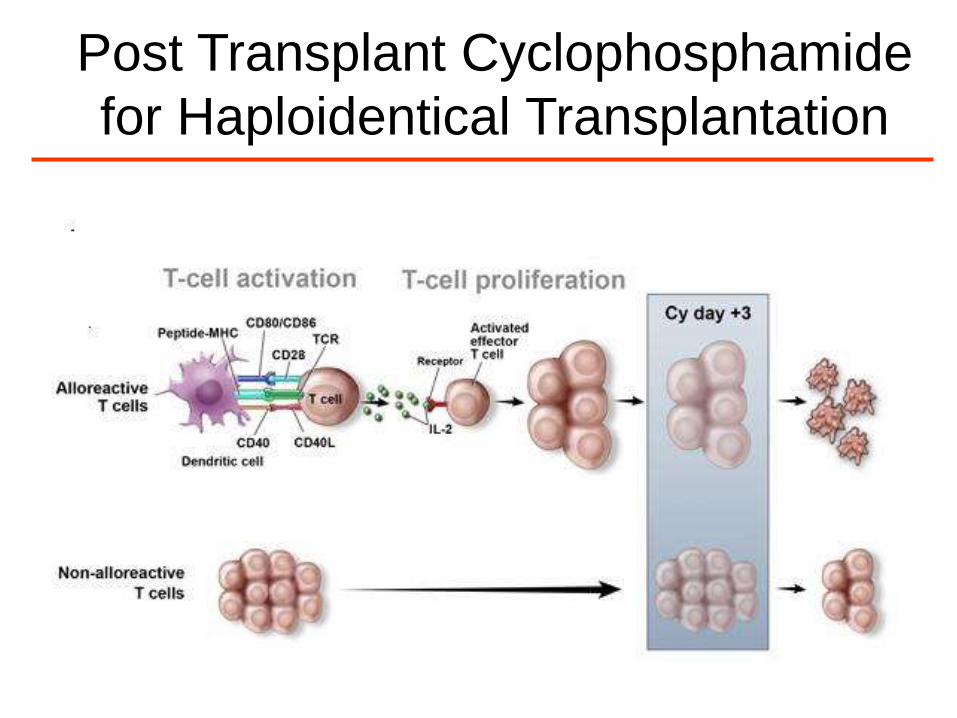
Post Transplant Cyclophosphamide
for Haploidentical Transplantation
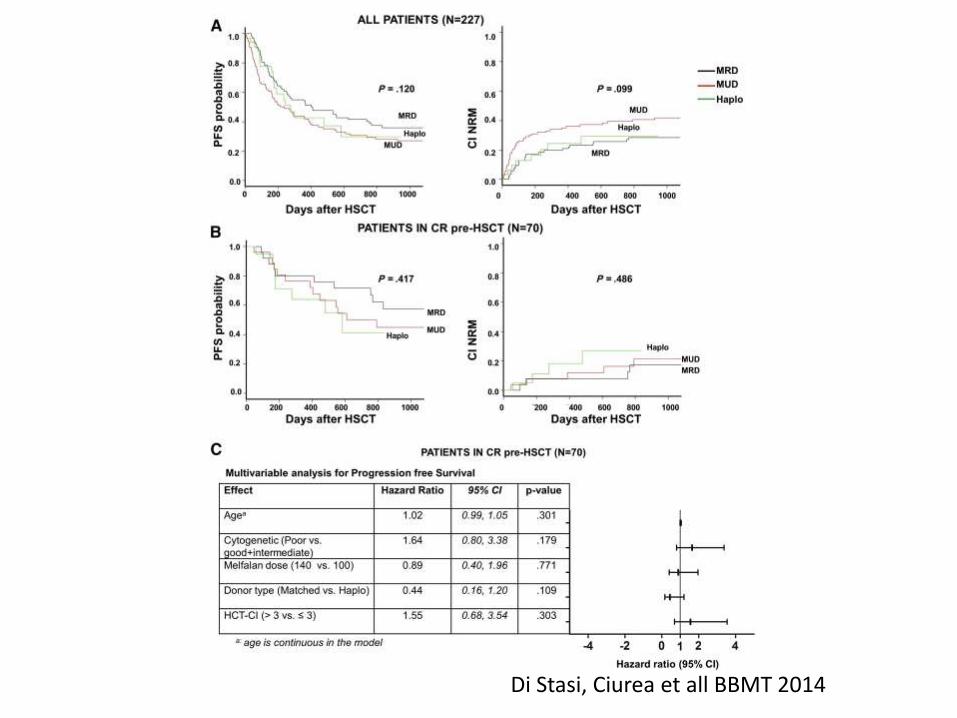
Di Stasi, Ciurea et all BBMT 2014
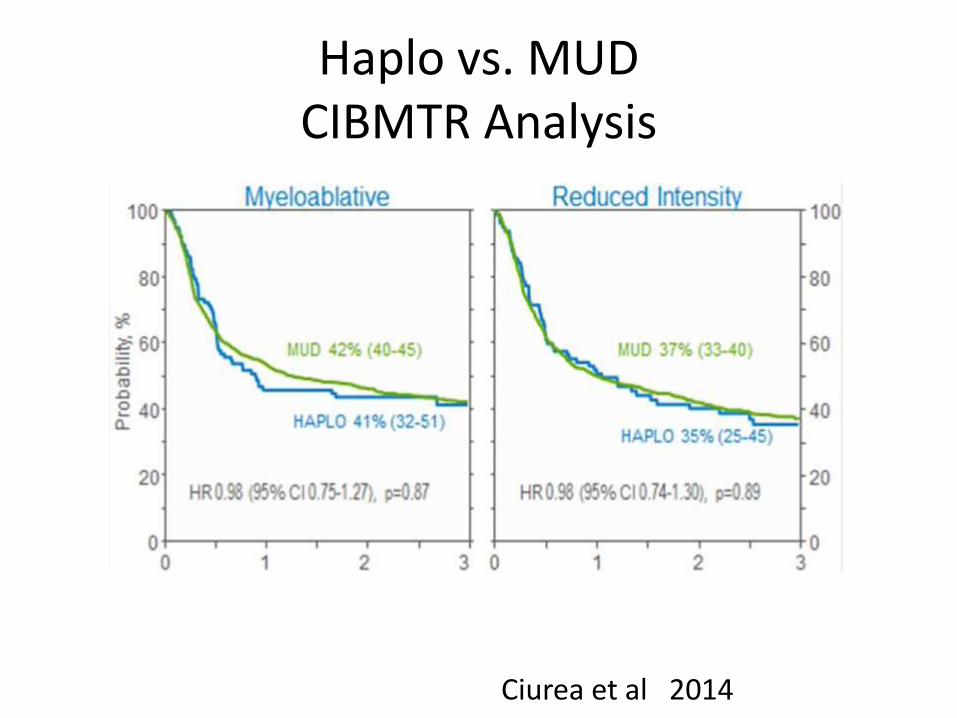
Haplo vs. MUDCIBMTR Analysis
Ciurea et al 2014

Conclusions• Matched sibling preferred donor• Matched unrelated donor- more GVHD, but similar
results for most diagnoses- current gold standard for those without matched sib
• Cord Blood- results similar to MUD in some studies, slower recovery, being addressed with ex vivo expansion technology, greater GVL suggested in some studies
• Haploidentical- improved results with post transplant Cy, similar results to MUD in preliminary studies
• Prospective studies needed to compare modalities• Ultimately each cells source likely to have a role, and
further research is needed to improve each modality
Which Cell Source Will Win?
• I don’t know.
• Innovative strategies to improve outcomes are
needed with all cell sources- premature to pick
a winner.
– Cord Blood: ? Advantage for GVL; problem is
GVHD, immune reconstitution
– Haplo- Good control of GVHD; post transplant Cy
likely to impair GVL; major problem may be relapse
• BMT CTN randomized study to directly
compare double cord blood vs. haplo
• BMT CTN proposed study to compare haplo vs.
MUD- hypothesize shorter time to transplant
would favor haploidentical transplant