Prostate Cancer Genetics and Diagnosis
Luke FrederickSUNA 2015
Outline
• Prostate cancer genetics– Hereditary risk– Genetics
• Prostate cancer diagnosis– PSA and prostate cancer screening– Pre-biopsy tools for diagnosing prostate cancer
• Recent advances in prostate cancer diagnosis– Biopsy techniques– Prostate MRI
• The future of prostate cancer diagnosis
Prostate cancer inheritance
• Familial studies• Ethnicity• Single nucleotide polymorphisms• BRCA1/BRCA2
Familial studies• Prostate cancer risk– 2x increased risk with first degree relative– 5-11x increased risk with 2-3 affected relatives– Relative dx at age <55 increases risk
• Twin study– Much higher risk if identical twin had prostate
cancer• Sons prognosis correlates with fathers
prognosis– Sons of fathers who survived 5 years vs. Sons
of fathers who survived 2 years
Ethnicity
• African-American men– 1.6x increased risk of diagnosis– Earlier age of onset• 8.3% of AA men <50• 3.3% white men <50
Genome studies
• Single nucleotide polymorphisms– Alleles that are associated with an increased
susceptibility to prostate cancer• Swedish study– Panel of five SNPs from three loci in 8q24, as well
as single sites in 17q12 and 17q24.3– If 4/5 SNPs were present then 4x increased risk– 4/5 SNPs with family hx of prostate cancer then 9x
risk
BRCA1/BRCA2• BRCA1– Breast, ovarian, fallopian, and prostate cancer– 1.8x increased risk of prostate cancer
• BRCA2– Breast, ovarian, Fallopian tube, prostate, and
pancreatic cancer– 4.7x increased risk of prostate cancer
HOXB13
• Homeobox B13 (HOXB13) gene – codes for a transcription factor that is important in
prostate development. – The G84E variant of the HOXB13 gene• 20-fold increase in the frequency of this variant in men
with prostate cancer compared with those without prostate cancer
Prostate cancer diagnosis
• Prostate cancer screening• What is PSA• Guidelines on PSA screening• What’s new? Pre-biopsy tools
Cancer screening test
• Goals of a screening test– Find cancer before symptoms appear– Screens for a cancer that is easier to treat and
cure when found early– Has few false-negative test results and false-
positive test results– Decreases the chance of dying from cancer
• Screening tests do NOT diagnose cancer
PSA
• Prostate specific antigen– Enzyme secreted by the prostate gland– Produced for the ejaculate it liquefies semen
and allows sperm to swim freely• PSA elevation– Cancer– Benign prostatic hyperplasia (BPH)– Infection
PSA as a screening test
• Find cancer before symptoms appear– Yes
• Screens for a cancer that is easier to treat and cure when found early– Yes, metastatic prostate cancer is not curable
• Has few false-negative test results and false-positive test results– Needs some work
• Decreases the chance of dying from cancer– Yes
AUA guidelines on prostate cancer screening
• < 40: No screening• 40-54: May screen men with family history or
African Americans• 55-69: Shared decision making process• >70: No screening, or if the person's life
expectancy is less than 10 years• Screen every 2-4 years
PSA is high (>3), What’s next?
• Has few false-negative and false-positive test results
• Pre-biopsy tools– First recheck PSA– Available tools• Individualized Risk Assessment of Prostate Cancer• Free and total PSA• Prostate health index• PCA3
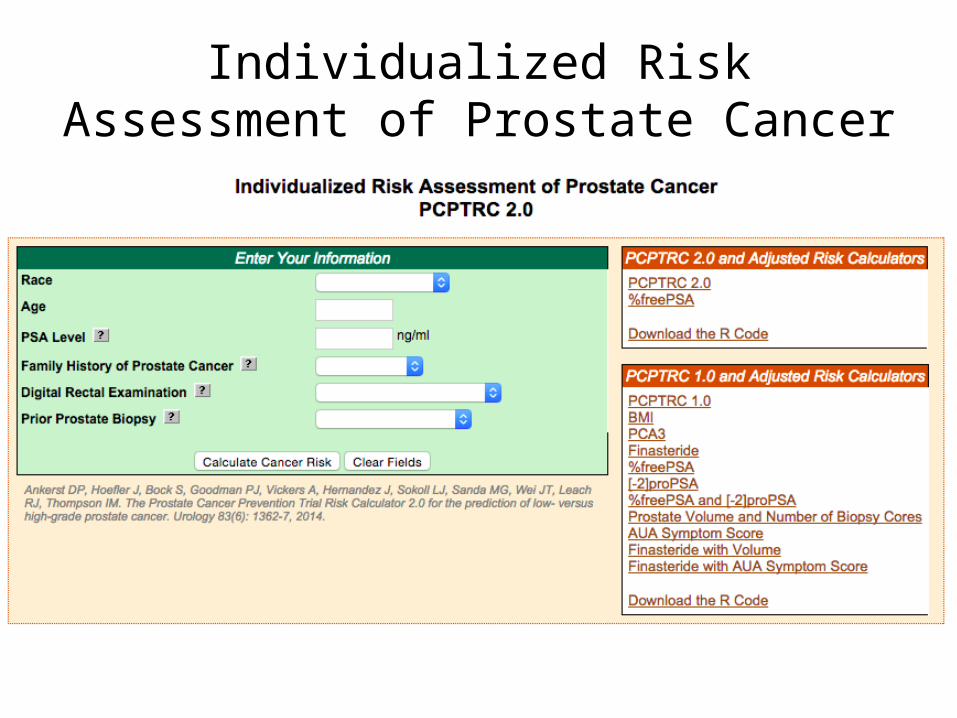
Individualized Risk Assessment of Prostate Cancer
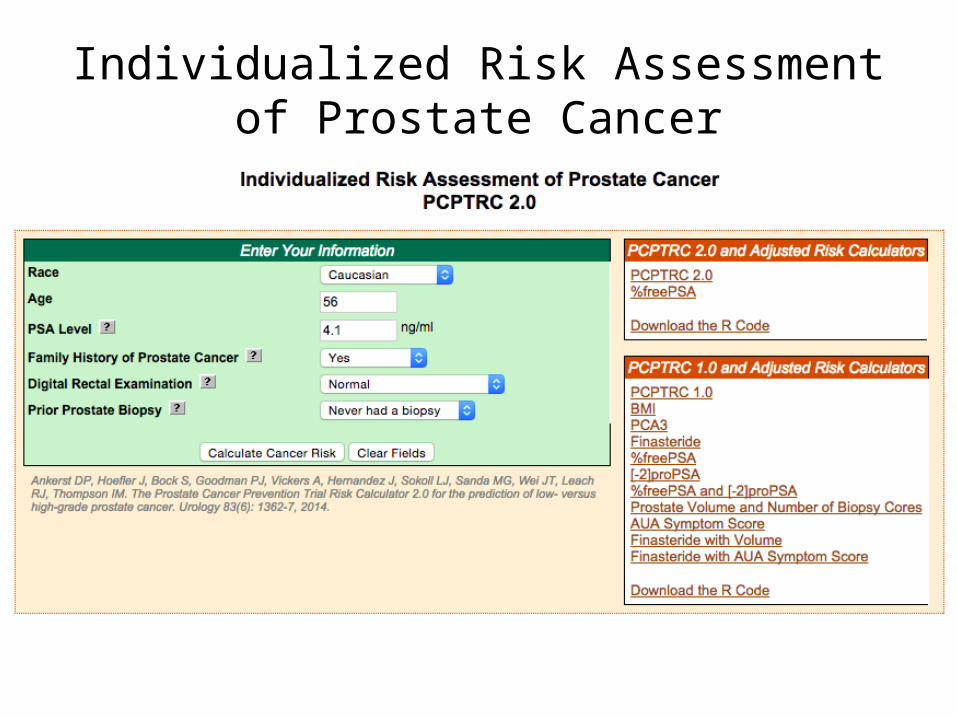
Individualized Risk Assessment of Prostate Cancer
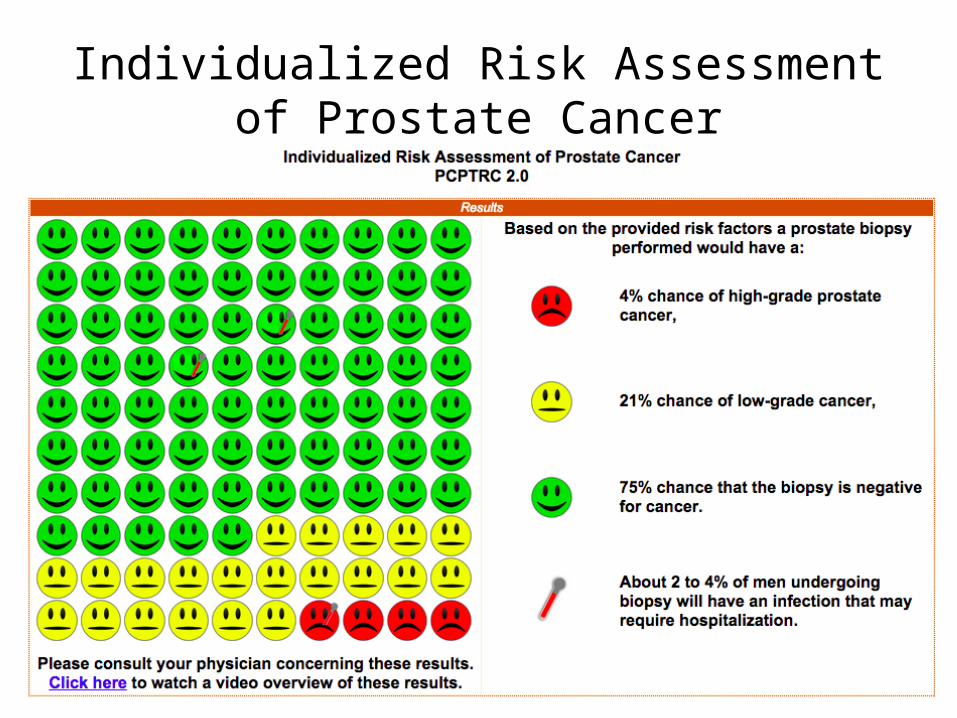
Individualized Risk Assessment of Prostate Cancer
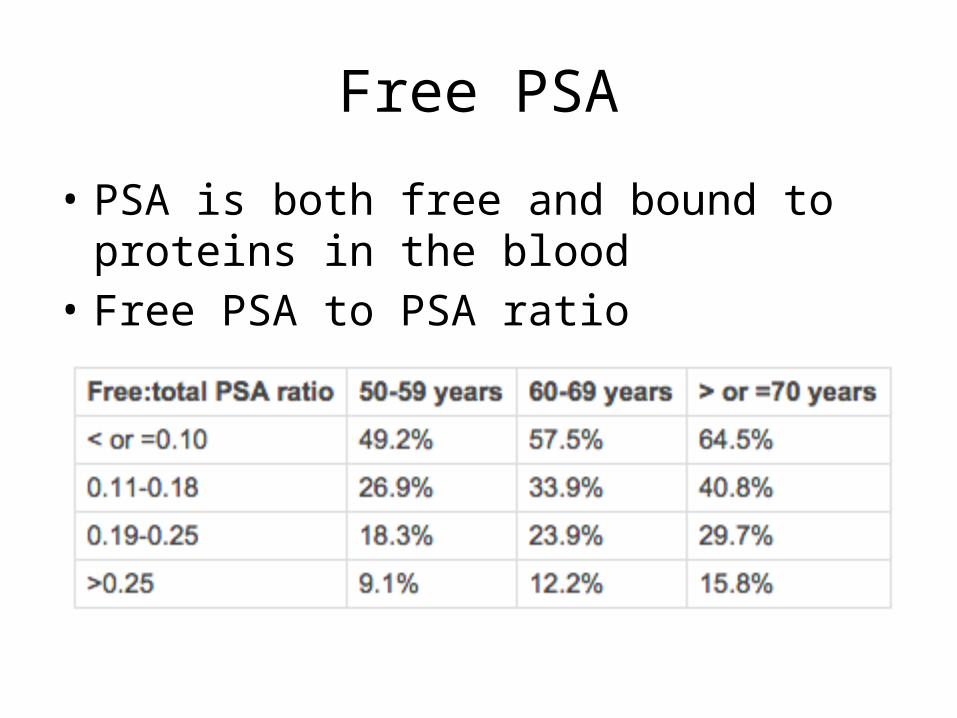
Free PSA
• PSA is both free and bound to proteins in the blood
• Free PSA to PSA ratio
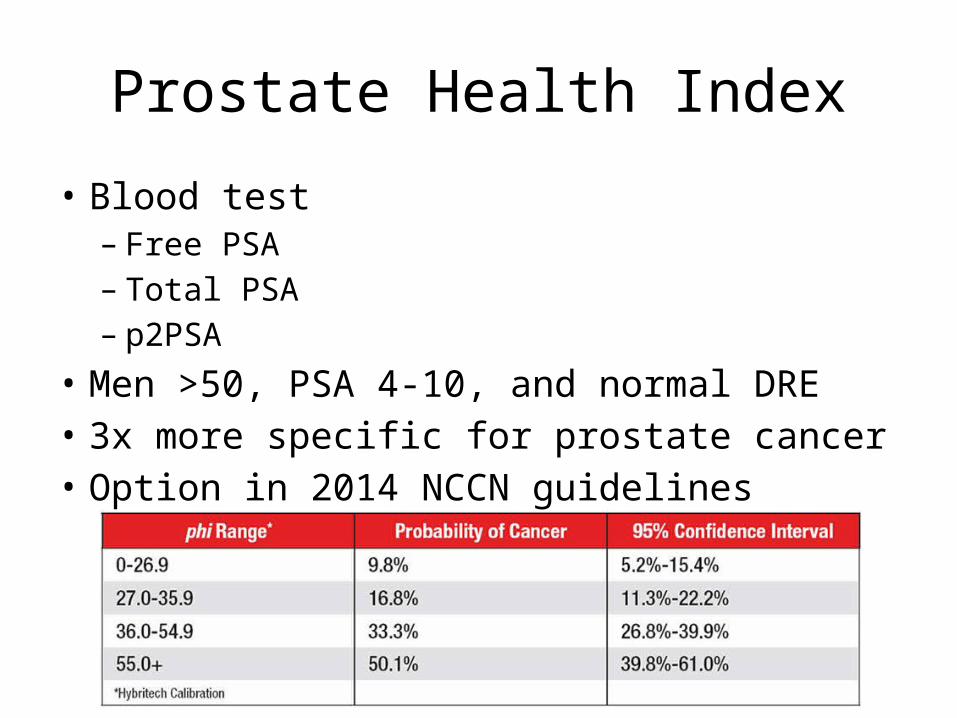
Prostate Health Index
• Blood test– Free PSA– Total PSA – p2PSA
• Men >50, PSA 4-10, and normal DRE• 3x more specific for prostate cancer• Option in 2014 NCCN guidelines
PCA3
• Urine test– Nucleic acid amplification test– Measures the concentration of prostate cancer gene 3
(PCA3) and PSA– Uses that to provide a score
• Procedure– DRE, first catch urine specimen, sent to outside lab
• FDA approved for men 50 years of age or older who have had one or more previous negative prostate biopsies
PCA3
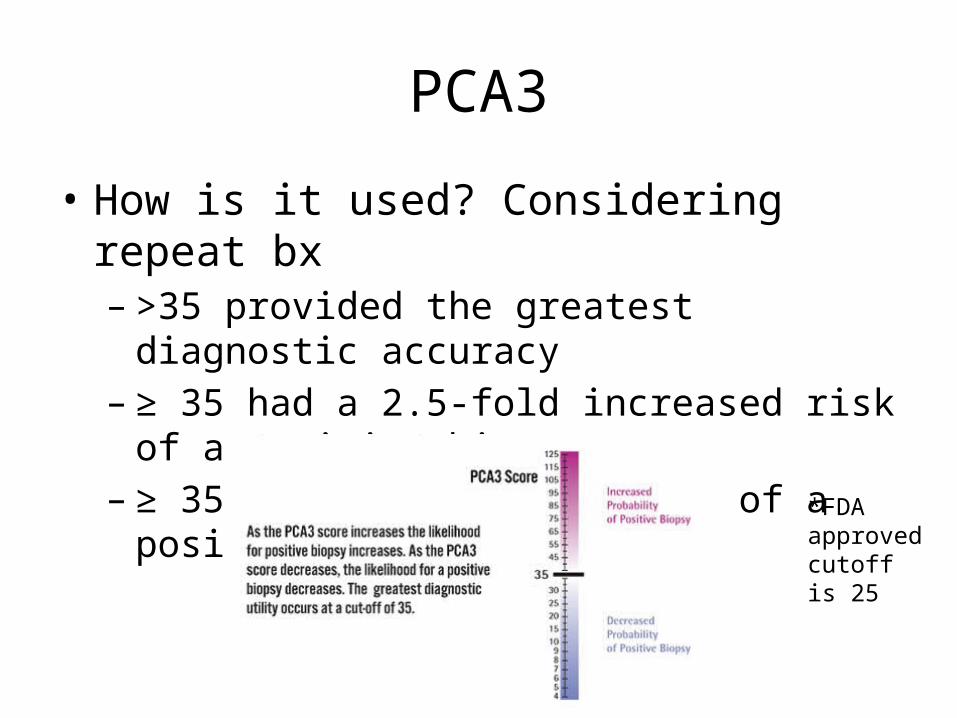
• How is it used? Considering repeat bx – >35 provided the greatest diagnostic accuracy– ≥ 35 had a 2.5-fold increased risk of a positive
biopsy– ≥ 35 had a 43% probability of a positive biopsy
*FDA approved cutoff is 25
PCA3
• What about initial biopsy?– Not FDA approved• ≥ 35 had a 2-fold increased risk of a positive biopsy• ≥ 35 had a 62% probability of a positive biopsy
– PCA3 cutoff of 35: 21% false negative– PCA3 cutoff of 25: 15% false negative– PCA3 cutoff of 10: 5% false negative
What’s next?
• Elevated PSA rechecked PSA pre biopsy tool of choice confirms risk prostate biopsy
• In order to dx cancer you must have tissue
Prostate biopsy
• Transrectal ultrasound guided prostate biopsy• Prostate MRI• MRI fusion prostate needle biopsies
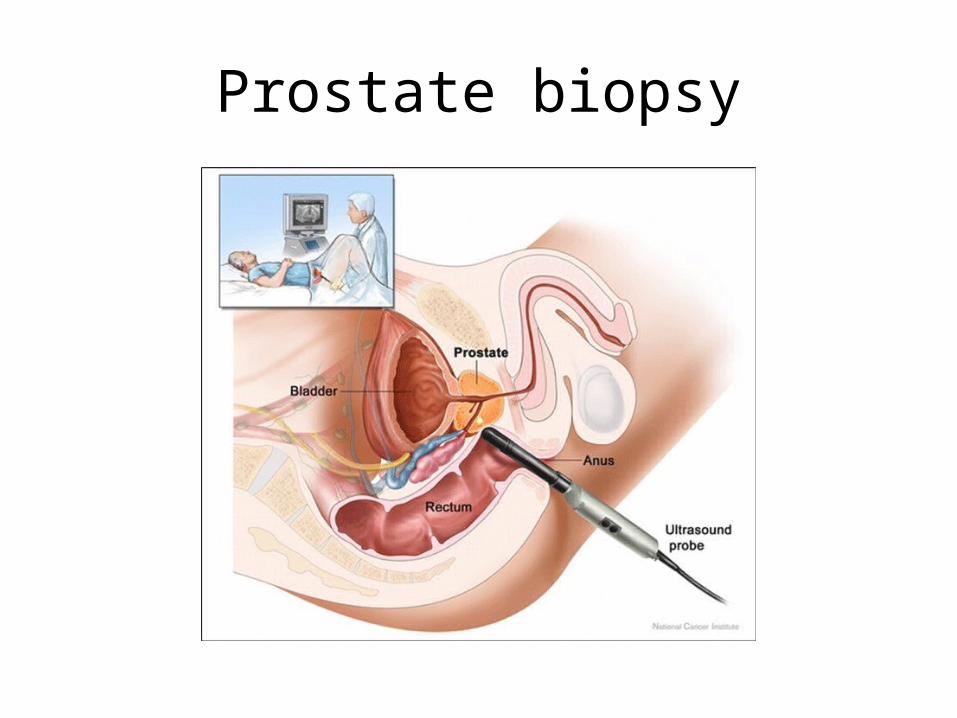
Prostate biopsy
TRUS bx
• Results– 75% of those biopsied will be negative– 50% will have hematuria/hematospermia– 4% will have fever/hospitalization after bx
• Up to 20% will miss cancer• Up to 40% will be under sampled– i.e. actually have intermediate risk cancer when
only low risk cancer was found
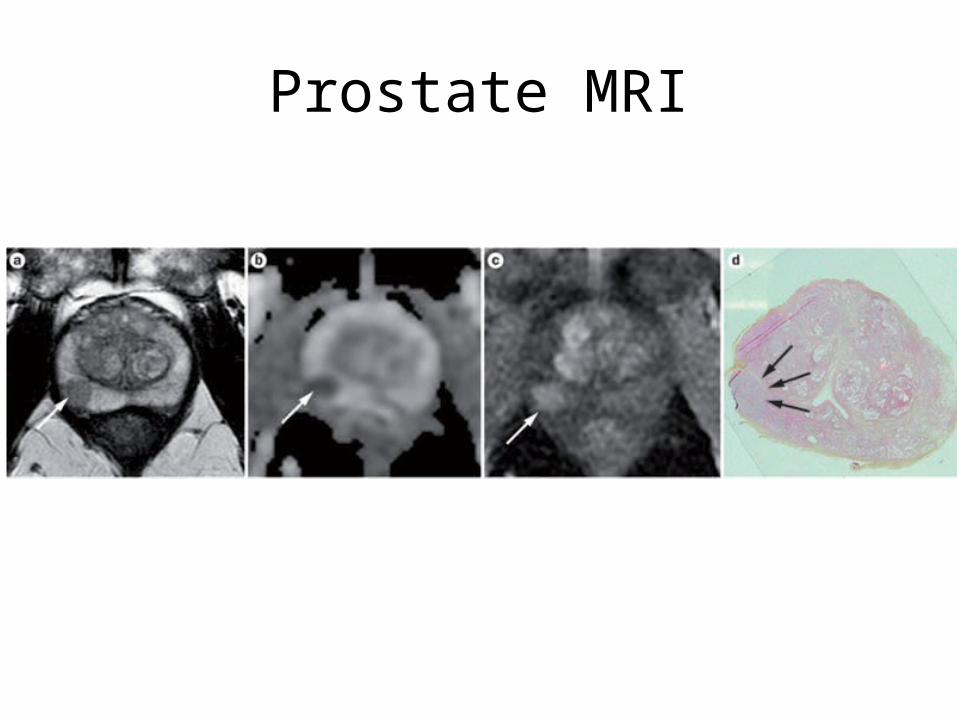
Prostate MRI
• Multiparametric MRI, no endorectal coil• Three elements– T2 weighted images– Diffusion weighted images– Perfusion images
Prostate MRI
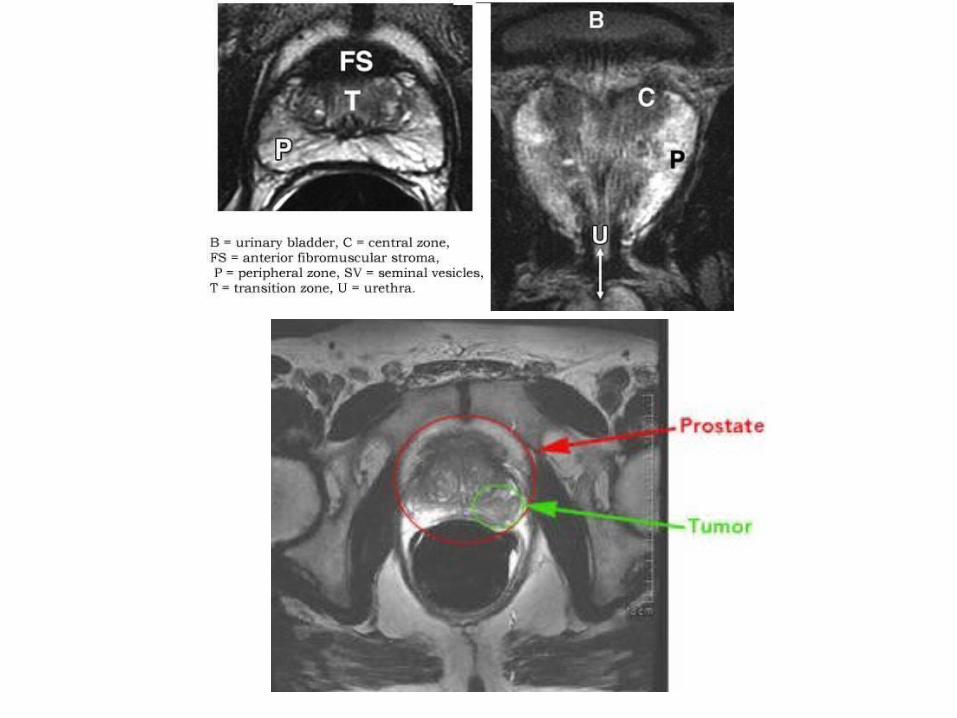
• T2 weighted images– Tissue water content– Clearly define the zonal anatomy of the prostate – Prostate cancer can appear as an area of low
signal intensity. – The degree of intensity decrease differs with
Gleason score as higher Gleason score components show lower signal intensities
Prostate MRI
Prostate MRI
• Diffusion weighted images– Diffusion weighted MRI measures the random
motion of water molecules. – Prostate cancer shows a low apparent diffusion
coefficient
Prostate MRI
• Perfusion images– Contrast enhanced MRI – Sequences covering the prostate before and after
gadolinium– Prostate cancer typically enhances faster and to a
greater extent than the surrounding prostate, and will also show more rapid washout of contrast
Prostate MRI
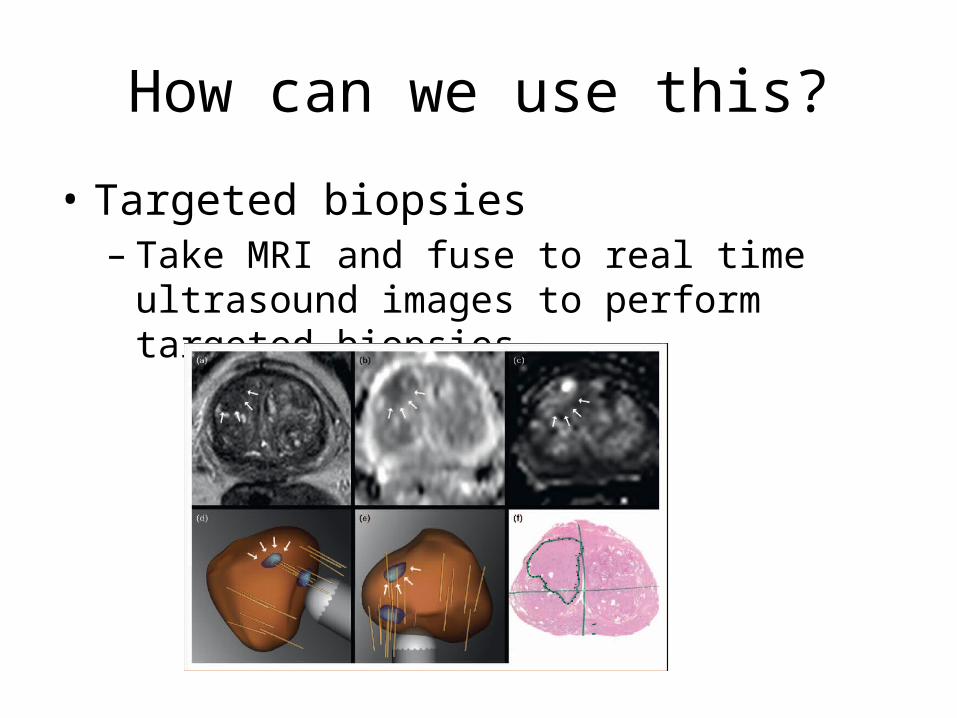
How can we use this?
• Targeted biopsies– Take MRI and fuse to real time ultrasound images
to perform targeted biopsies
MRI fusion biopsy
• Potential benefits– Reduce false negative biopsies – Improve accuracy in risk classification through
better tumor sampling– Reduction in false-negative biopsies could reduce
the necessity of repeat biopsies
MRI fusion biopsy
• 223 men• TRUS bx detected PCa in 56.5% and 37.3% were low
risk. • MRI bx detected 69.7% with equivocal or suspicious
MRI, of which 6.1% were low risk. • MRI pathway– Reduced the need for biopsy by 51%, – Decreased the diagnosis of low-risk PCa by 89.4%, and – Increased the detection of intermediate/high-risk PCa by
17.7%. European Urology 2014PMID: 24666839
SIU Urology
• SIU/SJH - prostate MRI imaging using MSK protocols
• SIU has one of the most extensive experiences in Illinois– Dr. Kevin McVary and Dr. Shaheen Alanee
• SIU/SJH – One of only 2 MRI targeted biopsy centers in Illinois
What’s next?
• Will Multi-Parametric Magnetic Resonance Imaging be the Future Tool to Detect Clinically Significant Prostate Cancer?
Review
• Prostate cancer genetics– Hereditary risk– Genetics
• Prostate cancer diagnosis– PSA and prostate cancer screening– Pre-biopsy tools for diagnosing prostate cancer
• Recent advances in prostate cancer diagnosis– Biopsy techniques– Prostate MRI
Recommended