
ORIGINAL ARTICLE
Prenatal expectations in Mexican Americanwomen: development of a culturally sensitive measure
Jenna L. Gress-Smith & Danielle S. Roubinov &
Rika Tanaka & Keith Cirnic & Nancy Gonzales &
Craig Enders & Linda J. Luecken
Received: 20 December 2012 /Accepted: 27 March 2013 /Published online: 17 April 2013# Springer-Verlag Wien 2013
Abstract Prenatal expectations describe various domains awoman envisions in preparation for her role as a new motherand influence how women transition into the maternal role.Although the maternal role is strongly influenced by theprevailing familial and sociocultural context, research char-acterizing prenatal expectations in ethnic minority and low-income women is lacking. As part of the largest growingminority group in the USA, Latina mothers represent animportant group to study. Two hundred and ten low-income Mexican American women were administered thePrenatal Experiences Scale for Mexican Americans(PESMA) that was adapted to capture specific cultural as-pects of prenatal expectations. Measures of current support,prenatal depressive symptoms, and other sociodemographiccharacteristics were also completed to assess validity. Ex-ploratory factor analysis identified three underlying factorsof prenatal expectations: paternal support, family support,and maternal role fulfillment. Associations among thesesubscales and demographic and cultural variables wereconducted to characterize women who reported higher andlower levels of expectations. The PESMA demonstratedgood concurrent validity when compared to measures ofsocial support, prenatal depressive symptoms, and othersociodemographic constructs. A culturally sensitive mea-sure of prenatal expectations is an important step towardsa better understanding of how Mexican American womentransition to the maternal role and identify culturally specifictargets for interventions to promote maternal health.
Keywords Expectations . Pregnancy . Mexican American .
Social support . Family support
Introduction
The transition to motherhood begins prenatally, with prepa-rations for the parental role. Becoming a mother has beendescribed as a transformational process during which wom-en anticipate and cognitively “rehearse” for their postpartumrole by forming expectations of what life may be likefollowing childbirth (Lederman 1996). The construct ofprenatal expectations has been used in prior researchto describe various domains of parenthood that a wom-an envisions during pregnancy. The maternal role hasbeen described as a “social construct” with qualities thatare strongly influenced by the prevailing familial andsociocultural context (Guendelman et al. 2001;Sagrestano et al. 1999). Yet, research characterizingmaternal prenatal expectations has been largelyconducted among samples of middle-class, Caucasianwomen, with little attention to how ethnic minorityand low-income women approach motherhood. As thelargest minority group in the USA with fertility rates30–40 % higher than any other ethnic group (Hamiltonet al. 2005; US Census Bureau 2011), Hispanic mothersrepresent a particularly important cultural group to stud-y. Among Hispanic women, Mexican Americans1 havethe highest birthrates (Martin et al. 2012) and are alsomore likely to be exposed to life stressors that may bear
1 For the purposes of this research, “Mexican American” refers to anywomen of Mexican heritage residing in the USA, regardless of nativityor citizenship.
J. L. Gress-Smith (*) :D. S. Roubinov : R. Tanaka :K. Cirnic :N. Gonzales :C. Enders : L. J. LueckenDepartment of Psychology, Arizona State University, 950 S.McAllister St., P.O. Box 871104, Tempe, AZ 85287-1104, USAe-mail: [email protected]
Arch Womens Ment Health (2013) 16:303–314DOI 10.1007/s00737-013-0350-2

considerably on the pregnancy period, including decreasedlikelihood of having insurance, lower levels of financial re-sources, and increased discrimination (Flores et al. 2008;Hamilton et al. 2006; Ramierez and de la Cruz 2002). Theunique socioeconomic and psychosocial risk factors facingMexican American women during the transition to parent-hood support a dedicated study of their prenatal experiences.The current study describes the psychometric properties of anexisting measure that was adapted to evaluate prenatal expec-tations among low-income Mexican American pregnantwomen and explores the demographic, cultural, and psycho-social correlates of women’s anticipated views of the earlypostpartum period.
Forming expectations serves an important purpose duringmajor transitions, countering the uncertainty associated withsignificant life changes by contributing to the sense thatevents are predictable and under one’s personal control(Lawrence et al. 2007). Rubin (1984) suggested that prena-tal expectations are conjectures or hypotheses of what par-enthood will entail that originate from values, priorexperiences, and contexts with which women approach thematernal role. Expectations formed prenatally about thepostpartum period may be adaptive, preparing women tocope with parenting stressors, and successfully transitioninto the maternal role following the birth of a child.Pancer et al. (2000) observed that pregnant women whoenvisioned more positive infant caring experiences ex-perienced lower levels of depression and increased self-esteem following childbirth as compared to women whoendorsed poorer expectations for the postpartum period.
In prior research, frequently assessed domains ofprenatal expectations include women’s projections aboutparenting self-efficacy, fulfillment anticipated from thematernal role, expected changes in employment, lifestyleor household responsibilities, anticipated receipt of so-cial support during the early postpartum period from herpartner and family, and assumptions of positive/negativechanges in other social relationships (Coleman et al. 1999;Delmore-Ko et al. 2000; Kiang et al. 2004; McHale et al.2004; Tamis-Lemonda and Kahana-Kalman 2009). Categoriesof prenatal expectations have been formed on the basis ofqualitative analysis of in-depth prenatal interviews (Delmore-Ko et al. 2000; Pancer et al. 2000; Tamis-Lemonda andKahana-Kalman 2009) and quantitative analysis of self-reportscales (Coleman et al. 1999; Kiang et al. 2004; McHale et al.2004). Expectations may vary along a continuum of verypositive to very negative; although expectant mothers mayanticipate parenthood with enthusiasm and excitement, theprenatal period may also be marked by significant concernsabout the challenges of caring for a newborn (Fox et al. 2000).
Although little is known about the demographic andpsychosocial characteristics of women who form higherand lower prenatal expectations, previous experience with
infants and confidence in one’s ability to handle the care of anewborn baby may contribute to more positive expectationsfor transitioning into the maternal role. Other characteristicssuch as family context, socioeconomic status, and maternaleducation level may also bear on the formation of prenatalexpectations. For example, anticipated postpartum paternalsupport may be higher among women married to and/orresiding with the father of their baby, while expectationsof the financial impact of a child may vary depending onwomen’s socioeconomic status and levels of current finan-cial hardship. Additionally, relations between expectationsand prenatal mood are important to explore, as negativeprenatal expectations have been posited to correlate withprenatal distress (Lucas 2010). Prenatal distress, in turn,has been associated with poor birth outcomes and elevatedrisk of postpartum depression (Field 2011).
Prenatal expectations likely vary across cultures, but ethnicand cultural considerations have rarely been addressed in priorstudies. The influence of social and ecological forces onmaternal prenatal expectations may be accentuated amongMexican American women for whom the meaning of moth-erhood is shaped by strong cultural values and norms relatedto motherhood and family relationships. Hispanic womenhave been described as adhering strongly to familism valuesthat emphasize attachment to the nuclear and extended family(Germán et al. 2009; Rafaelli and Ontai 2004), and priorqualitative research has observed that the prenatal expecta-tions of Mexican American women are more likely includethemes related to the effect of a new child on the family unit ascompared to women from other ethnic groups (Tamis-Lemonda and Kahana-Kalman 2009). Familism values arealso related to marianismo, a construct that sets forthgender-specific role expectations regarding the centrality ofmotherhood and childcare in the lives of Hispanic women(Castillo et al. 2010). Mexican American women often incor-porate the maternal role into their self-identity, finding valueand meaning in being a mother. Culturally specific constructsrelated to mothering (e.g., motherhood as a valued and re-warding life experience) have been associated with positivepregnancy and birth experiences among Mexican Americanwomen (Page 2004). The content of Mexican Americanwomen’s prenatal expectations and their relation to culturalvalues may vary with level of acculturation. The transition toparenthood may be influenced by acculturation as majorityculture values of individualism, self-development, and per-sonal goals, and egalitarian gender role attitudes are increas-ingly adopted (Wilson 1998).
Cultural beliefs related to parenthood and child rearingoffer a unique framework by which Mexican American wom-en prepare to assume the maternal role, requiring adaptation ofexisting measures of prenatal expectations that were devel-oped for majority populations. The current paper describes thedevelopment and validation of the Prenatal Experiences Scale
304 J.L. Gress-Smith et al.

for Mexican Americans (PESMA), a culturally sensitive as-sessment of prenatal expectations for low-income MexicanAmerican women. Taking prior empirical research and cultur-al considerations into account, the Prenatal Maternal Expec-tations Scale (Coleman et al. 1999) was extensively modifiedto evaluate prenatal expectations for life following the birth ofa child in low-income Mexican American women. Explorato-ry factor analyses examined the structure underlying prenatalexpectations. Additional analyses evaluated relations amongexpectations and concurrent measures of social support, de-pression, cultural constructs (e.g., familism and acculturation),and other sociodemographic factors to further characterize thenature of prenatal expectations among low-income MexicanAmerican women and provide concurrent validation for thePESMA.
Materials and methods
Participants
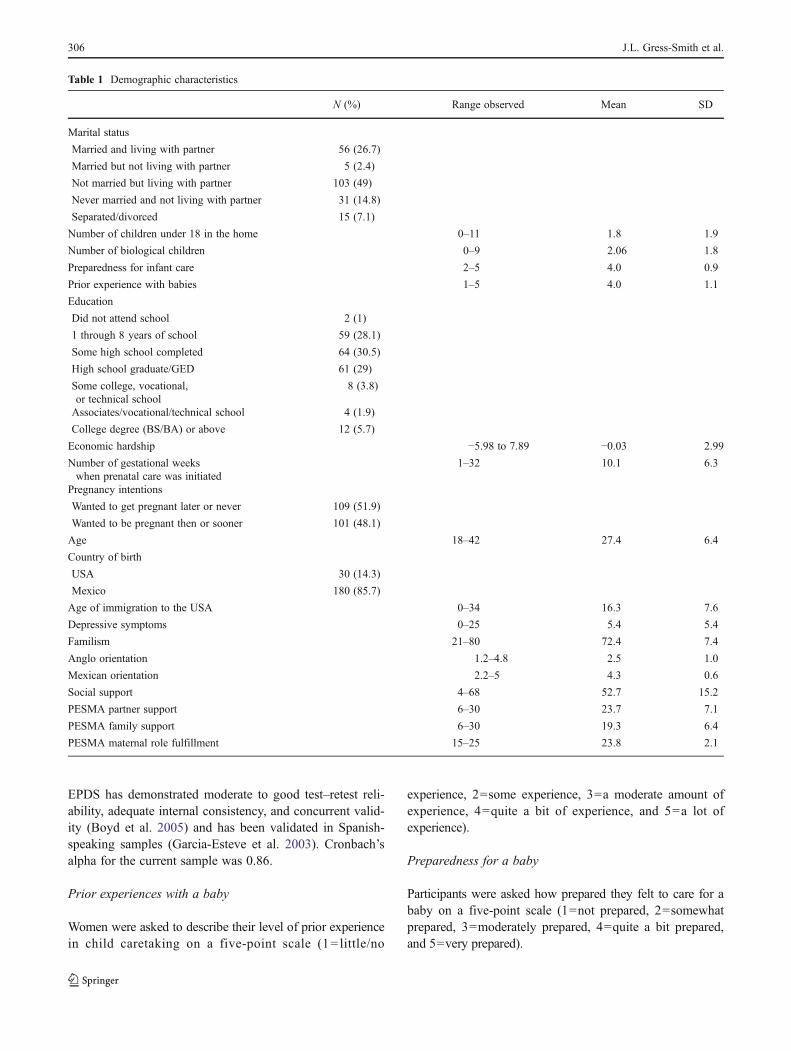
Participants included 210 self-identified Mexican Americanwomen (M age=27.4 years, SD=6.4) recruited for a largerlongitudinal study of maternal and infant health thatfollowed women and their infants for 3 years followingthe birth. Data collected during the prenatal assessment onlywere used for the current study. Women were invited toparticipate if the following eligibility criteria were met: (1)self-identification as Mexican American, (2) English orSpanish language fluency, (3) age 18 or older, (4) low-income status (self-reported income below $25,000 or eli-gibility for federal emergency medical services funding),and (5) anticipated delivery of a healthy, singlet baby. De-mographic characteristics of the sample are shown inTable 1.
Procedures
Women were recruited from a hospital-based clinic that pro-vides prenatal care to low-income women in the surroundingurban community. During prenatal care appointments, preg-nant women prior to 38 weeks gestation were introduced to thestudy by a female, bilingual interviewer. A total of 343 womenwere approached for recruitment during a prenatal care ap-pointment. Of these, 286 (83 %) agreed to be contacted toschedule a prenatal home visit, at which informed consent wasobtained. Of the women who agreed to schedule a home visit,36 (13%) could not be contacted to schedule the visit, 17 (6%)refused to participate, and 23 (8 %) were ineligible (were notMexican American, delivered prior to completing a prenatalhome visit, had a miscarriage, or moved out of state). Our finalsample consisted of 210 women who consented to be part ofthe study.
Prenatal home visits took place between 23 and 41 weeksgestation (M=35.2, SD=2.9). Interviews were conducted inthe language with which participants were most comfortable(82% Spanish and 18% English). Due to variations in literacy,informed consent and all study questions were read aloud towomen, and responses were entered by the interviewer into alaptop computer. Women were compensated $75 for the inter-view and received small gifts in preparation for their baby’sbirth (e.g., bath oils, lip balm, and lotion).
Measures
Validated Spanish versions of the measures were used whenavailable. For measures without a validated Spanish version,measures were translated and back translated by certifiedSpanish–English translators. The translations were thenchecked for accuracy by a separate team of bilingual studypersonnel to ensure they were culturally sensitive and ap-propriate to the local population of Spanish speakers. Anydiscrepancies were resolved by principal investigators or thelead translators.
Demographic characteristics
Women were queried about marital status, number of bio-logical children, total number of children under 18 years ofage residing in the home, educational history, age, andcountry of birth. Because the majority of the women wereborn in Mexico (86 %), women were also asked how longthey had lived in the USA.
Economic hardship
Perceived financial difficulties were assessedwith the econom-ic hardship scale (EHS; Barrera et al. 2001). The EHS wasdeveloped for low-income families and measures psychologi-cal aspects of poverty, including overall financial strain, lack ofmoney for necessities, need for economic adjustments or cut-backs, and inability to make ends meet. Assessing the subjec-tive nature of financial difficulties, rather than categorical totalincome, provides more information regarding need and depri-vation in impoverished families (Barrera et al. 2001). Partici-pants considered their financial situation for a 3-month timeframe and answered 20 questions using a Likert scale rangingfrom 1 to 5, with lower scores indicating higher levels offinancial strain. Scores from the four subscales were standard-ized and combined to form a single score of economic hardship(α=0.74)
Prenatal depressive symptoms
Depressive symptoms were measured with the EdinburghPostnatal Depression Scale (EPDS; Cox et al. 1987). The
Prenatal expectations in Mexican American women 305
EPDS has demonstrated moderate to good test–retest reli-ability, adequate internal consistency, and concurrent valid-ity (Boyd et al. 2005) and has been validated in Spanish-speaking samples (Garcia-Esteve et al. 2003). Cronbach’salpha for the current sample was 0.86.
Prior experiences with a baby
Women were asked to describe their level of prior experiencein child caretaking on a five-point scale (1= little/no
experience, 2=some experience, 3=a moderate amount ofexperience, 4=quite a bit of experience, and 5=a lot ofexperience).
Preparedness for a baby
Participants were asked how prepared they felt to care for ababy on a five-point scale (1=not prepared, 2=somewhatprepared, 3=moderately prepared, 4=quite a bit prepared,and 5=very prepared).
Table 1 Demographic characteristics
N (%) Range observed Mean SD
Marital status
Married and living with partner 56 (26.7)
Married but not living with partner 5 (2.4)
Not married but living with partner 103 (49)
Never married and not living with partner 31 (14.8)
Separated/divorced 15 (7.1)
Number of children under 18 in the home 0–11 1.8 1.9
Number of biological children 0–9 2.06 1.8
Preparedness for infant care 2–5 4.0 0.9
Prior experience with babies 1–5 4.0 1.1
Education
Did not attend school 2 (1)
1 through 8 years of school 59 (28.1)
Some high school completed 64 (30.5)
High school graduate/GED 61 (29)
Some college, vocational,or technical school
8 (3.8)
Associates/vocational/technical school 4 (1.9)
College degree (BS/BA) or above 12 (5.7)
Economic hardship −5.98 to 7.89 −0.03 2.99
Number of gestational weekswhen prenatal care was initiated
1–32 10.1 6.3
Pregnancy intentions
Wanted to get pregnant later or never 109 (51.9)
Wanted to be pregnant then or sooner 101 (48.1)
Age 18–42 27.4 6.4
Country of birth
USA 30 (14.3)
Mexico 180 (85.7)
Age of immigration to the USA 0–34 16.3 7.6
Depressive symptoms 0–25 5.4 5.4
Familism 21–80 72.4 7.4
Anglo orientation 1.2–4.8 2.5 1.0
Mexican orientation 2.2–5 4.3 0.6
Social support 4–68 52.7 15.2
PESMA partner support 6–30 23.7 7.1
PESMA family support 6–30 19.3 6.4
PESMA maternal role fulfillment 15–25 23.8 2.1
306 J.L. Gress-Smith et al.

Weeks pregnant at first prenatal care visit
Women reported how far along they were in their pregnancywhen they first saw a physician to begin prenatal care.
Pregnancy intention
The intendedness of the current pregnancy was assessed byasking women if they wished to be pregnant: sooner/at thecurrent time or at a later time/never.
Familism
Familism values were evaluated with 16 items from the Mex-ican American Cultural Values Scale (Knight et al. 2009).Three subscales assessed beliefs about the family unit asrelated to familial obligations (e.g., “Parents should be willingto make great sacrifices to make sure their children have abetter life;” five items,α=0.59), family support and emotionalcloseness (e.g., “It is important for family members to showtheir love and affection for one another;” six items, α=0.77),and the use of the family as a source of reference (e.g., “Whenit comes to important decisions, the family should ask foradvice from close relatives;” five items, α=0.68). Participantsindicated how much they agreed or disagreed with each itemon a scale from 1 (strongly disagree) to 5 (strongly agree).Correlations among the subscales ranged from r=0.60 tor=0.69 and were subsequently combined to form a singlevariable representative of overall endorsement of familismvalues (α=0.86).
Acculturation
The Acculturation Rating Scale for Mexican Americans(Cuellar et al. 1995) evaluated women’s level of accultura-tion. The 30-item scale is a widely used measure of accul-turation that assesses adaptation to majority culture (13-itemAnglo Orientation Scale; α=0.93) and ethnic culture (17-item Mexican Orientation Scale; α=0.87) to provide amultidimensional assessment of acculturation.
Social support
Level of current social support was assessed with 17 itemsfrom the Medical Outcome Study Social Support Survey(Sherbourne and Stewart 1991). Participants were asked toindicate the frequency with which they had someone theycould rely on for emotional/informational support (e.g.,someone to confide in or someone who will give you goodadvice), tangible support (e.g., someone to take you to thedoctor), affectionate support (e.g., someone who shows youlove), and positive social interactions (e.g., someone to gettogether with for relaxation). Items were rated on a five-
point scale from 1 (never) to 5 (all the time) with higherscores indicative of greater availability of social support.Items were summed across dimensions to provide an overallindex of the perceived availability of support (α=0.96).
Satisfaction with paternal support
Level of satisfaction from the baby’s father was evaluatedwith a single item, “Overall, how satisfied are you with thesupport that you get from your baby’s biological father?”,rated on a five-point scale ranging from 1 (not at all satis-fied) to 5 (extremely satisfied).
Prenatal maternal expectations
Development of the PESMA, a culturally sensitive measureof prenatal maternal expectations, was guided by prior re-search on maternal expectations and research on culturalcharacteristics of Mexican American families. Twelve itemswere selected from the Prenatal Maternal Expectations Scale(PMES; Coleman et al. 1999), a measure that assessedbeliefs and expectations about motherhood among a sampleof middle-class, predominantly Caucasian women. ThePMES scale was chosen as the basis for development ofthe PESMA because it was the only known prospectivemeasure that assessed prenatal maternal expectations overa broad range of domains and had been validated in priorsamples (e.g., Baor and Soskolne 2010). Prior research haspredominantly relied on qualitative studies or retrospectivemeasures of prenatal expectations or has focused on a spe-cific domain of expectations (e.g., marital adjustment anddivision of household labor). The original PMES measurecontained 46 items organized a priori into five subscales,including expectations about the baby’s appearance andwell-being, enjoyment of motherhood, influence on friend-ships and other relationships, impact on the mother’s per-sonal life, and expectations related to how a womanenvisions herself as a mother. Items retained from the orig-inal PMES measure were those that were considered alignedwith culturally relevant motherhood themes (e.g., familysupport and centrality of the maternal role). Items reflectingthe loss of extracurricular activities and hobbies followingchildbirth were omitted. Minor changes were made from theoriginal wording to accommodate the low literacy level ofthe current sample. Based on theory and prior empiricalresearch, items were added to capture culturally specificexpectancies about life following the birth of a child. Suchitems assessed expectations of family support followingchildbirth (e.g., “Your mother or other women in yourfamily will teach you how to care for your baby”) andanticipated beliefs related to the centrality of marianismoto women’s identities (e.g., “Becoming a mother will be oneof the best things you’ve ever done”). The final measure
Prenatal expectations in Mexican American women 307

contained 34 items rated on a five-point scale from 1=“notat all” to 5=“completely,” with higher scores reflectinghigher expectations for the postpartum period in eachdomain.
Data analyses
Because previous studies have not examined the psychometricproperties of prenatal expectations in Mexican Americanmothers, an exploratory factor analysis (EFA) was completedto examine the underlying factor structure in this population.The EFAwas conducted in MPlus 6.2 (Muthen and Muthen)using maximum likelihood factor analysis and geomin rota-tion (a type of oblique rotation) to allow for correlationsamong the factors, obtain fit statistics for the EFA model,and account for the small amount (2 %) of missing data.Current statistical recommendations have criticized using ei-genvalues greater than 1 as the sole determinant of the numberof factors to be extracted (Fabrigar et al. 1999). More recently,employing model fit statistics, specifically root mean squareerror of approximation (RMSEA) values of ≤0.08, has beensuggested as appropriate criteria to determine the number oftotal factors (Fabrigar et al. 1999). For the current analyses, fitindices [RMSEA≤0.08, comparative fit index (CFI)≥0.95,and standardized root mean square residual (SRMR)<0.08values; Hu and Bentler 1999] and critical evaluation of thesubstantive content of the items that loaded on each factorwere used to determine the final factor solution.
Results
Preliminary analyses
Initial analyses revealed three types of problematic item-level issues. First, the 12 items that were reverse coded (e.g.,“There will be times that you feel stuck or trapped being amother”) tended to have low loadings on all of the factors,regardless of the number of factors extracted. Measurementliterature suggests that reverse-coded items may place asubstantial cognitive burden on participants (Weems et al.2003) and may be especially problematic when translatedinto Spanish (Knight et al. 2009); thus, these items mayhave been problematic for our sample given lower literacylevels. Second, two items assessing maternal expectations ofinfant appearance and health had very low variability (e.g.,“My baby will be beautiful,” M=4.92, SD=0.4; and “Mybaby will be healthy,” M=4.63, SD=0.7), as almost allmothers answered “5, very much so.” A third group of threeitems had low loadings (ranging from 0.13 to 0.20) or didnot substantively fit within any factor solution (e.g. “Youwill have enough money to provide for your baby”). Thus,17 items were eliminated, leaving a total of 17 items.
Primary analyses
Exploratory factor analyses
Two, three, and four factor models with the 17-item PESMAwere examined using the data analytic procedures describedabove. The EFA with the 17 items indicated that a three-factor solution provided a good fit to the data (CFI=0.95,RMSEA=0.08, SRMR=0.03). The two-factor solution pro-vided a worse fit to the data according to the aforementionedfit indices (CFI=0.87, RMSEA=0.11, SRMR=0.08) andwas disregarded as a viable solution. Mathematically, thefour-factor solution presented as a somewhat better fit to thedata (CFI=0.97, RMSEA=0.06, SRMR=0.03); however,the substantive content of the fourth factor was not theoret-ically cohesive. Furthermore, the content of the three-factorsolution deteriorated as items were loaded onto the fourthfactor. Therefore, the three-factor solution was selected forthe subsequent analyses and interpretations.
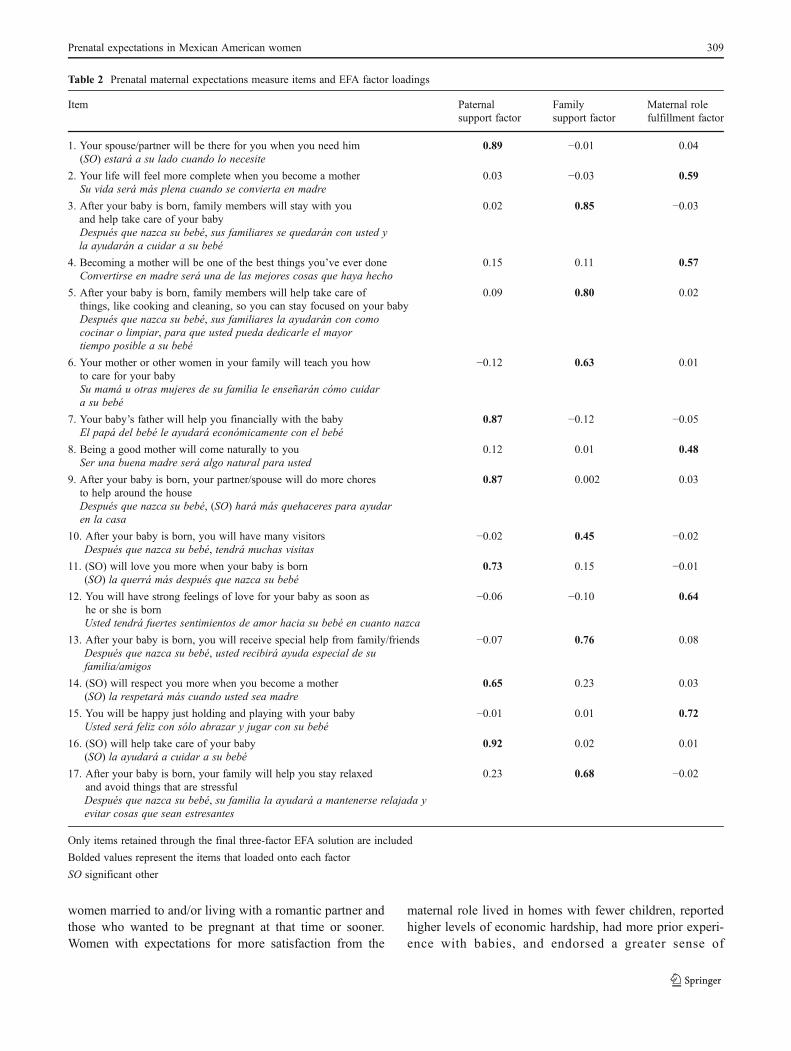
Within the three-factor solution, the first factor (termedpaternal support) consisted of six items assessing expecta-tions of partner support, with loadings ranging from 0.65 to0.92 (see Table 2). Factor 2 (termed family support)consisted of six items pertaining to anticipated family sup-port during the postpartum period and had factor loadingsranging from 0.48 to 0.72. Lastly, the third factor (termedmaternal role fulfillment) was comprised of five items thatassessed expectations about the transition to the maternalrole and satisfaction anticipated from motherhood (factorloadings ranged from 0.48 to 0.72). The paternal supportfactor correlated with family support factor (r=0.22) andwith maternal role fulfillment factor (r=0.34). The correla-tion between family support and maternal role fulfillmentfactors was r=0.26. Scale scores were formed by summingthe individual items identified by each factor in the EFA.The paternal support, family support, and maternal rolefulfillment subscales had internal reliabilities of Cronbach’salpha=0.91, 0.85, and 0.69, respectively. Cronbach’s alphafor the entire PESMA scale was 0.86.
Correlates of prenatal expectations
Following the EFA, Pearson product correlation analyseswere conducted to describe the demographic and culturalcorrelates of paternal support, family support, and maternalrole fulfillment expectations. Correlations between prenatalexpectations and measures of prenatal psychosocial func-tioning were also calculated to explore the concurrent va-lidity of the newly developed measure. Results are shown inTable 3 and described in more detail below.
Demographic characteristics Expectations of paternal sup-port and maternal role fulfillment were higher among
308 J.L. Gress-Smith et al.
women married to and/or living with a romantic partner andthose who wanted to be pregnant at that time or sooner.Women with expectations for more satisfaction from the
maternal role lived in homes with fewer children, reportedhigher levels of economic hardship, had more prior experi-ence with babies, and endorsed a greater sense of
Table 2 Prenatal maternal expectations measure items and EFA factor loadings
Item Paternalsupport factor
Familysupport factor
Maternal rolefulfillment factor
1. Your spouse/partner will be there for you when you need him 0.89 −0.01 0.04(SO) estará a su lado cuando lo necesite
2. Your life will feel more complete when you become a mother 0.03 −0.03 0.59Su vida será más plena cuando se convierta en madre
3. After your baby is born, family members will stay with youand help take care of your baby
0.02 0.85 −0.03
Después que nazca su bebé, sus familiares se quedarán con usted yla ayudarán a cuidar a su bebé
4. Becoming a mother will be one of the best things you’ve ever done 0.15 0.11 0.57Convertirse en madre será una de las mejores cosas que haya hecho
5. After your baby is born, family members will help take care ofthings, like cooking and cleaning, so you can stay focused on your baby
0.09 0.80 0.02
Después que nazca su bebé, sus familiares la ayudarán con comococinar o limpiar, para que usted pueda dedicarle el mayortiempo posible a su bebé
6. Your mother or other women in your family will teach you howto care for your baby
−0.12 0.63 0.01
Su mamá u otras mujeres de su familia le enseñarán cómo cuidara su bebé
7. Your baby’s father will help you financially with the baby 0.87 −0.12 −0.05El papá del bebé le ayudará económicamente con el bebé
8. Being a good mother will come naturally to you 0.12 0.01 0.48Ser una buena madre será algo natural para usted
9. After your baby is born, your partner/spouse will do more choresto help around the house
0.87 0.002 0.03
Después que nazca su bebé, (SO) hará más quehaceres para ayudaren la casa
10. After your baby is born, you will have many visitors −0.02 0.45 −0.02Después que nazca su bebé, tendrá muchas visitas
11. (SO) will love you more when your baby is born 0.73 0.15 −0.01(SO) la querrá más después que nazca su bebé
12. You will have strong feelings of love for your baby as soon ashe or she is born
−0.06 −0.10 0.64
Usted tendrá fuertes sentimientos de amor hacia su bebé en cuanto nazca
13. After your baby is born, you will receive special help from family/friends −0.07 0.76 0.08Después que nazca su bebé, usted recibirá ayuda especial de sufamilia/amigos
14. (SO) will respect you more when you become a mother 0.65 0.23 0.03(SO) la respetará más cuando usted sea madre
15. You will be happy just holding and playing with your baby −0.01 0.01 0.72Usted será feliz con sólo abrazar y jugar con su bebé
16. (SO) will help take care of your baby 0.92 0.02 0.01(SO) la ayudará a cuidar a su bebé
17. After your baby is born, your family will help you stay relaxedand avoid things that are stressful
0.23 0.68 −0.02
Después que nazca su bebé, su familia la ayudará a mantenerse relajada yevitar cosas que sean estresantes
Only items retained through the final three-factor EFA solution are included
Bolded values represent the items that loaded onto each factor
SO significant other
Prenatal expectations in Mexican American women 309

preparedness for motherhood. Interestingly, Mexican Amer-ican mothers who expected to feel greater fulfillment frommotherhood reported earlier initiation of prenatal care.Higher expectations of family support were associated withyounger maternal age, fewer biological children, increasedeconomic hardship, and higher maternal education.
Psychosocial characteristics All three factors of the PESMAwere negatively correlated with prenatal depressive symptoms(correlations ranged between −0.18 and −0.41) and positivelycorrelated with prenatal social support (r=0.26 to 0.52). Themagnitude of these correlations is consistent with Cohen’s(1988) definition of effect sizes ranging from small to mediumfor depressive symptoms and medium to large for socialsupport. In sum, higher levels of expectations for paternalsupport, family support, and maternal role fulfillment weresignificantly associated with fewer prenatal depressive symp-toms and higher social support.
Cultural characteristics We also examined correlationsamong the three domains of the PESMA and cultural char-acteristics, including country of origin, age of immigration
to the USA, and orientation to majority/minority culture.Women who were born in the USA had higher expec-tations of family support compared to women born inMexico. However, women born in Mexico had signifi-cantly higher expectations for paternal support thanthose born in the USA. Similarly, women who immi-grated to the USA at a younger age endorsed signifi-cantly higher levels of expected family supportcompared to women who immigrated to the USA atan older age. Age of immigration and country of originwere not significantly correlated with partner support ormaternal role fulfillment expectations. Higher expecta-tions across all three domains were positively associatedwith greater endorsement of familism values, with correlationsranging from 0.19 to 0.38, which is consistent a small tomedium effect size (Cohen 1988). Women who anticipatedgreater family support after the birth of their baby also endorseda cultural orientation characterized by higher identification withAnglo culture and lower identification with Mexican culture.However, greater identification with Mexican culture wasassociated with higher expectations for the maternal role andpaternal support.
Table 3 Correlations between prenatal expectation factors, demographics, psychosocial measures, and cultural variables (N=210)
Paternalsupport factor
Familysupport factor
Maternalrolefulfillmentfactor
Marital statusa −0.62** −0.02 −0.17*
No. of children under 18 in the home −0.14 −0.13 −0.24**
No. of other biological children 0.02 −0.25** 0.04
Preparedness for infant care 0.07 0.03 0.21**
Experience with infants 0.01 −0.06 0.16*
Economic hardship −0.11 −0.32** −0.14*
Maternal education −0.03 0.24* 0.04
Gestational weeks whenprenatal care was initiated
−0.05 −0.04 −0.18**
Pregnancy intentionsb 0.19** −0.01 0.13
Maternal age 0.05 −0.33** 0.10
Country of birthc 0.14* −0.24** −0.01
Immigration age to USA 0.08 −0.26** 0.07
Satisfaction with supportfrom biological father
0.80** 0.26** 0.22**
Depressive symptoms −0.41** −0.18** −0.22**
General social support 0.35** 0.52** 0.26**
Familism 0.19** 0.20** 0.38**
Anglo orientation −0.04 0.38** 0.05
Mexican orientation 0.15* −0.19** 0.16*
*p≤0.05; **p≤0.01a 0=married or living together; 1=not living with partnerb 0=wanted to be pregnant later or never; 1=wanted to be pregnant then or soonerc 0=born in USA; 1=born in Mexico
310 J.L. Gress-Smith et al.

Validity testing Correlational analyses also served the pur-pose of providing discriminant and concurrent validity forthe PESMA. First, we explored relations between eachsubscale of expectations and constructs with which theyshould be positively correlated. For example, we wouldexpect anticipated partner and family support to be positive-ly related to measures of current general social support. Infact, social support was positively correlated with prenatalexpectations of partner support (r=0.35) and family support(r=0.52). The respective moderate and large magnitude ofthese relations demonstrated that each subscale of thePESMA is related to general social support but is alsodistinct and contains unique information. As we wouldexpect that women who were married or in a relationship(r=−0.62) and those who were more satisfied with thecurrent levels of support from their baby’s father (r=0.80)demonstrated higher expectations for greater paternal sup-port. Prenatal expectations were also positively correlatedwith familism (r=0.19 to 0.38), a construct emphasizingstrong familial bonds and the importance of family cohe-sion. The magnitude of the correlations between expecta-tions and familism was lower than the correlations observedbetween expectations and general social support, which maybe expected given the stronger conceptual link betweenexpectations of social support and current general socialsupport.
Next, when we explored associations with constructs, wewould expect to bear a negative relation with prenatal ex-pectations. Feelings of hopelessness are a hallmark featureof depressive disorders, and as such, we would expectwomen reporting higher levels of depressive symptoms toendorse lower positive expectations for the future. Asexpected, prenatal depressive symptoms were negativelycorrelated with each of the three expectations subscales(r=−0.18 to −0.41). Women who had lower expectationsfor maternal role fulfillment initiated prenatal care later intheir pregnancies (r=−0.18). Women may be less likely toengage in positive health behaviors during pregnancy whenthey hold negative expectations for the maternal role. Fur-ther, prenatal care initiation was not significantly associatedwith expectations for paternal or family support. The ab-sence of significant relations among prenatal care and part-ner and family support may be expected, as maternal roleexpectations should bear a stronger correlation with mater-nal self-care and health.
Discussion
The current literature on prenatal expectations has focusedprimarily on middle-class, Caucasian samples, resulting in agap in our understanding and measurement of prenatal ex-pectations in high-risk, low-income minority samples. The
current study adapted an existing measure of prenatal ex-pectations for use with low-income Mexican Americanwomen, who have the highest birthrate in the USA(Martin et al. 2012). The Prenatal Maternal ExpectationsScale (Coleman et al. 1999) formed the initial basis for themeasure but was extensively modified to reflect culturallyrelevant domains of expectations and form the PrenatalExpectations Scale for Mexican Americans (PESMA).Three distinct factors emerged underlying prenatal expecta-tions in this sample of low-income Mexican Americanwomen: paternal support, family support, and maternalrole fulfillment. The correlations among the factors weremodest, suggesting that each is an important individualdomain that characterizes the content of women’s pre-natal expectations. This underlying structure of prenatalexpectations also demonstrated good concurrent validitywhen compared to measures of social support and pre-natal depression.
The current investigation offers a novel description ofantepartum Mexican American women’s perceptions of whatmotherhood will entail. Women cognitively and emotionallyprepare for motherhood during the prenatal period by evaluat-ing, appraising, and forming expectations about qualities of thepostpartum environment (Lawrence et al. 2007). Prenatal ex-pectations also represent beliefs about distinct sources of stressand fulfillment women may experience when they become amother (Lederman 1996) and have been postulated to affect awoman’s behavior and mood during the prenatal period(Lucas 2010). An understanding of relations among prenatalexpectations, emotional functioning, and healthy pregnancybehaviors may suggest important targets for interventions topromote maternal and infant health during the prenatal period.AmongMexican American women for whom elevated rates ofprenatal depression have been observed (Lara et al. 2009), suchefforts may be particularly critical.
Little is known about the individual, familial, and culturalcharacteristics associated with expectations formed aboutthis transformative life experience. Examining these person-al and contextual qualities are critical to understanding thecharacteristics of women who form higher and lower levelsof prenatal expectations. In the present study, women whohad higher expectations for maternal role fulfillment weremore likely to be married and have fewer young childrenliving in the home. Women may expect that adjusting totheir role as mothers will be more enjoyable or fulfilling ifthey do so with a partner, rather than alone. Women withhigher expectations of postpartum family support were morelikely to have higher levels of education, less subjectiveeconomic hardship, and be younger in age. Younger womenmay be more likely to live at home and expect the support oftheir nuclear and extended family following the birth of theirbaby. High existing levels of personal and socioeconomicresources in the prenatal environment may also contribute to
Prenatal expectations in Mexican American women 311

expectations for support during the postpartum period. The-se findings extend our understanding of prenatal expecta-tions in a sample focused exclusively on low-incomeMexican American women.
Prior research has observed lower levels of prenatal andpostpartum depression amongMexicanAmerican womenwhoreport higher prenatal social support (Campos et al. 2008;Martinez-Schallmoser et al. 2003; Sheng et al. 2010); however,these studies focused on received support rather than expecta-tions of future support. Measuring expectations differs fromassessing currently available resources because expectationscapture an element of cognitive appraisal, including how awoman perceives or feels about the resources in her life andtheir future availability. The emotional correlates of theseappraisals of the postpartum period are likely associated withwomen’s stress levels and mood during pregnancy(Lucas 2010). In the current study, women with higher expec-tations for postpartum partner and family support had fewerprenatal depressive symptoms. Although correlational in na-ture, these findings may provide insight into the positive orprotective effects that cognitive appraisal or rehearsal of post-partum expectations may have during the prenatal period. As afunction of self-fulfilling prophecies or pressures to ensureconfirmation of anticipated future events, prenatal expectationsfor support may shape the type and extent of support receivedfollowing the birth of a child (Hackel and Ruble 1992;Lawrence et al. 2007). As low levels of postpartum socialsupport have been identified as a risk factor in the developmentof postpartum depression among Hispanic women (Martinez-Schallmoser et al. 2003), assessing prenatal expectations ofpostpartum support may offer an early identification strategyfor women at risk for poor adjustment in the postpartumperiod.
Prenatal depressive symptoms were also lower amongwomen who endorsed higher expectations for the maternalrole. Changes in a woman’s self-concept are a significantpart of pregnancy (Smith 1999), and prior research suggeststhat positive cognitive rehearsal of becoming a mother con-tributes to psychological well-being during pregnancy(Lederman 1996; Rubin 1984). It is also possible that de-pressive symptoms contribute to more negative expectationsabout the upcoming maternal role. Women’s prior experi-ence with babies and feelings of preparedness to care for aninfant were significantly associated with expectations for amore rewarding experience in the maternal role. Educatingwomen about how to care for a new baby ameliorates thestress that infant care often brings in the early postpartumperiod (Darvill et al. 2010; Shaw et al. 2006). The currentfindings raise the possibility that such education may alsocontribute to more positive expectations that one will beable to manage and be fulfilled by the maternal role. Impor-tantly, women who had higher expectations that motherhoodwould be a fulfilling experience reported earlier initiation of
prenatal care. Models of prenatal care utilization in low-income populations have not been heavily investigated,and these results suggest that bolstering the prenatal expec-tations for maternal role may be a promising pathway toexplore.
Among Mexican American women, prevailing valuesoffer a cultural lens to interpret and understand beliefssurrounding the transition to the maternal role. We exam-ined multiple elements of acculturation and Mexican Amer-ican cultural values to broadly assess relations betweencultural factors and prenatal expectations. Familism high-lights the value of the maternal role (Castillo et al. 2010) andimportance of close familial bonds (Marin 1993) such thatwomen with these beliefs may approach the transition toparenthood with more positive expectations. Indeed, womenwith more positive expectations across all three factors ofprenatal expectations reported stronger endorsement of fam-ilism values, and those who more strongly identified withMexican culture anticipated greater fulfillment from thematernal role. Analyses also revealed a negative relationbetween Mexican cultural orientation and expectations offamily support and a positive relation between Anglo cul-tural orientation and expectations of family support in thepostpartum period. Although this finding might appearcounterintuitive, given expectations that traditional womenwould be more family-oriented, prior research has shownthat expectations of family support do not diminish withincreasing acculturation, and as a result, later generationsand more acculturated individuals may benefit from morefamily support simply because they have more family mem-bers residing in the USA (Martin et al. 2012). Identificationwith Anglo culture was also associated with earlier age ofimmigration to the USA or birth in the USA, supporting theinterpretation that the more acculturated women in the sam-ple may have a stronger and more stable network of familymembers available.
There are several limitations in the current study. First, thesmall number of items may have limited the identification ofother important domains of women’s expectations about thepostpartum period. Though empirical and theoretical supportwas used to adapt the PESMA for use with Mexican Americanwomen from an existing measure of prenatal expectations,qualitative studies and focus groups may identify additionalitems or factors. Second, the formation of expectations may berelated to other factors not assessed in the current study,including personality factors, attachment style, or lifetime his-tory of depression or other mental health issues. Third, becausesteps were taken to ensure the applicability of the domains andcontent of the PESMA to Mexican American women, it maynot be generalizable to other Latino populations. Fourth, thereliability of the maternal role fulfillment subscale appeared tobe affected by the presence of reverse-coded and low-variability items. While item elimination during exploratory
312 J.L. Gress-Smith et al.

analyses and measure development is expected, future studiesrefining the items for this subscale may be particularly impor-tant. Fifth, the single-item measure of satisfaction with currentpaternal support may have provided only limited informationabout relations between expectations and support related to thefather role. Future studies should examine relations betweenexpectations and different domains of paternal support. Finally,the PESMA requires further testing of its psychometric prop-erties with a larger sample size to enhance the support for itsuse with Mexican American women. Evidence of constructvalidity and test–retest reliability may be achieved throughadditional administrations and confirmatory factor analysesof the proposed factor structure.
Conclusion
Investigations of prenatal expectations in Mexican Ameri-can women are scarce. The few studies that have examinedthis construct have done so through qualitative interviews(Guendelman et al. 2001; Lucas 2010; Tamis-Lemonda andKahana-Kalman 2009). The current study provides a signif-icant contribution to the current literature by developing andvalidating the PESMA, a measure of prenatal expectationsin low-income Mexican American women. A culturallyrelevant assessment of expectations for the postpartum pe-riod offers important insight into how Mexican Americanwomen anticipate the positive and negative changes thataccompany new motherhood. The three domains of expec-tations assessed by the PESMA (family support, partnersupport, and maternal role fulfillment) represent a broadprenatal snapshot of women’s anticipated experiences dur-ing the postpartum period and demonstrate informative re-lations with concurrent demographic, psychosocial, andcultural factors. Culturally sensitive measurement of prena-tal expectations is an important step towards a better under-standing of the transition to motherhood among uniquepopulation of women.
Acknowledgments This research was supported by a grant R01MH083173-01A1 from NIMH (to Linda Luecken, Nancy Gonzales,and Keith Crnic). The first author of this manuscript was supported bya National Research Service Award, F31MH0953141, NIMH.
Conflict of interest The authors of this manuscript have no potentialconflicts of interests, including financial interests or gains.
References
Baor L, Soskolne V (2010) Mothers of IVF and spontaneously con-ceived twins: a comparison of prenatal maternal expectations,coping resources and maternal stress. Hum Reprod 25(6):1490–1496. doi:10.1093/humrep/deq045
Barrera M, Caples H, Tien J (2001) The psychological sense ofeconomic hardship: measurement models, validity, and cross-ethnic equivalence for urban families. Am J Community Psychol29:493–517
Boyd R, Le H-N, Somberg R (2005) Review of screening instrumentsfor postpartum depression. Arch Womens Ment Health 8:141–153. doi:10.1007/s00737-005-0096-6
Campos B, Dunkel Schetter C, Abdou C, Hobel C, Glynn L, SandmanC (2008) Familism, social support, and stress: positive implica-tions for pregnant Latinas. Cult Divers Ethn Minor Psychol14(2):155–162. doi:10.1037/1099-9809.14.2.155
Castillo L, Perez F, Castillo R, Ghosheh M (2010) Construction andinitial validation of the Marianismo beliefs scale. Couns PsycholQ 23(2):163–175. doi:10.1080/09515071003776036
Cohen J (1988) Statistical power analysis for the behavioral sciences,2nd edn. Erlbaum, New York
Coleman P, Nelson E, Sundre D (1999) The relationship betweenprenatal expectations and postnatal attitudes among first-timemothers. J Reprod Infant Psychol 17(1):28–39. doi:10.1080/02646839908404582
Cox JL, Holden JM, Sagovsky R (1987) Detection of postnatal de-pression: development of the 10-item Edinburgh postnatal depres-sion scale. Br J Psychiatry 150:782–786. doi:10.1192/bjp.150.6.782
Cuellar I, Arnold B, Maldonado R (1995) Acculturation rating scale forMexican Americans-II: a revision of the original ARSMA scale.Hisp J Behav Sci 17:275–303. doi:10.1177/07399863950173001
Darvill R, Skirton H, Farrand P (2010) Psychological factors thatimpact on women’s experiences of first-time motherhood: a qual-itative study of the transition. Midwifery 26:357–366.doi:10.1016/j.midw.2008.07.006
Delmore-Ko P, Pancer S, Hunsberger B, Pratt M (2000) Becoming aparent: the relation between prenatal expectations and postnatalexperience. J Fam Psychol 14(4):625–640. doi:10.1037/0893-3200.14.4.625
Fabrigar L, Wegener D, MacCallum R, Strahan E (1999) Evaluatingthe use of exploratory factor analysis in psychological research.Psychol Methods 4(3):272–299. doi:10.1037/1082-989X.4.3.272
Field T (2011) Prenatal depression effects on early development: areview. Infant Behav Dev 34(1):1–14. doi :10.1016/j.infbeh.2010.09.008
Flores E, Tschann JM, Dimas JM, Bachen EA, Pasch LA, de Groat CL(2008) Perceived discrimination, perceived stress, and mental andphysical health among Mexican-origin adults. Hisp J Behav Sci30(4):401–424. doi:10.1177/0739986308323056
Fox G, Bruce C, Combs-Orme T (2000) Parenting expectations andconcerns of fathers and mothers of newborn infants. Fam Relat49(2):123–131. doi:10.1111/j.1741-3729.2000.00123.x
Garcia-Esteve L, Ascaso C, Ojuel J, Navarro P (2003) Validation of theEdinburgh Postnatal Depression Scale (EPDS) in Spanishmothers. J Affect Disord 75:71–76. doi:10.1016/S0165-0327(02)00020-4
Germán M, Gonzales N, Dumka L (2009) Familism values as aprotective factor for Mexican-origin adolescents exposed to devi-ant peers. J Early Adolesc 29(1):16–42. doi:10.1177/0272431608324475
Guendelman S, Malin C, Herr-Harthorn B, Vargas P (2001) Orienta-tions to motherhood and male partner support among women inMexico and Mexican-origin women in the United States. Soc SciMed 52:1805–1813. doi:10.1016/S0277-9536(00)00296-3
Hackel L, Ruble D (1992) Changes in the marital relationship after thefirst baby is born: predicting the impact of expectancy disconfir-mation. J Pers Soc Psychol 62(6):944–957. doi:10.1037/0022-3514.62.6.944
Hamilton B, Martin J, Ventura S, Sutton P, Mecacker F (2005) Births:preliminary data for 2004. National Vital Statistics Reports
Prenatal expectations in Mexican American women 313

54(8):1–20. Retrieved November 2, 2012 from http://www.cdc.gov/nchs/data/nvsr/nvsr54/nvsr54_08.pdf
Hamilton ER, Hummer RA, You XH, Padilla YC (2006) Healthinsurance and health care utilization of U.S. born Mexican Amer-ican children. Soc Sci Quart 87(5):1280–1294. doi:10.1111/j.1540-6237.2006.00428.x
Hu L, Bentler PM (1999) Cutoff criteria for fit indexes in covariancestructure analysis: conventional criteria versus new alternatives.S t r u c t E q u Mo d e l i n g 6 ( 1 ) : 1 – 5 5 . d o i : 1 0 . 1 0 8 0 /10705519909540118
Kiang L, Moreno A, Robinson J (2004) Maternal preconceptions aboutparenting predict child temperament, maternal sensitivity, andchildren’s empathy. Dev Psychol 40(6):1081–1092. doi:10.1037/0012-1649.40.6.1081
Knight G, Gonzales N, Saenz D, Bonds D, Germán M, Deardorff J,Roosa M, Updegraff K (2009) The Mexican American culturalvalues scales for adolescents and adults. J Early Adolesc30(3):444–481. doi:10.1177/0272431609338178
Lara M, Le H-N, Letechipia G, Hochhausen L (2009) Prenatal depres-sion in Latinas in the U.S. and Mexico. Matern Child Health J13:567–576. doi:10.1007/s10995-008-0379-4
Lawrence E, Nylen K, Cobb R (2007) Prenatal expectations andmarital satisfaction over the transition to parenthood. J FamPsychol 21(2):155–164. doi:10.1037/0893-3200.21.2.155
Lederman R (1996) Psychosocial adaptation in pregnancy: Assessmentof seven dimensions of maternal development (2nd edn). SpringerPub Co, New York
Lucas F (2010) Pregnant women of Mexican descent: constructions ofmotherhood. Soc Work Health Care 49(10):946–962.doi:10.1080/00981389.2010.518875
Marin G (1993) Influence of acculturation on familism and self-identification among Hispanics. In: Bernal ME, Knight GP (eds)Ethnic identity: Formation and transmission among Hispanics andother minorities. SUNY Press, New York, pp 181–196
Martin JA, Hamilton BE, Ventura SJ, Osterman MJK, Wilson EC,Matthews TJ (2012) Births: final data for 2010. National VitalStatistics Reports 54(8):1–20. Retrieved April 8, 2013 from http://www.cdc.gov/nchs/data/nvsr/nvsr61/nvsr61_01.pdf
Martinez-Schallmoser L, Telleen S, MacMullen N (2003) The effect ofsocial support and acculturation on postpartum depression inMexican-American women. J Transcult Nurs 14(4):329–333.doi:10.1177/1043659603257162
McHale J, Kazali C, Rotman T, Talbot J, Carleton M, Lieberson R (2004)The transition to coparenthood: parents’ prebirth expectations andearly coparental adjustment at 3 months postpartum. DevPsychopathol 16:711–713. doi:10.1017/S0954579404004742
Page R (2004) Positive pregnancy outcomes in Mexican immigrants:what can we learn? J Obst Gyn Neo 33(6):783–790. doi:10.1177/0884217504270595
Pancer S, Pratt M, Hunsberger B, Gallant M (2000) Thinking ahead:complexity of expectations and the transition to parenthood. JPers 68(2):253–280. doi:10.1111/1467-6494.00097
Rafaelli M, Ontai L (2004) Gender socialization in Latino/a families:results from two retrospective studies. Sex Roles 50:287–299.doi:10.1023/B:SERS.0000018886.58945.06
Ramierez RR, de la Cruz GP (2002) The Hispanic population in theUnited States: March 2002. Current Population Reports (pp. 20–545). US Census Bureau, Washington DC
Rubin R (1984) Maternal identity and maternal experience. Springer,New York
Sagrestano L, Feldman P, Rini C, Woo G, Dunkel-Schetter C(1999) Ethnicity and social support during pregnancy. Am JCommuni ty Psycho l 27(6 ) :869–898 . do i :10 .1023 /A:1022266726892
Shaw E, Levitt C, Wong S, Kaczorowski J, The McMaster UniversityPostpartum Research Group (2006) Systematic review of theliterature on postpartum care: effectiveness of postpartum supportto improve maternal parenting, mental health, quality of life, andphysical health. Birth 33:210–220. doi:10.1111/j.1523-536X.2006.00106.x
Sheng X, Le H-N, Perry D (2010) Perceived satisfaction with socialsupport and depressive symptoms in perinatal Latinas. J TranscultNurs 21:35–44. doi:10.1177/1043659609348619
Sherbourne CD, Stewart AL (1991) The MOS social support survey. SocSci Med 32(6):705–714. doi:10.1016/0277-9536(91)90150-B
Smith J (1999) Identity development during the transition tomotherhood: an interpretative phenomenological analysis. JReprod Infant Psychol 17(3):281–299. doi:10.1080/02646839908404595
Tamis-Lemonda C, Kahana-Kalman R (2009) Mothers’ views at thetransition to a new baby: variation across ethnic groups. Parent-Sci Pract 9:36–55. doi:10.1080/15295190802656745
U.S. Census Bureau (2011) The Hispanic population: 2010. RetrievedNovember 2, 2012. http://www.census.gov/prod/cen2010/briefs/c2010br-04.pdf
Weems G, Onwuegbuzie A, Lustig D (2003) Profiles of respondentswho respond inconsistently to positively- and negatively-wordeditems on rating scales. Eval Res Educ 17(1):45–60. doi:10.1080/14664200308668290
Wilson E (1998) Acculturation and changes in the likelihood of preg-nancy and feelings about pregnancy among women of Mexicanorigin. Women Health 47(1):45–64. doi:10.1300/J013v47n01_03
314 J.L. Gress-Smith et al.
Recommended

















