Polycystic Ovarian Syndrome
John Miell
University Hospital Lewisham
Kings College Hospital
A heterogenous condition (or many conditions)
Stein-Leventhal Syndrome (1935)
Menstrual Irregularity Hirsutism, Acne, Alopecia Obesity
Stein I and Leventhal M (1935) Amenorrhoea associated with bilateral polycystic ovaries. Am J Obst Gyn 29:181
Hyperinsulinism, glucose intolerance and hyperandrogenism Achard C and Thiers J (1921): Le virilisme
pilaire et son association a l’insufficiance glycolytique (diabetes des femmes a barb)
Bulletin of the Academy of National Medicine
Features of PCOS
Clinical: Menstrual abnormalities Anovulatory subfertility Hirsutes, acne, alopecia Weight gain ?recurrent miscarriage
Features of PCOS
Endocrine: Elevated androgen Elevated LH Elevated estrogen and prolactin Elevated androstenedione Decreased SHBG
Biochemistry not reliable
LH elevated in 40% Serum testosterone not always elevated In a study of 1741 women with PCOS
confirmed on clinical features and USS only 28.9% had elevated testosterone
Features of PCOS
Metabolic: Insulin resistance Impaired GT and T2 DM Lipid abnormalities Cardiovascular risks Neoplastic risk (?)
PCOS-Definition Ovulatory dysfunction and clinical features
of hyperandrogenism
Polycystic ovaries plus one or more of the clinical features
Revised Diagnostic criteria for PCOS 1999: Chronic anovulation Clinical/biochemical signs of hyperandrogenism and
exclusion of other pathologies*
2003: 2/3 of Oligo and/or anovulation Clinical/biochemical signs of hyperandrogenism Polycystic ovaries
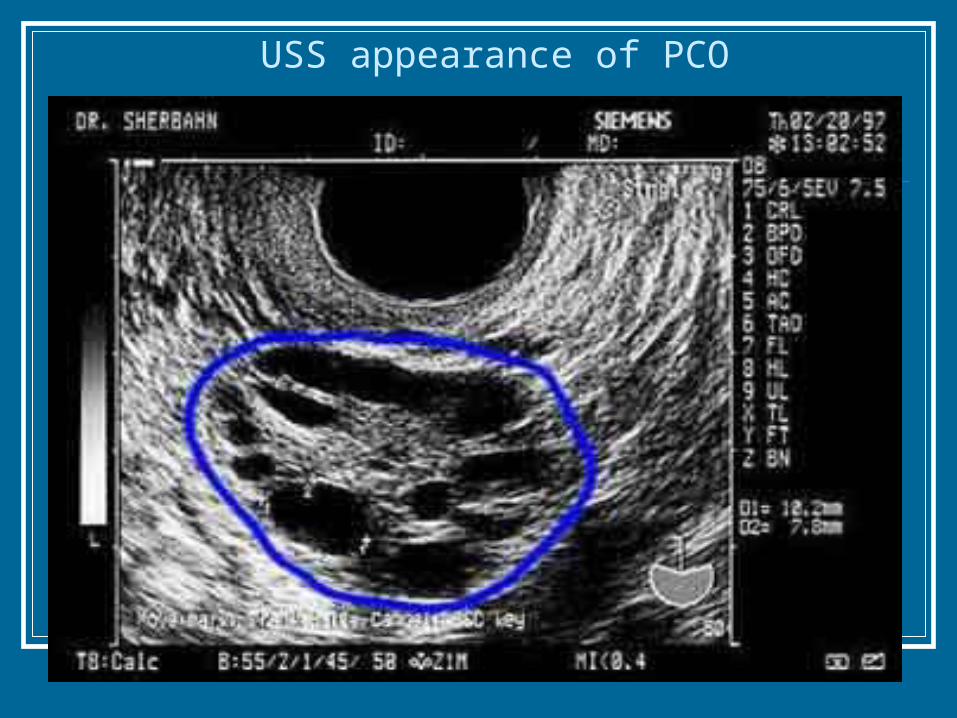
USS appearance of PCO
PCOS Definition
Two out of the following Oligo/anovulation Clinical or Biochemical hyperandrogenism PCO
Rotterdam consensus meeting 2003
Cause of PCOS 1 Unknown - but probably a vicious cycle
with a number of entry points: Defect in insulin action and secretion - Defect in insulin action and secretion -
hyperinsulinemia and insulin resistancehyperinsulinemia and insulin resistance Neuroendocrine defect - high LH pulse frequency and Neuroendocrine defect - high LH pulse frequency and
amplitudeamplitude Defect of androgen synthesis - enhanced ovarian Defect of androgen synthesis - enhanced ovarian
androgen productionandrogen production Defect in cortisol metabolism - enhanced adrenal Defect in cortisol metabolism - enhanced adrenal
androgen productionandrogen production
Cause of PCOS 2 Insulin resistance
-Hyperinsulinaemia
-Increased ovarian androgen
-inhibits SHBG production in liver
-increased free Testosterone
-inhibits IGFBP-1 production
-more free IGF-I Weight gain
-hyperinsulinaemia
Mechanism of hyperinsulinemia Insulin resistance:
Obese PCOS>obese>lean PCOS>Lean
Pancreatic Beta cell secretory dysfunction Decreased hepatic clearance of insulin Abnormal insulin signalling -
serine vs tyrosine phosphorylation serine phosphorylation inhibits receptor TK
activity and accentuates P450c17 activity
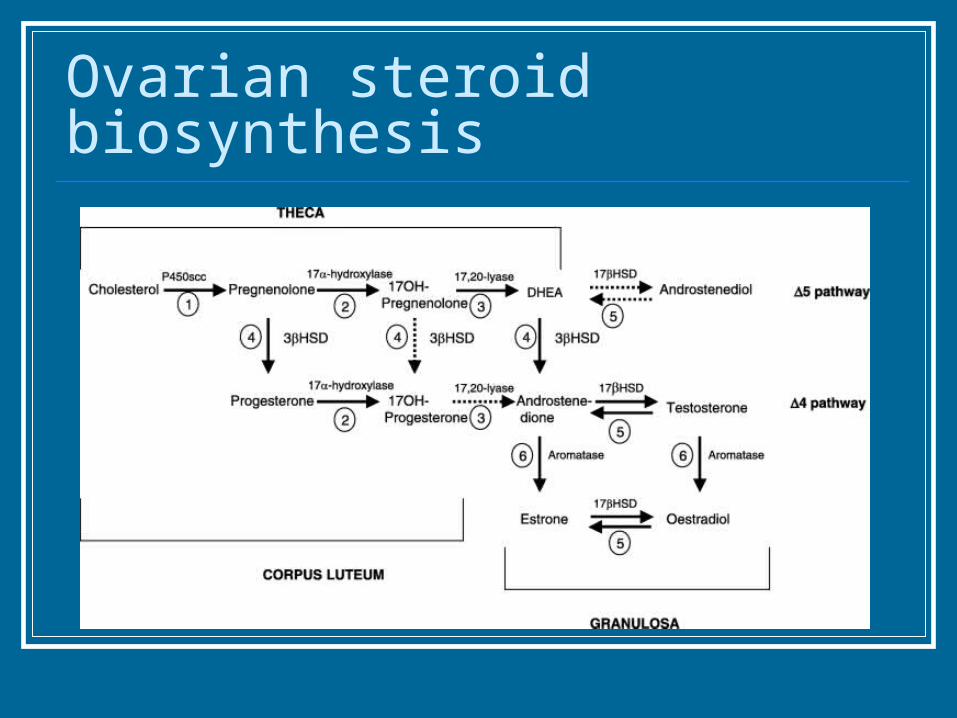
Ovarian steroid biosynthesis
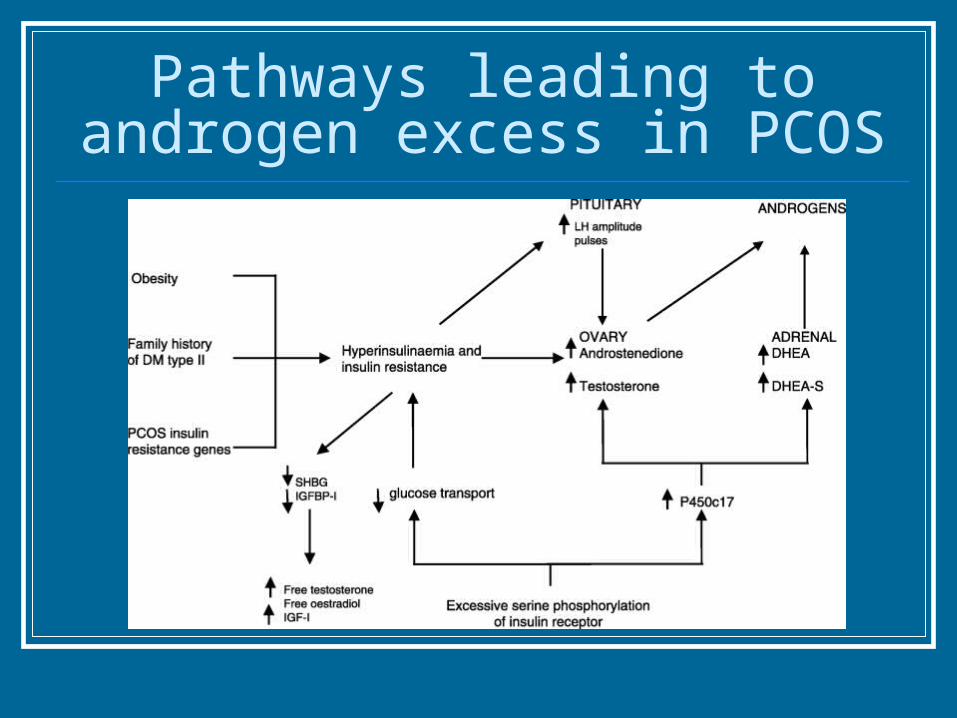
Pathways leading to androgen excess in PCOS
Increased cortisol metabolism Increased adrenal androgen production
may occur secondary to alteration in cortisol metabolism
Increased 5alphaR or reduced 11betaHSD may lead to reduced cortisol
This leads to increased ACTH (to maintain normal cortisol levels) at the expense of excess adrenal androgen stimulation
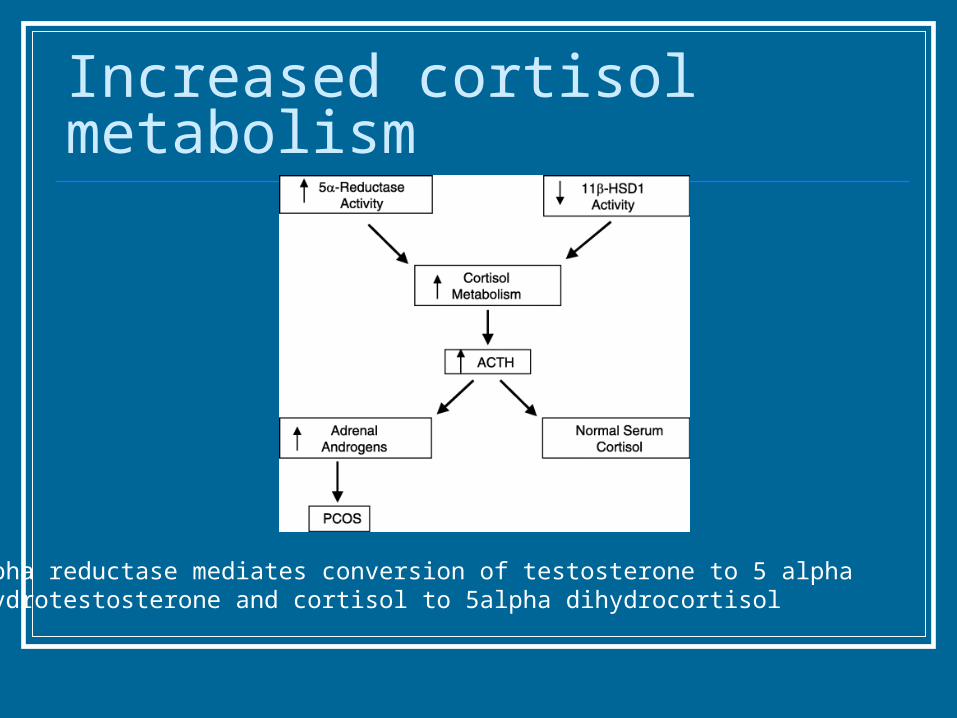
Increased cortisol metabolism
5alpha reductase mediates conversion of testosterone to 5 alphaDihydrotestosterone and cortisol to 5alpha dihydrocortisol
Genetics of PCOS High correlation between twin pairs for hyperinsulnemia and
hyperandrogenism (monogenic trait, 2 alleles, autosomal locus) Prospective study of 1st degree relatives of women with PCOS –
46% affected – half have hyperandrogenemia with regular cycles, half have PCOS
Association between PCOS and polymorphism at INS VNTR No difference in polymorphisms at CYP17 (encoding P450c17a) No real luck looking at follistatin or CYP11a (coding P450scc) ?type I IGF receptor/insulin receptor
Long term consequences of PCOS
Increased risk of diabetes Increased risk of cardiovascular disease Increased risk of carcinoma
Increased risk of diabetes Insulin resistance and beta cell dysfunction
precede Type2 DM Up to 40% of PCOS have IGT or T2DM (vs
10.3% in normal population studies) Legor et al (1999): 31.1% IGT (vs 7.8% in
age, weight, race matched controls) and 7.5% frank diabetes (vs 1.0%). Lean PCOS – 10.3% IGT, 1.5% frank T2DM.
Increased risk of diabetes Gestational diabetes is very common in
PCOS (? Role for Metformin in pregnancy).
PCOS and cardiovascular disease The metabolic syndrome:
Impaired glucose tolerance Type 2 DM Abdominal obesity Adverse lipid profiles

PCOS and cardiovascular disease The metabolic syndrome Diagnosis based on 3/5 of:
Fasting Triglycerides >1.7 mmol/L HDL – C < 1.3 mmol/L BP > 135/85 FBG > 6 mmol/L Waist circumference > 88cms
PCOS and cardiovascular disease Angiography reveals increased incidence in
coronary artery disease in women with Hirsutism (Wild et 1990)
USS evidence of PCO (Birdsall et al 1997)
PCOS and cardiovascular disease Follow up of women who have had wedge
resection
7.4 fold increase in risk of MI
PCOS and cardiovascular disease 30 year follow up of 786 women fulfilling reasonable
diagnostic criteria for PCOS ( Pierpoint et al 1998, Wild et al, 2000)
Increase in mortality/morbidity from diabetes and increased risk of non-fatal cerebrovascular disease.
No increase in deaths from heart disease mean BMI was 27 kg/m2 No increase in prevalence of T2DM in this study ? Protective effects of unopposed estrogen and increased
levels of VEGF
PCOS and cardiovascular risk factors
Dyslipidemia – secondary to: Elevated androgens, body fat distribution and
hyperinsulinemia Raised triglycerides Marginal elevation of LDL Reduced HDL Raised small dense LDL-III Increased hepatic lipase activity Elevated plasminogen activator inhibitor, PAI-1
?Consequence of androgens or hyperinsulinemia.
PCOS prevention of long term consequences
Advise to modify risk factors
Lose weight – diet/exercise
Stop smoking
Insulin sensitisation (?)
Screen for diabetes
Increased risk of cancer (??) No powerful well controlled studies using
accurately defined diagnostic criteria Possibly no overall increased risk of cancer in
practice (Venn et al, Lancet, 1999)
Increased risk of cancer (??) Endometrial cancer Theoretical risk of amenorrhoea and unopposed estrogen Mayo clinic – 3X increased risk of endometrial cancer in
women with anovulation without hypoestrogenemia (prob PCOS – Coulam, ObsGyn, 1983)
BUT – no good studies, poordiagnostic criteria, retrospective analyses etc.
Increased risk of cancer (??) Breast cancer Theoretical risk of amenorrhoea and unopposed
estrogen PCOS protective against Breast cancer in a self
reported historical study (Odd ratio 0.52 (0.32-0.87 – Gammon 1991)
No significant excess deaths from Breast cancer in a large group of PCOS (Pierpoint, J Clin Epidemiol, 1998)
Increased risk of cancer (??) Ovarian cancer The jury is out 2 studies suggest an increased risk - possibly
both subject to recall bias 3 studies suggest no increased risk
Treatment Depends on Symptoms
Clinical Presentation Oligo/amenorrhoea Subfertility Obesity Acne Hirsutism
Exercise and weight loss Improves insulin sensitivity Reduces serum testosterone Improves menstrual regularity Induces regular ovulation
Visceral fat Responsible for the adverse effects of
obesity Strong correlation with insulin resistance
Obesity and PCOS Waist circumference is better guide to
metabolic risk factors than is waist:hip ratio or BMI
waist ideally should be < 87cm
( and possibly <79cm) Exercise is more important than diet in
reducing visceral fat and correcting metabolic abnormalities
Oligo/amenorrhoea Risk of endometrial pathology
Combined oral contraceptive Cyclical progestagen
OR Annual TVS assessment of endometrium
Treatment of Hirsutism Shaving, Electrolysis or waxing Ornithine decarboxylase inhibitors COC Cyproterone acetate Spironolactone Flutamide and Finasteride Metformin
Hirsutism Oestrogen
suppresses ovarian testosterone
Increases SHBG Cyproterone acetate (progestogen)
Androgen antagonist
Suppresses LH
Oral contraceptive Ethinyl oestradiol 35mcg
Cyproterone Acetate 2mg Ethinyl Oestradiol 30 or 50mcg
Desogestrel 150mcg
Equally effective in treatment of Hirsutism
Porcile & Gallardo 1991
Ethinyl oestradiol +drosperinone
Reverse sequential Regime Dianette
Plus Cyproterone acetate 50-100mg
day 1-10 of pill packet
Earlier improvement in hirsutism
Barth et al 1991
Metformin Reduces insulin resistance 1000mg -1500mg daily
reduces serum insulin reduces serum testosterone Improves lipid profile Improves menstrual irregularity Improves fertility
Metformin & Clomiphene 61 women with BMI>28 Received Metformin 500mg tds or placebo
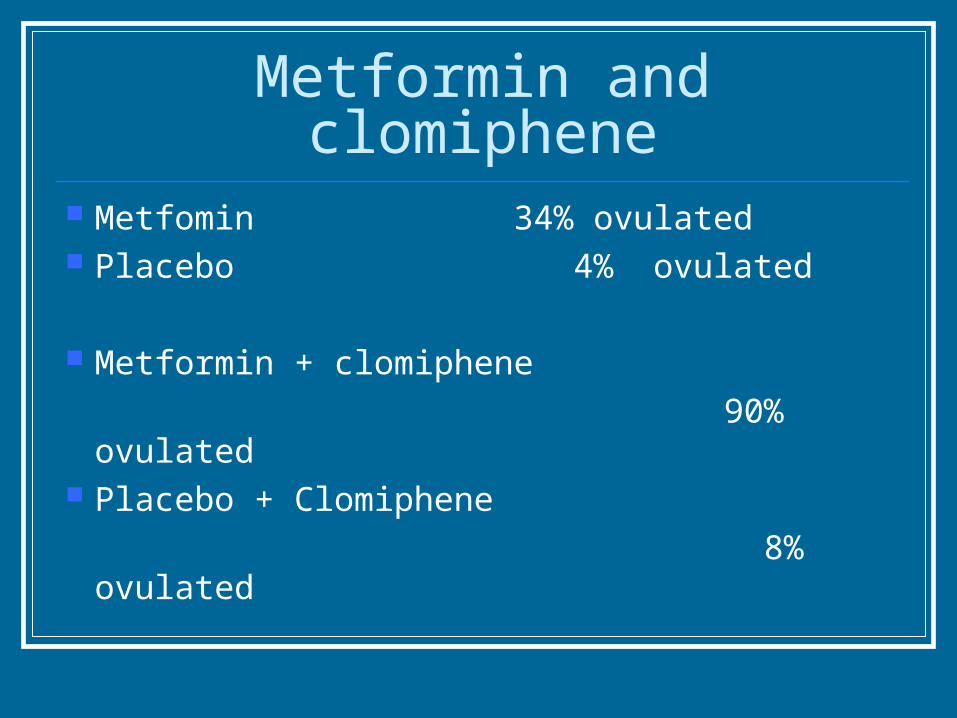
Metformin and clomiphene Metfomin 34% ovulated Placebo 4% ovulated
Metformin + clomiphene
90% ovulated Placebo + Clomiphene
8% ovulated
PCOS - conclusions Insulin resistance, hyperandrogenism, unusual
gonadotrophin dynamics Familial though no stron evidence of candidate
gene identity Links with obesity, cardiovascular disease, DM
and maybe endometrial cancer Needs lifestyle modification which remains the
mainstay of treatment Metformin has been a revelation
Surgical or medical treatment of PCOS
And/or
Recommended