Polycystic Ovarian Syndrome
Christina C DingConsultant in Obstetrics and gynaecology
Subspecialist in Reproductive Medicine and Surgery

Overview
Definition (and Prevalence)- much debated• Diagnostic Criteria update
Management update:• General:
– Life style changes– insulin sensitising agents– Prevention of long term health risks (CVD, Cancers, Psychological)
• Specific: symptomatic control– Obesity Mx – Antiobesity drugs, Bariatric surgery– Hyperandrogenism Tx – Infertility: Anoulatory cycles– Menstrual irregularities

Definition -PCOS
• Why is reaching consensus difficult?
• Problems with the lack of unified definition?
• New criteria in 2003

Definition- PCOS Challenges in reaching a consensus
• Heterogeneity in symptom and sign
• For an individual, these may change over time
• PCO can exist without clinical signs of the syndrome, which may become expressed overtime

Range of presenting complaints• Menstrual irregularities (unopposed E2)
• Anolulatory Infertility
• Hyperandrogenism (Acne/Hirsutism/Alopecia)
• Obesity
• Metabolic Risks (DM, H/T, CVD)
• Asymptomatic – incidental Scan finding of PCO

DefinitionProblems without a consensual definition
• Progress in Clinical Research hampered
• Inconsistencies and poor delivery of clinical care

Definition Revised 2003 Rotterdam diagnostic criteria
Two out of three
• Oligo / Anovulation
• Hyperandrogenism: clinical or biochemical
• USS Features– >12 follicles of 2-9 mm in diameter , or– ovarian volume >10 cm3 in one or both ovaries
Excluding: thyroid dysfunction, congenital adrenal hyperplasia, hyperprolactinaemia, androgen-secreting tumours and Cushing syndrome

Prevalence
• NIH criteria 1990– 6-7%
• Rotterdam consensus 2003– 20-25% UK Caucasian– 52% UK South Asian immigrant

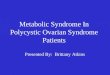
Wt. increase
Insulin receptor disorder
Insulin increase
Free estradiolincrease
High LHLow FSH
Free testosteroneincrease
Androstenandione increase
SHBG decrease
atresia
Theca (IGF-I)
Endometrial cancer
Testosteroneincrease
Estroneincrease
hirsutism
IGFBP-I**** decrease
IGFBP*** insulin like growth factor binding protein

Clinical Challenges
• Menstrual irregularities (unopposed E2)
• Anolulatory Infertility
• Hyperandrogenism (Acne/Hirsutism/Alopecia)
• Obesity
• Metabolic Risks (DM, H/T, CVD)

Management Update• General:
– Life style changes– insulin sensitising agents– Prevention of long term health risks (CVD, Cancers, Psychological)
• Specific: symptomatic control– Obesity Mx – Antiobesity drugs, Bariatric surgery– Hyperandrogenism Tx – Infertility: Anoulatory cycles– Menstrual irregularities

Management Update• General:
– Life style changes– insulin sensitising agents– Prevention of long term health risks (CVD, Cancers, Psychological)
• Specific: symptomatic control– Obesity Mx – Antiobesity drugs, Bariatric surgery– Hyperandrogenism Tx – Infertility: Anoulatory cycles– Menstrual irregularities

Life Style Changes
• The best diet and exercise regimens are unknown, but caloric restriction and increased physical activity are recommended.
RCOG guideline


Management Update• General:
– Life style changes– insulin sensitising agent– Prevention of long term health risks (CVD, Cancers, Psychological)
• Specific: symptomatic control– Obesity Mx – Antiobesity drugs, Bariatric surgery– Hyperandrogenism Tx – Infertility: Anoulatory cycles– Menstrual irregularities

Metformin
• Not licensed outside DM treatment• Safe (not established in pregnancy)
• Short term benefits (Wt. loss, OI, hirsutism)
• No long term benefits

Management Update• General:
– Life style changes– insulin sensitising agents– Prevention of long term health risks (CVD, Cancers, Psychological)
• Specific: symptomatic control– Obesity Mx – Antiobesity drugs, Bariatric surgery– Hyperandrogenism Tx – Infertility: Anoulatory cycles– Menstrual irregularities

Cancer risks
• Endometrial Cancer – Risk is 3.1 x higher (95% C I 1.1- 7.3)
Coulam et al, 1983 (1270 chronic anovulation pt)
• Breast Cancer– No significant increased risks
Pierpoint et al., 1998; Coulam et al., 1983; Anderson et al., 1997
• Ovarian Cancer– No significant increased risks
Pierpoint et al., 1998

Long term risks : CVD
PCOS metabolic abnormalities suggesting increased cardiovascular risk
Observation Reference
Triglycerides↑, HDL↓ Rajkhowa et al. (1997); Orio et al. (2004)C-reactive protein↑ Taponen et al. (2004); Boulman et al. (2004)Homocysteine↑ Carmina et al. (2005)Leucocytes↑ Orio et al. (2005)Fibrinolytic activity↓ Yildiz et al. (2002)Metabolic syndrome↑ Apridonidze et al. (2005)
The ESHRE Capri Workshop Group, ‘Hormones and cardiovascular health in women’, Human Reproduction Update, 2006

Long term risks: DM,H/T
Follow-up studies of PCOS
Authors Patients Intermediate outcomes CVD outcomes
Dahlgren et al. (1992) 33 followed for 22–31 years More diabetes and hypertensionPierpoint et al. (1998) 786 diagnosed between 1930 -79 SMR 0.9 (95% CI:
0.7, 1.2)Wild et al. (2000) 240 PCOS diagnosed before 1979 More cerebral disease and diabetes Similar CHD mortalityElting et al. (2001) 346 followed for 2–32 years More diabetes and hypertension
SMR, Standardized Mortality Ratio
The ESHRE Capri Workshop Group, ‘Hormones and cardiovascular health in women’, Human Reproduction Update, 2006

Long term risks : obstetricMeta –analysis of 15 studies involving 720 women presenting with PCOS and 4505 controls
Higher risks of • Gestational DM (OR 2.94; 95% CI: 1.70–5.08)
• Pregnancy-induced H/T (OR 3.67; 95% CI: 1.98–6.81)
• Preterm birth (OR 1.75; 95% CI: 1.16–2.62) • Perinatal mortality (OR 3.07; 95% CI: 1.03–9.21)
Hum. Reprod. Update 2006, A meta-analysis of pregnancy outcomes in women with PCOS

Psychological: Quality of Life
Symptoms such as acne, hirsutism, irregular menses, amenorrhoea, obesity and subfertility are a major source of psychological morbidity and can negatively affect quality of life (QoL).
Systematic review: PCOS has a significant negative impact on a woman’s health-related quality of life
Health-related quality of life measurement in women with polycystic ovary syndrome: a systematic review. Jones et al, Human Reproduction Update (2008)

Management Update• General:
– Life style changes– insulin sensitising agents– Prevention of long term health risks (CVD, Cancers, Psychological)
• Specific: symptomatic control– Obesity Mx – Antiobesity drugs, Bariatric surgery– Hyperandrogenism Tx – Infertility: Anoulatory cycles– Menstrual irregularities

Management Update• General:
– Life style changes– insulin sensitising agents– Prevention of long term health risks (CVD, Cancers, Psychological)
• Specific: symptomatic control– Obesity Mx – Antiobesity drugs, Bariatric surgery– Hyperandrogenism Tx – Infertility: Anoulatory cycles– Menstrual irregularities

Antiobesity Drug
• Orlistat (Xenical)– gastric/pancreatic Lipase inhibitor
• Sibutramine (Reductile)– SNRI– Withdrawn since Jan 2010 due to increased heart
attack and stroke risks

Bariatric Surgery
• Two groups: malabsorptive & restrictive procedures • Malabsorptive procedures induce decreased
absorption of nutrients by shortening the functional length of the small intestine. The created short-bowel syndrome leads to a negative energy balance and weight loss.
• Restrictive operations reduce the storage capacity of the stomach and as a result early satiety arises, leading to a decreased caloric intake.

Figure 1 Bariatric procedures. (a) Jejunoileal bypass; (b) biliopancreatic diversion; (c) biliopancreatic diversion with duodenal switch; (d) vertical banded gastroplasty; (e) laparoscopic adjustable gastric band; and (f) Roux-en-Y gastric bypass.

Bariatric Surgery
Benefits– Average weight loss 20–40 kg – Recovery from type 2 diabetes in 76.8%
Risks– Mortality: early (<30/7) 0.1-2%– Morbidity:
• VTE (0.4-3.1%)• Infection• Anastomotic leak / stenosis (20-30%)

Management Update• General:
– Life style changes– insulin sensitising agents– Prevention of long term health risks (CVD, Cancers, Psychological)
• Specific: symptomatic control– Obesity Mx – Antiobesity drugs, Bariatric surgery– Hyperandrogenism Tx – Infertility: Anoulatory cycles– Menstrual irregularities

Hyperandrogenism
• Acne
• Hirsutism
• Male pattern hair loss– Sign of severe androgen excess (virilization)

Hirsutism• 5-10% women of child bearing age
– 70% PCOS– 23% idiopathic– 4.3% CAH– 0.2% A S tumour (ovarian or adrenal)
• Hx: sudden onset, rapid virilization
• Ix: testosterone, free testosterone.– If [testosterone] > 5nmol/L => [DHEA-S] & [androstenedione]
to exclude an adrenal or ovarian tumour

Hirsutism - treatment options
Systemic (over 3-6 months)• COCP: less androgenic progesterone: cyproterone acetate Diannette , drospirenone Yasmin• Antiandrogens (uncommonly used)
– Spironolactone (Aldactone), an aldosterone antagonist
– Cyproterone acetate – Flutamide is a pure nonsteroidal antiandrogen that acts as an androgen receptor blocker.
– Finasteride is a potent inhibitor of the type 2 isoenzyme of 5-á-reductase, which blocks the conversion of testosterone to 5-á-dihydrotestosterone
• Corticosteroids : late onset CAHTopical
– Eflornithine cream (Vaniqa)Cosmetic
Direct Hair Removal: plucking, waxing, electrolysis, laser removal

Management Update• General:
– Life style changes– insulin sensitising agents– Prevention of long term health risks (CVD, Cancers, Psychological)
• Specific: symptomatic control– Obesity Mx – Antiobesity drugs, Bariatric surgery– Hyperandrogenism Tx – Infertility: Anoulatory cycles– Menstrual irregularities

Ovulation Induction: stepwise approach (RCOG)
1. Weight loss: If BMI >30 K/m2
2. Clomiphene citrate 3. CC + Metformin4. Low dose FSH injection5. Ovarian drilling 6. IVF

Laparoscopic ovarian drilling• Diathermy or laser• Clomid resistant anovulatory PCOS
Benefits
• Ovulation rate >70%Pregnancy rates >50%
• Similar pregnancy and miscarriage rates to Gonadotrophins
• No increase in multiple pregnancies and reduces ovarian hyperstimulation.
Risks
• Risk of loss of ovarian tissue and thus reducing the ovarian reserve
• Risk of surgery• ?Adhesions

Ovarian drilling

Management Update• General:
– Life style changes– insulin sensitising agents– Prevention of long term health risks (CVD, Cancers, Psychological)
• Specific: symptomatic control– Obesity Mx – Antiobesity drugs, Bariatric surgery– Hyperandrogenism Tx – Infertility: Anoulatory cycles– Menstrual irregularities

Mx of a/oligomenorrhea
• Progesterone induced Bleeding– 3 monthly– Reduce risks of E hyperplasia and E carcinoma

Overview
Definition (and Prevalence)- much debated• Diagnostic Criteria update
Management update:• General:
– Life style changes– insulin sensitising agents– Prevention of long term health risks (CVD, Cancers, Psychological)
• Specific: symptomatic control– Obesity Mx – Antiobesity drugs, Bariatric surgery– Hyperandrogenism Tx – Infertility: Anoulatory cycles– Menstrual irregularities

Recommended