
Predictive Analytics: It’s the Intervention That Matters
P L A N T E M O R A N H E A L T H C A R E E X E C U T I V E S U M M I T June 4-5, 2014

What Motivates Human Beings?
Like it or not, fast or slow, your company now adapts to change, at the speed of software.
The decisions you make as executives and leaders about the software that your company uses to run its operations will determine your
company’s long long term success or failure. It’s not just facilities, people, and products anymore.

The Agenda
Alignment Human, societal, and organizational motives with
software strategies General overview of predictive analytics Nuclear delivery, counter-terrorism, and
healthcare delivery The odd parallels
Predictive analytics in healthcare When does it work and when doesn’t it? How much should we expect from it and when? What about Long Term Care?

4
Before Healthcare:An Oddly Relevant Career Path
US Air Force CIO• Nuclear warfare operations
TRW Credit risk scoring, nuclear ballistic missile
maintenance and engineering
• NSA• Nuclear Command & Control Counter Threat
Program
• Joint Chiefs of Staff• Strategic Execution Decision Aid

5
Key Messages & Themes
1. Predictions without interventions are useless-- and potentially worse than useless And those interventions better align with your economic model
2. Some of the most valuable predictions don’t need a computer algorithm Nurses and physicians can tell you We already know what the interventions should be
3. Missing data = Poor predictions4. When it comes to analytics, there is lowering
hanging fruit than predictive analytics Target wasteful healthcare, first

Alignment of MotivesHuman, Societal, Corporate, and Software
6

What Motivates Human Beings?
Mastery: The opportunity to master a skill and be recognized for it
Autonomy: An environment in which people are given the tools and support to work under their own authority
Purpose: Living and working for something larger than themselves
Economics: Enough material wealth to at least live safely and comfortably, if not more
With influence from Daniel Pink

Homo Economicus vs. Homo Reciprocans?
Motivated by self-interest or motivated by cooperation?
“…the individual [and company] seeks to attain very specific and predetermined goals to the greatest extent, with the least possible cost.”
“When times are tight, good will takes flight.”
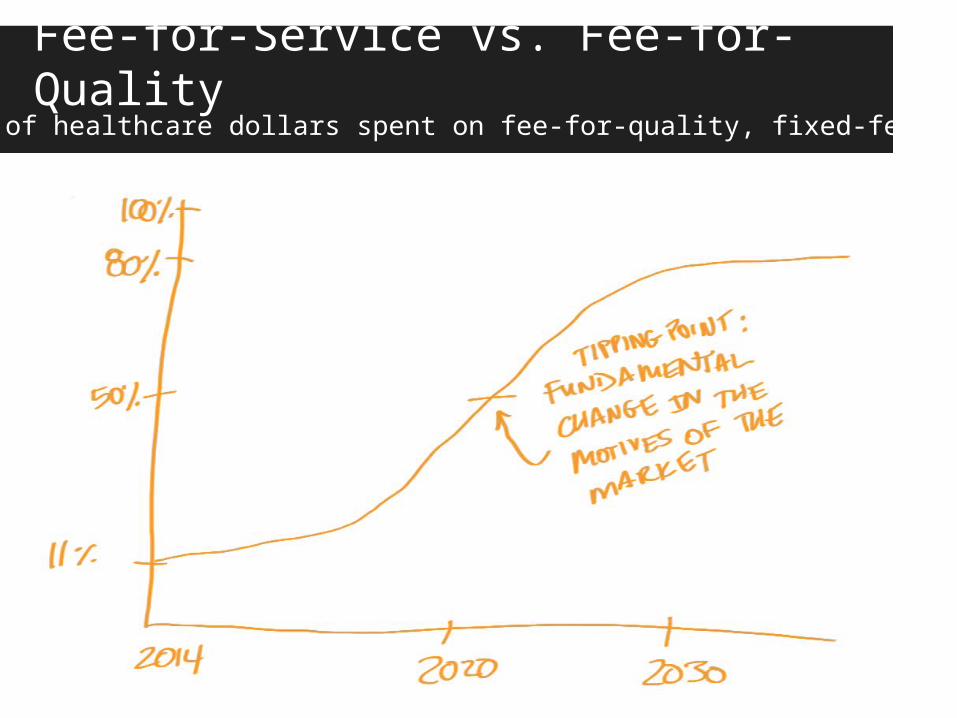
Fee-for-Service vs. Fee-for-QualityPercentage of healthcare dollars spent on fee-for-quality, fixed-fee contracting

General Concepts of Predictive Analytics
10

11
Challenge of Predicting Anything Human

The Basic Process of Predictive Analytics

13
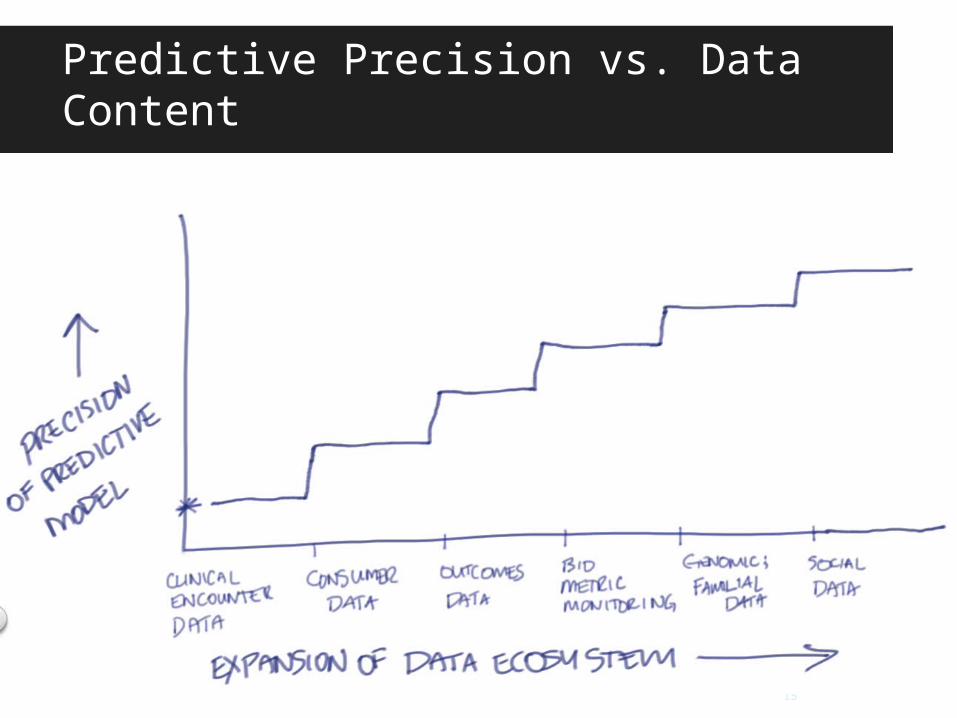
Sampling Rate vs. Predictability
The sampling rate and volume of data in an experiment is directly proportional to the
predictability of the next experiment

14
The Human Data Ecosystem
15
Predictive Precision vs. Data Content

16
Our Healthcare Sampling Rate

17
We Are Not “Big Data” in Healthcare, Yet

The Odd Parallels
Nuclear Weapons Delivery, Terrorism, and Healthcare Delivery
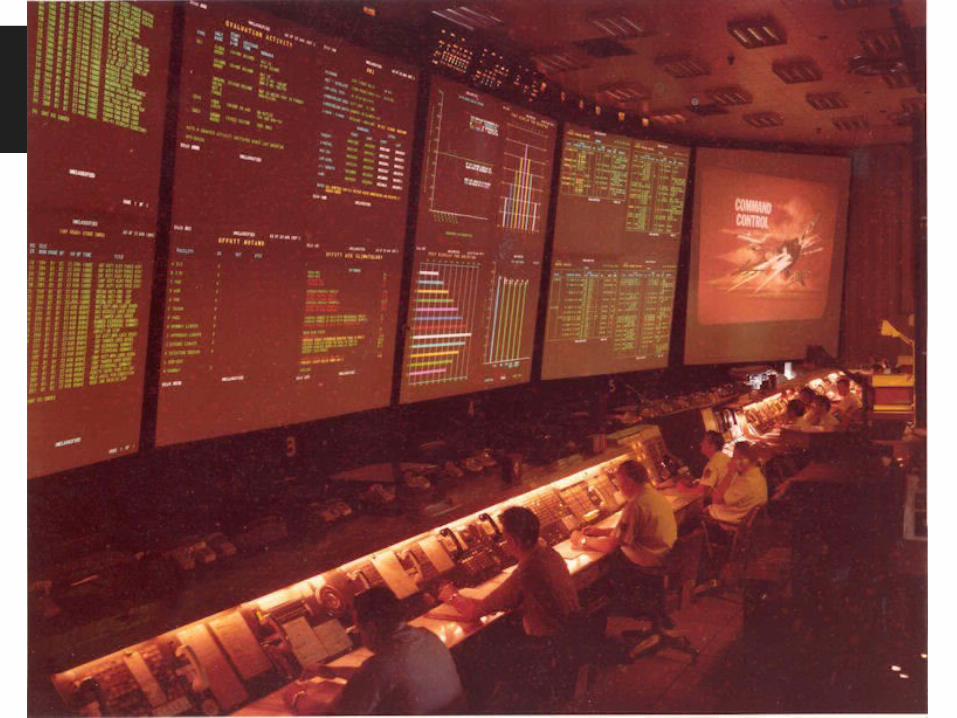


Where And How Can A Computer Help?Reduce variability in decision making & improve outcomes
22
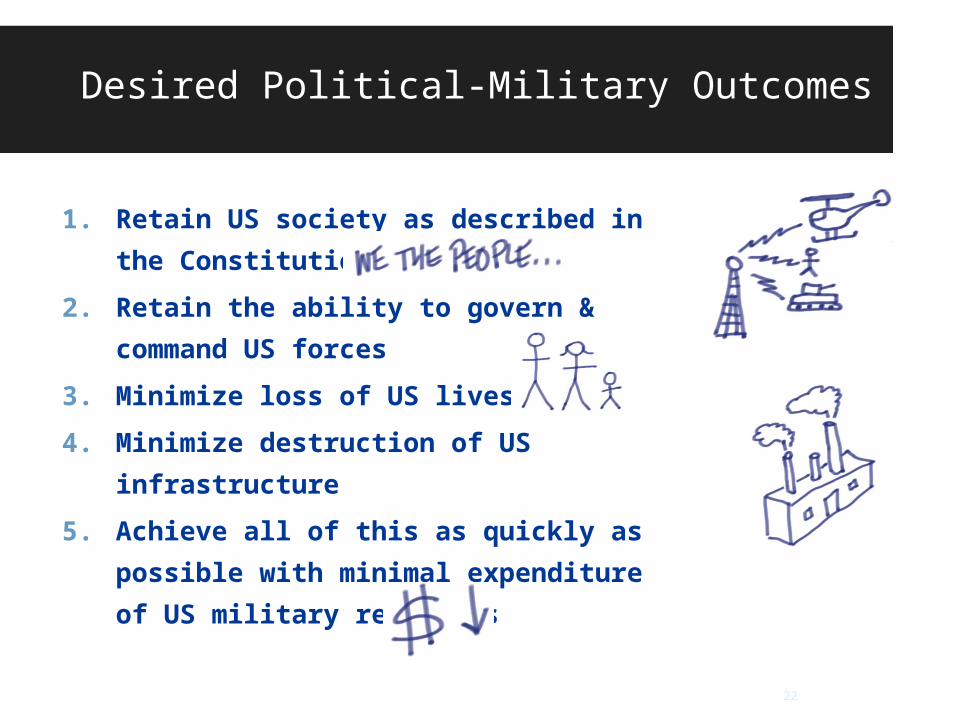
Desired Political-Military Outcomes
1. Retain US society as described in the Constitution
2. Retain the ability to govern & command US forces
3. Minimize loss of US lives4. Minimize destruction of US infrastructure
5. Achieve all of this as quickly as possible with minimal expenditure of US military resources

Can We Learn From Nuclear Warfare Decision Making?
“Clinical” observations• Satellites and radar indicate an enemy
launch Predictive “diagnosis”
• Are we under attack or not? Decision making timeframe
• <4 minutes to first impact when enemy subs launch from the east coast of the US
“Treatment” & intervention• Launch on warning or not?

24
Sortie Turnaround TimesThe Goal: Predictable, fast turnaround of aircraft to a successful battle

25
Patient Fight Path ProfilerThe Goal: Predictable, fast turnaround of patients to a good life

Healthcare As a Battle Field…??The Order of Battle and the Order of Care
Demand forecasting: What do we need and when?

27
NSA, Terrorists, and PatientsThe Odd Parallels of Terrorist Registries and Patient Registries
27

28
Predicting Terrorist Risk
Risk = P(A) × P(S|A) × C• Probability of Attack• Probability of Success if Attack occurs• Consequences of Attack (dollars, lives, national psyche,
etc.)
• What are the costs of intervention and mitigation?
• Do they significantly outweigh the Risk?

29
Predicting Patient Risk

Predictive Analytics in Healthcare
30

*Apologies for non-attribution. This diagram was taken from a text book many years ago and the specific reference has been lost.
COLLECTIVE CONSUMPTION COLLECTIVE CONSUMPTIONNATURAL PROGRESSION OF DISEASE PERSONAL CONSUMPTION
LOW RISK
AT RISK
EARLY SIGNS AND SYMPTOMS
DISEASE
DISABILITY (BODY STRUCTURE
AND FUNCTION)
CHRONIC CONDITION AND FUNCTIONAL
DECLINE
DEPENDENCY FOR SELF CARE
DEATH
GOVERNANCE AND HEALTH
SYSTEM ADMINISTRATION
COLLECTIVE PREVENTION: Epidemiologic
Surveillance and Risk and Disease Control Program
Management
CURE, TREATMENT, REHABILITATION
MAINTENANCE, LTC, PALLIATIVE CARE
PERSONAL PREVENTION:
Information & Counseling, Immunization, Early Case
Detection, Health Condition Monitoring
The Healthcare Ecosystem*
32
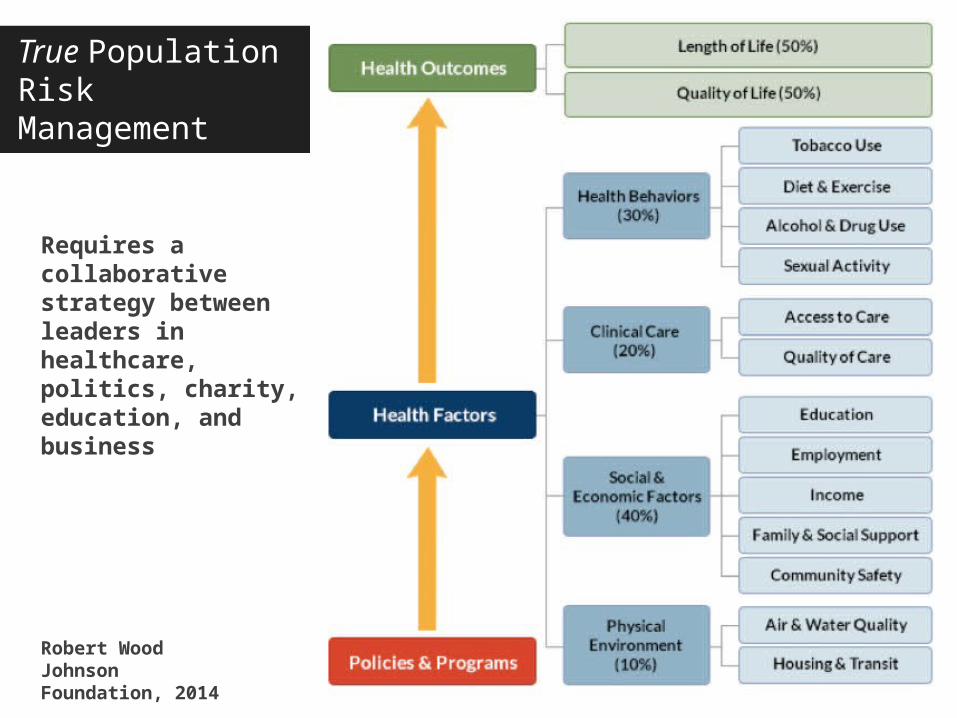
True Population RiskManagement
Robert Wood Johnson Foundation, 2014
Requires a collaborative strategy between leaders in healthcare, politics, charity, education, and business

Healthcare Analytics Adoption Model
Level 8 Cost per Unit of Health Payment & Prescriptive Analytics
Contracting for & managing health. Tailoring patient care based on population outcomes.
Level 7 Cost per Capita Payment & Predictive Analytics
Diagnosis-based financial reimbursement & managing risk proactively
Level 6 Cost per Case Payment& The Triple Aim
Procedure-based financial risk and applying “closed loop” analytics at the point of care
Level 5 Clinical Effectiveness & Accountable Care Measuring & managing evidence based care
Level 4 Automated External Reporting Efficient, consistent production & agility
Level 3 Automated Internal Reporting Efficient, consistent production
Level 2 Standardized Vocabulary & Patient Registries Relating and organizing the core data
Level 1 Integrated, Enterprise Data Warehouse Foundation of data and technology
Level 0 Fragmented Point Solutions Inefficient, inconsistent versions of the truth
What Are Trying To Predict and Why?
In the current economic model Those patients and situations that maximize our revenue
In the future economic model Those patients and situations that maximize our margin
Healthcare predictive analytics vendors are, for the most part, selling concepts that are suited for the latter, not the reality of the former

35
What Are We Trying to Predict? Why?
Common applications being marketed today Identifying preventable readmissions Risk management of decubitus ulcers LOS predictions in hospital and ICU Cost per patient per inpatient stay Likelihood of inpatient mortality Likelihood of ICU admission Appropriateness of C-section Emerging: Genomic phenotyping

Example Variables: Readmission Drivers
Newborn delivery Multiple prior admissions High creatinine High ammonia High HBA1C Low Oxygen Sats Age Admitting physician is
pulmonologist or infectious diseases
Prior admission for CHF Prior traumatic stupor & coma Prior nutritional disorders Diabetic drugs
Swati Abbott
Weighted Predictive
Model
Now what?
Risk of Readmission
36

37
Most Common Causes for Readmission
Robert Wood Johnson Foundation, Feb 2013
1. Patients have no family or other caregiver at home2. Patients did not receive accurate discharge instructions,
including medications3. Patients did not understand discharge instructions4. Patients discharged too soon5. Patients referred to outpatient physicians and clinics not
affiliated with the hospital

38
Forecasting: Process Model Structural Model: Bill of Resources
Patient Seen inEmergency Dept
Admit Patient:Presumptive
Diagnosis:Pneumonia
DischargeMonitor
CareDelivery
StandardOrder Sets
Equipment
LaborMaterials
Facilities
Nursing Orders:
Respiratory Therapy:
Medication Orders:
ResourceDemand
Day 1 Day 2 Day 3 Day 4 Day 5
Edgewater Consulting
39
Predictive Analytics: Socioeconomic Data Matters In Healthcare
Not all patients can participate in a protocol At Northwestern, we found that 30% of patients
fell into one or more of these categories Cognitive inability Economic inability Physical inability Geographic inability Religious beliefs Contraindications to the protocol Voluntarily non-compliant

40
Accounting For These Patients
30% of your patients will have to be treated and/or reached in a unique way
• Your predictive algorithms must be adjusted these attributes, especially for readmission
• These patients are a unique numerator in the overall denominator of patients under accountable care
• You need a data collection & governance strategy for these patient attributes
• You need a different interventional strategy for each of the 7 categories
• Your physician compensation model must be adjusted for these patient types

How Do You Get Started?
41

Start Within Your Scope of InfluenceWe are still learning how to manage outpatient populations
42



Where Do We Start, Clinically?
We see consistent opportunities, across the industry, in the following areas:
• CAUTI
• CLABSI
• Pregnancy management, elective induction
• Discharge medications adherence for MI/CHF
• Prophylactic pre-surgical antibiotics
• Materials management, supply chain
• Glucose management in the ICU
• Knee and hip replacement
• Gastroenterology patient management
• Spine surgery patient management
• Heart failure and ischemic patient management
47

What About Long Term Care?
48

The State of Long Term Care
12 million: The number of Americans expected to need long-term care in 2020.
40%: The percentage of the older population with long-term care needs who are poor or near-poor (income below 150% of the federal poverty level).
78%: Percentage of the elderly in need of long-term care who receive that care from family members and friends.
2.44 years: Average length of stay for current nursing-home residents
Morningstar, 2012
The Pending Tsunami

50
Economics of Long Term Care
Kaiser Family Foundation

State of Healthcare IT in LTC
HIT is used primarily for state or federal payment and certification requirements.
There is minimal use of clinical HIT applications. HIT systems are not integrated. HIT systems are underused.
California Health Care Foundation
No Data, No Predictions

52
Summary
1. Alignment of human, societal, company motives with software strategies is CRITICAL
2. Predictions without interventions are useless3. Some of the most valuable predictions don’t need a
computer algorithm We already know what the interventions should be
4. Missing data = Poor predictions5. When it comes to analytics, there is lowering
hanging fruit Target wasteful variability, first Deming: Where there is variability, there is opportunity

53
Many Thanks…!
• Contact information• [email protected]• @drsanders• www.linkedin.com/in/dalersanders

54
Group Discussion
1. What would you like to predict in today’s economic model and why?
2. What would you like to predict in tomorrow’s economic model and why?
3. What data do you need to support precise predictive analytics?
4. What types of new intervention strategies do you need to complement these predictive models?
What about Long Term Care?
Recommended

















