591
American Journal of
EPIDEMIOLOGYCopyright © 2001 by the Johns Hopkins University
Bloomberg School of Public Health
Sponsored by the Society for Epidemiologic Research
Published by Oxford University Press
Volume 154
Number 7
October 1, 2001
Magnetic Fields, Light-at-Night, and Melatonin Davis et al.ORIGINAL CONTRIBUTIONS
Residential Magnetic Fields, Light-at-Night, and Nocturnal Urinary 6-Sulfatoxymelatonin Concentration in Women
Scott Davis,1,2 William T. Kaune,3 Dana K. Mirick,1 Chu Chen,1 and Richard G. Stevens4
Exposure to 60-Hz magnetic fields may increase breast cancer risk by suppressing the normal nocturnal risein melatonin. This 1994–1996 Washington State study investigated whether such exposure was associated withlower nocturnal urinary concentration of 6-sulfatoxymelatonin in 203 women aged 20–74 years with no historyof breast cancer. Each woman was interviewed and provided data on the following for a 72-hour period at twodifferent seasons of the year: 1) magnetic field and ambient light measured every 30 seconds in her bedroom,2) personal magnetic field measured at 30-second intervals, and 3) complete nighttime urine samples on threeconsecutive nights. Lower nocturnal urinary 6-sulfatoxymelatonin level was associated with more hours ofdaylight, older age, higher body mass index, current alcohol consumption, and current use of medicationsclassified as beta blockers, calcium channel blockers, or psychotropics. After adjustment for these factors, higherbedroom magnetic field level was associated with significantly lower urinary concentration of 6-sulfatoxymelatonin during the same night, primarily in women who used these medications and during times ofthe year with the fewest hours of darkness. These results suggest that exposure to nighttime residential 60-Hzmagnetic fields can depress the normal nocturnal rise in melatonin. Am J Epidemiol 2001;154:591–600.
breast neoplasms; carcinogens, environmental; circadian rhythm; electricity; electromagnetic fields; melatonin
Received for publication July 6, 2000, and accepted for publica-tion December 20, 2000.
Abbreviation: BMI, body mass index.1 Program in Epidemiology, Division of Public Health Sciences,
Fred Hutchinson Cancer Research Center, Seattle, WA.2 Department of Epidemiology, School of Public Health and
Community Medicine, University of Washington, Seattle, WA.3 EM Factors, Richland, WA.4 Department of Community Medicine, University of Connecticut
Health Center, Farmington, CT.Reprint requests to Dr. Scott Davis, Fred Hutchinson Cancer
Research Center, 1100 Fairview Avenue North MP-474, P.O. Box19024, Seattle, WA 98109-1024 (e-mail: [email protected]).
It has been suggested that exposure to 60-Hz magneticfields may increase the risk of breast cancer by suppressingthe normal nocturnal rise in melatonin production andrelease (1), thereby resulting in increased levels of circulat-ing estrogen. Several lines of inquiry have been pursued toinvestigate a possible link between pineal function, circulat-ing estrogen level, and breast cancer risk (summarized byStevens and Davis and by Brainard et al. (2, 3)). Other thanlimited evidence that blood melatonin levels are reduced inhuman volunteers exposed to magnetic fields (4), there have
been few studies of the effect of magnetic field exposure onpineal function in humans. Although some results fromexperimental and occupational studies suggest that nocturnalmelatonin levels can be reduced by exposure to magneticfields, the evidence thus far is inconsistent and incomplete(5–10). More importantly, it remains unknown whether suchexposures can alter the endogenous hormonal environmentin women in a manner that might be important in the etiol-ogy of breast cancer. Therefore, the present study wasundertaken in 1994–1996 to investigate, for the first knowntime in women, whether exposure to magnetic fields and/orlight-at-night is associated with lower nocturnal concentra-tion of the primary metabolite of melatonin found in theurine (6-sulfatoxymelatonin).
MATERIALS AND METHODS
Study participants
Participants were women aged 20–74 years selected froma group of 591 women in King and Snohomish counties inWashington State who participated as controls in a case-control study of breast cancer and exposure to electromag-
Downloaded from https://academic.oup.com/aje/article-abstract/154/7/591/107343by gueston 13 February 2018

592 Davis et al.
Am J Epidemiol Vol. 154, No. 7, 2001
netic fields (11). The women initially were identified by ran-dom digit dialing (12). A sample was selected to provideapproximately equal representation of the highest and low-est bedroom magnetic field exposures. Of the 31 womenstill living in homes classified as Very High CurrentConfiguration according to the scheme developed byWertheimer and Leeper (13) to approximate exposuresinside a residence on the basis of external wiring configura-tions, 26 (84 percent) agreed to participate. Each of theremaining 556 potentially eligible women was ordered bythe mean magnetic field level measured in her bedroom overa 48-hour continuous period during her participation in thecase-control study. Eighty-three (82 percent) of the 101 eli-gible women who had the highest measured exposures and94 (85 percent) of the 110 eligible women who had the low-est measured exposures agreed to participate. The institu-tional review board approved the protocol for contactingpotential participants and the manner in which informedconsent was obtained.
Data collection and laboratory methods
Data collection consisted of the elements described intable 1 for a 72-hour measurement period. The entire proto-col was repeated approximately 3 or 6 months later, basedon random assignment, to provide measurements in differ-ent seasons of the year. This study design made it possibleto investigate the effects of different lengths of daily dark-ness on any potential association between magnetic field
exposure and urinary 6-sulfatoxymelatonin level. The studytook place over approximately 14 months.
The volume of urine was determined, and each samplewas assayed for creatinine concentration based on a kineticmodification of the Jaffe reaction using the Roche Reagentfor Creatinine (Roche Diagnostic Systems, Nutley, NewJersey). Urinary concentrations of the primary metabolite ofmelatonin, 6-sulfatoxymelatonin, were determined by usingcommercially available radioimmunoassay kits (CIDtechResearch Inc., Mississauga, Ontario, Canada). The assaywas run in duplicate with 500 µl of diluted sample. Each runincluded the kit control provided by the manufacturer and anin-house control using a urine sample provided by a volunteer at the beginning of the study was used. Assay sen-sitivity was 0.5 ng/ml urine, and intra- and interassay per-cent coefficients of variation were approximately 9 and 13percent, respectively.
Statistical methods
Nine exposure variables were defined prior to analysis tocharacterize a participant’s exposure to magnetic fields. Thefollowing three reflected exposure to magnetic fields in thebedroom at night: 1) mean nighttime bedroom magneticfield exposure, 2) proportion of nighttime bedroom mag-netic field measurements ≥0.2 µT, and 3) short-term vari-ability in the bedroom magnetic field. Nighttime wasdefined for each subject and each night as the time periodbetween the last void before going to bed and the first void
TABLE 1. Data elements studied to determine a possible association between exposure to magneticfields and/or light-at-night and urinary 6-sulfatoxymelatonin concentration, Washington State, 1994–1996
In-person interview
Personal magnetic field exposure*
Bedroom magnetic field exposure*
Ambient light*
Urine sample§
Protocol adherence form
Patterns of electric blanket useCurrent medication useUpdate of personal habits since case-control study
EMDEX Lite meter†Broadband (40–800 Hz) x, y, and z orthogonal components of
fieldMeasurements at 30-second intervals on a 24-hour basisDiary of activities in 30-minute time segments
EMDEX II meter†Broadband (40–800 Hz) and harmonics (100–800 Hz)Measurements at 30-second intervals during the nightMeter placed on floor near head of bed where magnetic field
is within ±0.05 µT of field on pillow
Commercial light sensor‡Measured at 30-second intervals at head of bed during the night
Complete nighttime urine sample on 3 consecutive nights
Documented subject’s night and any problems with urinecollection
Element Description
* All meters were calibrated prior to the start of the study and periodically on a regular basis thereafter.† Enertech Consultants, Campbell, California.‡ Graseby Electronics, Orlando, Florida.§ Participants were instructed to void their bladder just prior to retiring; any urine excreted after that time,
including the first morning void just after rising, was collected.
Downloaded from https://academic.oup.com/aje/article-abstract/154/7/591/107343by gueston 13 February 2018

Magnetic Fields, Light-at-Night, and Melatonin 593
Am J Epidemiol Vol. 154, No. 7, 2001
the next morning. Mutually exclusive 10-minute timeblocks were used to group exposure measurements. A statis-tic (Y) was computed to characterize short-term variabilityin the bedroom magnetic field, as follows:
where Bk, k = 1, 2, … , 20 are the 20 values of the measuredmagnetic field recorded at 30-second intervals during a 10-
minute time period. This statistic, when divided by (i.e., the number of measurement intervals – 1), is equal tothe “rate-of-change metric” introduced by Yost (14). Thebedroom variability statistic was defined as the average ofall 10-minute Y statistics during the nighttime period.
Three variables reflected personal exposure to magneticfields on a continual (24-hour) basis: 1) mean 24-hour per-sonal magnetic field exposure, 2) proportion of 24-hour per-sonal magnetic field measurements ≥0.2 µT, and 3) short-term variability in the personal magnetic field (defined asabove). In addition, one variable was constructed to reflectthe wire code configuration assigned to each participant’sresidence according to the scheme developed by Wertheimerand Leeper (13). Two variables were defined to characterizeexposure to light-at-night: 1) proportion of nighttime bed-room light measurements ≥10 lux and 2) number of timesthe subject reported getting up and turning on a light.
Additional factors known or suspected to affect mela-tonin levels were specified a priori for use in covariateadjustment. Primary covariates were defined as those wellestablished from previous research to affect melatonin lev-els and included participant age, menopausal status, andduration of darkness. Participants were classified as pre-menopausal if they reported regular or irregular periods,did not use hormone replacement therapy, and had notundergone a hysterectomy with oophorectomy; otherwise,they were classified as postmenopausal. Fifteen partici-pants were considered “indeterminate” according to thisdefinition and were classified as premenopausal if aged<50 years and as postmenopausal otherwise. Numbers ofhours of darkness each night that urine was collected wereobtained from the US Naval Observatory for the Seattle,Washington, metropolitan area. Secondary covariates weredefined as factors suspected to affect melatonin levels andincluded the following: 1) alcohol consumption within theprevious 24 hours; 2) current or recent (within the last 30days) use of an electric blanket; 3) smoking within the last7 days; 4) body mass index (BMI; weight (kg)/height(m)2), categorized according to the Surgeon General’sReport on Nutrition and Health (15); 5) height; and 6)nightly use of any medications categorized as a betablocker, calcium channel blocker, or psychotropic. Toascertain medication use, participants listed any medica-tions used during each night of urine collection. A phar-macologist subsequently grouped the reported medicationsinto these three categories, which were selected on thebasis of evidence that drugs of these types can affect mela-tonin levels (16–18).
219
Y � B a19
k�11Bk�1 � Bk2
2
Since urine samples and exposure data were collected foreach participant on 3 consecutive days during two differentsessions, each subject contributed up to 6 days of exposureand melatonin data. Individual observations were highlycorrelated; thus, a repeated-measures analysis was required.The presence of exposure variables and covariates thatchanged with each measurement day and/or session requiredthat these variables be considered time dependent in therepeated-measures setting. All analyses used the SASMIXED procedure to fit linear regression models with cor-related error structure to account for the correlation of therepeated measurements on each subject (19–23). The errorstructure had restricted maximum likelihood estimation of a6 × 6 covariance matrix with three unknown parameters:day-to-day variation, session-to-session variation, and resid-ual error. For all regression analyses, the response variablewas the natural log transformation of 6-sulfatoxymelatoninconcentration normalized to creatinine (nanograms of mela-tonin divided by milligrams of creatinine). Mean nighttimebedroom magnetic field, short-term variability in the bed-room magnetic field, mean 24-hour magnetic field, andshort-term variability in the 24-hour magnetic field weretransformed by using the natural log transformation. Theproportions of nighttime bedroom and 24-hour personalmagnetic field measurements ≥0.2 µT, and the proportion ofnighttime bedroom light measurements ≥10 lux, were trans-formed by using a modified definition of the logit transfor-mation (24). If there was an indication of an exposure effecton 6-sulfatoxymelatonin concentration, an interaction termbetween the exposure measure of interest and the number ofhours of darkness was added to the model to investigateexposure effect modification by different lengths of dailydarkness.
RESULTS
Descriptive characteristics
Of the 203 participants enrolled in the first measurementsession, 200 provided complete (72-hour) bedroom metermeasurements, 201 provided complete personal meter mea-surements, 168 provided three complete urine samples, and200 provided at least one urine sample. Three subjectsbecame ineligible for the second measurement sessionbecause they changed residences between sessions. Of theremaining 200 women, 198 provided complete bedroommeasurements, 200 provided complete personal measure-ments, 171 provided three complete urine samples, and 195provided at least one urine sample. Most data losses wereaccounted for by partial urine collection. Samples from par-ticipants who reported spillage of urine that the laboratorytechnician estimated to represent >2 percent of the total vol-ume were deemed unusable (n = 37 samples, 21 in session 1and 16 in session 2). There were eight samples from fivesubjects whose concentrations of 6-sulfatoxymelatonin werebelow the detectable limits of the assay (0.5 ng mela-tonin/ml urine). These samples were assigned one half thevalue of the detectable limit of the assay before being nor-malized to creatinine level. Samples from both measure-ment sessions for one participant and one measurement ses-
Downloaded from https://academic.oup.com/aje/article-abstract/154/7/591/107343by gueston 13 February 2018

594 Davis et al.
Am J Epidemiol Vol. 154, No. 7, 2001
sion for two participants were excluded from the analysisbecause they reported using melatonin supplements at leastonce during the measurement period, which resulted in 6-sulfatoxymelatonin levels that were elevated more than 100times over the unsupplemented values.
Table 2 shows the distributions of two of the three pri-mary covariates and the secondary covariates. The distribu-tion of number of hours of daily darkness was slightly U-shaped (data not shown), reflecting a slightly greaternumber of total sample days occurring at the extremes of therange of daily darkness (8.0 hours at the summer solsticeand 15.6 hours at the winter solstice).
Urinary 6-sulfatoxymelatonin concentration
A total of 1,106 nocturnal urine samples were available foranalysis. The distribution of urinary 6-sulfatoxymelatoninconcentration was right skewed, meaning that the majority ofthe measurements were at the low end of the scale (mean,19.3 ng/mg creatinine; standard deviation, 12.8). The concen-
tration varied somewhat according to the season of the year;each season was defined as the 3 months centered on therespective equinox or solstice. Concentrations were highest inwinter (mean, 22.5 ng/mg creatinine) and lowest in summer(mean,16.8 ng/mg creatinine). Spring and fall values wereintermediate (means, 20.1 and 18.1, respectively). Urinary 6-sulfatoxymelatonin concentrations were highly and signifi-cantly correlated from day to day within each measurementsession (Spearman’s rank correlation coefficients: 0.90 and0.85, respectively for the two sessions; p < 0.0001 for both)as well as between measurement sessions (Spearman’s rankcorrelation coefficient: 0.75; p < 0.0001).
Measures of exposure to magnetic fields and light-at-night
Table 3 summarizes the measures of exposure to mag-netic fields and light-at-night. Mean nighttime bedroommagnetic field levels were low; half of the subjects hadmean levels of <0.04 µT. Mean 24-hour personal magneticfield levels were higher. The distributions for both measureswere highly right skewed. The distribution of the proportionof nighttime bedroom measurements ≥0.2 µT was alsohighly right skewed, with more than 70 percent of the nightshaving no time ≥0.2 µT. However, only two measurementdays had 24-hour personal magnetic field levels with notime ≥0.2 µT. For both nighttime bedroom and 24-hour per-sonal measurements, mean magnetic field levels and proportions of levels ≥0.2 µT were highly and significantlycorrelated from day to day within each measurement session.
The distributions of the variables reflecting short-termvariability in bedroom and 24-hour personal magnetic fieldlevels were similar for all four seasons. Values were signif-icantly correlated day to day within each measurement ses-sion; bedroom measures were more highly correlated than24-hour measures. Wire code classification of the homes ofthe 203 subjects was distributed as follows (data notshown): 57 lived in homes classified as Very Low CurrentConfiguration, 72 in UnderGround, 20 in Ordinary LowCurrent Configuration, 28 in Ordinary High CurrentConfiguration, and 26 in Very High Current Configuration.For each of the four seasons, the lowest two categoriesaccounted for the greatest proportion of subjects.
The distributions of both the proportion of nighttime bed-room light measurements ≥10 lux and the number of timesthe subject reported getting up and turning on a light werehighly right skewed. The distributions of both measureswere similar for all four seasons and were significantly cor-related day to day within measurement session, althoughonly moderately so.
Effects of exposure to magnetic fields and light-at-night
Table 4 summarizes the parameter estimates and the esti-mated difference in nocturnal urinary 6-sulfatoxymelatoninlevel per unit change in each of the primary and secondarycovariates. The estimated effects of each covariate wereconsistent across all models, regardless of the exposure term
TABLE 2. Distribution of participants in a study of exposureto magnetic fields and light-at-night, according to primaryand secondary covariates, Washington State, 1994–1996
Age group (years)<4040–4445–4950–5455–5960–6465–6970–7475–79
Menopausal statusPremenopausalPostmenopausal
Alcohol consumption (same night)
Electric blanket useSame nightWithin 1 month of the study
Current smoker
Body mass index†15.0–23.023.1–27.227.3–32.132.2–49.9
Medication useBeta blockersCalcium channel blockersPsychotropicsOther
15283122232432271
59144
96*
32*42
29
71594330
15*16*34*17*
Covariate No.
714151111121613
1
2971
47
1621
14
35292115
78
178
%
* At least once during the six nights of data collection.† Weight (kg)/height (m)2; categorized according to the Surgeon
General’s Report on Nutrition and Health. Washington, DC: USDepartment of Health and Human Services, Public Health Service,1988. (Publication 88-50210).
Downloaded from https://academic.oup.com/aje/article-abstract/154/7/591/107343by gueston 13 February 2018

Magnetic Fields, Light-at-Night, and Melatonin 595
Am J Epidemiol Vol. 154, No. 7, 2001
in the model (listed in table 5). Participant age was signifi-cantly inversely associated with urinary 6-sulfatoxymela-tonin concentration: each additional year in age was associ-ated with approximately a 1 percent lower nocturnal urinary6-sulfatoxymelatonin level. Adding a quadratic term for agedid not materially alter the relation. Number of hours ofdarkness was directly associated with nocturnal 6-sulfa-toxymelatonin level: each additional hour of darkness wasassociated with a 2 percent higher 6-sulfatoxymelatoninconcentration. In none of the models was menopausal statusassociated with 6-sulfatoxymelatonin.
Relative to the lowest BMI category, each higher categorywas associated with approximately an 8 percent lower noc-turnal 6-sulfatoxymelatonin concentration. Reported use ofbeta blockers, calcium channel blockers, or psychotropicmedications was associated with approximately a 28 percentlower nocturnal urinary 6-sulfatoxymelatonin concentra-tion. Consumption of alcohol in the 24 hours precedingmorning urine collection was consistently related to a lower6-sulfatoxymelatonin concentration, but at suggestive levelsof significance (this relation is explored further in reference(25)). The following factors were not significantly associatedwith 6-sulfatoxymelatonin levels in any of the analyses andthus were excluded from subsequent models: current orrecent use of an electric blanket, measured magnetic fieldfrom an electric blanket if used, smoking, and height.
After adjustment for the primary covariates, higher meannighttime bedroom magnetic field level was associated withlower 6-sulfatoxymelatonin level in the urine at night (table5). Inclusion of an interaction term between number ofhours of darkness and mean nighttime magnetic fieldrevealed that the overall effect changed with differentlengths of daily darkness (i.e., at different times of the year).Higher mean nighttime magnetic field was significantlyassociated with lower 6-sulfatoxymelatonin concentrationuntil the length of darkness exceeded about 12 hours, thevernal and autumnal equinoxes (table 6).
Further adjusting this model for BMI category or alcoholconsumption did not materially change the relation betweenmean nighttime magnetic field level and nocturnal 6-sulfa-toxymelatonin concentration. However, adjustment formedication use did alter this relation. Mean nighttime mag-netic field remained inversely related to 6-sulfatoxymela-tonin concentration, but, overall, this effect was no longersignificant. Inclusion of an interaction term between meannighttime magnetic field and medication use showed thatthe effect of exposure differed between those who did anddid not use medications that might affect melatonin. Amongsubjects who reported taking medications that can affectmelatonin level, there was a significant exposure effect thatchanged in a continuous manner with number of hours ofdarkness. A statistically significant inverse association was
TABLE 3. Descriptive summary of measures of exposure to magnetic fields and light-at-night, Washington State, 1994–1996
Nighttime bedroom magnetic field (µT)
Proportion bedroom measurements ≥0.2 µT
Variability statistic of bedroom magneticfield (µT)
24-hour personal magnetic field (µT)
Proportion personal measurements ≥0.2 µT
Variability statistic of personal magneticfield (µT)
Ambient nighttime light (lux)
Proportion nighttime light measurements≥10 lux
No. of times light turned on at night
1,171(nights)
1,171(nights)‡
1,171(nights)
1,188(days)
1,188(days)§
1,188(days)
1,171(nights)
1,171(nights)¶
1,195(nights)#
Exposure measure No.*
0.039
0.0
0.016
0.083
0.064
0.17
2.1
0.019
0
Allseasons
0.0–1.6
0.0–1.0
0.0–1.1
0.0–2.1
0.0–1.0
0.0–1.4
0.7–786
0.0–1.0
0–6
0.039
0.0
0.018
0.089
0.079
0.18
2.9
0.03
0
0.031
0.0
0.013
0.072
0.044
0.15
3.5
0.04
0
0.039
0.0
0.016
0.082
0.065
0.16
1.6
0.01
0
0.049
0.0
0.019
0.099
0.083
0.20
1.7
0.01
0
0.99
0.95
0.93
0.88
0.77
0.55
0.53
0.56
0.62
0.98
0.95
0.90
0.85
0.77
0.58
0.67
0.58
0.54
Median exposurelevels by season
Median Range Spring Summer Fall Winter
Day-to-daycorrelation†
Session 1 Session 2
* No. of observations: bedroom magnetic field and light-at-night (nights); personal measurements (days).† Spearman’s rank correlation coefficient of day-1-to-day-2 exposure measures within each session; p ≤ 0.0001 for all exposure
measures.‡ 844 nights with no measurement ≥0.2 µT.§ 2 days with no measurement ≥0.2 µT.¶ 395 nights with no measurement ≥10 lux.# 742 nights with no episode of turning on a light.
Downloaded from https://academic.oup.com/aje/article-abstract/154/7/591/107343by gueston 13 February 2018

596 Davis et al.
Am J Epidemiol Vol. 154, No. 7, 2001
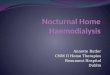
observed between mean nighttime magnetic field and 6-sulfatoxymelatonin concentration until length of darknessexceeded about 12 hours (table 6). Among those who did notreport taking such medications, there was an indication of aninverse association between nighttime magnetic field and 6-sulfatoxymelatonin concentration, but this association wasnonsignificant regardless of the number of hours of dark-ness. This relation is displayed graphically in figure 1 forboth users and nonusers of these medications.
To summarize these results in a more practical format, thedose-response slopes shown in table 6 were used to estimate
TABLE 4. Parameter estimates and estimated difference innocturnal urinary 6-sulfatoxymelatonin concentration forprimary and secondary covariates, evaluated as a group,Washington State, 1994–1996
Age (years)‡
Darkness (no. of hours)‡
Postmenopausal status
Any medication use
Body mass index§
Any alcohol consumption
Current electric blanket use
Recent electric blanket use
Measured magnetic field ofelectric blanket (if used)‡
Smoker
Subject-reported height (inches)‡
–0.01*
0.02*
0.22
–0.33*
–0.08**
–0.05
–0.06
0.06
0.00
–0.19
–0.02
FactorParameterestimate
(β)
–1
2
24
–28
–8
–5
–6
6
0
–17
–2
Estimated differencein melatonin†
–2, 0
1, 4
–12, 75
–38, –17
–15, 0
–11, 1
–24, 15
–11, 28
0, 1
–36, 7
–6, 2
%95%
confidenceinterval
* p ≤ 0.001, using two-sided t test of significance; ** p ≤ 0.05,using two-sided t test of significance.
† Per unit change if factor treated as a continuous variable, yesvs. no if categorical.
‡ Continuous variable.§ Body mass index category (values 1–4) analyzed as a
continuous variable.
TABLE 5. Parameter estimates from regression analysesbetween log 6-sulfatoxymelatonin and nine indicators ofexposure to residential magnetic fields and light-at-night,Washington State, 1994–1996
Bedroom magnetic field (0.1 µT)†
Proportion bedroommeasurements ≥0.2 µT‡
Bedroom magnetic field variability (0.1 µT)†
24-hour magnetic field (0.1 µT)†
Proportion 24-hour measurements≥0.2 µT‡
24-hour variability (0.1 µT)†
Wire code configuration
Proportion of night light ≥10 lux‡
No. of times light turned on
Exposurevariable
Dose-response
slope*(β)
–0.05
–0.01
0.00
–0.01
0.00
0.00
0.00
0.00
0.00
Two-sided95%
confidenceinterval
–0.09, 0.00
–0.02, 0.00
–0.04, 0.05
–0.06, 0.04
–0.02, 0.02
–0.04, 0.05
–0.07, 0.07
–0.02, 0.00
–0.03, 0.04
* Adjusted for the effects of age and no. of hours of darkness.† Variable analyzed by using the natural log transformation.‡ Variable analyzed by using a modified definition of the logit
transformation.
TABLE 6. Parameter estimates from regression analysesbetween log 6-sulfatoxymelatonin and nighttime bedroommagnetic field level, Washington State, 1994–1996
Mean bedroom magnetic field(0.1 µT)*
All participants† (n = 1,089)‡Vernal/autumnal equinox§Summer solsticeWinter solstice
By medication use¶Users (n = 245)‡
Vernal/autumnal equinoxSummer solsticeWinter solstice
Nonusers (n = 844)‡Vernal/autumnal equinoxSummer solsticeWinter solstice
Proportion bedroommeasurements (≥0.2 µT)#
All participants† (n = 1,089)Vernal/autumnal equinoxSummer solsticeWinter solstice
By medication use¶Users (n = 245)
Vernal/autumnal equinoxSummer solsticeWinter solstice
Nonusers (n = 844)Vernal/autumnal equinoxSummer solsticeWinter solstice
–0.05–0.07–0.02
–0.09–0.11–0.06
–0.02–0.05
0.00
–0.01–0.03
0.00
–0.02–0.04
0.00
–0.01–0.02
0.01
–0.10, 0.00–0.14, –0.01–0.08, 0.04
–0.18, 0.00–0.21, –0.01–0.16, 0.03
–0.08, 0.02–0.12, 0.01–0.06, 0.06
–0.03, 0.00–0.06, –0.01–0.01, 0.02
–0.04, 0.00–0.07, –0.01–0.03, 0.02
–0.02, 0.01–0.05, 0.00–0.01, 0.03
* Variable analyzed using the natural log transformation.† Adjusted for the effects of age and no. of hours of darkness.‡ No. of nights includes up to six per individual study
participant.§ Specific days (equinoxes and solstices) chosen to illustrate the
relation between magnetic field and 6-sulfatoxymelatonin, whichchanges in a continuous manner with no. of hours of darkness (referto the text).
¶ Adjusted for the effects of age, no. of hours of darkness, bodymass index, alcohol consumption, and medication use.
# Variable analyzed using a modified definition of the logittransformation.
Exposurevariable
Dose-response
slope(β)
Two-sided95%
confidenceinterval
Downloaded from https://academic.oup.com/aje/article-abstract/154/7/591/107343by gueston 13 February 2018

Magnetic Fields, Light-at-Night, and Melatonin 597
Am J Epidemiol Vol. 154, No. 7, 2001
FIGURE 1. Estimated effect (and 95% confidence interval), using the dose-response slopes presented in table 6, of log mean nighttime bed-room magnetic field on log urinary 6-sulfatoxymelatonin concentration for female nonusers (top panel) and users (bottom panel) of medicationsthat can affect melatonin levels, Washington State, 1994–1996. Test of no overall difference between the two regression lines, p = 0.1, using thechi-square reduced model likelihood ratio test.
the percentage decrease in urinary 6-sulfatoxymelatoninconcentration associated with higher levels of mean night-time bedroom magnetic field for both users and nonusers ofmedications that can affect melatonin levels. Table 7 dis-plays these results for four specific days of the year corre-sponding to the midpoints of the four seasons. A referencelevel of 0.04 µT was chosen since it was the median valueof magnetic field exposure for all 1,171 nights. The resultsshowed, for example, that among women taking medica-tions that can affect melatonin level, a twofold higher meannighttime bedroom magnetic field level was associated withan 8 percent lower urinary 6-sulfatoxymelatonin concentra-tion at the summer solstice.
The analysis was repeated by using both untransformedand square-root-transformed mean nighttime magnetic field
in the regression model, and the results essentially wereunchanged. Additionally, results were not materially differ-ent when the model was restricted to the medication usersrather than all participants.
Similar results were found after adjustment for the pri-mary covariates when exposure was characterized by theproportion of bedroom magnetic field measurements ≥0.2µT (table 5). After further adjustment for the secondarycovariates, for those subjects who reported taking medica-tions that can affect melatonin level, there was a statisticallysignificant inverse association between the proportion ofnighttime magnetic field measurements ≥0.2 µT and 6-sulfatoxymelatonin concentration until the length of dark-ness exceeded about 12 hours (table 6). The association wasstrongest with the lowest number of hours of darkness. For
Downloaded from https://academic.oup.com/aje/article-abstract/154/7/591/107343by gueston 13 February 2018

598 Davis et al.
Am J Epidemiol Vol. 154, No. 7, 2001
subjects who did not report taking such medications, therewas an indication of an inverse association, but this relationwas nonsignificant regardless of the number of hours ofdarkness. The results were essentially unchanged when themodel was restricted to medication users.
Although the logit transformation was used to helpaccount for the fact that the proportion of nighttime mag-netic field levels ≥0.2 µT was highly right skewed, anattempt also was made to evaluate how sensitive the resultswere to this aspect of the data by creating an indicator vari-able (yes if the measurement for any nighttime interval was≥0.2 µT, no if otherwise). When this variable was used, theresults were essentially unchanged.
After adjustment for the primary covariates, there was noevidence of significant differences in 6-sulfatoxymelatoninconcentration associated with any of the following (table 5):1) variability in nighttime bedroom magnetic field, 2) mean24-hour magnetic field based on the personal measure-ments, 3) proportion of personal magnetic field measure-ments ≥0.2 µT, 4) variability in personal magnetic fieldmeasurements, 5) wire code configuration, 6) proportion ofnighttime light levels ≥10 lux, and 7) reported number oftimes a participant got up and turned on the light. Resultswere unchanged when the regression models for these expo-sure variables were extended to adjust for the effects of thesecondary covariates (results not shown).
DISCUSSION
This study suggests that exposure to a higher magneticfield strength, as measured in a woman’s bedroom duringthe night, is associated with a lower concentration of 6-sulfatoxymelatonin in the woman’s urine during the samenight. It is noteworthy that a number of findings were con-sistently observed regarding factors previously reported toaffect melatonin levels. A strong association was found withthe number of hours of darkness. Season of the year isknown to affect the nocturnal rise in melatonin (16), duepresumably to seasonal shifts in the time of the nocturnalpeak in melatonin (26). Increasing age was significantlyassociated with lower melatonin levels, a finding consistentwith some previous studies (27, 28) but not all (29).Consumption of alcohol was associated with lower mela-tonin levels, consistent with findings in rats (30, 31) andhumans (32, 33). Finally, a substantially lower 6-sulfa-toxymelatonin concentration was observed in those whoreported taking classes of medications (beta blockers, cal-cium channel blockers, psychotropics) known to affectmelatonin levels (16–18). These results demonstrate internalconsistency and suggest that the present study was capableof detecting changes in urinary melatonin levels that mightbe expected.
Several findings from this study suggest that there maybe variability in individual susceptibility to the effects ofmagnetic field exposure. That is, those persons with lowerbaseline melatonin levels, for whatever reason, may bemore susceptible to the additional effects of magneticfields in lowering their melatonin concentration. The lower6-sulfatoxymelatonin concentration associated with mag-netic field exposure was most pronounced in those whoused medications known to reduce melatonin levels.Furthermore, the strongest magnetic field effects wereobserved during the summer months when melatonin lev-els were lowest, regardless of participants’ medication use.Since melatonin levels were lower at increasing ages, anexploratory analysis was conducted in which age wasinvestigated as a potential modifier of the magnetic fieldeffect on 6-sulfatoxymelatonin concentration. The magni-tude of the magnetic field effect increased somewhat witholder age, but not significantly so. Consistent with thesefindings are two studies that reported considerable individ-ual variability in sensitivity to the effects of light-at-nighton melatonin levels in humans (34, 35) and results from anexperiment conducted by Graham et al. whereby reduc-tions in melatonin associated with exposure to 20.0-µTmagnetic fields were observed only in those with low base-line melatonin levels (5). However, two subsequent exper-iments conducted in a similar manner failed to replicatethis finding (5, 6).
A number of exposure measures were not associated withnocturnal urinary 6-sulfatoxymelatonin concentration,including 1) 24-hour personal magnetic field measurements,2) variability in magnetic field levels, 3) two measures oflight-at-night, and 4) wire code configuration. It is not clearfrom existing studies whether daytime exposure to magneticfields could act on melatonin rhythms at night or whether 24-hour measurements are sensitive enough to detect such an
TABLE 7. Estimated percentage decrease in urinary 6sulfatoxymelatonin concentration on 4 days of the year,for selected levels of mean nighttime magnetic fieldexposure, Washington State, 1994–1996
Vernal/autumnal equinox0.040†,‡0.0800.120.16
Summer solstice0.040‡0.0800.120.16
Winter solstice0.040‡0.0800.120.16
DoubleTripleQuadruple
DoubleTripleQuadruple
DoubleTripleQuadruple
6 (0, 12)9 (0, 18)
11 (0, 22)
8 (1, 14)12 (1, 21)14 (2, 26)
4 (–2, 10)6 (–4, 16)8 (–5, 20)
* Dose-response slopes from table 6 were used, adjusted for theeffects of age, no. of hours of darkness, medication use, body massindex, and alcohol consumption.
† 0.040 µT is the median value of all mean nighttime bedroommagnetic fields (n = 1,171).
‡ Referent.
Mean nighttimemagnetic field level
(µT) Notmedication
users
Estimated % decrease(two-sided 95%
confidence interval)*Increase
fromreferencemagneticfield level
Medicationusers
2 (–2, 5)3 (–3, 8)4 (–3, 10)
4 (–1, 8)6 (–2, 12)7 (–2, 15)
0 (–4, 4)0 (–7, 7)0 (–9, 8)
Downloaded from https://academic.oup.com/aje/article-abstract/154/7/591/107343by gueston 13 February 2018

Magnetic Fields, Light-at-Night, and Melatonin 599
Am J Epidemiol Vol. 154, No. 7, 2001
effect if one exists. Short-term variability in magnetic fieldlevels was investigated based on limited evidence that varia-tion in the application of a magnetic field (e.g., intermittentvs. constant) might enhance the biologic effect of exposure(8). Since a measure of natural light was included in theanalysis, the proportion of light measurements ≥10 lux pri-marily reflected the ambient light levels in the bedroom,which were extremely low. Self-report of turning on a lightduring the night may be subject to a greater degree of mis-classification than actual bedroom measurements of light. Inthis study, wiring configuration, a surrogate measure of mag-netic field exposure, was poorly correlated with nighttimemagnetic field measurements.
The biologic significance of the reductions in urinary 6-sulfatoxymelatonin concentration found in this study overlong periods of time is unknown. Nevertheless, these resultsare of considerable interest in the context of mechanismsthat could affect development of breast cancer. In its role asa neuroendocrine transducer, the pineal gland provides ahormonal signal that can affect release of gonadotropins(luteinizing hormone and follicle-stimulating hormone)from the pituitary (36–39). These two hormones are criticalin the biosynthesis of steroid hormones in the ovary, includ-ing estradiol (40, 41). Consequently, pineal function,through the reduced secretion and action of melatonin, mayinfluence ovarian function and estrogen production andthereby result in increased levels of circulating estrogen.There is a substantial body of experimental, epidemiologic,and clinical evidence that breast cancer risk is influenced byendogenous hormones (reviewed by Bernstein and Rossand by Dao (42, 43)). Animal studies have repeatedlydemonstrated that estrogens can induce and promote mam-mary tumors in rodents (43), and numerous epidemiologicstudies have found increased estrogen levels to be animportant factor in determining risk of breast cancer inhumans (42).
Evidence has recently emerged that melatonin levels canbe suppressed by electric and magnetic fields and by light,that manipulation of melatonin levels can affect develop-ment of mammary carcinoma in animals, and that exposureto either magnetic fields or light can enhance developmentof chemically induced mammary carcinoma in animals(reviewed by Stevens and Davis and by Brainard et al. (2,3)). The weight of this evidence provides a framework forpostulating a mechanism that might explain how exposureto power-frequency magnetic fields could influence therisk of breast cancer. The results reported here provideintriguing suggestions that exposure to magnetic fields inthe home setting at night is sufficient to depress the normalnocturnal rise in circulating melatonin. In the presentstudy, these effects were associated with relatively lowlevels of exposure and focus attention on the possibilitythat they occur primarily in persons whose melatonin lev-els are already low or perhaps are more susceptible tochange. Additional studies designed to clarify the influ-ence of magnetic field exposures on reproductive hor-mones in humans, and individual variation in baseline lev-els of melatonin and susceptibility to change in melatoninlevels, would be most useful.
ACKNOWLEDGMENTS
This research was supported by the Electric PowerResearch Institute through contracts with EM Factors ofRichland, Washington (WO 2964-25) and the FredHutchinson Cancer Research Center in Seattle, Washington(WO 2964-24).
The authors thank the following persons for their valuablecontributions to this study: Norma Logan, project manage-ment; Laurie Ludwig, management of field operations;Elizabeth Carosso, data management; Peggy Adams Myers,contract administration; JoAnn Prunty, melatonin analysis;Betsy Gilbert and Christine Karlsen, field technicians; andDr. Leeka Kheifets, project support at the Electric PowerResearch Institute.
REFERENCES
1. Stevens RG. Electric power use and breast cancer: a hypothe-sis. Am J Epidemiol 1987;125:556–61.
2. Stevens RG, Davis S. The melatonin hypothesis: electricpower and breast cancer. Environ Health Perspect 1996;104(suppl 1):135–40.
3. Brainard GC, Kavet R, Kheifets LI. The relationship betweenelectromagnetic field and light exposures to melatonin andbreast cancer risk: a review of the relevant literature. J PinealRes 1999;26:65–100.
4. Semm P. Pineal function in mammals and birds is altered byearth-strength magnetic fields. In: Moore-Ede MC, CampbellSS, Reiter RJ, eds. Electromagnetic fields and circadian rhyth-micity. Cambridge, MA: Birkhauser Boston, 1992.
5. Graham C, Cook MR, Riffle DW, et al. Nocturnal melatoninlevels in human volunteers exposed to intermittent 60 Hz mag-netic fields. Bioelectromagnetics 1996;17:263–73.
6. Graham C, Cook MR, Riffle DW. Human melatonin duringcontinuous magnetic field exposure. Bioelectromagnetics1997;18:166–71.
7. Wood AW, Armstrong SM, Sait ML, et al. Changes in humanplasma melatonin profiles in response to 50 Hz magnetic fieldexposure. J Pineal Res 1998;25:116–27.
8. Burch JB, Reif JS, Yost MG, et al. Nocturnal excretion of uri-nary melatonin metabolite among electric utility workers.Scand J Work Environ Health 1998;24:183–9.
9. Burch JB, Reif JS, Yost MG, et al. Reduced excretion of amelatonin metabolite in workers exposed to 60 Hz magneticfields. Am J Epidemiol 1999;150:27–36.
10. Juutilainen J, Stevens RG, Anderson LE, et al. Nocturnal 6-hydroxymelatonin sulfate excretion in female workers exposedto magnetic fields. J Pineal Res 2000;28:97–104.
11. Davis S, Mirick DK, Stevens RG. Residential magnetic fieldsand the risk of breast cancer. Am J Epidemiol (in press).
12. Waksberg J. Sampling methods for random digit dialing. J AmStat Assoc 1978;73:40–6.
13. Wertheimer N, Leeper E. Adult cancer related to electricalwires near the home. Int J Epidemiol 1982;11:345–55.
14. Yost MG. Alternative magnetic field exposure metrics: occu-pational measurements in trolley workers. Radiat ProtectDosim 1999;83:99–106.
15. The Surgeon General’s report on nutrition and health.Washington, DC: US Department of Health and HumanServices, 1988. (DHHS (PHS) publication 88-50210).
16. Beck-Friis J, von Rosen D, Kjellman BF, et al. Melatonin inrelation to body measures, sex, age, season, and the use ofdrugs in patients with major affective disorders and healthysubjects. Psychoneuroendocrinology 1984;9:261–77.
17. Yen SSC. Chronic anovulation due to CNS-hypothalamic-
Downloaded from https://academic.oup.com/aje/article-abstract/154/7/591/107343by gueston 13 February 2018

600 Davis et al.
Am J Epidemiol Vol. 154, No. 7, 2001
pituitary dysfunction. In: Yen SSC, Jaffe RB, eds.Reproductive endocrinology. 3rd ed. Philadelphia, PA: W BSaunders, 1991:631–89.
18. Reiter RJ, ed. The pineal gland. Vol I–III. Boca Raton, FL:CRC Press, 1981.
19. Harville DA. Mixed models methodology: theoretical justifi-cations and future directions. Proceedings of the StatisticalComputing Section, American Statistical Association, NewOrleans, Louisiana, 1988:41–9.
20. Jennrich RI, Schluchter MD. Unbalanced repeated-measuresmodels with structured covariance matrices. Biometrics1986;42:805–20.
21. Laird NM, Ware JH. Random-effects models for longitudinaldata. Biometrics 1982;38:963–74.
22. SAS Institute, Inc. SAS/STAT software: changes and enhance-ments through release 6.11. Cary, NC: SAS Institute, Inc,1996.
23. Goodnight JH. Tests of hypotheses in fixed-effects linear mod-els. Cary, NC: SAS Institute Inc, 1978. (SAS technical reportR-101).
24. Armitage P. Statistical methods in medical research. London,United Kingdom: Blackwell Scientific Publications, 1971:376.
25. Stevens RG, Davis S, Mirick DK, et al. Alcohol consumptionand urinary concentration of 6-sulfatoxymelatonin in healthywomen. Epidemiology 2000;11:660–5.
26. Bojkowski CJ, Arendt J. Annual changes in 6-sulfatoxymela-tonin in man. Acta Endocrinol (Copenh) 1988;117:470–6.
27. Wetterberg L, Eberhard G, Von Knorring L, et al. The influ-ence of age, sex, height, weight, urine volume and latitude onmelatonin concentrations: a multinational study. In:Wetterberg L, ed. Light and biological rhythms in man.Stockholm, Sweden: Pergamon Press, 1993.
28. Waldhauser F, Walentich W, Ehrhart B. The physiologicalsecretion pattern of melatonin in man. In: Touitou Y, Arendt J,Pevets P, eds. Melatonin and the pineal gland: from basic sci-ence to clinical application. New York, NY: Elsevier SciencePublishers, 1993:331–8.
29. Zeitzer JM, Daniels JE, Duffy JF. Do plasma melatonin con-centrations decline with age? Am J Med 1999;107:432–6.
30. Moss HB, Tamarkin L, Majchrowicz E, et al. Pineal functionduring ethanol intoxication, dependence, and withdrawal. LifeSci 1986;39:2209–14.
31. Chik CL, Ho AK. Ethanol reduces norepinephrine-stimulatedmelatonin synthesis in rat pinealocytes. J Neurochemistry1992;59:1280–6.
32. Ekman AC, Leppäluoto J, Huttunen P, et al. Ethanol inhibitsmelatonin secretion in healthy volunteers in a dose-dependentrandomized double blind cross-over study. J Clin EndocrinolMetab 1993;77:780–3.
33. Rojmark S, Wikner J, Adner N, et al. Inhibition of melatoninsecretion by ethanol in man. Metabolism 1993;42:1047–51.
34. McIntyre IM, Norman TR, Burrows GD, et al. Human mela-tonin suppression by light is intensity dependent. J Pineal Res1989;6:149–56.
35. McIntyre IM, Norman TR, Burrows GD, et al. Melatoninsupersensitivity to dim light in seasonal affective disorder.(Letter). Lancet 1990;335:488.
36. Bittman EL, Kaynard AK, Olster DH. Pineal melatonin medi-ates photoperiodic control of pulsatile luteinizing hormonesecretion in the ewe. Neuroendocrinology 1985;40:409–18.
37. Yellon SM, Foster DL. Melatonin rhythms time photoperiod-induced puberty in the female lamb. Endocrinology 1986;119:44–9.
38. Robinson JE, Kaynard AH, Karsch FJ. Does melatonin alterpituitary responsiveness to gonadotropin-releasing hormone inthe ewe? Neuroendocrinology 1986;43:635–40.
39. Robinson JE. Photoperiodic and steroidal regulation of theluteinizing hormone pulse generator in ewes. In: Crowley WF,Hofler JG, eds. The episodic secretion of hormones. NewYork, NY: John Wiley & Sons, 1987:159.
40. Catt KJ, Dafau ML. Gonadotropic hormones: biosynthesis,secretion, receptors, and actions. In: Yen SSC, Jaffe RB, eds.Reproductive endocrinology. 3rd ed. Philadelphia, PA: W BSaunders, 1991:144–51.
41. Adashi EY. The ovarian life cycle. In: Yen SSC, Jaffe RB, eds.Reproductive endocrinology. 3rd ed. Philadelphia, PA: W BSaunders, 1991:202–4.
42. Bernstein L, Ross RK. Endogenous hormones and breast can-cer risk. Epidemiol Rev 1993;15:48–65.
43. Dao TL. The role of ovarian steroid hormones in mammarycarcinogenesis. In: Pike MC, Siiteri PK, Welsch CW, eds.Hormones and breast cancer. (Banbury report no. 8). ColdSpring Harbor, NY: Cold Spring Harbor Laboratory, 1981:281–95.
Downloaded from https://academic.oup.com/aje/article-abstract/154/7/591/107343by gueston 13 February 2018
Recommended