The Temporal Bone
Ch. Venkateswararao MDS P.G 1st yr

The temporal bones are situated at the sides and base of the skull. Each consists of five parts, viz., the squama, the petrous, mastoid, and tympanic parts, and the styloid process
Articulations.—The temporal articulates with five bones: occipital, parietal, sphenoid, mandible and zygomatic.
Styloid processMastoid process
External acousticmeatus
Zygomaticprocess (arch)
Temporal bone
Occipital
Parietal bone
Spheoidbone Frontal bone
Nasal boneZygomatic
Mandible
Maxilla

Squamous part2 surfaces: external (temporal),internal (cerebral)
2 borders : superior and antero inferior .
1 process: zygomatic process
1 fossa: mandibular fossa

The squama forms the anterior and upper part of the bone, and is scale-like, thin, and translucent.Surfaces.—Its outer surface :: Is smooth and convex; Presents:: 1)Groove for middle temporal vessels:: on its hinder part is a vertical groove for the middle temporal artery. above the opening of external auditory meatus 2)supramastoid crest :: runs backward and upward across its posterior part; it serves for the attachment of the temporal fascia, and limits the origin of the Temporalis muscle.. Projecting from the lower part of the squama is a long, arched process, the zygomatic process.

3)Squamo-mastoid suture::
Lies about 1.25 cm below and behind the supramastoid crest,indicates line of fusion b/w squamous and mastoid parts
4)Suprameatal triangle: a small triangular depression b/w the anterior end of supramastoid crest, and the postero- superior sector of external auditory meatus ..Imp: land mark for mastoid antrum ,in adults lies 1.25cm deep to it 5)Suprameatal spine :: small bony projection at anterior part of suprameatal triangle.The posterior end is connected to the squama by two roots, the anterior and posterior roots. The anterior root, continuous with the lower border, is short but broad and strong; it is directed medial ward and ends in a rounded eminence, the articular tubercle (eminentia articularis).
This tubercle forms the front boundary of the mandibular fossa, and in the fresh state is covered with cartilage

6)Zygomatic process:: A long arched process projecting horizontally, laterally and then directed anteriorly from the lower and anterior part of temporal surface; articulates in front with the temporal process of zygomatic bone .
Possesses:: 2 parts , anterior , posterior
a) Anterior part : thin and flat:
has 2 surfaces: lateral :convex & subcutaneous
medial: convex & gives origin to
masseter muscle from its
lower part.
2 borders:: upper: gives attachement to
temporal fascia.
lower: arched; gives origin to
masseter muscle.

2 ends:: anterior : serrated ; articulates with temporal process of zygomatic bone..
Posterior : continous with posterior part of zygomatic process…
b)Posterior part :: thick and triangular ..
Presents:
3 borders; base: united with squamous part.
anterior: constitues anterior root of process.
posterior: constitue posterior root of process .
.

2 surfaces: superior : concave and continous with temporal surface.
inferior: convex and mostly occupied by inferior surface of the anterior root which forms a thickened bar of bone in front of mandibular fossa .
The thickened bar of bone is known as articular tubercle. This articulates with the articular disc of TMJ..
7) Squamosal foramen :: very rarely present, just above the anterior root of zygomatic process
Imp: transmits petrosquamous sinus
11) Mandibular fossa: formed by squamous part & partly by tympanic part …

Mandibular fossa :: possesses 2 parts :
Anterior (articular): formed by squamous part, smooth, oval, convex, articulates with articular disc of TMJ..
Posterior : ( non articular) : formed by tympanic part ,contains a portion of parotid gland .
Presents::
Post glenoid tubercle: 3rd root of zygomatic process, seperates articular part with non articular part .
Squamo-tympanic fissure :.lies between auricular part of mandibular fossa and tympanic part of bone,
a) Petrotympanic fissure:: b/w tegmen tympani and tympanic part, transmits anterior tympanic branch of maxillary artery to middle ear, chordatympani nerve,..
b) Petro squamous fissure:: b/w tegmen tympani and squamous part, doesnot transmit any structure..

1. Impressions:: corresponding to convolutions of temporal lobe of cerebral hemisphere which lies in relation with it but separated from it by meninges..
2. Grooves: for middle meningeal vessels..
3.Petro squamosal suture: present inferiorly, where cerebral surface of squamous unites with petrous part .
4. Petro squamosal sulcus : present close to the site of union of cerebral surface of squamous part with petrous part; it lodges petro-squamosal sinus..
BORDERS:: Superior & antero inferior
Superior border unites with the inferior border of parietal bone, forms squamosal suture.
Antero inferior border articulates with the greater wing of sphenoid…
Internal surface::

Mastoid Portion (pars mastoidea).—The mastoid portion forms the posterior part of the boneThicker then squamous part.
Presents:
2 surfaces: external (lateral), internal (medial or cerebral);
2 borders: superior & posterior.
1 process: mastoid process
Mastoid process: conical projection from antero inferior part of external surface ; larger in males,
Presents::
External surface: continous with external part of main part;
Mastoid notch: lies in medial aspect of process,
Occipital groove:shallow groove ,lies below the notch
Mastoid foramen: lies close to the posterior border

Transmits: emissiray vein from sigmoid sinus ,small branch of occipital artery
Internal surface:: concave , forms part of posterior cranial fossa.
Sigmoid sulcus:: deep curved groove lodges sigmoid sinus;
Borders:: superior: short thick serrated, forms a notch with superior border of squamous part; articulates with postero inferior part of parietal bone( mastoid angle).
Posterior border: thick & serrated ,articulates with inferior border of squamous part of occipital bone..

Mastoid air cells:: A number of irregular air spaces are present in mastoid part which can be seen in section.
larger air space is known as Mastoid or Tympanic antrum; mastoid air cells are inter communicating and they also communicate with middle ear cavity ( tympanic cavity)

Petrous Portion (pars petrosa [pyramis]).—The petrous portion or pyramid is pyramidal and is wedged in at the base of the skull between the sphenoid and occipital. contains organ of hearing.
Parts::
Base: fused with squamous and mastoid parts.
Apex: lies b/w greater wing of sphenoid and basillar part of occipital ,perieced by anterior orrifice of carotid canal, forms postero lateral boundary of foramen lacerum.
3. surfaces: anterior, posterior, inferior.
3. borders ; anterior, superior , posterior.
Anterior surface: continues with cerebral surface of squamous part, forms floor of middle cranial fossa

Parts:1. Impressions for sulci and gyri of
temporal lobe of cerebral hemisphere.
2. Trigeminal impression: depressed area just behind the apex; lodges trigeminal ganglion.
3. second hollow behind the trigeminal impression but seperated from it by an irregular ridge; forms roof of internal auditory meatus & covers cochlea
4. Arcuate eminence : elevation behind the second hollow, caused by superior semicircular canal of internal ear ;

5. Tegmen tympani ::thin plate of bone lying between the squamous part laterally & arcuate eminence & the two hollows medially
Forms the roof of mastoid antrum (tympanic), tympanic cavity(middle ear) & canal for tensor tympani;
Lateral part meets with the squamous part of petro-squamosal suture & turns down in front to form the lateral canal for tensor tympani, bony part of auditory tube..(pharyngo-tympanic or eustachian tube or acoustic;
Presents:: hiatus for greater petrosal nerve, hiatus for lesser petrosal nerve

Posterior surface:: continues with cerebral surface of mastoid part, forma anterior part of posterior cranial fossa
Presents:
1. orifice of internal auditory meatus(acousti.)
Gives entrance to motor root of facial nerve.
Entrance to labyrinthine artery
Exit to sensory root of facial nerve
Exit to vestibulo- cochlear nerve
Exit to labyrinthine vein.Diagram of relationship of nerves in the internal acoustic meatus.VII = facial nerveNI = nervus intermediusVIIIc = cochlear nerveVIIIvs = superior division of vestibular nerveVIIIvi = inferior division of vestibular nerve

2. Opening of aqueduct of vestibule :small slit, behind the opening of vestibule ,contains saccus, ducts endolymphatics
3.Subarcuate fossa”:: irregular depression above & b/w two openings, lodges a process of dura mater..
3.Inferior surface:: forms part of inferior surface of base of skull..
Presents::
1.A quadrilateral rough area near the apex
gives attachement to cartilaginous part of auditory tube.
Its lower part articulates with basillar part of occipital bone.
2. External or lower opening of carotid canal ::
Transmits; internal carotid artery, with plexus of sympathetic nerves, internal carotid plexus of veins.

3.Jugular fossa:: depression behind the carotid canal.,lodges superior bulb of IJV
4. A Triangular depression lodges the glossopharyngeal nerve..
5. Opening of cochlear canaliculus:: present at apex of triangular depression,leads to cochlear canaliculus, lodges aqueduct of cochlea,prolongation of duramater,
6. Opening of tympanic canaliculus: seperates the opening of carotid canal from jugular fossa.
7.Opening of mastoid canaliculus: present at lateral part of jugular fossa, transmits auricular branch of vagus
Jugular surface:: articulates with jugular process of occipital bone

Borders::
1.Superior border: longest & grooved, lodges superior petrosal sinus, gives attachment to tentorium cerebelli,
2. Posterior border: smaller then superior border, divides in to medial and lateral ..
Medial: articulates with lateral border of basilar part of occipital bone, and forms a groove for inferior petrosal sinus..
Lateral : forms the jugular foramen, transmits 9,1o, cranial nerves, and inferior petrosal sinus & sigmoid sinus.
3. Anterior border: divides in to lateral and medial border.
Lateral: joins with squamous part at petro squamosal suture.
Medial articulates with greater wing of sphenoid..

Lies between squamous & mastoid parts
In front it Joins with squamous part to form squamotympanic fissure.
Behind it joins with mastoid part to form tympano mastoid fissure through which auricular branch of vagus nerve comes out..
Medially fused with petrous part possess:
2. Surfaces , anterior and posterior
3.borders: lateral,upper,lower.
Anterior surface: concave, quadrilateral, forms non articular part of mandibular fossa related to a portion of parotid gland.
Tympanic part

Posterior surface: forms the anterior wall, floor,& lower part of posterior wall of bony part of external auditory meatus..
Presents: tympanic sulcus, a sulcus at the medial end, gives attachement to margin of tympanic membrane..
BORDERS:
1.Lateral border: forms greater part of circumference of lateral end of bony part of external auditory meatus
Gives attachment to cartilaginous part of external auditory meatus.
2.Upper border: lateral part fused with post glenoid tubercle,
3. Lower border: extends opening of carotid canal to styloid process sharp and gives attachment to cervical fascia..

.
The external acoustic meatus is nearly 2 cm. long and is directed inward and slightly forward: at the same time it forms a slight curve, so that the floor of the canal is convex upward.
In sagittal section it presents an oval or elliptical shape with the long axis directed downward and slightly backward.
Its anterior wall and floor and the lower part of its posterior wall are formed by the tympanic part;
the roof and upper part of the posterior wall by the squama. Its inner end is closed, in the recent state, by the tympanic membrane;
the upper limit of its outer orifice is formed by the posterior root of the zygomatic process, immediately below which there is sometimes seen a small spine, the suprameatal spine, situated at the upper and posterior part of the orifice

The styloid process is a slender pointed piece of bone just below the ear. It projects down and forward from the inferior surface of the temporal bone, and serves as an anchor point for several muscles associated with the tongue and larynx.
Its proximal part (tympanohyal) is ensheathed by the vaginal process of the tympanic portion.
Its distal part (stylohyal)
The stylohyoid ligament extends from the apex of the process to the lesser cornu of the hyoid bone, and in some instances is partially, in others completely, ossified.
Development
The styloid process arises from endochondral ossification of the cartilage from the second branchial arch.
Styloid process

It is situated about 3 cm. behind, and a little above the level of the zygomatic process of the temporal bone.It marks the junction between four bones:the parietal bonethe squamous part of temporal bonethe greater wing of sphenoid bonethe frontal bone
Clinical significance
The pterion is known as the weakest part of the skull.In the clinical setting, the pterion is relevant because the anterior division of the middle meningeal artery runs beneath it, on the inner side of the skull, which is quite thin at this point. The combination of both a vital artery in this area and the relatively thin bone structure has lent itself to the name "God's little joke" by some physicians.[
A blow to the pterion (e.g., in boxing) may rupture the artery causing an epidural haematoma. The pterion may also be fractured indirectly. Blows to the top or back of the head may not cause fracture at the site of impact, but may place sufficient force on the skull that its weakest part, the pterion, will fracture

PTERION: A SITE FOR NEUROSURGICAL APPROACH
Chandana Bhargavi, Vasudha Saralaya, Vasudha Saralaya, Kishan K, Kishan K
Vol 2, No 12 (2011)
It is commonly used neurosurgical landmark. The anatomic location of the pterion is important in surgical interventions following surgical approaches to the anterior and middle cranial fossae, following extradural hemorrhage as well as tumors involving inferior aspects of the frontal lobe, such as olfactory meningioma, used in operations on the Broca's motor speech area and in repairing aneurysms of the middle cerebral artery as well as those of the upper basilar complex and also the anatomical varieties of the pterion, is of interest mainly to anthropologists and forensic pathologists, for assessing the location of the pterion in incomplete archeological remains or forensic materials

Developmentally -4 parts
Squamous ::develops as a dermal bone to protect the brain..(membrane)
Petro mastoid:: develops as a cartilaginous capsule (protective capsule) around the membranous labyrinth of internal ear…
Tympanic::develops in membrane as a ring of bone in connection with external auditory meatus to conduct sound waves in air medium
Styloid process::develops as a skeletal detivative of 2nd branchial arch.

Ossification.—The temporal bone is ossified from eight centers, exclusive of those for the internal ear and the tympanic ossicles, viz., one for the squama including the zygomatic process, one for the tympanic part, four for the petrous and mastoid parts, and
two for the styloid process. Just before the close of fetal life the temporal bone consists of three principal parts: 1.The squama is ossified in membrane from a single nucleus, which appears near the root of the zygomatic process about the second month

2. The petro mastoid part is developed from four centers, which make their appearance in the cartilaginous ear capsule about the fifth or sixth month.
One (proötic) appears in the neighborhood of the eminentia arcuata, it forms part of the cochlea, vestibule, superior semicircular canal, and medial wall of the tympanic cavity.
A second (opisthotic) appears at the medial wall of the tympanic cavity and surrounds the fenestra cochleæ ; it forms the floor of the tympanic cavity and vestibule, surrounds the carotid canal.
A third (pterotic) roofs in the tympanic cavity and antrum;
while the fourth (epiotic) appears near the posterior semicircular canal and extends to form the mastoid process (Vrolik)

Membranous ossification : squamous, tympanic parts
Cartilaginous ossification : petromastoid , styloid process
For squamous, tympanic parts
(1) 1 center : 7 th or 8 th week in the region of root of zygomatic process,
.
At birth tympanic part is represented by incomplete ring
Tympanic part unites with squamous part shortly before birth.

(2) 1 centre: 12 th week, besides tympanic part , it also forms external auditory meatus.
For…(b) petromastoid , styloid process
(1) several centres as many as 14
20 th week, appears in cartilaginous otic capsule
Small centres fuse soon, whole otic capsule is ossified almost completely by end of 24 th week of intra uterine life.
Petro mastoid part fuses with squamous part amd tympanohyal part of styloid process during 1st year.
(2) Develops from cranial end of cartilage of 2nd brachial arch by 2 centres.

1 for proximal part: ( tympanohyal)
Appears shortly before birth
Forms basal part of process embedded in tympano mastoid part . Forms projected part outside.
1 for distal part stylohyal , 1/2nd year after birth ..
Stylohyal part does not unite with rest of bone until after puberty or never at all..

The squamoso-petrous sinus is the commonest anomalous venous sinus of the dura
mater, running in the angle between the petrous and squamous portions of the
temporal bone. The squamoso -petrous sinus is known to be present in fetal life. It
develops from the pro-otic group of veins and communicates with external veins via
a post glenoid vein in fetal life. The sinus decreases in size with growth although it
frequently persists into postnatal life (Butler, 1957). In all mammalian embryos the
Squamoso -petrous sinus communicates with the external jugular vein by an emissary
vein running through the spheno -parietal fontanelle. In some, e.g. the rat, this
communication persists throughout life (Butler, 1968). However, in man this
communication normally disappears and is present in under 1% of adult skulls
(Cheatle, 1889). Breathnach (1965) stated that the communication becomes diploic in
nature with growth.
The squamoso- petrous sinus: a fetal remnant J. Anat. (1991), 175, pp. 269-271


THE INFRATEMPORAL FOSSAThe infratemporal fossa is the space located deep to the ramus of the mandible together with the temporal fossa, pterygoid processes and maxillary tuberosity, the infratemporal fossa has been thought of by some anatomists as part of a ‘masticatory muscle compartment’ or ‘masticatory space’.
THE BOUNDARIES The fossa is bounded Anteriorly:: by the posterior surface of the maxilla posteriorly:: by the styloid apparatus, carotid sheathand deep part of the parotid gland. Medially:: lateral pterygoid plate and the superior constrictor muscle of the pharynx.
Laterally:: ramus of the mandible. The roof:: formed by the infratemporal surface of the greater wing of the sphenoid.

The infratemporal fossa has no anatomical floor, being continuous with tissue spaces in the neck.
The infratemporal fossa communicates with the temporal fossa deep to the zygomatic arch.
It also communicates with the pterygo palatine fossa through the pterygo maxillary fissure.
At the base of the cranium, the foramen ovale, the foramen spinosum and the sphenoidal emissary foramen (of Vesalius) enter the fossa through the sphenoid bone.

THE CONTENTS OF THE INFRATEMPORAL FOSSAThe major structures that occupy the infratemporal fossa are:• The lateral and medial pterygoid muscles• The mandibular division of the trigeminal nerve• The chorda tympani branch of the facial nerve• The otic parasympathetic ganglionThe maxillary artery and branches• The pterygoid venous plexus• The deep ‘lobe’ of the parotid gland.

B. Temporal fossa
Has the following boundaries:
Anterior : zygomatic process of the frontal bone and the frontal process of the zygomaticbone.Posterior : temporal line.Superior : temporal line.Lateral : zygomatic arch.Inferior : infratemporal crest.Floor : parts of the frontal, parietal, temporal, and greater wing of the sphenoid bone.

Contents::Contains the temporalis muscle, the deep temporal nerves and vessels, the auriculotemporal nerve,and the superficial temporal vessels.

Squamous part:: Temporalis muscle.
Auricularis posterior muscle b/w supra mastoid crest and squamo mastoid suture.
Zygomatic process:: medial surface gives origin to masseter muscle from its lower part
temporal fascia from its upper border
masseter muscle from its lower border
MUSCLES ATTACHED TO TEMPORAL BONE

Temporalis



















MASTOID PART:: External surface gives origin to
Auricularis posterior: close to middle of squamo mastoid suture.
Occipital belly of occipito-frontalis
Insertion of sternocleido mastoid
Insertion of splenius captitis
Insertion of longissismus captitis

Inferior surface near apex gives origin to LEVATOR PALATINI MUSCLE
The tensor veli palatini tenses the soft palate and by doing so, assists the levator veli palatini in elevating the palate to occlude and prevent entry of food into the nasopharynx during swallowing
Petrous part

Its distal part (stylohyal) gives attachment to the following: • stylohyoid ligament• stylomandibular ligament• styloglossus muscle (innervated by the
hypoglossal nerve)• stylohyoid muscle (innervated by the
facial nerve)• stylopharyngeus muscle (innervated by
the glossopharyngeal nerve)
Styloid process

VascularityPosterior auricular artery- skin over the mastoid process,auricle,
Styloid branch: supplies the mastoid antrum and mastoid air cells
Superficial temporal: temple
Deep auricular :external acoustic meatus ,tympanic membrane.
Anterior tympanic: tympanic membrane.
Deep temporal : Temporalis.
Petrous part of ICA

Diagram of relationship of nerves in the internal acoustic meatus.
VII = facial nerve
NI = nervus intermedius
VIIIc = cochlear nerve
VIIIvs = superior division of vestibular nerve
VIIIvi = inferior division of vestibular nerve
Innervation

Petrotympanic fissure:: b/w tegmen tympani and tympanic part, transmits anterior tympanic branch of maxillary artery to middle ear, chordatympani nerve,..
Petrous Portion Presents:: hiatus for greater petrosal nerve, hiatus for lesser petrosal nerve

Presents:: hiatus for greater petrosal nerve,
Auriculotemporal nervedeep temporal nerves



Classification:
Ulrich's classification:
Ulrich in 1926 classified temporal bone fractures into either transverse or longitudinal.
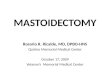
Longitudinal fractures:
This is the commonest type accounting for 80% of all temporal bone fractures. These fractures are caused by lateral blows like temporal or parietal types.
TEMPORAL BONE FRACTURES
The fracture line parallels the long axis of the petrous pyramid. It starts from the squamous portion of the temporal bone, extends through the postero superior portion of the external auditory canal, continues across the roof of the middle ear space, anterior to labyrinth to end anteromedially in the middle cranial fossa close to foramen lacerum and ovale

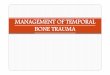
Transverse fractures:
This type of fracture comprises about 20% of all temporal bone fractures. They are usually caused by frontal / parietal blow. Rarely it could result from occipital blow also.
The fracture line runs at right angle to the long axis of the petrous pyramid. Usually it starts in the middle cranial fossa close to foramen lacerum, it crosses the petrous pyramid transeversely to end at the foramen magnum. Sometimes it may run across the internal acoustic meatus causing damage to auditory and facial nerves

longitudinal fracture line
Signs / Symptoms:
1. Bleeding from external canal due to laceration of skin and ear drum
2. Haemotympanum (conductive deafness)
3. Fractures involving the bony portion of external canal
4. Ossicular chain disruption causing conductive deafness.
5. Facial palsy (rare) 20% usually at the level of horizontal segment distal to geniculate ganglion
6. CSF otorrhoea (usually temporary)
7. Sensorineural hearing loss can occur due to consussion

transverse fracture line
Clinical features:
1. Sensorineural hearing loss due to damage to 8th cranial nerve
2. Facial palsy due to damage of facial nerve
3. Vertigo
4. Labyrinthitis ossificans


Common sequelae of temporal bone fractures:
1. Facial nerve palsy2. Damage to cochleo vestibular apparatus causing sensorineural hearing loss3. Conductive hearing loss due to ossicular disruption4. Balance disturbance5. Tinnitus / vertigo6. C.S.F. leak7. Perilymph fistula8. Post traumatic endolymphatic hydrops9. Cholesteatoma10. Menigocele / encephalocele11. Otogenic meningitis 12. Injuries to cranial nerves like VI, IX and cranial nerves up to XI 13 Vascular injuries i.e. injuries to internal carotid artery and sigmoid sinus

Imaging:
HRCT: HRCT of temporal bone is useful in assessing injuries complicated with CSF leak, facial palsy or suspected vascular injury. Usually 1mm cuts in both axial and cor0nal planes must be performed. Bone window cuts would be really useful.
It is also indicated when surgical intervention for otologic complications following temporal bone fracture becomes necessary.
It is indicated in patients with persistent cranial nerve injuries following skull base fracture.
CT angiography:This is indicated in evaluation of petrous carotid injury.
MRI:Helps in identification of intra labyrinthine haemorrhage, brain stem injury and nerve compression.

General clinical presentation of temporal bone fractures:
Neurologic injuries:
Commonly seen neurologic injuries in these patients are:1. Subdural hematoma2. Subarachnoid hemorrhage3. Contusion of brain4. Tension penumocephalus5. Injury to facial nerve6. Injury to vestibulocochlear nerve

CSF leak: is mostly in the form of otorrhoea. In the acute phase it could be missed as it would be admixed with blood. In patients with intact ear drum the csf would be shunted out via the eustachean tube and hence could easily be missed. Hence a high degree of suspicion is important in diagnosing these patients.
Following signs could point towards the diagnosis:1. Halo sign2. Reservoir sign3. Presence of Beta - 2 - transferrin in the fluid is diagnostic CSF leak is three / four times more common in patients with otic capsule violating type fractures.
Vascular injuries: All temporal bone fractures involving the jugular fossa / sigmoid groove always resulted in breech of internal jugular vein wall. Traumatic dissecting aneurysm of internal carotid artery can also be seen in patients with otic capsule violating injuries.

Delayed sequelae:
Cholesteatoma is a destructive and expanding growth consisting of keratinizing squamous epithelium in the middle ear and/or mastoid proces
Findings–Focal unilateral mass in EAC–Scalloping of bony EAC, most commonly in posterior, inferior aspect–Matrix with bony flecks–Progressive enlargement
Etiology•Congenital -ectodermal rest, rare•Spontaneous -abnormal migration of ectoderm•Acquired -postsurgical, post-traumatic

Menigocele / encephalocele:
Encephalocele, sometimes known by the Latin name cranium bifidum, is a neural tube defect characterized by sac-like protrusions of the brain and the membranes that cover it through openings in the skull. These defects are caused by failure of the neural tube to close completely during fetal development. Encephaloceles cause a groove down the middle of the skull, or between the forehead and nose, or on the back side of the skull. The severity of encephalocele varies, depending on its location

It is situated about 3 cm. behind, and a little above the level of the zygomatic process of the temporal bone.It marks the junction between four bones:the parietal bonethe squamous part of temporal bonethe greater wing of sphenoid bonethe frontal bone
Clinical significance
The pterion is known as the weakest part of the skull.In the clinical setting, the pterion is relevant because the anterior division of the middle meningeal artery runs beneath it, on the inner side of the skull, which is quite thin at this point. The combination of both a vital artery in this area and the relatively thin bone structure has lent itself to the name "God's little joke" by some physicians.[
A blow to the pterion (e.g., in boxing) may rupture the artery causing an epidural haematoma. The pterion may also be fractured indirectly. Blows to the top or back of the head may not cause fracture at the site of impact, but may place sufficient force on the skull that its weakest part, the pterion, will fracture

PTERION: A SITE FOR NEUROSURGICAL APPROACH
Chandana Bhargavi, Vasudha Saralaya, Vasudha Saralaya, Kishan K, Kishan K
Vol 2, No 12 (2011)
It is commonly used neurosurgical landmark. The anatomic location of the pterion is important in surgical interventions following surgical approaches to the anterior and middle cranial fossae, following extradural hemorrhage as well as tumors involving inferior aspects of the frontal lobe, such as olfactory meningioma, used in operations on the Broca's motor speech area and in repairing aneurysms of the middle cerebral artery as well as those of the upper basilar complex and also the anatomical varieties of the pterion, is of interest mainly to anthropologists and forensic pathologists, for assessing the location of the pterion in incomplete archeological remains or forensic materials

Temporal approachFirst described by Gillies for zygomatic arch #
AdvantagesAllow the application of great amount of controlled force to disimpact even the most difficult zygomatic #
Useful in later treatment when partial consolidation has already occurred

Technique 3x3cm area of hair is shaved approximately 2.5cm above & 2.5cm anterior to helix of the ear
2.5 cm incision made through the skin & SC tissue at an angle running from anterosupr to posteroinferior
White glistening temporalis fascia is visualized
Second deeper incision made through the fascia
Plane is identified B/W temporalis fascia & muscle

Intially periosteal elevator is placed to occupy the medial aspect of zygomatic arch & infratemporal surface of zygoma
Then elevator is replaced by rowe zygomatic elevator
Fracture is reduced
An audible crunch or crack usually accompanies the elevation

Quantifying Male and Female Shape Variation in the Mastoid
Region of the Temporal Bone
Proceedings of the 5th Annual GRASP Symposium, Wichita State University, 2009
there is variation in the size of the mastoid processes among males and females asdemonstrated by descriptive statistics. For each measurement, the male mean is slightly larger than the female mean

Some syndromesTrisomy 21 (Down
syndrome)
poorly developed Mastoids
Hypertelorism; epicanthic fold; slanting eyes; strabismus; narrowed nasal space; hypoplastic paranasal sinuses; protruding tongue; high palate; flattened skull; VSD/ASD, PDAs, situs inversus;

Crouzon’s disease
(craniofacial dysostosisatresia of EAC; narrow tympanic cavity;
Ocular proptosis; hypertelorism; hypoplasia of the maxilla; parrot-like nose; craniosynotosis
Hemifacial microsomiaatresia/ stenosis of EAC, Descent of tegmen.
Unilateral mandibular/ maxillary hypoplasia; macrostomia; hypoplastic TMJ; hemivertebrae or hypoplasia; coloboma of upper lid
Osteopetrosis (Albers- Schonberg disease
Obliteration of mastoid air cells.
Generalized increase in bone density with narrowed neural foramina; obliterated paranasal sinuses and mastoid air cells fractures; anemia; facial paralysis

Treacher-Collins syndrome (mandibulofacial dyostosis)
decreased size of middle ear cavity; underdeveloped mastoids..
Antimongoloid slant of palpebral fissures; coloboma of internal third of lower lid; malar/ mandibular hypoplasia; scalp hair projecting onto side of face


Superficial temporal spaceBetween temporal fascia & continuation of parotido masseteric fascia
Boundaries
Anterior superficial temporal space
Inferior zygomatic arch
Contents
Leaflet of buccal fat pad
Small veins—drain temporal
region
Temporal fat pad
Temporal branch of facial.n
Likely causes
Upper & lower molars
Neighbouring spaces
Buccal
temporal

Deep temporal spacesBoundaries
Lateral : temporalis muscle
Medial: squamous temporal bone,
sphenoid bone.
Inferior : superior surface of lateral pterygoid muscle
Superior : attachment of temporalis muscle to cranium of temporal crest
Anterior :posterior wall of maxillary sinus
pterygo maxillary fissure
posterior surface of orbit

Temporal space
Upper molars
Temparo cranial flaps
Circum zygomatic wiring
Buccal space
thrombophlebitis
Inferior petrosal sinus
ContentsPterygoid plexus maxillary artery & veinMandibular division of trigeminal.n Skull base foramina

Clinical features
Pain
Trismus -severe
Swelling over temporal region
Treatment
Extra orally
Small horizantal incision
|
|| to the zygomatic branch of facial .n
Dis advantage not producing
dependent drainage


Incised intra orally
Vertical incision just medial to
upper extent of anterior border of
mandibular ramus
Heamostat along medial aspect
of coronoid process into infra
temporal region
Blunt dissection damage to lingual .n avoided

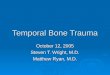
Battle's sign::
mastoid ecchymosis, is an indication of fracture of middle cranial fossa of the skull, and may suggest underlying brain trauma. Battle's sign consists of bruising over the mastoid process, as a result of extravasation of blood along the path of the posterior auricular artery. The sign is named after William Henry Battle..
J Neuro surg 112:186–188, 2010

Eagle's syndrome :Is an elongation of the styloid process or excessive calcification of the stylohyoid ligament or styloid process that causes neck, throat, or facial pain and dysphagia (difficulty in swallowing).
The pain may occur due to compression of the glossopharyngeal nerve,
which winds around the styloid process or stylohyoid ligament as it descends to supply the tongue, pharynx, and neck.
In addition, the pain is presumed to be caused by pressure on the internal and external carotid arteries by a medially or laterally deviated and elongated styloid process.
Additional symptoms may include taste disturbance, earache, headache, dizziness, and transient syncope (loss of consciousness resulting from cerebral ischemia).
The treatment for Eagle's syndrome is styloidectomy.

A Rare Cause for Cervical Pain: Eagle’s Syndrome
International Journal of Dentistry
Volume 2009, Article ID 781297, 3 pages
Eagle primarily described two syndromes
(1) Classic styloid syndrome: it frequently follows tonsillectomy and is characterized by pharyngodynia localized in the tonsillar fossa and sometimes accompanied by disphagia, hypersalivation,foreign body sensation, and more rarely by temporaryvoice changes;
(2) The stylo-carotid syndrome: it is not correlated withtonsillectomy. In this condition, the stylohyoid apparatuscompresses the internal and/or the externalcarotid arteries and especially their perivascularsympathetic fibers, resulting in a persistent painirradiating in the carotid territory

Temporal (giant cell) arteritis : is granulomatous inflammation with multinucleated giant cells, affecting the medium-sized arteries, especially the temporal artery.
Symptoms include severe headache, excruciating pain in the temporal area, temporal artery tenderness, visual impairment, transient diplopia, jaw claudication, fever, fatigue, and weight loss.
Diagnosis of this vascular disease of unknown origin can be confirmed by a temporal artery biopsy.
Temporal arteritis frequently responds to treatment with corticosteroids such as prednisone. AMA, January 2, 2002—Vol 287, No. 1

Tumors :: Tumors of the temporal bone are rare.
The following tumors can be seen:
•Exostoses
•External auditory canal carcinomas
•Glomus tumor
•Adenoma
•Congenital cholesteatoma
•EndoLymphatic Sac Tumor (ELST) ::
Low Grade Papillary Adenocarcinoma of the Endolymphatic Sac ,Papillary Adenoma of the Endolymphatic Sac

Rupture of the middle meningeal artery : may be caused by fracture of the squamous part of the temporal bone as it runs through the foramen spinosum and just deep to the inner surface of the temporal bone. It causes epidural hematoma with increased intracranial pressure.
Tripod fracture is a facial fracture involving the three
supports of the malar (cheek or zygomatic) bone including the zygomatic processes of the temporal, frontal, and maxillary bones.

Diseases of the temporal bone::
Systemic bone diseases
(1) Osteogenesis imperfecta (Van der Hoeve syndrome)
(2) Osteitis deformans (Paget's disease)
(3) Fibrous dysplasia
(4) Osteopetrosis
(5) Neurofibromatosis
(6) Genetic craniotabular hyperostoses
(a) hyperostosis corticalis
(b) sclerosteosis
(c) congenital hyperphosphatasia
(d) progressive diaphyseal dysplasia
(7) Genetic craniotabular dysplasias
(a) craniometaphyseal dysplasia
(b) frontometaphyseal dysplasia
(8) Craniofacial dysostosis
(9) Osteopathia striata

Recommended