
Brifi,sh Journal of’l’htic Surgery (1996), 49, 115-I 18 0 1996 The British Association of Plastic Surgeons
The injured foot: cutaneous coverage with a distally based posterior tibia1 cross leg flap
F. Giraldo, M. D. Garcia, J. de Grado, C. Gonzalez, and J. A. Rus Plastic und Reconstructive Surgery Unit, Regional Hospital “Carlos Huya”, Mdlagu, Spain
S UMMAR Y. Treatment of extensive soft tissue defects of the foot has long been a challenging problem for the reconstructive surgeon. We report a series of 5 injured feet with major soft tissue loss and significant bony injury, treated with distally based cross leg flaps based on the posterior tibia1 artery, with satisfactory cosmetic and functional results. The survival of the flap was complete in 4 of the 5 patients; in one case, the flap suffered about 2-3 cm distal partial necrosis. The mean hospital stay was 30 days, and walking without ambulatory support was possible about 60 days postoperatively. We consider this procedure a potential alternative to microvascular techniques for the treatment of severe foot injuries, in an area where microsurgery reconstruction is fraught with difficulties.
The particular characteristics of the soft tissues in the weight-bearing region of the foot can make coverage of severe foot injuries a very difficult and complex problem. The main parameters of successful foot reconstruction are the obtaining of bone stability, sensation and adequate soft tissue cover. The first step in reconstruction of the foot after injury is evaluation of the wound. Bearing in mind the foot injury classification of Hidalgo and Shaw,’ we report a series of 5 patients with foot injuries type II (an important injury with major soft tissue loss with or without distal amputation) and type III (crushing of the skeletal structures with open fracture of the ankle, calcaneum or distal extremity with injury to a major blood vessel without distal ischaemic compromise), treated with distally based posterior tibia1 artery cross leg fasciocutaneous island flaps, as previously described by Sharma and Kola.’ We consider the disadvantages of the procedure as well as the potential indications for its use.
Patients and methods
Since December 1992 to August 1994, we have chosen to reconstruct difficult injuries of the foot with distally based cross leg flaps based on the posterior tibia1 artery, with good results. Reconstruction of severe defects of the foot has been successfully performed in 5 young male patients, age 18 to 34 years (mean 26.6 years) (Table I).
Surgical technique
We have basically used the same technique as described by Hong et a1.3 in 1989, to raise flaps distally based on the posterior tibia1 artery. Following Sharma and Kola,2 we have used flaps taken from the opposite healthy leg as cross leg flaps. We assessed
115
the continuity of the deep plantar arterial arch of the foot with preoperative arteriograms in our first two patients. We noted the presence of distal palpable pulses of the posterior tibia1 and dorsalis pedis arteries in all 5 patients. We designed the flap in a racket fashion, the size of the racket ‘handle’ being 10 x 3 cm and the size of the ‘racket’ 12-15 x7-12 cm (Fig. 1A). The longitudinal axis of the flap is centred over the medial intermuscular septum of the lower leg. The dissection is carried out from distal to proximal, first identifying the posterior tibia1 neurova- scular pedicle, and dissecting free the posterior tibia1 nerve. Next, the fascia and skin are raised as a unit from the medial and lateral margins until the medial intermuscular septum is reached, preserving the septo- cutaneous and musculocutaneous perforators of the posterior tibia1 vessels. A vascular clamp is applied to the posterior tibia1 vessels proximal to the flap, and the tourniquet is released. If the circulation of the flap and leg is satisfactory, the vessels are divided proximally. The exposed posterior tibia1 nerve is covered by approximating adjacent muscles, and the flap donor site and the exposed part of the pedicle are covered with split thickness skin grafts (which protect the pedicle vessels). The limbs are placed in a suitable position and the ‘racket’ of the flap is inset into the defect (Figs lB, 2B). The mean operating time is 2.5 hours.
The limbs are immobilised for 21 days, after which the flap pedicle is divided under local anaesthesia. For defects on the heel and the dorsum of the foot, the flap reaches the recipient site with minimal flexion of the knees; in such cases, only the ankles are immobilised by a padded bandage and a plaster splint. Defects of the lateral and distal foot require significant flexion of the knees; in these cases, the ankles are also immobilised by a bandage and plaster splint, and the knee is immobilised with a soft bandage during the first postoperative week.
116 British Journal of Plastic Surgery
Table I Patient Summary
Age iyeursi. Hidalgo and Shawl foot Associated Outcome and long-term Case sex Site of d+ct injuries clussification fractures Size of flap complications
18, male Dorsum of right foot
34, male Dorsum of left foot
30, male Lateral region of right foot
4 29, male Distal region of right foot
5 22, male Posterior region of right heel
Type III
Type III
Type III
Type II (iatrogenic)
Metatarsals II and III
Metatarsals I to v
Calcaneum Metatarsals
IV and V none
Type II none
l5x8cm 100% survival
12xl2cm 2 cm distal necrosis
l5x9cm 100% survival Amputation
l5x7cm 100% survival Accidental ulceration
l5x7cm 100% survival
Fig. 1
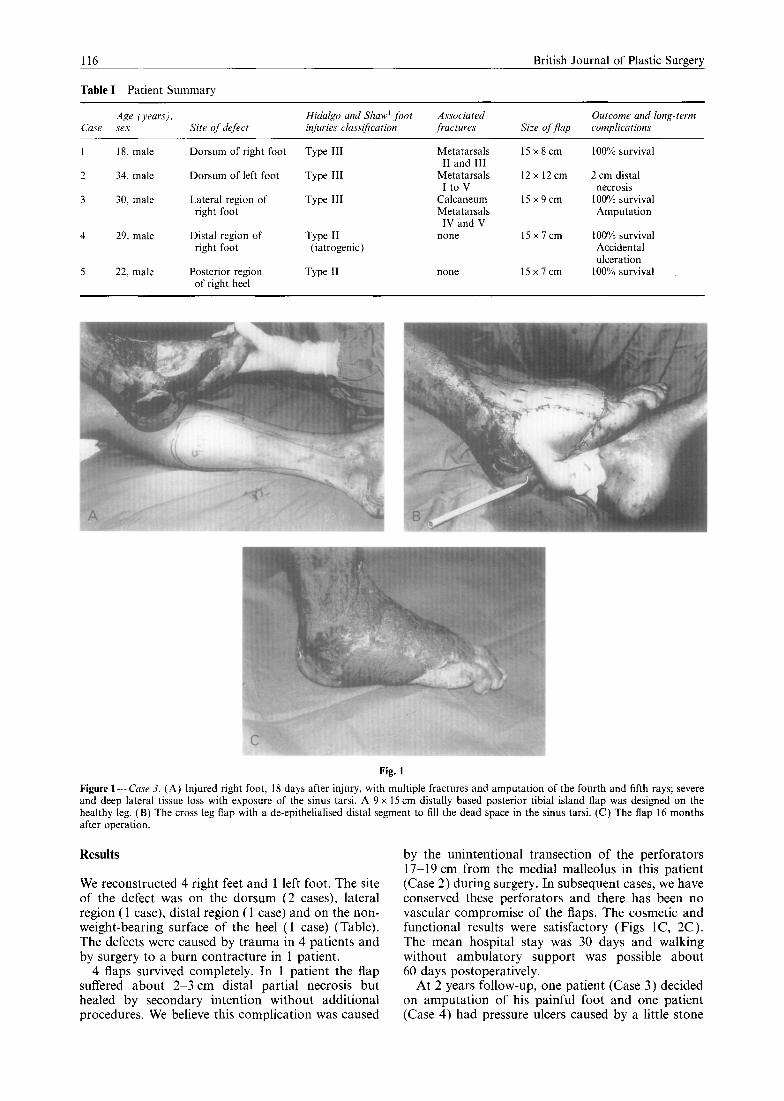
Figure l-Case 3. (A) Injured right foot, 18 days after injury, with multiple fractures and amputation of the fourth and fifth rays; severe and deep lateral tissue loss with exposure of the sinus tarsi. A 9 x 15 cm distally based posterior tibia1 island flap was designed on the healthy leg. (B) The cross leg flap with a de-epithelialised distal segment to fill the dead space in the sinus tarsi. (C) The flap 16 months after operation.
Results
We reconstructed 4 right feet and 1 left foot. The site of the defect was on the dorsum (2 cases), lateral region (1 case), distal region (1 case) and on the non- weight-bearing surface of the heel ( 1 case) (Table). The defects were caused by trauma in 4 patients and by surgery to a burn contracture in 1 patient.
4 flaps survived completely. In 1 patient the flap suffered about 2-3 cm distal partial necrosis but healed by secondary intention without additional procedures. We believe this complication was caused
by the unintentional transection of the perforators 17-19 cm from the medial malleolus in this patient (Case 2) during surgery. In subsequent cases, we have conserved these perforators and there has been no vascular compromise of the flaps. The cosmetic and functional results were satisfactory (Figs lC, 2C). The mean hospital stay was 30 days and walking without ambulatory support was possible about 60 days postoperatively.
At 2 years follow-up, one patient (Case 3) decided on amputation of his painful foot and one patient (Case 4) had pressure ulcers caused by a little stone
Posterior tibia1 cross leg flap
Fig. 2
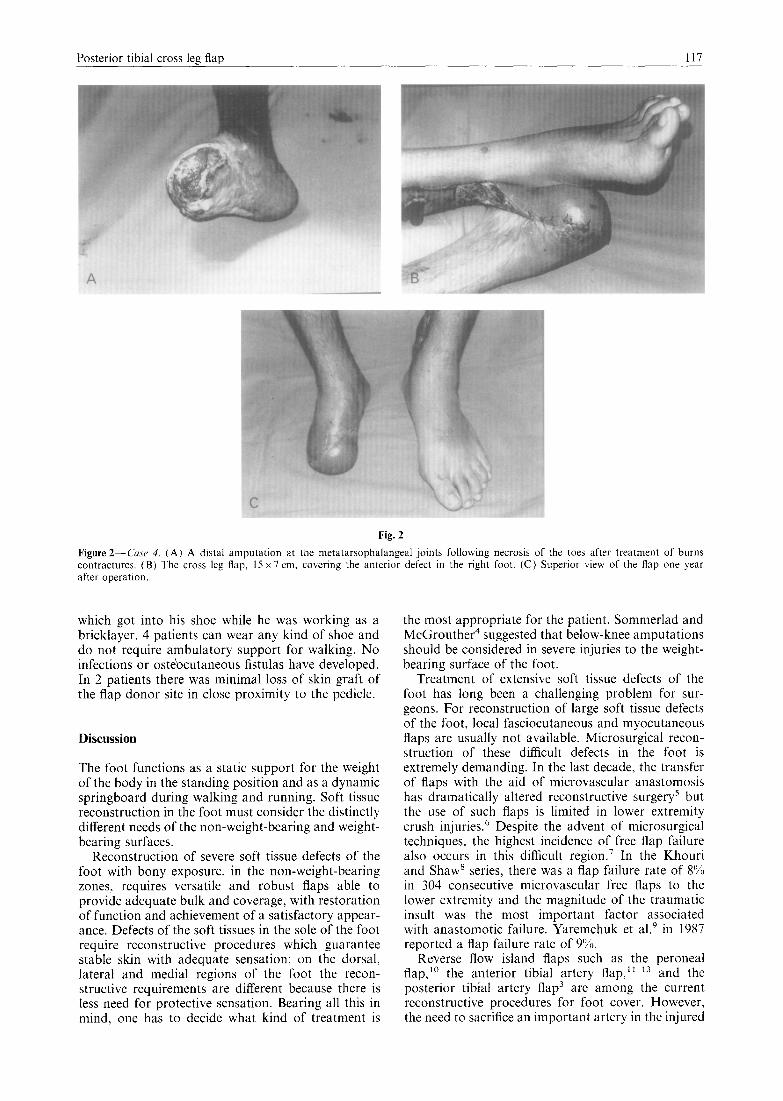
Figure2-Cusr 4. (A) A distal amputation at the metatarsophalangeal joints following necrosis of the toes after treatment of burns contractures. (B) The cross leg flap, I5 x 7 cm. covering the anterior defect in the right foot. (C) Superior view of the flap one year after operation
which got into his shoe while he was working as a bricklayer. 4 patients can wear any kind of shoe and do not require ambulatory support for walking. No infections or oste’ocutaneous fistulas have developed. In 2 patients there was minimal loss of skin graft of the flap donor site in close proximity to the pedicle.
Discussion
The foot functions as a static support for the weight of the body in the standing position and as a dynamic springboard during walking and running. Soft tissue reconstruction in the foot must consider the distinctly different needs of the non-weight-bearing and weight- bearing surfaces.
Reconstruction of severe soft tissue defects of the foot with bony exposure, in the non-weight-bearing zones, requires versatile and robust flaps able to provide adequate bulk and coverage, with restoration of function and achievement of a satisfactory appear- ance. Defects of the soft tissues in the sole of the foot require reconstructive procedures which guarantee stable skin with adequate sensation; on the dorsal, lateral and medial regions of the foot the recon- structive requirements are different because there is less need for protective sensation. Bearing all this in mind, one has to decide what kind of treatment is
the most appropriate for the patient. Sommerlad and McGrouther4 suggested that below-knee amputations should be considered in severe injuries to the weight- bearing surface of the foot.
Treatment of extensive soft tissue defects of the foot has long been a challenging problem for sur- geons. For reconstruction of large soft tissue defects of the foot, local fasciocutaneous and myocutaneous flaps are usually not available. Microsurgical recon- struction of these difficult defects in the foot is extremely demanding. In the last decade, the transfer of flaps with the aid of microvascular anastomosis has dramatically altered reconstructive surgery5 but the use of such flaps is limited in lower extremity crush injuries.6 Despite the advent of microsurgical techniques, the highest incidence of free flap failure also occurs in this difficult region.’ In the Khouri and Shaw’ series, there was a flap failure rate of 8% in 304 consecutive microvascular free flaps to the lower extremity and the magnitude of the traumatic insult was the most important factor associated with anastomotic failure. Yaremchuk et al.” in 1987 reported a flap failure rate of 9%.
Reverse flow island flaps such as the peroneal flap,” the anterior tibia1 artery flap,“-13 and the posterior tibia1 artery flap3 are among the current reconstructive procedures for foot cover. However, the need to sacrifice an important artery in the injured

118 British Journal of Plastic Surgery
lower leg is a potentially serious disadvantage. For this reason, we reconstructed severe soft tissue defects in the foot with cross leg distally based posterior tibia1 artery fasciocutaneous island flaps. This operat-
5ve procedure was described by Sharma and Kola’ for reconstructing defects of the middle and lower third of the leg but there are no reports of the use of this flap for foot defects. We have not used simple cross leg fasciocutaneous flapsr4,15 because of the forced and uncomfortable position of immobilisation. The long pedicle of the posterior tibia1 flap also permits versatile cutaneous coverage with a minor risk of complications of the pedicle and a comfortable knee joint position. The disadvantages of cross leg flaps are well known; they have major morbidity in terms of time in hospital and require two operations. Nevertheless, in using this particular form of cross leg flap we have achieved good results with a mini- mum of complications, similar to the series of 12 cases published by Barclay et a1.15 in 1983. The liberal use of these techniques for reconstruction of difficult problems in the lower leg has allowed surgeons to salvage feet which previously might have been amputated.
We believe the cross leg flap distally based on the posterior tibia1 artery is an optional method for reconstructive surgery of the foot when: (1) a major soft tissue defect is located in a non-weight-bearing surface; (2) there are associated vascular injuries in the injured limb; (3) the patient is young and so is better able to tolerate the cross leg position; and (4) in areas where microsurgery reconstruction is fraught with difficulties or when the use of a free flap has a significant risk because of the absence of good recipient vessels near the defect.
References
1. Hidalgo DA, Shaw WW. Reconstruction of foot injuries. Clin Plast Surg 1986; 13: 663-80.
2. Sharma RK, Kola G. Cross leg posterior tibia1 artery fascio- cutaneous island flap for reconstruction of lower leg defects. Br J Plast Surg 1992; 45: 62-5.
3. Hong G, Steffens K, Wang FB. Reconstruction of the lower
leg and foot with the reverse pedicled posterior tibia1 fasciocutaneous flap. Br J Plast Surg 1989; 42: 512-16.
4. Sommerlad BC, McGrouther DA. Resurfacing the sole: long- term follow-up and comparison of techniques. Br J Plast Surg 1978; 31: 107-16.
5. Thatte RL, Yelikar AD, Chajlani P, Thatte MR. Successful detachment of cross-leg fasciocutaneous flaps on the tenth day: a report of 10 cases. Br J Plast Surg 1986; 39: 491-7.
6. Uhm KI, Shin KS, Lew JD. Crane principle of the cross leg fasciocutaneous flap: aesthetically pleasing technique for damaged dorsum of the foot. Ann Plast Surg 1985; 15: 257-61.
7. Godina M. Early microsurgical reconstruction of complex trauma of the extremities. Plast Reconstr Surg 1986; 78: 285-92.
8. Khouri RK, Shaw WW. Reconstruction of the lower extremity with microvascular free flaps: a IO-year experience with 304 consecutive cases. J Trauma 1989; 29: 1086-94.
9. Yaremchuk MJ, Brumback RJ, Manson PN, Burgess AR, Poka A, Weiland AJ. Acute and definitive management of traumatic osteocutaneous defects of the lower extremity. Plast Reconstr Surg 1987; 80: l-14.
10. Yoshimura M, Imura S, Shimamura K, Yamauchi S, Nomura S. Peroneal flap for reconstruction in the extremity: preliminary report. Plast Reconstr Surg 1984; 74: 402-9.
11. Wee JTK. Reconstruction of the lower leg and foot with the reverse-pedicled anterior tibia1 flap: preliminary report of a new fasciocutaneous flap. Br J Plast Surg 1986; 39: 327737.
12. Morrison WA, Shen TY. Anterior tibia1 artery flap: anatomy and case report. Br J Plast Surg 1987; 40: 230-5.
13. Satoh K, Yoshikawa A, Hayashi M. Reverse-flow anterior tibia1 flap type III. Br J Plast Surg 1988; 41: 62447.
14. Barclay TL, Cardoso E, Sharpe DT, Crockett DJ. Repair of lower leg injuries with fascia-cutaneous flaps. Br J Plast Surg 1982; 35: 127-32.
15. Barclay TL, Sharpe DT, Chisholm EM. Cross-leg fascio- cutaneous flaps. Plast Reconstr Surg 1983; 72: 843-6.
The Authors
F. Giraldo MD, PhD, Plastic Surgeon M. D. Garcia MD, PhD, Resident in Plastic Surgery J. de Grado MD, Resident in Plastic Surgery C. Gonzalez MD, Plastic Surgeon J. A. Rus MD, Chief of the Plastic and Reconstructive Surgery Unit
Regional Hospital “Carlos Haya”, Malaga, Spain.
Correspondence to: Francisco Giraldo MD, Plastic and Reconstructive Surgery Unit, Regional Hospital “Carlos Haya”, 29010-Malaga, Spain.
Paper received 13 July 1995 Accepted 26 September 1995, after revision.
Recommended

















