Embed Size (px)
Citation preview

CASE PRESENTATION & REVIEW OF LITERATURE

52 yr old male from Theog
Date & time of presentation in casualty- 7th May 2014/9:20
pm
Chief complaints: Back pain since 7th May 2014/7:30 pm

HOPI- Patient was apparently asymptomatic till about 2 hours ago when he was travelling to Theog on his motorcycle when he started having back pain: localised to interscapular region, sudden in onset, severe in intensity, stabbing in nature, radiating to the front of chest, no aggravating or relieving factors
no h/o any associated sweating no h/o presyncope/syncope no h/o LOC/weakness of any limb no h/o SOB/palpitations no h/o fever/cough no h/o any recent trauma/lifting heavy weights

PAST HISTORY- no h/o similar episodes in past not a k/c/o HTN/DM/CAD PERSONAL HISTORY- smoker with a SI=360(12*30) occasional alcoholic non vegetarian no h/o any illicit drug abuse engineer in PWD deptt.
FAMILY HISTORY- no family history of HTN/DM/CAD no h/o any sudden death in family

ExaminationGPE: conscious , restless, oriented to T/P/P BP
PR(right radial) 74/min regular, good volume P-/I-/Cy-/Cl-/LAP-/JVP-/PE- No radio-radial/radio-femoral delay No pulsus paradoxus Kussmaul sign negative
no local tenderness on chest/back
Rt arm 190/110 Lt arm 172/100
Radial Femoral Popiliteal
Post tibial
Dors pedis
Rt +++ ++ ++ ++ +Lt ++ ++ ++ ++ +

Respiratory: trachea central, b/l symmetrical, both sides moving equally, b/l VBS with no added sounds
CVS- precordium normal S1 S2 normal no added sounds
P/A- soft, slight tenderness in epigastrium, G-/R-/RT-
CNS- HMF/motor/sensory /CN/speech-NAD plantars- b/l flexor response

Fundus examn- no e/o hypertensive
retinopathy
ECG- normal axis, HR 74/min, no e/o any
chamber hypertrophy
CXR PA view(portable): NAD
Troponin-T : negative

Provisional diagnosis? AORTIC DISSECTION??CAD:ACS:USA

RBS 138 mg%
S.Na+ 141S.K+ 3.7 meq/lS.Cl- 111
Urea 69Creatinine 2.3 mg%
Urine for RBC- no RBC seen
TLC 8400/ mm3
Hb 10.9 g/dl

CECT AORTIC ANGIOGRAPHY: flap in the aorta dividing it into true and false
lumens just after the origin of the left subclavian artery upto the level of aortic bifurcation
“STANFORD Type B Aortic Dissection with multiple hepatic and renal cysts ?ADPKD”



Final diagnosisStanford type B aortic dissection with ?AKI ?Acute on CKD with ?ADPKD

CoursePatient was managed with antihypertensives( NTG infusion
and I/V beta blockers) and analgesic support (morphine).
Consultation taken from Cardiology and CTVS departments for any intervention.
As the patient was still in severe pain despite analgesics and had started experiencing signs of vital organ damage, we were advised referral to higher centre.
Due to inavailability of stent at the higher centre the intervention was delayed for 2 days. Eventually endovascular intervention done on 3rd day after referral.
Patient collapsed on the 4th day after referral.

Review of Literature

Acute aortic dissection is the most common catastrophic event affecting the aorta with an estimated annual incidence of approximately 5 to 30 per million.
The early mortality rate: 1-2% per hour reported in the first several hours after dissection occurs
Twice more common in men than in womenAortic dissection is more common in blacks than
in whites and is less common in Asians than in whites.
MC age group: 50-60 years (ascending) 60-70 years (descending)Patients with Marfan syndrome present earlier,
usually in the third and fourth decades of life.The International Registry of Acute Aortic Dissection (IRAD): new insights into an old disease.

Two main hypothesis: first- primary tear in aortic intima -> blood in the
aortic lumen penetrates into the diseased media leading to dissection -> creation of true and false lumen
second- primary rupture of vasa vasorum -> hemorrhage in the aortic wall -> subsequent intimal disruption -> intimal tear -> dissection

The pressure of the pulsatile blood within the aortic wall after dissection leads to the extension of dissection.
Usually propagate in antegrade direction.
Arterial pressure and shear forces may lead to further tears in the intimal flap producing exit sites or additional entry sites for blood flow into the false lumen.
Distension of the false lumen with blood causes the intimal flap to compress the true lumen, narrowing its caliber and distorting its shape, which leads to malperfusion


Classification

Most ascending aortic dissections begin within a few centimeters of the aortic valve and most descending dissections have their origin just distal to the the left subclavian artery.
Approx 65% intimal tears in ascending aorta, 30% in descending aorta, <10% in aortic arch, and approx 1% in abdominal aorta.
The treatment depends on the site with emergency surgery recommended for acute type A dissections and initial medical management for type B dissections.
Also classified according to its duration: acute <2 weeks
chronic >2 weeks
The morbidity and mortality rates of acute dissection are highest in the first 2 weeks , especially within the first 24 hours

Causes •Approximately 75% of all pts have HTN
•Cystic medial degeneration is the chief predisposing factor in aortic dissection. Cystic medial degeneration is an intrinsic feature of several hereditary defects of connective tissue, most notably Marfan and Ehlers-Danlos syndromes, and is also common among patients with bicuspid aortic valve. In fact, Marfan syndrome accounts for 5 percent of all aortic dissections.
•Pregnancy can be a risk factor for aortic dissection, particularly in patients with an underlying anomaly such as Marfan syndrome. An estimated 50% of all cases of aortic dissection that occur in women younger than 40 years are associated with pregnancy. Most cases occur in the third trimester or early postpartum period.
Wilson SK, Hutchins GM. Aortic dissecting aneurysms:causative factors in 204 subjects. Arch Pathol Lab Med 1982

Clinical manifestationsThe most common initial symptom of acute aortic dissection
is pain, which is found in up to 96 percent of cases, whereas the large majority of those without pain are found to have chronic dissections.
The pain is typically severe and of sudden onset and is as severe at its inception as it ever becomes, in contrast to the pain of myocardial infarction, which usually has a crescendo-like onset and is not as intense. In fact, the pain of aortic dissection may be all but unbearable in some instances and force the patient to writhe in agony, fall to the ground, or pace restlessly in an attempt to gain relief.
Several features of the pain should arouse suspicion of aortic dissection. The quality of the pain as described by the patient is often morbidly appropriate to the actual event, with adjectives such as “tearing,” “ripping,” “sharp,” and “stabbing” frequently used in more than one half the cases.

Another important characteristic of the pain of aortic dissection is its tendency to migrate from its point of origin to other sites, generally following the path of the dissection as it extends through the aorta. However, such migratory pain is described in as few as 17 percent of cases.
Spittell and colleagues found that when the location of chest pain was anterior only (or if the most severe pain was anterior), more than 90 percent of patients had involvement of the ascending aorta. Conversely, when the chest pain was interscapular only (or when the most severe pain was interscapular), more than 90 percent of patients had involvement of the descending thoracic aorta (i.e., DeBakey type I or III).
The presence of any pain in the neck, throat, jaw, or face strongly predicted involvement of the ascending aorta, whereas pain anywhere in the back, abdomen, or lower extremities strongly predicted involvement of the descending aorta.
Spittell PCet al. Clinical features and differential diagnosis of aortic dissection: experiencewith 236 cases (1980 through 1990). Mayo Clin Proc 1993;68:642–651

Less common symptoms at initial evaluation, occurring with or without associated chest pain, include congestive heart failure (7 percent), syncope (13 percent), cerebrovascular accident (6 percent), ischemic peripheral neuropathy, paraplegia, and cardiac arrest or sudden death.
Patients may have abdominal pain and on occasion, develop severe nausea and vomiting related to abdominal visceral involvement. These symptoms may delay diagnosis and increase mortality rate.
Painless aortic dissection was reported in 6% of the patients in one study and was more commonly associated with diabetes, prior aortic aneurysm, and prior cardiac surgery. Hirst AE Jr, Johns VJ Jr, Kime SW Jr. Dissecting aneurysms of the aorta: a review of 505 cases. Medicine 1995; 37:217–279

Physical findingsHypertension is seen in 70 percent of patients with distal
aortic dissection but in only 36 percent with proximal dissection.
Hypotension, on the other hand, occurs much more commonly among those with proximal than those with distal aortic dissection (25 and 4 percent, respectively).
True hypotension is usually the result of cardiac tamponade, acute severe aortic regurgitation, intrapleural rupture, or intraperitoneal rupture. Dissection involving the brachiocephalic vessels may result in pseudohypotension, an inaccurate measurement of blood pressure caused by compromise or occlusion of the brachial arteries.
An interarm blood pressure differential greater than 20 mm Hg should increase the suspicion of aortic dissection, but it does not rule it in. Significant interarm blood pressure differentials may be found in 20% of people without aortic dissection.

Acute, severe aortic regurgitation may result in signs suggestive of congestive heart failure: dyspnea, orthopnea, bibasilar crackles, or elevated jugular venous pressure.
Other cardiovascular manifestations include findings suggestive of cardiac tamponade (eg, muffled heart sounds, hypotension, pulsus paradoxus, jugular venous distention, Kussmaul sign). Tamponade must be recognized promptly.
Patients with right coronary artery ostial dissection may present with acute myocardial infarction, commonly inferior myocardial infarction. It remains essential that when evaluating patients with acute myocardial infarction, particularly inferior infarctions, one carefully considers the possibility of an underlying aortic dissection before thrombolytic or anticoagulant therapy is instituted.

Neurologic deficits are a presenting sign in up to 20% of cases. The most common neurologic findings are syncope and altered mental status
Extension of aortic dissection into the abdominal aorta can cause other vascular complications. Compromise of one or both renal arteries occurs in about 5 to 8 percent and can lead to renal ischemia or frank infarction and, eventually, severe hypertension and acute kidney injury.
Mesenteric ischemia and infarction—occasional and potentially lethal complications of abdominal dissection—occur in 3 to 5 percent of cases.
In addition, aortic dissection may extend into the iliac arteries and cause diminished femoral pulses (12 percent) and acute lower extremity ischemia.

Additional clinical manifestations of aortic dissection include the presence of small pleural effusions, seen more commonly on the left side.
The physical findings most typically associated with aortic dissection—pulse deficits, the murmur of aortic regurgitation, and neurological manifestations—are more characteristic of proximal than of distal dissection. Reduced or absent pulses in patients with acute chest pain strongly suggests the presence of aortic dissection. Such pulse abnormalities are present in about 30 percent of proximal aortic dissections and occur throughout the arterial tree, but occur in only 15 percent of distal dissections, where they usually involve the femoral or left subclavian artery.

DIAGNOSIS CHEST X RAY: Although chest radiography may help
support a diagnosis of suspected aortic dissection, the findings are nonspecific and rarely diagnostic.
The most common abnormality seen on a chest radiograph in cases of aortic dissection is widening of the aortic silhouette, which appears in 81 to 90 percent of cases. Less often, nonspecific widening of the superior mediastinum is seen. If calcification of the aortic knob is present, separation of the intimal calcification from the outer aortic soft tissue border by more than 1.0 cm—the “calcium sign”—is suggestive, although not diagnostic, of aortic dissection. Pleural effusions are common, typically occur on the left side, and are more often associated with dissection involving the descending aorta.
Up to 12 percent, have chest radiographs that appear unremarkable. Therefore, a normal chest radiograph can never exclude the presence of aortic dissection.


ECG-Electrocardiographic findings in patients with aortic dissection are nonspecific.
One third of electrocardiograms show changes consistent with left ventricular hypertrophy, whereas another one third are normal.
In acute thoracic aortic dissection, the ECG changes can mimic those seen in acute cardiac ischemia. In the presence of chest pain, these signs can make distinguishing dissection from acute myocardial infarction very. Keep this in mind when administering thrombolytics to patients with chest pain.
The incidence of abnormal ECG findings is greater in Stanford type A dissections than in other types of dissections. ST segment elevation can be seen in Stanford type A dissections because the dissection interrupts blood flow to the coronary arteries. In one study, 8% of patients with type A dissections had ST segment elevation, whereas no patients with type B dissections had ST segment elevation. More commonly, the ECG abnormality is ST segment depression.
If the dissection involves the coronary ostia, the right coronary artery is most commonly involved. This can result in ST segment elevation in leads II, III, and aVF, a pattern similar to that seen in inferior wall infarctions.

D-dimer:In a series comparing 94 consecutive patients
with aortic dissection and 94 controls, a d-dimer of >400 ng/ml had a sensitivity of 99 percent and a specificity of 34 percent. Moreover, D-dimer levels correlated with the anatomical extent of the dissection and with in-hospital mortality.
This suggests that D-dimer levels may be useful as a screening test in the emergency department, with elevated levels prompting at least clinical consideration, if not diagnostic investigation, of possible aortic dissection.

Myocardial muscle creatine kinase isoenzyme, myoglobin, and troponin I and T levels are elevated if the dissection has involved the coronary arteries and caused myocardial ischemia. The lactate dehydrogenase level may be elevated because of hemolysis in the false lumen.
Measurement of the degradation products of plasma fibrin and fibrinogen can facilitate the diagnosis of acute aortic dissection. In symptomatic patients, aortic dissection with a patent false lumen should be considered if the plasma fibrin degradation product (FDP) level is 12.6 μg/mL or higher; the possibility of dissection with complete thrombosis of the false lumen should be considered if the FDP level is 5.6 μg/mL or higher.
A smooth muscle myosin heavy-chain assay is performed in the first 24 hours. Increased levels in the first 24 hours are 90% sensitive and 97% specific for aortic dissection. Levels are highest in the first 3 hours. A cutoff of 2.5 has a sensitivity of 91%, a specificity of 98%, and an accuracy rate of 96%, respectively.

Once suspected on clinical grounds, it is essential to confirm the diagnosis of aortic dissection both promptly and accurately. The modalities currently available for this purpose include
AortographyContrast-enhanced CTMRI TTE or TEE

Aortography-The diagnosis of aortic dissection is based on direct angiographic signs, including visualization of two lumina or an intimal flap (considered diagnostic) or on indirect signs (considered suggestive), such as deformity of the aortic lumen, thickening of the aortic walls, branch vessel abnormalities, and aortic regurgitation. Prospective studies have found that for the diagnosis of aortic dissection, the sensitivity of aortography is 88 percent and the specificity is 94 percent.

Contrast-enhanced CT scanning- In contrast-enhanced CT scanning, aortic dissection is diagnosed by the presence of two distinct aortic lumina, either visibly separated by an intimal flap or distinguished by a differential rate of contrast opacification. Several series have found that spiral CT scanning has both a sensitivity and specificity for acute aortic dissection of 96 to 100 percent.
CT is helpful in identifying the presence of thrombus in the false lumen and in detecting pericardial effusion.
The use of CT angiography permits assessment of branch vessel compromise in both the thoracic and abdominal segments.



MRI- Magnetic resonance imaging has both a
sensitivity and a specificity of approximately 98 percent. Intravenous administration of gadolinium yields a magnetic resonance angiogram, which defines the patency of aortic branch vessels. Still, MRI does have a number of disadvantages. MRI provides only limited images of branch vessels (unless gadolinium is used) and does not consistently identify the presence of aortic regurgitation. In most hospitals, magnetic resonance scanners are not readily available on an emergency basis.

Echocardiography is well suited for the evaluation of patients with suspected aortic dissection because it is readily available in most hospitals, it is noninvasive and quick to perform, and the full examination can be completed at the bedside.
The echocardiographic finding considered diagnostic of an aortic dissection is the presence of an undulating intimal flap within the aortic lumen that separates the true and false channels. Reverberations and other artifacts can cause linear echodensities within the aortic lumen that mimic aortic dissection. To distinguish an intimal flap definitively from such artifacts, the flap should be identified in more than one view, it should have motion independent of that of the aortic walls or other cardiac structures, and a differential in color Doppler flow patterns should be noted between the two lumina.

Transthoracic echocardiography has a sensitivity of 59 to 85 percent and a specificity of 63 to 96 percent for the diagnosis of aortic dissection. Such poor sensitivity significantly limits the general usefulness of this technique.
The results of large prospective studies have demonstrated that the sensitivity of TEE for aortic dissection is 98 to 99 percent, whereas the sensitivity for detecting an intimal tear is 73 percent.
TEE detects both aortic regurgitation and pericardial effusion in 100 percent of cases. The specificity of TEE for the diagnosis of aortic dissection is less well defined but is likely in the range of 94 to 97 percent.

In a setting in which all these imaging modalities are available, CT should be considered first in the evaluation of suspected aortic dissection in light of its accuracy, safety, speed, and convenience.
When CT identifies a type A aortic dissection, the patient may be taken directly to the operating room, where TEE can then be performed to assess the anatomy and competence of the aortic valve without unduly delaying surgery.
However, in cases of suspected aortic dissection in which aortic valve disease is suspected or the patient is unstable, TEE may be the initial procedure of choice.

Management
Therapy for aortic dissection aims to halt progression of the dissecting hematoma because lethal complications arise not from the intimal tear itself but rather from the subsequent course taken by the dissecting aorta, such as vascular compromise or aortic rupture. Without treatment, aortic dissection has a high mortality rate.

Aggressive medical treatment of aortic dissection was first advocated by Wheat and colleagues in the 1960s. The authors established reduction of systolic blood pressure and diminution of the rate of left ventricular ejection (dP/dt) as the two primary goals of pharmacological therapy.
Originally introduced for patients too ill to withstand surgery, medical therapy is now the initial treatment for virtually all patients with aortic dissection before definitive diagnosis and furthermore serves as the primary long-term therapy in a subset of patients, particularly those with distal dissections.

Initial therapyInitial therapeutic goals include the elimination of pain and
reduction of systolic blood pressure to 100 to 120 mm Hg (mean of 60 to 75 mm Hg) or the lowest level commensurate with adequate vital organ (cardiac, cerebral, renal) perfusion. Beta-blocking agents should be administered simultaneously, regardless of whether pain or systolic hypertension is present. Pain, which may itself exacerbate hypertension and tachycardia, should be promptly treated with intravenous morphine sulfate.
For the acute reduction of arterial pressure, the potent vasodilator sodium nitroprusside is effective. When used alone, however, sodium nitroprusside can actually cause an increase in dP/dt, which in turn may potentially contribute to propagation of the dissection. Therefore, concomitant beta-blocking treatment is essential. For those patients with acute or chronic renal insufficiency, intravenous fenoldopam may be preferable to sodium nitroprusside.

To reduce dP/dt acutely, an intravenous beta blocker should be administered in incremental doses until evidence of satisfactory beta blockade is noted, usually indicated by a heart rate of 60 to 80 beats/min in the acute setting. Because propranolol was the first generally available beta blocker, it has been used most widely in treating aortic dissection.
Labetalol, which acts as both an alpha- and a beta-adrenergic receptor blocker, can be especially useful in the setting of aortic dissection because it effectively lowers both dP/dt and arterial pressure.
The ultra-short-acting beta blocker esmolol may be particularly useful in patients with labile arterial pressure, especially if surgery is planned, because use of this drug can be abruptly discontinued if necessary.

When contraindications exist to the use of beta blockers—including severe sinus bradycardia, second- or third-degree atrioventricular block, congestive heart failure, or bronchospasm—other agents to reduce arterial pressure and dP/dt should be considered. Calcium channel antagonists, which are effective in managing hypertensive crisis, are used on occasion in the treatment of aortic dissection. The combined vasodilator and negative inotropic effects of both diltiazem and verapamil make these agents well suited for the treatment of aortic dissection. Moreover, these agents may be administered intravenously.
Refractory hypertension may result when a dissection flap compromises one or both of the renal arteries, thereby causing the release of large amounts of renin. In this situation, the most efficacious antihypertensive may be the intravenous angiotensin-converting enzyme (ACE) inhibitor enalaprilat.

In the event that a patient with suspected aortic dissection has significant hypotension, rapid volume expansion should be considered, given the possible presence of cardiac tamponade or aortic rupture. Before initiating aggressive treatment of such hypotension, however, the possibility of pseudohypotension, which occurs when arterial pressure is being measured in an extremity where the circulation is selectively compromised by the dissection, should be carefully excluded. If vasopressors are absolutely required for refractory hypotension, norepinephrine or phenylephrine is preferred. Dopamine should be reserved for improving renal perfusion and used only at very low doses, given that it may raise dP/dt.

When a patient with acute aortic dissection complicated by cardiac tamponade is relatively stable, the risks of pericardiocentesis probably outweigh the benefits and every effort should be made to proceed as urgently as possible to the operating room for direct surgical repair of the aorta with intraoperative drainage of the hemopericardium.
However, when patients have pulseless electrical activity or marked hypotension, an attempt to resuscitate the patient with pericardiocentesis is warranted and may indeed be successful. A prudent strategy in such cases is to aspirate only enough pericardial fluid to raise blood pressure to the lowest acceptable level.

Definitive Therapy

Definitive surgical therapy was pioneered by DeBakey and colleagues in the early 1950s.
The usual objectives of definitive surgical therapy include resection of the most severely damaged segment of aorta, excision of the intimal tear when possible, and obliteration of entry into the false lumen by suturing of the edges of the dissected aorta both proximally and distally. After the diseased segment containing the intimal tear is resected, typically a segment of the ascending aorta in proximal dissections or the proximal descending aorta in distal dissections, aortic continuity is then reestablished by interposing a prosthetic sleeve graft between the two ends of the aorta.
One of the more promising avenues of investigation is the use of endovascular techniques for treating high-risk patients with aortic dissection. More recently, intraluminal stent-grafts placed percutaneously by the transfemoral catheter technique have been introduced as a potential alternative to aortic repair. This procedure aims to close the site of entry into the false lumen (intimal tear), decompress and promote thrombosis of the false lumen, and relieve any obstruction of branch vessels that may accompany the dissection.


When patients with type B aortic dissection are managed medically, in addition to the reduction in dP/dt and heart rate, a second goal is to monitor the patient vigilantly for any evidence of branch arterial compromise, with the most lethal consequence being mesenteric ischemia.
Late follow-up of patients leaving the hospital with treated aortic dissection shows an actual survival rate not much worse than that of individuals of comparable age without dissection. No significant differences are seen among discharged patients when comparing proximal versus distal dissection, acute versus chronic dissection, or medical versus surgical treatment. Five-year survival rates for all these groups (among discharged patients) are typically 75 to 82 percent.
Thus, the initial success of surgical or medical therapy is usually sustained on long-term follow-up. Late complications include aortic regurgitation, recurrent dissection, and aneurysm formation or rupture. The presence of a persistently patent false lumen is one of the strongest predictors of adverse late outcomes, including more rapid aortic dilatation, a greater likelihood of requiring subsequent aortic surgery, and late mortality.

Long-term medical therapy to control hypertension and reduce dP/dt is indicated for all patients who have sustained an aortic dissection, regardless of whether their in-hospital definitive treatment was surgical or medical.
Systolic blood pressure should be maintained at or below 130 mm Hg. The preferred agents are beta blockers or, if contraindicated, other agents with a negative inotropic as well as a hypotensive effect, such as verapamil or diltiazem. ACE inhibitors and angiotensin receptor blockers are attractive antihypertensive agents for treating aortic dissection and may be of particular benefit in patients with some degree of renal ischemia as a consequence of the dissection. Pure vasodilators, such as dihydropyridine calcium channel antagonists or hydralazine, may cause an increase in dP/dt and should therefore be used only in conjunction with adequate beta blockade.

Follow-up evaluation of patients after aortic dissection should include serial aortic imaging with CT, MRI, or TEE.
Patients are at highest risk immediately after hospitalization and during the first 2 years, with the risk progressively declining thereafter. It is therefore important to have more frequent early follow-up; for example, patients can be seen and imaged at 1, 3, and 6 months initially and then return every 6 months for 2 years, after which time they can often be re-imaged at 12-month intervals, depending on the given patient's risk.

In its natural evolution, without treatment, acute type A aortic dissection reportedly has a mortality rate of about 1% per hour initially, with half of the patients expected to be dead by the 3rd day, and almost 80% by the end of the 2nd week.
Death rates are lower but still significant in acute type B aortic dissection: 10% minimum at 30 days, and 70% or more in the highest-risk groups.
Hagan PG, Nienaber CA, Isselbacher EM, Bruckman D, Karavite DJ, Russman PL, et al. The International Registry of Acute Aortic Dissection (IRAD): new insights into an old disease. JAMA 2000;283(7):897–903.

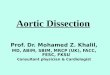
Atypical Aortic DissectionIn aortic dissection as classically described, two other
diseases of the aorta are closely related, intramural hematoma of the aorta and penetrating atherosclerotic ulcer of the aorta. These two conditions share with aortic dissection many of the predisposing risk factors and initial symptoms, and indeed, both may lead to either classic aortic dissection or aortic rupture. In light of their clinical similarities, it is appropriate to consider classic aortic dissection and its variants collectively among the “acute thoracic aortic syndromes,” a category that also includes traumatic aortic transection and rupture, contained rupture (pseudoaneurysm), or acute expansion of thoracic aortic aneurysms.

Schematic of aortic dissection (left), penetrating ulcer (middle), and IMH (right).
Tsai T T et al. Circulation. 2005;112:3802-3813




Thanks
The tragedies of life are largely arterial — Sir William Osler