British Journalof Plastic Surgery (1992), 45,59-61
Transtibial transposition of gastsocnemius muscle and musculscutaneons
orris and J. J. Pribaz
Barney Hospital, Dorchester, Massachusetts and Harvard Medical School/Brigham and Woman’s hospital, Boston, Massachusetts, US.A
SUMMARY. The medial and lateral gastrocnemins muscle flaps have become the workhorses of prohal calf reconstruction since their initial description by M&raw et al. in 1977. Since that time many authors have presented varying and often ingeniotns techniques by which the range of these flaps can be expanded, This report adds anotber modi@cation of the standiurd gastrocnemius muscle flap: transtibiad transposition of the muscle tbrougb the posterior cortex.
The medial and lateral gastocnemius muscle flaps have become the workhorses of proximal calf recon- struction evet since their initial description by McGraw et al.. (1977). Since that time many authors have presented varying and often ingenious techniques by which the range of these flaps can be expanded. Arnold and Mixter (1983) presented a case of transposition of a gastrocnemius flap through a bony defect after a failed total knee replacement. The principal of filling bony dead space with healthy vascularised tissue is now universally accepted.
This report adds another modification of the standard gastrocnemius muscle flap : transtibial trans- position of the muscle through the posterior cortex, which may oEer a better route than prior techniques.
Case reports
Case d a 5%year-old parks department foreman suffered a shrapnel
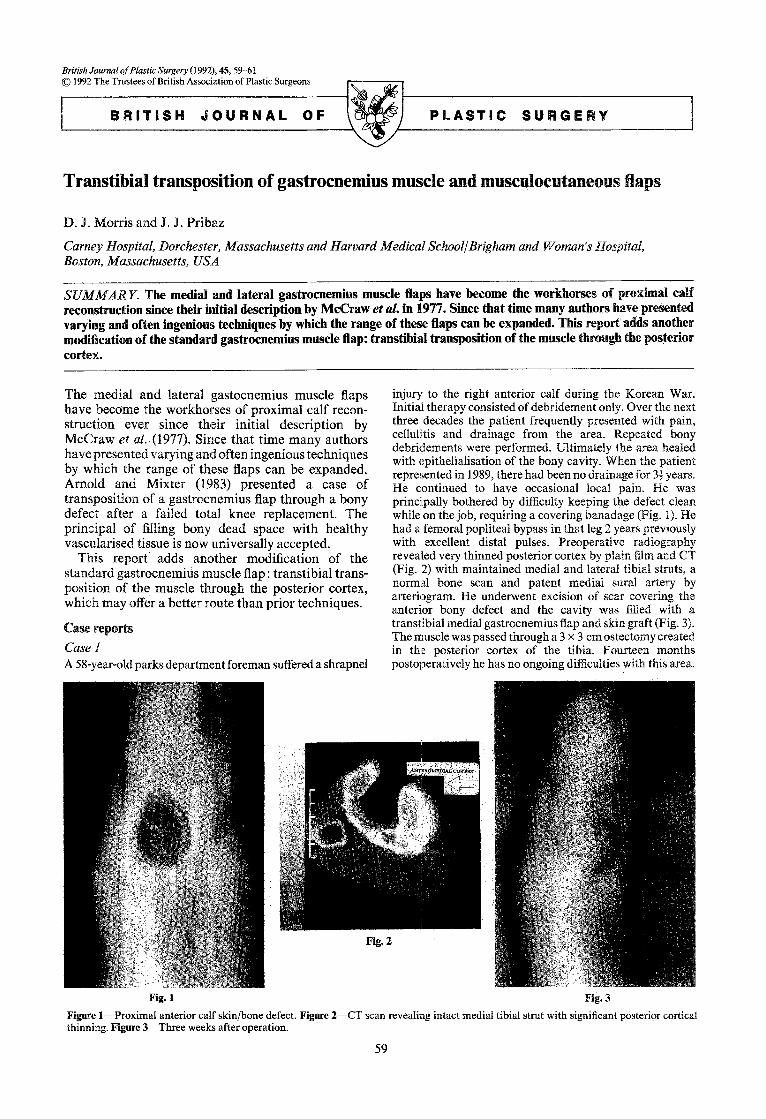
injury to the right anterior calf during the Korean War. Initial therapy consisted of debridement only. Over the next three decades the patient frequently presented with pain, cellulitis and drainage from the area. Repeated bony debridements were performed. Ultimately the area healed with epithelialisation of the bony cavity. When the patient represented in 1989, there had been no drainage for 3f years. He continued to have occasional local pain. He was principally bothered by difficulty keeping the defect clean while on the job, requiring a covering banadage (Fig. 1). He had a femoral popliteal bypass in that leg 2 years previously with excellent distal pulses. Preoperative radiography revealed very thinned posterior cortex by plain film and CT (Fig. 2) with maintained medial and late& tibia1 struts, a normal bone scan and patent medial sural artery by arteriogram. He underwent excision of scar covering the anterior bony defect and the cavity was filled with a transtibial medial gastrocnemius flap and skin graft (Fig. 3). The muscle was passed through a 3 x 3 cm ostectomy created in thle posterior cortex of the tibia. Fourteen months postoperatively he has no ongoing difficulties with this area.
Fig. 2
Fig. 3
Figure I-Proximal anterior calf skin/bone defect. Figure Z-CT scan revealing intact medial tibial strut with significant posterior cortical thinning. Figure S-Three weeks after operation.
59
60 British Journal of Plastic Surgery
Case 2
This 70-year-old man presented following a failed total knee replacement which ultimately required removal of the hardware and coverage with a conventional medial gastroc- nemius flap. Following wound healing he underwent knee fusion, with development of late chronic osteomyelitis. After operative debridement, he had a significant anterior bony and skin defect but continued fusion with healed bone posteriorly, laterally and medially.
thinning of the proximal muscle can decrease contour deformity.
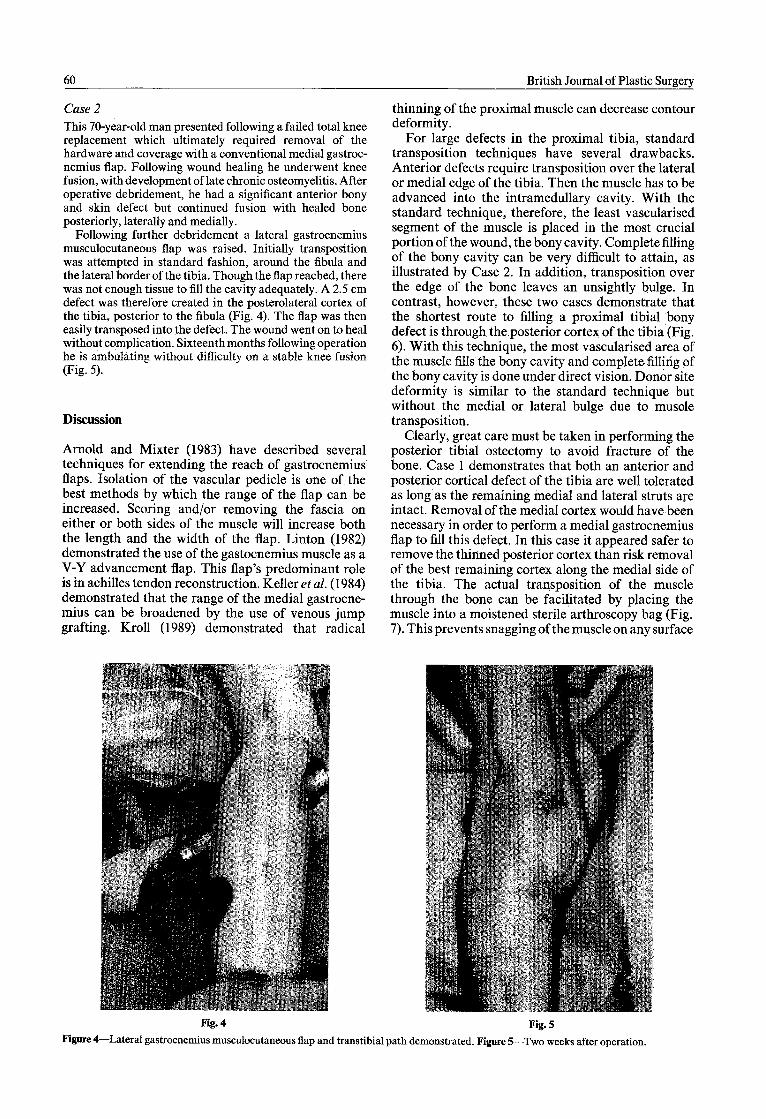
Following further debridement a lateral gastrocnemius musculocutaneous flap was raised. Initially transposition was attempted in standard fashion, around the fibula and the lateral border of the tibia. Though the flap reached, there was not enough tissue to fill the cavity adequately. A 2.5 cm defect was therefore created in the posterolateral cortex of the tibia, posterior to the fibula (Fig. 4). The flap was then easily transposed into the defect. The wound went on to heal without complication. Sixteenthmonths following operation he is ambulating without difficulty on a stable knee fusion (Fig. 5).
Discussion
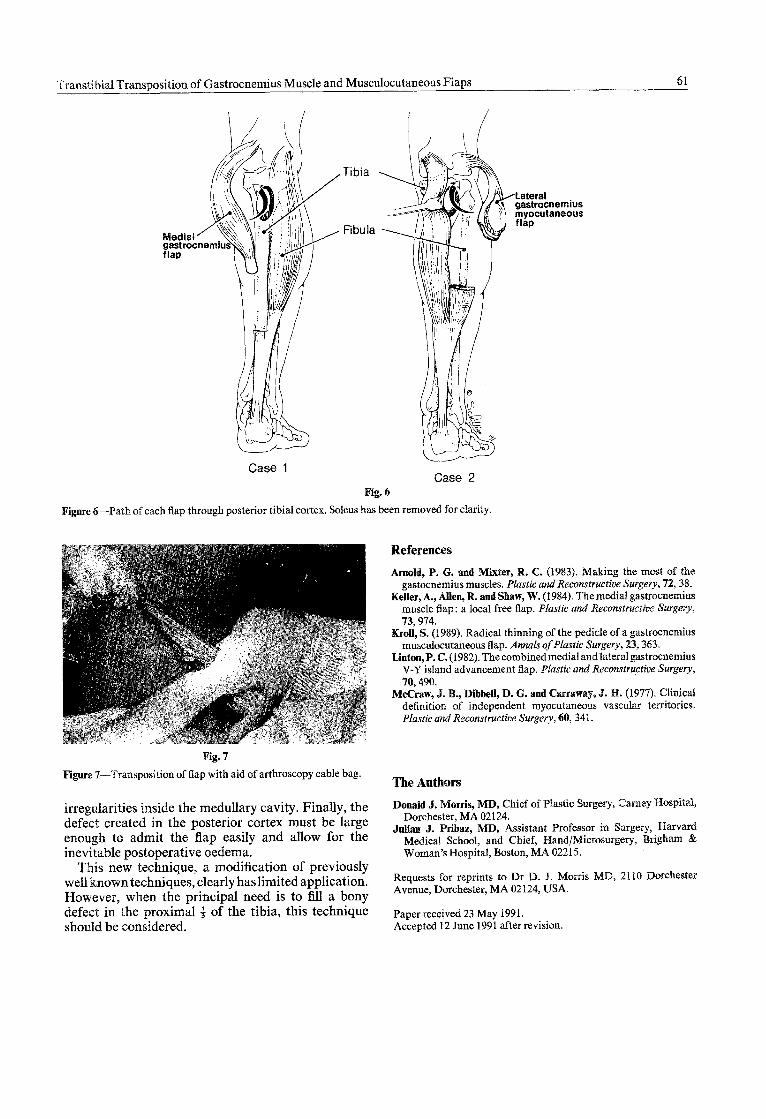
For large defects in the proximal tibia, standard transposition techniques have several drawbacks. Anterior defects require transposition over the lateral or medial edge of the tibia. Then the muscle has to be advanced into the intramedullary cavity. With the standard technique, therefore, the least vascularised segment of the muscle is placed in the most crucial portion of the wound, the bony cavity. Complete filling of the bony cavity can be very difficult to attain, as illustrated by Case 2. In addition, transposition over the edge of the bone leaves an unsightly bulge. In contrast, however, these two cases demonstrate that the shortest route to filling a proximal tibia1 bony defect is through the posterior cortex of the tibia (Fig. 6). With this technique, the most vascularised,area of the muscle fills the bony cavity and complete. filling of the bony cavity is done under direct vision. Donor site deformity is similar to the standard technique but without the medial or lateral bulge due to musole transposition.
Arnold and Mixter (1983) have described several techniques for extending the reach of gastrocnemius flaps. Isolation of the vascular pedicle is one of, the best methods by which the range of the flap can be increased. Scoring and/or removing the fascia on either or both sides of the muscle will increase both the length and the width of the flap. Linton (1982) demonstrated the use of the gastocnemius muscle as a V-Y advancement flap. This flap’s predominant role is in achilles tendon reconstruction. Keller et al. (1984) demonstrated that the range of the medial gastrocne- mius can be broadened by the use of venous jump grafting. Kroll (1989) demonstrated that radical
Clearly, great care must be taken in performing the posterior tibia1 ostectomy to avoid fracture of the bone. Case 1 demonstrates that both an anterior and posterior cortical defect of the tibia are well tolerated as long as the remaining medial and lateral struts are intact. Removal of the medial cortex would have been necessary in order to perform a medial gastrocnemius flap to fill this defect. In this case it appeared safer to remove the thinned posterior cortex than risk removal of the best remaining cortex along the medial side of the tibia. The actual transposition of the muscle through the bone can be facilitated by placing ‘the muscle into a moistened sterile arthroscopy bag (Fig. 7): This prevents snagging of the muscle on any surface
Fig. 4 Fig. 5
Figure &Lateral gastrocnemius musculocutaneous flap and transtibial path demonstrated. Figure ~--TWO weeks after operation.
Transtibial Transposition of Gastrocnemius Muscle and Musculocutaneous Flaps 61
Figure &-Path of ‘each flap through posterior tibia1 cortex. Soleus has been removed for clarity.
Case 1
Tibia
Fibuia
Case 2 Fig. 6
References
Am&%, P. 6. and Miter, R. C. (1983). Making the most of the gaslocnemius muscles. Plastic and Reconstructive Surgery, 72, 38.
Keller, A., Alien, R. and Shaw, W. (1984). The medial gastrocnemius muscle flap : a local free flap. Plastic and Reconstructive Surgery, 73,974.
KroTl, S. (1989). Radical thinning of the pedicle of a gastrocnemius musculocutaneous Rap. Annals of Plastic Surgery, 23,363.
kinton,P. C. (1982). The combinedmedialandlateralgastrocnemius V-Y island advancement flap, Plastic and Reconstructive Surgery, 70,490.
McGraw, 9. B., DihbeR, D. G. and Carraway, J. ET. (1977). Clinical definition of independent myocutaneous vascular territories. Plastic and Reconstmctive Surgery, 60, 341.
Pig. 7
Figure 7-Transposition of flap with aid of arthroscopy cable bag.
irregularities inside the medullary cavity. Finally, the defect created in the posterior cortex must be large enough to admit the flzp easily and allow for the inevitable postoperative oedema.
This new technique, a modification of previously well known techniques, clearly has limited application. However, when the principal need is to fill a bony defect in the proximal f of the tibia, this technique should be considered.
The Authsrt~
DonaId J. Morris, MD, Chief of Plastic Surgery, Camey Hospital, Dorchester, MA 02124.
Julian J. Pribaz, MD, Assistant Professor in Surgery, Harvard Medical School, and Chief, Hand/Microsurgery, Brigham L Woman’s Hospital, Boston, MA 02215.
Requests for reprints to Dr D. 3. Morris MD, 2110 Dorchester Avenue, Dorchester, MA 02124, USA.
Paper received 23 May 1991. Accepted 12 June 1991 after revision.
Recommended

















