163D.H. Best and J.J. Swensen (eds.), Molecular Genetics and Personalized Medicine, Molecular and Translational Medicine, DOI 10.1007/978-1-61779-530-5_8, © Springer Science+Business Media, LLC 2012
Introduction
Metabolic disorders affect the transformation of nutrients in energy or in other compounds necessary for growth. They are due to defi ciencies in enzymes or trans-porters involved in the metabolism of sugars, amino acids, fatty acids, and macro-molecules. There is a wide spectrum of clinical presentation with onset of symptoms ranging from the newborn period to adult life. The consequences of untreated met-abolic disorders can be extremely severe and devastating, independently from the age of onset. Early identifi cation and treatment of these conditions before symp-toms appear and irreversible damage has occurred can improve overall outcome and quality of life, with reduction of morbidity, mortality, and disabilities. In recent years, advances in technology, such as the introduction of tandem mass spectrom-etry, has enabled neonatal screening for many diseases caused by impaired metab-olism of amino acids and fatty acids through multiplex analysis of several metabolites. This chapter will discuss some of the most common disorders of metabolism identifi ed through universal newborn screening and how molecular genetics can integrate the screening and biochemical tests to reach a defi nite diag-nosis of metabolic disorders in the asymptomatic patient.
M. Pasquali , Ph.D., FACMG (*) Department of Pathology , University of Utah and ARUP Laboratories , 500 Chipeta Way , Salt Lake City , UT 84108 , USA e-mail: [email protected]
N. Longo , M.D., Ph.D. Division of Medical Genetics, Department of Pediatrics , University of Utah, 2C412 SOM, 50 N Mario Capecchi Drive, School of Medicine , Salt Lake City , UT 84132, USA e-mail: [email protected]
Chapter 8 Newborn Screening for Metabolic Disorders
Marzia Pasquali and Nicola Longo

164 M. Pasquali and N. Longo
Newborn Screening
Newborn screening is a public health activity that started in the early 1960s, thanks to Dr. Robert Guthrie, who developed a bacterial inhibition assay to screen for phenylketonuria using newborns’ blood spotted and dried on fi lter paper [ 1 ] .
Since then, millions of infants in the United States have been screened for a variety of genetic and congenital disorders.
Each state in the United States decides the panel of disorders included in their newborn screening programs. The use of tandem mass spectrometry (MS/MS), detecting simultaneously amino acids and acylcarnitines in the same blood spot, has greatly increased the number of disorders amenable to newborn screening [ 2, 3 ] . In 2005, the American College of Medical Genetics (ACMG) released a report, commissioned by the Maternal and Child Health Bureau (MCHB) of HRSA (Health Resources and Services Administration), with recommendations for a uniform panel for newborn screening [ 4 ] . This report recommended screening all newborns in the United States for 29 conditions, including fi ve fatty acid oxidation disorders, nine organic acidemias, six aminoacidopathies, three hemoglobinopathies, and six other disorders (Table 8.1 ). Of these conditions, 20 are screened for using tandem mass spectrometry, while the others use more “traditional” methods (isoelectrofocusing, immunoassay, HPLC, etc.). At the beginning of 2011, the addition of SCID (severe combined immunodefi ciency) to the uniform panel was recommended and intro-duced the fi rst DNA-based screening test in newborn screening [ 5 ] .
Two main classes of metabolites are detected by tandem mass spectrometry: amino acids and acylcarnitines. Amino acids become elevated in certain aminoaci-dopathies and urea cycle defects (phenylketonuria, tyrosinemia, maple syrup urine disease, etc.), while the study of the acylcarnitine profi le can identify defects of fatty acid oxidation (medium-chain acyl-CoA dehydrogenase defi ciency, very-long-chain acyl-CoA dehydrogenase defi ciency, and others) and organic acidemias (propionic acidemia, methylmalonic acidemia, glutaric acidemia type I, etc.). Disorders of car-bohydrate metabolism (such as galactosemia) cannot yet be detected by MS/MS; however, methods are in development [ 6– 8 ] .
Blood is collected from a heel stick from each newborn and spotted on a fi lter paper card, and then the card is sent to a centralized laboratory where testing occurs. Typically, the sample is collected prior to discharge from the hospital of birth, between 24 and 48 h of life. This allows enough time to have a build-up of abnormal metabolites as a result of a “full” feeding, necessary to identify amino acidopathies, yet maintaining the ability to identify fatty acid oxidation disorders, which require a more “stressed” sample. Abnormal results, i.e., results outside the range observed for the normal population, are followed up with diagnostic tests to confi rm or exclude a diagnosis of a metabolic disorder.
Typically, biochemical genetics tests (amino acids, organic acids, acylcarnitines analyses in blood, and/or urine) represent the fi rst line of testing and are suffi cient to diagnose or exclude a metabolic disorder. This is especially true when patients are symptomatic and their biochemical phenotype is grossly abnormal. With the expansion of newborn screening, metabolic disorders are now identifi ed before the

1658 Newborn Screening for Metabolic Disorders
Table 8.1 Recommended uniform screening panel (core conditions) of the Secretary’s Advisory Committee on Heritable Disorders in Newborns and Children
ACMG code Core condition
Organic acidemia PROP Propionic acidemia MUT Methylmalonic acidemia (methylmalonyl-CoA mutase) Cbl A,B Methylmalonic acidemia (cobalamin disorders) IVA Isovaleric acidemia 3-MCC 3-Methylcrotonyl-CoA carboxylase defi ciency HMG 3-Hydroxy-3-methylglutaric aciduria MCD Holocarboxylase synthase defi ciency ßKT ß-Ketothiolase defi ciency GA1 Glutaric acidemia type I
Fatty acid oxidation CUD Carnitine uptake defect/carnitine transport defect MCAD Medium-chain acyl-CoA dehydrogenase defi ciency VLCAD Very-long-chain acyl-CoA dehydrogenase defi ciency LCHAD Long-chain L-3 hydroxyacyl-CoA dehydrogenase defi ciency TFP Trifunctional protein defi ciency
Amino acidopathy ASA Argininosuccinic aciduria CIT Citrullinemia, type I MSUD Maple syrup urine disease HCY Homocystinuria PKU Classic phenylketonuria TYR I Tyrosinemia, type I
Endocrinopathy CH Primary congenital hypothyroidism CAH Congenital adrenal hyperplasia
Hemoglobinopathy Hb SS S,S disease (sickle cell anemia) Hb S/ßTh S, b -thalassemia Hb S/C S,C disease
Others BIOT Biotinidase defi ciency CCCHD Critical cyanotic congenital heart disease (pending secretary approval) CF Cystic fi brosis GALT Classic galactosemia HEAR Hearing loss SCID Severe combined immunodefi ciencies
The nomenclature for conditions is based on the report “Naming and counting disorders (conditions) included in newborn screening panels” Pediatrics 2006;117(5) Suppl:S308-14
patients become symptomatic, at least in the majority of the cases. This brings an additional level of complexity, as the biochemical phenotype is now less obvious, and the fi nal diagnosis may require additional tests such as enzyme/receptor/trans-porter assays and/or molecular analysis. In addition, for some metabolic condi-tions, heterozygotes may show the same abnormalities as the affected individuals;

166 M. Pasquali and N. Longo
therefore, the inclusion of molecular analysis in confi rmatory algorithms (see, e.g., those recommended by the American College of Medical Genetics: http://www.acmg.net/AM/Template.cfm?Section=NBS_ACT_Sheets_and_Algorithms_Table&Template=/CM/HTMLDisplay.cfm&ContentID=5072 ) is increasingly used.
This chapter will review the groups of metabolic disorders identifi ed by newborn screening, with special emphasis on the molecular diagnosis of these conditions.
Disorders of Amino Acid Metabolism
The concentrations of free amino acids in physiological fl uids refl ects the balance between exogenous intake, endogenous release from the catabolism of proteins, the kidney function responsible for fi ltration and reabsorption, and the body utilization to synthesize proteins or produce energy. Changes in any of these steps can result in accumulation or defi ciency of one or more amino acids.
The aminoacidopathies phenylketonuria, maple syrup urine disease, homocysti-nuria, tyrosinemia type I, and the two defects of the urea cycle, citrullinemia and argininosuccinic aciduria, are the amino acid disorders included in the core panel of conditions recommended by the American College of Medical Genetics to be screened for in each infant (Table 8.1 ). The characteristic amino acids elevated in these conditions are identifi ed by tandem mass spectrometry. Other disorders of the urea cycle (such as ornithine transcarbamylase defi ciency and carbamyl phosphate synthase defi ciency), characterized by low concentrations of citrulline and arginine, are not included in this panel because the reliability of newborn screening in identi-fying analytes present at low concentrations is not optimal. To overcome this prob-lem, the use of ratios of amino acids seems promising. Table 8.2 lists selected disorders of amino acid metabolism identifi able by newborn screening and the strat-egy for confi rming or excluding the diagnosis.
Phenylketonuria
Phenylketonuria (PKU) results from the impaired conversion of phenylalanine to tyrosine leading to increased concentration of phenylalanine in body fl uids. Phenylketonuria is caused by a defi ciency of phenylalanine hydroxylase, the enzyme converting phenylalanine into tyrosine, in about 98% of cases. In the remaining 2% of the cases, elevated phenylalanine is due to a defect in the synthesis or recycling of tetrahydrobiopterin, the essential cofactor of phenylalanine hydroxylase. The combined incidence of these conditions is about 1:10,000 to 1:20,000 live births. In addition to accumulation of phenylalanine, some of its metabolites, such as phe-nyllactate and phenylpyruvate (phenylketones), can also accumulate and be excreted in the urine. The pathophysiology is due to the neurotoxic effect of high concentra-tions of phenylalanine and defi ciency of tyrosine, which interferes with the synthesis of neurotransmitters [ 10 ] .

1678 Newborn Screening for Metabolic Disorders
Tabl
e 8.
2 D
iagn
ostic
str
ateg
y an
d D
NA
test
ing
in s
elec
ted
diso
rder
s of
am
ino
acid
met
abol
ism
iden
tifi a
ble
by n
ewbo
rn s
cree
ning
Dis
ease
G
ene
New
born
scr
eeni
ng
Bio
chem
ical
fi nd
ings
E
nzym
e as
say
Firs
t-lin
e D
NA
te
stin
g A
dditi
onal
D
NA
test
ing
Phen
ylke
tonu
ria
(PK
U)
PAH
�
Phen
ylal
anin
e �
Phen
ylal
anin
e (P
AA
) N
orm
al p
teri
n pr
ofi le
N
orm
al D
HPR
act
ivity
Liv
er (
not
usua
lly
done
)
Full
gene
seq
uenc
ing
NA
Tyro
sine
mia
ty
pe I
(T
YR
-I)
FAH
�
Succ
inyl
acet
one
(� T
yros
ine
not
relia
ble)
� Su
ccin
ylac
eton
e (U
OA
) �
Tyro
sine
(an
d ot
her
amin
o ac
ids)
(PA
A)
Liv
er (
DN
A
test
ing
pref
erab
le)
Targ
eted
mut
atio
nal
anal
ysis
Fu
ll ge
ne
sequ
enci
ng
Hom
ocys
tinur
ia
(Cla
ssic
) (H
CY
)
CB
S �
Met
hion
ine
� M
ethi
onin
e �
Hom
ocys
tine
(PA
A)
Fibr
obla
sts
Full
gene
seq
uenc
ing
NA
Map
le S
yrup
Uri
ne
Dis
ease
(M
SUD
)
BC
KD
HA
(E
1 a )
BC
KD
HB
(E
1 b )
DB
T (
E2)
� L
euci
ne
� L
euci
ne, v
alin
e,
isol
euci
ne
� A
llois
oleu
cine
(PA
A)
Fibr
obla
sts
Full
gene
seq
uenc
ing
NA
Citr
ullin
emia
ty
pe I
(C
IT)
ASS
1 �
Citr
ullin
e �
Citr
ullin
e (P
AA
) Fi
brob
last
s Fu
ll ge
ne s
eque
ncin
g N
A
Citr
ullin
emia
ty
pe I
I (c
itrin
de
fi cie
ncy)
SLC
25A
13
� C
itrul
line
(mig
ht
be n
orm
al
at b
irth
)
� C
itrul
line
(and
oth
er
amin
o ac
ids)
(PA
A)
Not
indi
cate
d Fu
ll ge
ne s
eque
ncin
g N
A
Arg
inin
osuc
cini
c ac
idur
ia (
ASA
) A
SL
� C
itrul
line
� A
rgin
inos
ucci
nic
acid
� C
itrul
line,
ar
gini
nosu
ccin
ic
acid
(PA
A)
Fibr
obla
sts
Full
gene
seq
uenc
ing
NA
PAA
pla
sma
amin
o ac
ids,
UO
A u
rine
org
anic
aci
ds

168 M. Pasquali and N. Longo
Patients with phenylketonuria (PKU) do not show any symptoms at birth nor suffer any acute metabolic decompensation attacks. Delays in development, chronic eczema, and acquired microcephaly appear after a few months of life. Early identi-fi cation and treatment (before 2 weeks of life) prevents mental retardation and other complications. For this reason, all infants are screened at birth for this condition. Newborn screening is done by measuring phenylalanine in blood spots collected usually 24–48 h after birth. The ratio phenylalanine/tyrosine is also used to differ-entiate false positive results, due to intravenous hyperalimentation or liver immatu-rity/disease, from true positives. The diagnosis of PKU is confi rmed by plasma amino acid analysis. In all infants identifi ed by newborn screening with elevated phenylalanine, even if the elevation is minimal, disorders of the cofactor (tetrahyd-robiopterin) synthesis or recycling need to be excluded by measuring urine pterin profi le and activity of dihydropterine reductase (DHPR) in red blood cells. Phenylalanine hydroxylase defi ciency is diagnosed when plasma phenylalanine concentrations are above the normal reference interval and tyrosine is low or nor-mal, with a normal urine pterin profi le and normal DHPR activity.
Dietary therapy for PKU consists of a special formula without phenylalanine but containing tyrosine. Therapy should be started as soon as possible and ideally before 3 weeks of age [ 9– 11 ] and needs to be continued for life. Phenylalanine concentra-tions are monitored periodically and should remain between 60 and 360 m M (nor-mal 30–80 m M) to assure adequate brain development. High concentrations of phenylalanine in the fi rst years of life lead to mental retardation. Dietary control of phenylalanine is especially important for patients with PKU during pregnancy. In fact, phenylalanine at high concentrations is teratogenic and, depending on the period of exposure, leads to an increased risk of spontaneous abortion, congenital heart defects, facial dysmorphism, microcephaly, and developmental delay. Adverse pregnancy outcome in pregnant women with PKU can be minimized by maintaining phenylalanine concentrations <360 m M [ 12– 14 ] .
Benign hyperphenylalaninemia (phenylalanine <300 m M) is a condition occa-sionally identifi ed by newborn screening because of a moderately elevated phenyla-lanine. These patients have a partial defi ciency of phenylalanine hydroxylase with residual enzyme activity up to 35% of normal. Although they may not require dietary treatment, plasma concentrations of phenylalanine should be monitored periodically, especially when changes in the diet are implemented.
Patients with a defect in the synthesis or recycling of tetrahydrobiopterin (BH 4 )
present with signs of neurological involvement despite adequate dietary control of phenylalanine. This is due to the fact that BH
4 is also involved in the synthesis of the
neurotransmitters serotonin and dopamine. These patients are clinically indistin-guishable from classic PKU (phenylalanine hydroxylase defi ciency) at the time of the newborn screening; however, they deteriorate rapidly with loss of head control, truncal hypotonia with hypertonia of the extremities, drooling, swallowing diffi cul-ties, and myoclonic seizures between 2 and 6 months of age [ 15 ] . Their treatment requires supplements with BH
4 and neurotransmitter precursors. The diagnosis is
suspected by biochemical fi ndings (hyperphenylalaninemia, abnormal CSF neu-rotransmitters, abnormalities in CSF/urine pterins, and/or dihydropteridine reductase activity in blood cells) and confi rmed by DNA testing [ 15 ] .

1698 Newborn Screening for Metabolic Disorders
DNA Testing
Phenylalanine hydroxylase is expressed only in the liver, and confi rmation of the diagnosis by enzyme assay is not usually performed. DNA sequencing of the caus-ative gene can defi nitively confi rm the diagnosis if needed and can guide the therapy [ 16, 17 ] . Recently, trials with high doses BH
4 in addition to diet have been proven
effective in controlling phenylalanine concentrations in patients with PKU [ 16, 18, 19 ] , and certain mutations in the PAH gene are more frequently encountered in the responding population ( http://www.biopku.org/biopkudocs/PAH_domains.pdf ). A total of 564 different mutations have been described in patients with PKU ( http://www.pahdb.mcgill.ca ) by April 2011. The majority are missense mutations (about 60% of total) that impair enzyme stability or its active site. The remaining mutations can affect splicing, result in insertions or deletions (sometimes in frame), or result in the direct insertion of a premature stop codon. For some mutations and variations of unknown signifi cance, the mechanism of action remains unclear. DNA testing for phenylalanine hydroxylase defi ciency is clinically available, and the procedure of choice is DNA sequencing of all exons, unless familial mutations are already known.
DNA testing for defects of biopterin synthesis and recycling is clinically avail-able, and there is a public database collecting all mutations identifi ed in these patients ( http://www.biopku.org/dbsearches/BIODEF_Start.asp ). Biochemical test-ing in blood spots (DHPR defi ciency), urine (GTPCH1 and PTPS), and CSF (SR) can guide toward the genes to study.
Tyrosinemia Type I
Hepatorenal tyrosinemia (tyrosinemia type I, TYR-I) is an autosomal recessive dis-ease caused by defi ciency of fumarylacetoacetate hydrolase, an enzyme expressed primarily in the liver and kidney [ 20 ] . The incidence of TYR-I is approximately 1 in 100,000, with well-known clustering of cases in the Lac-St.-Jean region of Quebec (Canada). Patients with tyrosinemia type I can present before 6 months of age with severe liver involvement or after 6 months of age with chronic failure to thrive, mild hepatocellular dysfunction, renal involvement, and rickets due to renal Fanconi syndrome [ 20 ] . They can have extreme irritability due to peripheral neu-ropathy mimicking acute intermittent porphyria. This is caused by an accumulation of delta-aminolevulinic acid due to inhibition of delta-aminolevulinic acid dehy-dratase by succinylacetone [ 20 ] , a toxic compound and biochemical marker accu-mulating in tyrosinemia type I. Untreated patients can develop liver cirrhosis and are at very high risk for liver cancer.
Patients with tyrosinemia type I have elevated concentrations of tyrosine in the plasma amino acids, but this elevation is not usually as marked as in patients with other forms of tyrosinemia. Elevated tyrosine can be seen in other forms of tyrosine-mia (tyrosinemia types II and III), transient tyrosinemia of the newborn, prematu-rity, hepatocellular dysfunction of almost any cause (including those caused by

170 M. Pasquali and N. Longo
disorders of sugar metabolism, galactosemia, fructosemia, peroxisomal disorders, mitochondrial DNA depletion syndrome), and with diets very rich in proteins. The biochemical diagnosis of tyrosinemia type I is based on the detection in the urine organic acids of succinylacetone (4,6-dioxaneheptanoic acid), the by-product of fumarylacetoacetic acid, which is the intermediate immediately upstream of the enzyme defect [ 20 ] . Tyrosinemia type I can be identifi ed by newborn screening only when succinylacetone is used as the primary marker (delta-aminolevulinic acid is also used as a primary marker in urine), since tyrosine is not usually elevated in the newborn period in these patients [ 21– 23 ] .
Therapy consists of a diet low in tyrosine and phenylalanine (the precursor of tyrosine) and NTBC (2-(2-nitro-4-trifl uoro-methylbenzoyl)-1,3-cyclohexanedione), an inhibitor of 4-hydroxyphenylpyruvate dioxygenase, the enzyme located upstream of fumarylacetoacetate hydrolase. NTBC prevents the synthesis of succinylacetone that disappears almost immediately from the urine organic acids after initiation of treatment. The adequacy of the diet is monitored by plasma amino acids. The mea-surement of alpha-fetoprotein is also used to monitor these patients since liver can-cer is a complication of this condition. Liver transplantation is indicated in patients progressing to liver failure or with liver cancer [ 20 ] .
DNA Testing
The diagnosis of tyrosinemia type I is usually confi rmed by DNA testing. This is much less invasive than measurement of enzyme activity in a liver biopsy. Targeted mutation analysis (c.1062+5G>A/IVS12+5G>A; c.554-1G>T/IVS6-1G>T; c.607-6T>G/IVS7-6T>G; and p.P261L) is fi rst performed, followed by full gene sequenc-ing in case mutations have not been identifi ed and the diagnosis is still clinically considered. The above panel will also identify the most common mutations in peo-ple of French-Canadian descent (c.1062+5G>A/IVS12+5G>A) and in Ashkenazi Jews (p.P261L) [ 24– 28 ] .
Homocystinuria
Homocystinuria can be caused by several genetically different disorders. Methionine is converted into homocysteine through a series of S-adenosyl intermediates [ 29, 30 ] . Homocysteine condenses with serine via cystathionine beta-synthase to form cystathionine, which is then converted by cystathionase into cysteine. This pathway is also called the transsulfuration pathway. Homocysteine can also be remethylated back to methionine by the enzyme methionine synthase, which requires methylfo-late and methylcobalamin as cofactors. Defects in transsulfuration or remethyla-tion of homocysteine cause homocystinuria. The most common form is classic homocystinuria and is caused by reduced activity of cystathionine beta-synthase.

1718 Newborn Screening for Metabolic Disorders
The incidence is approximately 1:200,000 to 1:350,000 live births, with the highest incidence in Qatar (1:1,800) [ 31, 32 ] . Clinical manifestations include failure to thrive, developmental delay, downward dislocation of the lens, myopia, bone abnor-malities with marfanoid habitus and pectus excavatum, osteoporosis, mental retar-dation, and psychiatric disturbances. Thromboembolic episodes can be seen even in children and are a major cause of morbidity and mortality.
The biochemical diagnosis is made when plasma amino acids analysis shows increased plasma concentrations of methionine (especially in children) and the presence of free homocystine, a homodimer derived from two molecules of homocysteine. Total plasma homocysteine (free and peptide-bound homo-cysteine) is also markedly increased in this condition. Defects of homocysteine remethylation such as 5,10-methylene-tetrahydrofolate reductase defi ciency, methionine synthase (cblG) and methionine synthase reductase (cblE) defi ciency, and 5-methyl-tetrahydrofolate-homocysteine-methyltransferase defi ciency are characterized by markedly elevated total plasma homocysteine and free homo-cystine; however, in these conditions, the concentration of methionine is reduced. Methylcobalamin is a cofactor of methionine synthase; therefore, severe defi -ciency of vitamin B12 or defects in its metabolism (cb lC, cblD, cblF, and cblH) will result in homocystinuria . Patients with cblC and cblF and some patients with cblD defects also have an impairment in the synthesis of adenosylcobalamin, the cofactor of methylmalonyl-CoA mutase, and have combined methylmalonic acidemia/homocystinuria [ 33 ] .
The newborn screening marker for classic homocystinuria is elevated methion-ine. There are many different causes for elevated methionine in the newborn period, such as liver disease or liver immaturity, protein-rich diet, and other rare disorders of methionine metabolism (S-adenosylhomocysteine hydrolase defi ciency, glycine N-methyltransferase defi ciency, methionine adenosyltransferase (MAT) defi ciency). In these latter cases, homocystine is absent and total plasma homocysteine is normal or only mildly increased. Depending on the cutoff used by the screening laborato-ries for methionine, classic homocystinuria may be missed because the concentra-tion of methionine increases gradually, and it may not be abnormal at the time of the fi rst newborn screen. Homocystinuria caused by defects in remethylation of homo-cysteine can be identifi ed by newborn screening by very low concentrations of methionine [ 34 ] . Defi nitive confi rmation of diagnosis requires DNA testing for most of these conditions. Complementation studies in fi broblasts may be required to identify the specifi c cause of a cobalamin synthetic defect.
Treatment of classic homocystinuria requires a low-methionine, low-protein diet, high doses of pyridoxine (the cofactor of cystathionine beta-synthase), and admin-istration of betaine that facilitates the remethylation of homocysteine by donating a methyl group. Defects of vitamin B12 metabolism require high doses of intramus-cular hydroxycobalamin and oral betaine [ 33 ] . Mild genetic variations in the meth-ylenetetrahydrofolate reductase gene are frequent in the general population and are responsible for mild elevation of total plasma homocysteine, a risk factor for vascular disease [ 35 ] and neural tube defects [ 36 ] . These genetic variations are not identifi ed by newborn screening.

172 M. Pasquali and N. Longo
DNA Testing
Over 150 mutations have been reported in the cystathionine beta-synthase ( CBS ) gene ( http://cbs.lf1.cuni.cz/index.php ) [CBS Mutation Database]. Several of these mutations are common or regional, although many of them are private [ 30 ] . One of the mutations especially common in Northern Europe and in the United States is the B6-responsive p.I278T mutation, while the p.G307S mutation frequently identifi ed in Ireland is not. Diagnostic confi rmation is important to exclude other disorders causing elevated methionine levels and sometimes to predict B6 responsiveness. Full gene sequencing identifi es more than 95% of causative mutations. Targeted mutation analysis for p.I278T and p.G307S can identify less than 50% of mutations in affected patients.
Different genes are involved in disorders of homocysteine remethylation leading to homocystinuria [ 33 ] . Biochemical studies and complementation studies in fi broblasts should be performed to identify the defect prior to DNA analysis. The genes for all of these conditions have been identifi ed [ 33 ] , and DNA testing is available for the most frequent types (cblC, cblD, MTHFR), whereas testing for other more rare variants (cblE, cblF, cblG) is only available at selected centers. It must be noted that there are still other genes in the metabolism of vitamin B12 that remain to be identifi ed.
Maple Syrup Urine Disease
Maple syrup urine disease derives its name from the characteristic odor of the urine of these patients due to the presence of branched-chain keto acids (keto-methylval-eric, keto-isocaproic, keto-isovaleric). The disease is caused by impaired activity of branched-chain a -keto acid dehydrogenase (BCKD), a complex enzyme requiring thiamine pyrophosphate as a cofactor [ 37 ] , involved in the metabolism of the essen-tial branched-chain amino acids leucine, isoleucine, and valine. The BCKD com-plex is composed of four subunits, E
1 a , E
1 b , E
2 , and E
3 . The E
3 subunit is shared by
two other dehydrogenases, pyruvate dehydrogenase and a -ketoglutarate dehydro-genase [ 37 ] . A defect of any component of the complex causes maple syrup urine disease (MSUD), an autosomal recessive disorder with an incidence of approxi-mately 1:250,000 live births. There are several forms of this disease, depending on the severity of the mutations: (a) the classic form, which is the most severe and is characterized by very high plasma concentrations of branched-chain amino acids; (b) forms responsive to pharmacological amounts of thiamine (thiamine-responsive MSUD) [ 38 ] ; (c) intermediate or intermittent forms triggered by high consumption of proteins or catabolic state; and (d) E3 defi ciency with combined defi ciency of pyruvate and a -ketoglutarate dehydrogenase [ 39 ] .
Classic MSUD presents, following a normal birth and uneventful fi rst few days of life, with poor feeding and vomiting followed by lethargy and coma. The increased concentrations of branched-chain amino acids, especially leucine, become toxic. Leucine accumulates within the brain causing cerebral edema which is responsible

1738 Newborn Screening for Metabolic Disorders
for the progressive worsening of neurological symptoms. Routine laboratory tests may show only the presence of ketones in the urine.
Depending on the mutation and residual enzyme activity, some patients can pres-ent with recurrent episodes of vomiting, developmental delays, and seizures even after 1 year of age. In the intermittent form of the disease, patients may have epi-sodes of acute decompensation with vomiting, ataxia, and lethargy progressing to coma. They may or may not return to a normal status after recovery [ 39 ] .
Newborn screening can identify an elevated concentration of leucine/isoleucine with normal concentrations of other amino acids (such as phenylalanine) whose metabolism is not affected. However, patients with milder forms of the disease can be missed by screening [ 40 ] . The diagnosis of MSUD is confi rmed by plasma amino acid analysis that shows marked elevation of leucine (usually the prominent amino acid), isoleucine, and valine in addition to the pathognomonic presence of L-alloisoleucine. Urine organic acids show the presence of characteristic branched-chain keto acids and increased excretion of 2-hydroxyisovaleric acid during episodes of decompensation.
The therapy consists of a low-leucine and low-protein diet. Supplementation with valine and isoleucine may be necessary. Some patients improve with pharma-cological doses of thiamine.
DNA Testing
MSUD can be caused by mutations in any of three genes that encode components of the BCKD complex (E1alpha, E1beta, and E2) [ 41– 44 ] . Mutations in the E3 subunit produce a different phenotype that is not usually confused with MSUD. The geno-type has prognostic value to some extent; therefore, DNA analysis is important to predict long term outcome and treatment adherence. DNA testing can allow for pre-natal studies if the proband’s genotype is known. In general, diagnosis is confi rmed by enzyme assay in cultured skin fi broblasts. Western blot analysis in fi broblasts can sometimes identify the defective protein and direct subsequent DNA testing. Full gene sequencing of the genes encoding the E1alpha, E1beta, and E2 subunits is usu-ally necessary, starting from the one suggested by the results of Western blot analysis. In selected populations with a high frequency of MSUD due to a founder effect, targeted mutation analysis can be used as a fi rst-line DNA testing.
Urea Cycle Defects
Amino acids are metabolized to gluconeogenic and/or ketogenic precursors after their amino group has been disposed of by the urea cycle through several enzymes and mitochondrial transporters (Fig. 8.1 ). The ammonia generated from the nitro-gen groups of the amino acids is used in conjunction with CO
2 , ATP, and the enzyme

174 M. Pasquali and N. Longo
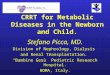
carbamyl phosphate synthase 1 (CPS-1) to generate carbamyl phosphate. The allosteric activator of CPS-1 is N-acetylglutamate, which is synthesized by N-acetylglutamate synthase (NAGS). Carbamyl phosphate combines with ornithine, which enters the mitochondria through the specifi c transporter ORC1, by the action of the enzyme ornithine transcarbamylase (OTC). This reaction generates citrulline, which exits the mitochondria through the ORC1 transporter (ornithine/citrulline exchanger) [ 45 ] . Aspartate, exported from mitochondria by the citrin transporter (aspartate/glutamate exchanger), combines with citrulline in the cytoplasm to form arginino-succinate through the enzyme argininosuccinate synthase (ASS). Argininosuccinate lyase (ASL) converts argininosuccinate into arginine and fumarate. In the last step of the urea cycle, arginase (ARG) generates urea and ornithine to restart the cycle. Defects in any of these enzymes or transporter will result in a block of the urea cycle and hyperammonemia. Newborn screening can identify elevated citrulline in citrul-linemia type I (ASS defi ciency) or II (citrin defi ciency) and, in addition to arginino-succinate, in argininosuccinate lyase defi ciency (ASL defi ciency) and elevated arginine in arginase defi ciency. Elevated ornithine and homocitrulline are theoreti-cally the markers for hyperammonemia, hyperornithinemia, and homocitrullinuria syndrome (ORC1 defi ciency/HHH syndrome), but it is unclear whether newborns with this condition show elevations of these amino acids. Low citrulline and arginine with elevated glutamine can be found in NAGS, CPS-1, and OTC defi ciency; however,
CYTOSOL
ASA synthase
ASA lyase
ArginaseORC1
ORC1
CITRINaspartate + citrulline
argininosuccinicacid
arginine
fumarate
UREA
CPS
ornithine
orotic acid
UTP CTP
N-acetyl-glutamate
aspartate
MITOCHONDRION
CO2+NH3+2ATP carbamylphosphateCPS-1
(HHH)
acetyl-CoA+glutamateNAG synthase
OTCcitrulline
+ornithine
Fig. 8.1 The urea cycle. The urea cycle leads to the formation of urea starting from ammonia (NH3). It requires many enzymes and mitochondrial transporters, any of which can be defective and impair the function of the urea cycle. Argininosuccinate lyase: ASA lyase ( ASL ); argininosuc-cinate synthase: ASA synthase ( ASS ); arginase: ARG ; aspartate/glutamate exchanger: citrin; car-bamyl phosphate: CP ; carbamyl phosphate synthase 1: CPS-1 ; cytidine triphosphate: CTP ; N-acetylglutamate ( NAG ) synthase ( NAGS ); ornithine/citrulline mitochondrial transporter: ORC1 ; ornithine transcarbamylase: OTC ; uridine triphosphate: UTP

1758 Newborn Screening for Metabolic Disorders
newborn screening by MS/MS has not allowed yet the consistent identifi cation of these disorders [ 46 ] .
Patients with urea cycle defects may present at any age [ 47, 48 ] , shortly after birth or later in infancy or adulthood. The pathophysiology is due to hyperammone-mia and the accumulation of glutamine in the brain leading to poor feeding, vomit-ing, and lethargy progressing to coma and death. The late onset presentation is often triggered by excess protein intake or catabolic state. In arginase defi ciency, the clinical picture is of spastic diplegia frequently diagnosed as cerebral palsy [ 49 ] , while hyperammonemia is not a consistent fi nding.
The dominant laboratory fi ndings in urea cycle defects are hyperammonemia and abnormalities of liver functions, with variably elevated transaminases and PT/PTT. Plasma amino acids, urine orotic acid, and, in some cases, urine amino acids are necessary for the diagnosis of these disorders. In the differential diagnosis of a patient with hyperammonemia, other conditions, such as organic acidemias and fatty acid oxidation defects, need to be considered. They can be excluded by urine organic acids and plasma acylcarnitine analyses. The treatment of urea cycle defects consists of a low-protein diet, in addition to scavengers (benzoate, phenylacetate, phenylbutyrate) that combine mainly with glutamine and glycine and facilitate their excretion, reducing the nitrogen pool. Citrulline (in OTC or CPS-1 defi ciencies) and/or arginine (in ASS and ASL defi ciencies) supplementation provides substrates of the urea cycle downstream from the specifi c block to allow protein synthesis to resume [ 47, 48 ] . Citrullinemia type II (citrin defi ciency) can present in the neonatal period as neonatal intrahepatic cholestasis. Infants with citrin defi ciency often have elevated galactose, methionine, and/or phenylalanine in their newborn screen. Citrulline may not be elevated in the fi rst days after birth, when the newborn screen is collected, but increases with time. The treatment for citrin defi ciency, different from the other urea cycle defects, consists of a high-protein diet [ 50– 56 ] . For this reason, it is very important to differentiate citrullinemia type I from type II. DNA analysis is currently the best procedure for this task.
DNA Testing
DNA testing should be directed by the biochemical fi ndings. Unfortunately, proxi-mal disorders of the urea cycle (ornithine transcarbamylase defi ciency, carbamyl phosphate synthetase 1 defi ciency, and N-acetyl glutamate synthase defi ciency) present the same biochemical fi ndings, although the urinary excretion of orotic acid is increased only in OTC defi ciency. Some of the urea cycle enzymes are expressed only in the liver; therefore, enzyme assays can be performed only on a liver biopsy. For this reason, DNA testing is becoming the procedure of choice to confi rm the diagnosis.
Outside of close communities, there are no predominant mutations, and, in most patients, full gene sequencing is the procedure of choice. One of the challenges in the past few years has been the identifi cation of patients with a mild form of

176 M. Pasquali and N. Longo
citrullinemia type I. These patients have only mild but persistent elevation of citrulline levels. It is still unclear whether they require therapy or not. DNA testing in these patients usually reveals at least one missense mutation either of unknown clinical signifi cance or associated with signifi cant residual enzyme activity. It is important to follow these patients over time since liver failure might develop even in adult age in citrullinemia type I [ 57 ] .
In the case of arginase defi ciency, the enzyme is expressed in red blood cells and can be assayed prior to DNA testing.
Organic Acidemias
Organic acidemias are inborn errors of metabolism characterized by the accumula-tion of intermediates in the catabolic pathways of amino acids.
The onset of symptoms is usually in the fi rst 48–72 h of life with vomiting, refusal of feeds, and lethargy progressing to coma. The accumulation of organic compounds results in metabolic acidosis (pH = 6.85–7.30) with low bicarbonate (<5–15 mEq/L), sometimes hyperammonemia, and a signifi cant anion gap. The biochemical diagnosis of organic acidemias is accomplished by urine organic acid analysis in addition to plasma amino acids and plasma acylcarnitine analysis. Table 8.3 lists selected organic acidemias identifi able by newborn screening and the strategy for confi rming or excluding the diagnosis.
Disorders of Propionate Metabolism
Propionyl-CoA is an intermediate in the catabolism of isoleucine, valine, threonine, methionine, pyrimidines (uracil and thymine), and cholesterol, and is the fi nal prod-uct of the b -oxidation of odd-chain fatty acids. Propionyl-CoA is converted by the biotin-dependent propionyl-CoA carboxylase to methylmalonyl-CoA, which is then converted to succinyl-CoA by an adenosylcobalamin-dependent mutase (methyl-malonyl-CoA mutase, MUT), for oxidation in the tricarboxylic acid cycle (Fig. 8.2 ) [ 58 ] . Primary or secondary defects of these two enzymes (propionyl-CoA carboxy-lase and methylmalonyl-CoA mutase) were among the fi rst organic acidurias to be discovered and the most commonly clinically diagnosed [ 58 ] .
The incidence of propionic acidemia is 1:35,000 to 1:75,000, while the incidence of methylmalonic acidemias is 1:48,000. Patients present typically after an uncom-plicated pregnancy and birth in the fi rst few days of life with vomiting, lethargy, coma, severe metabolic acidosis, hyperammonemia, often neutropenia, and thrombocytopenia.
Complications of these disorders include cardiomyopathy (mostly in propionic acidemia), acute and chronic pancreatitis, and progressive renal failure (in methyl-malonic acidemia) [ 58 ] . Patients who survive the initial event have developmental delay, hypotonia or hypertonia, and variable cognitive and neurological sequelae

1778 Newborn Screening for Metabolic Disorders
Tabl
e 8.
3 D
iagn
ostic
str
ateg
y an
d D
NA
test
ing
in s
elec
ted
orga
nic
acid
emia
s id
entifi
abl
e by
new
born
scr
eeni
ng
Dis
ease
G
ene
New
born
sc
reen
ing
Bio
chem
ical
fi nd
ings
E
nzym
e as
say
Firs
t-lin
e D
NA
test
ing
Add
ition
al
DN
A te
stin
g
Prop
ioni
c ac
idem
ia
(PR
OP)
P
CC
A
PC
CB
�
C3
� M
ethy
lcitr
ic a
cid
(UO
A)
Whi
te b
lood
cel
ls,
fi bro
blas
ts
Full
gene
seq
uenc
ing
NA
Met
hylm
alon
ic a
cide
mia
(m
utas
e, r
acem
ase,
cb
lA, c
blB
)
MU
T
MC
EE
M
MA
A
MM
AB
� C
3 �
C4D
C
� M
ethy
lmal
onic
aci
d (U
OA
) Fi
brob
last
s (c
ompl
emen
ta-
tion
stud
ies)
Full
gene
seq
uenc
ing
dire
cted
by
fi bro
blas
t res
ults
NA
Isov
aler
ic a
cide
mia
(I
VA
) IV
D
� C
5 �
Isov
aler
ylgl
ycin
e (U
OA
, uri
ne
acyl
glyc
ines
) Fi
brob
last
s Fu
ll ge
ne s
eque
ncin
g N
A
3-M
ethy
lcro
tony
l-C
oA
carb
oxyl
ase
defi c
ienc
y (3
MC
C)
MC
CA
M
CC
B
� C
5-O
H
� 3-
Hyd
roxy
isov
aler
ic a
cid
and
3-m
ethy
lcro
tony
l gly
cine
(U
OA
) W
hite
blo
od c
ells
, fi b
robl
asts
Fu
ll ge
ne s
eque
ncin
g N
A
3-H
ydro
xy-3
-m
ethy
lglu
tari
c ac
idur
ia (
HM
G)
HM
GC
L
� C
6-D
C
� C
5-O
H
� 3-
OH
-3-m
ethy
lglu
tari
c ac
id,
3-m
ethy
lglu
taco
nate
, 3-
OH
-iso
vale
rate
, and
3-m
ethy
l-gl
utar
ate
(UO
A)
Whi
te b
lood
cel
ls,
fi bro
blas
ts
Full
gene
seq
uenc
ing
NA
Hol
ocar
boxy
lase
sy
ntha
se d
efi c
ienc
y (M
CD
)
HL
CS
� C
5:1
� C
3 �
C5-
OH
� 3-
Hyd
roxy
isov
aler
ate,
3-m
ethy
l-cr
oton
ylgl
ycin
e, 3
-hyd
roxy
-pr
opio
nate
, met
hylc
itrat
e, la
ctat
e,
and
tigly
lgly
cine
Whi
te b
lood
cel
ls,
fi bro
blas
ts
Full
gene
seq
uenc
ing
NA
3-K
etot
hyol
ase
defi c
ienc
y ( b
KT
) A
CA
T1
� C
5-O
H
� C
5:1
� 2-
Met
hyl-
3-hy
drox
ybut
yrat
e,
2-m
ethy
lace
toac
etat
e, a
nd
tigly
lgly
cine
(U
OA
)
Fibr
obla
sts
Full
gene
seq
uenc
ing
NA
Glu
tari
c ac
idem
ia ty
pe I
(G
A-I
) C
GC
DH
�
C5D
C
� 3-
Hyd
roxy
glut
aric
and
glu
tari
c ac
id (
UO
A)
Fibr
obla
sts
Full
gene
seq
uenc
ing
NA
PAA
pla
sma
amin
o ac
ids,
UO
A u
rine
org
anic
aci
ds

178 M. Pasquali and N. Longo
Propionyl CoA D-Methylmalonyl CoA
L-Methylmalonyl CoA
SuccinylCoA
COOHCOOHCOOH
CH3CH3
CO2
CH2 CH3
H3C-CHHC-CH3
CO-S-CoACO-S-CoACO-S-CoACO-S-CoA
Biotin Adenosyl B12Propionyl CoAcarboxylase
MethylmalonylCoA racemase
MethylmalonylCoA mutase
ATP
Propionic acid + CO2 +ATP=Succinyl CoA+ADP
Fig. 8.2 Metabolism of propionic acid. Propionyl-CoA, derived from the catabolism of the amino acids threonine, valine, isoleucine, and methionine; odd-chain fatty acids; cholesterol; and nucle-otides is converted to succinyl-CoA that can enter the Krebs cycle
that are linked to the number and severity of acute episodes. There are milder forms of these conditions in which patients can develop neurological deterioration in childhood, sometimes without any acute episode of decompensation.
Newborn screening can identify elevated C3-carnitine in both propionic and methylmalonic acidemia, with higher concentrations usually seen in propionic aci-demia. Infants of mothers with severe vitamin B12 defi ciency are identifi ed also by elevated C3-carnitine with newborn screening. Diagnosis is confi rmed by urine organic acids, measurement of vitamin B12 (in the mother and child), plasma amino acids, and total plasma homocysteine (to exclude combined methylmalonic aci-demia/homocystinuria observed in a proximal defect of vitamin B12 metabolism, cblC, cblF, and some forms of cblD). Treatment is based on restriction of precursor amino acid and supplementation with carnitine and cofactors – biotin or hydroxyco-balamin – as indicated.
DNA Testing
An elevated level of C3 on the newborn screening can be caused by many different possibilities. The most common cause is maternal vitamin B12 defi ciency that can be excluded by measuring vitamin B12 levels in the mother and in the infant.
Propionic acidemia is caused by a defi ciency of propionyl-CoA carboxylase, a heteropolymeric mitochondrial enzyme composed of alpha- and beta-subunits encoded by the PCCA and PCCB genes, respectively. The diagnosis is usually con-fi rmed biochemically by the presence of methylcitric acid in urine, derived from the condensation of propionic acid with oxaloacetate. The enzyme is expressed in white blood cells and fi broblasts, and enzyme assay can easily confi rm the diagnosis. Mutations in both the PCCA and PCCB genes have been identifi ed in patients with propionic acidemia. There is great variability in mutations observed in the PCCA gene, especially in Caucasians, with none prevalent, while in the Japanese population,

1798 Newborn Screening for Metabolic Disorders
three mutations account for more than half of the alleles studied [ 59 ] . For the PCCB gene, a limited number of mutations are responsible for the majority of the alleles characterized in both Caucasian and Oriental populations. There is genotype-phe-notype correlation, and patients homozygous or compound heterozygous for null alleles have an earlier and more severe phenotype [ 60 ] .
In methylmalonic acidemia, methylmalonic acid is signifi cantly increased in the urine organic acid analysis and may be accompanied by elevated methylcitric acid. This condition can be caused by mutation in the methylmalonyl-CoA mutase and racemase [ 61, 62 ] genes and in several defects of vitamin B12 metabolism (cblA, cblB, cblC, cblD, cblF, cblF-like) [ 33 ] , some of which are also associated with homocystinuria due to defective homocysteine remethylation (cblC, cblF, cblF-like, and some forms of cblD) [ 33 ] . For this reason, a persistent increase in the concen-tration of methylmalonic acid not explained by defi ciency of vitamin B12 should be investigated by complementation studies in fi broblasts. Subsequently, DNA analy-sis can defi nitively establish the diagnosis.
Isovaleric Acidemia
Isovaleric acidemia (IVA) is a disorder of leucine catabolism caused by defi ciency of isovaleryl-CoA dehydrogenase [ 63 ] .
The clinical presentation can be with severe metabolic acidosis and hyperam-monemia leading to death shortly after birth. Milder variants can be completely asymptomatic or present with vomiting and failure to thrive, evolving into acute presentation triggered by fever or other illnesses. IVA is identifi ed by elevated C5-carnitine in the newborn screening. The diagnosis is confi rmed by urine organic acids and urine acylglycines analysis showing elevated isovalerylglycine and ele-vated 3-hydroxy-isovaleric acid in the untreated patients. In several patients identi-fi ed by newborn screening, the excretion of isovalerylglycine is only moderately elevated; in many cases, these patients carry a missense mutation (c.932C>T, p.A282V) associated with residual enzyme activity [ 63 ] . Treatment requires a low-protein diet, special formulas without leucine, glycine (250 mg/kg/day), and carnitine (50–100 mg/kg/day) supplements. The prognosis is usually good if acute metabolic decompensation is prevented.
DNA Testing
The biochemical profi le observed in the urine organic acids is usually characteristic for this condition. However, DNA testing by full gene sequencing confi rms the diagnosis and defi nes the presence of mutations associated with the milder outcome, possibly not requiring strict therapy. Enzyme assay in fi broblasts can be obtained but remains diffi cult to perform.

180 M. Pasquali and N. Longo
3-Methylcrotonyl-CoA Carboxylase Defi ciency
3-Methylcrotonyl-CoA carboxylase is a biotin-dependent mitochondrial enzyme involved in the catabolism of leucine [ 64, 65 ] converting 3-methylcrotonyl-CoA to 3-methylglutaconyl-CoA. This enzyme is composed of a larger alpha-subunit that binds biotin, bicarbonate, and ATP and a smaller beta-subunit containing the binding site for 3-methylcrotonyl-CoA [ 66, 67 ] , encoded by two different genes, MCCA and MCCB . Defi ciency of 3-methylcrotonyl-CoA carboxylase is inherited as an autosomal recessive trait, and heterogeneous mutations in the MCCA and MCCB genes have been reported in affected patients [ 68 ] . Patients have variable phenotypes, ranging from neurological involvement and developmental delays, to recurrent attacks of metabolic decompensation followed by complete recovery, to asymptomatic adults [ 68– 73 ] ; there is no clear correlation between genotype and phenotype [ 68 ] . Treatment consists of fasting avoidance and prompt treat-ment of fever and illnesses with IV fl uids containing glucose. Carnitine supple-ments are also indicated since most of these patients develop severe carnitine defi ciency.
Patients with 3-methylcrotonyl-CoA carboxylase defi ciency can be identifi ed through newborn screening by MS/MS because of an increased concentration of C5-OH (3-hydroxyisovaleryl-carnitine) [ 69, 74, 75 ] . Newborn screening has also identifi ed asymptomatic affected mothers of heterozygous babies [ 69 ] . Some of these mothers had a history of recurrent vomiting requiring IV fl uids after minor illnesses or high-protein meals [ 69 ] . Diagnosis is confi rmed by urine organic acid analysis showing a markedly increased excretion of 3-hydroxyisovaleric acid and the presence of 3-methylcrotonylglycine that increases during episodes of acute decompensation.
Urine acylglycine analysis might help in cases where 3-methylcrotonylglycine is only mildly elevated. Quantitative analysis of acylcarnitine profi les in plasma and urine provides further supporting evidence, showing a marked increase in C5-OH carnitine and the absence of other acylcarnitine species seen in other disorders such as 3-ketothiolase defi ciency, 3-hydroxy-3-methylglutaryl-CoA lyase defi ciency, or multiple carboxylase defi ciency. An isolated increase in C5-OH carnitine can be seen with biotinidase defi ciency that can be easily excluded by measurement of serum enzyme activity. The diagnosis is confi rmed by measuring enzyme activity in white blood cells.
DNA Testing
Full gene sequencing of both the MCAA and MCCB genes is clinically available. However, since there is an easy enzyme assay in white blood cells, this procedure is rarely used for diagnostic confi rmation.

1818 Newborn Screening for Metabolic Disorders
3-Hydroxy-3-Methylglutaric Aciduria
3-Hydroxy-3-methylglutaric aciduria is a disorder of ketogenesis and L-leucine catabolism caused by mutations in the 3-hydroxy-3-methylglutaryl-CoA lyase ( HMGCL ) gene. The clinical acute symptoms include vomiting, convulsions, meta-bolic acidosis, hypoketotic hypoglycemia, and lethargy, usually triggered by fasting or catabolic state resembling in many aspects a fatty acid oxidation defect rather than an organic acidemia. Urine organic acids show elevated excretion of 3-hydroxy-3-methylglutaric acid, 3-methylglutaconic acid, and 3-methylglutaric acid, with occa-sional elevation of 3-hydroxyisovaleric acid and 3-methylcrotonylglycine; ketone bodies are not (or only minimally) increased. In the plasma acylcarnitine profi le, there is characteristic elevation of 3-methylglutarylcarnitine (C6-DC) in addition to elevated C5OH-carnitine. Treatment consists of fasting avoidance, prompt treatment of decompensation with IV solution containing glucose, cornstarch and carnitine supplements as needed, and a diet moderately restricted in leucine.
DNA Testing
Heterogeneous mutations in the HMGCL gene have been reported in affected patients, and full gene sequencing is the procedure of choice to confi rm the diag-nosis [ 76 ] . Enzyme assay, although effective, is not easily available.
Holocarboxylase Synthase Defi ciency
Holocarboxylase synthase defi ciency (or multiple carboxylase defi ciency, MCD) leads to impaired activity of four biotin-dependent enzymes: acetyl-CoA carboxy-lase, propionyl-CoA carboxylase, 3-methylcrotonyl-CoA carboxylase, and pyruvate carboxylase (Fig. 8.3 ). This enzyme attaches biotin covalently to the active site of the different carboxylases. The clinical symptoms include feeding and breathing diffi culties, hypotonia, seizures, and lethargy, and there sometimes is progression to developmental delay or coma. Some children exhibit skin rash and alopecia. Affected children exhibit metabolic acidosis, organic aciduria, and mild to moderate hyperammonemia. The organic aciduria includes elevated concentrations of 3-hydroxyisovalerate, 3-methylcrotonylglycine, 3-hydroxy-propionate, methylci-trate, lactate, and tiglylglycine, refl ecting impaired activity of biotin-dependent enzymes. Plasma acylcarnitines show increased C5:1, C3, C5-OH acylcarnitines. The enzyme defect has been demonstrated in lymphocytes, cultured fi broblasts, and cultured lymphoblasts from affected children. Therapy consists of the administra-tion of high doses (up to 100 mg twice a day) of oral biotin and prompt treatment of fever, infections, and catabolic state with intravenous fl uids containing glucose.

182 M. Pasquali and N. Longo
DNA Testing
Heterogeneous mutations have been identifi ed in patients with multiple carboxy-lase defi ciency. Specifi c mutations (such as c.1519+5G>A/IVS10+5G>A prevalent in the Faroe Islands; p.L237P and c.780delG predominant in Japanese patients) have ethnic predilection, but in general, full gene sequencing is required for diag-nostic confi rmation [ 77 ] . There is genotype-phenotype correlation; patients with two severe mutations have an earlier presentation, and patients with higher residual activity present after the neonatal period and show a better clinical response to bio-tin therapy.
3-Ketothiolase Defi ciency
3-Ketothiolase (mitochondrial acetoacetyl-CoA thiolase, T2) is an enzyme involved in isoleucine catabolism and ketone bodies utilization. Its defi ciency is characterized by intermittent episodes of severe ketoacidosis, usually with nor-moglycemia or hyperglycemia (for which it can be confused with diabetes melli-tus), that can result in hyperventilation, dehydration, lethargy, coma, and death. Episodes are usually associated with severe vomiting and are triggered by infec-tions or other illnesses. Analysis of urine organic acids during acute episodes reveals high excretion of 2-methyl-3-hydroxybutyrate, 2-methylacetoacetate, and tiglylglycine with large amounts of 3-hydroxy-butyrate and acetoacetate. Analysis of acylcarnitines by MS-MS in whole blood or in plasma shows increased concen-trations of C5-OH (2-methyl-3-hydroxybutyryl) carnitine and C5:1 (tiglyl) carni-tine. The diagnosis can be confi rmed by enzyme assay in cultured fi broblasts or more easily by DNA testing. Therapy consists of mild protein restriction to limit
FreeBiotin
DietaryBiotin
Holocarboxylases
ProteinRecycling
BiocytinAcetyl CoAPropionyl CoAPyruvateβ-Methylcrotonyl CoAcarboxylases
HolocarboxylaseSynthaseBiotinidase
Fig. 8.3 Biotin metabolism. Dietary biotin is attached to the epsilon amino group of lysine in proteins. After digestion, biocytin is generated and biotin can be detached by the action of biotini-dase. Free biotin can then be incorporated into the active site of carboxylase enzymes by the action of holocarboxylase synthase. When these enzymes are recycled, biocytin is generated again, and biotin can be recycled by the action of biotinidase

1838 Newborn Screening for Metabolic Disorders
the intake of isoleucine, avoidance of fasting, supplementation with carnitine, avoidance of prolonged fasting, and prompt treatment of illnesses that can precipi-tate acute attacks.
DNA Testing
The gene coding for this enzyme, ACAT1 , maps to 11q22.3-23.1, and heterogeneous mutations have been reported in patients with 3-ketothiolase defi ciency [ 78– 81 ] . Two groups of patients have been identifi ed based on the presence of null mutations in both alleles or of mutations leaving some residual activity in at least one of the mutant alleles [ 82, 83 ] . Although there is no correlation between phenotype and genotype, in patients with milder mutations, the biochemical phenotype can nor-malize between episodes [ 78, 82 ] . For this reason, full gene sequencing should be performed in dubious cases.
Glutaric Acidemia Type I
Glutaric acidemia type I (GA-I) is caused by a defect in the catabolic pathway of lysine, hydroxylysine, and tryptophan due to impaired activity of glutaryl-CoA dehydrogenase. Affected individuals may have macrocephaly at birth or develop it in the fi rst year of life [ 84 ] . They have mild hypotonia and they can develop acute dystonia and spasticity with metabolic decompensation, usually triggered by fever or other illnesses. Brain imaging of affected individuals demonstrates frontotempo-ral atrophy, and after a crisis, the characteristic striatal degeneration with shrinkage of the caudate and Putamen [ 84 ] . Hypotonia followed by spasticity, abnormal move-ments, seizures, mild hypoglycemia, and metabolic acidosis have also been associ-ated with acute events.
Diagnosis of this condition is confi rmed by urine organic acids showing massive excretion of glutaric and 3-hydroxyglutaric acids. This is associated with increased concentrations of glutarylcarnitine (C5-DC) in plasma and increased urinary excre-tion of glutarylcarnitine. Some patients, referred to as low excretors, show a more subtle biochemical phenotype with normal or mildly elevated glutaric acid and mildly increased excretion of 3-hydroxyglutaric acid [ 84 ] . In these patients, the concentration of plasma glutarylcarnitine can be normal, although they tend to have elevated urinary excretion of glutarylcarnitine [ 85 ] . Infants with GA-I have usually elevated glutarylcarnitine identifi able by newborn screening, although some low excretors can be missed. Glutaryl carnitine can also be elevated in patients with kidney failure, but usually in association with other acylcarnitine species.
The treatment consists of a diet restricted in lysine and tryptophan and carnitine supplementation. Prompt treatment of infections or other illnesses and prevention of metabolic decompensation is also critical in this disease.

184 M. Pasquali and N. Longo
DNA Testing
Full gene sequencing of the GCDH gene is the procedure of choice to confi rm the diagnosis in a patient with abnormal newborn screening when the biochemical phenotype is ambiguous. Enzyme assay in cultured fi broblasts is also available, but low excretors usually retain signifi cant residual enzyme activity, and differentiation from carriers is sometimes diffi cult.
Disorders of the Carnitine Cycle and Fatty Acid Oxidation
Carnitine plays an essential role in the transport of long-chain fatty acids inside mito-chondria for beta-oxidation. During periods of fasting or high energy demands, the main substrates for energy production in the liver, cardiac muscle, and skeletal muscle are fatty acids which are released by the adipose tissue. The brain cannot directly utilize fatty acids, because they cannot cross the blood–brain barrier; however, it can oxidize ketone bodies derived from beta-oxidation of fatty acids in the liver [ 86 ] . If fatty acid oxidation is impaired, fatty acids will still be released by the adipose tissue during fasting or high energy demands, but they will accumulate in the liver, heart, or skeletal muscle. In the liver, impaired oxidation of fatty acids will result in steatosis and decreased production of ketones. Ketones are used by the heart, skeletal muscle, and brain as energy source sparing glucose, while in the liver, the increased acetyl-CoA, derived from beta-oxidation of fatty acids stimulates gluconeogenesis (production of glucose), mostly from the carbon skeleton of amino acids released from the muscle. In patients with fatty acid oxidation disorders, the excessive utilization of glucose and lack of gluconeogenesis cause hypoglycemia that, in addition to decreased availability of ketones, decreases the energy supply for the brain causing loss of consciousness, seizures, and coma. Fats can also accumulate in the heart and skeletal muscle causing cardiomyopathy and myopathy in addition to fatal arrhythmias.
Long-chain fatty acids, released from the adipose tissue, travel in blood bound mostly to albumin. There is a complex system involving membrane transporters and vectorial acylation by the action of acyl-CoA synthase that drives fatty acids inside cells. Once inside the cell, the carnitine cycle is essential to allow fatty acids to enter mitochondria for subsequent beta-oxidation (Fig. 8.4 ). This cycle requires enzymes and transporters that accumulate carnitine within the cell (OCTN2 carnitine trans-porter), conjugate it with long-chain fatty acids to form long-chain acylcarnitines (carnitine palmitoyl transferase 1, CPT1), transfer the acylcarnitines across the inner plasma membrane (carnitine-acylcarnitine translocase, CACT), and conjugate the fatty acids back to coenzyme A for subsequent beta-oxidation (carnitine palmi-toyl transferase 2, CPT2). Medium- and short-chain fatty acids can cross the mito-chondrial membrane independently from the carnitine cycle. In the mitochondrial matrix, long-chain fatty acids undergo a series of enzymatic reactions to progressively shorten their chain by two carbon units (acetyl-CoA). Dehydrogenases with different carbon chain length specifi city (from C18 to C4, very-long-chain acyl-CoA dehydro-genase (VLCAD), long-chain acyl-CoA dehydrogenase (LCAD), medium-chain

1858 Newborn Screening for Metabolic Disorders
CH3
CH3
H3COH
COO−N
CH3
CH3
H3COH
COO−N
CH3
CH3
H3COH
COO−N+
CH3
CH3
H3COH
COO−N
CH3
CH3
H3CO
COO−N−
CARNITINE
OUT
INVectorialAcylation
Acyl-S-CoACOOH COOH
CoA CoA
CPT-1
FABPc ACBP
Caveolin
CoASH
PlasmaMembrane
MEDIUM CHAINDICARBOXYLIC ACIDS
PEROXISOMES
ω ,ω-1oxidationMICROSOMES
MITOCHONDRION
Acyl-S-CoA
β-OXIDATIONAcyl
CH3
CH3
H3CO
COO−N+
Acyl
CPT-2
CACT
ACS
FATP
COOH
COOH
COOH
FA
AlbuminFATTYACID
HOOC
CD36
FABP pm
OCTN2
Fig. 8.4 The carnitine cycle in fatty acid oxidation. The carnitine cycle is responsible for deliver-ing long-chain fatty acid to the mitochondrial matrix for subsequent beta-oxidation. Fatty acids are bound to albumin or other proteins in plasma. They enter the cells through fatty acid transporters ( FATP : fatty acid transporter protein) that interact with other proteins (membrane-bound fatty-acid-binding proteins (FABPpm), caveolin, CD-36) to allow the transfer of the fatty acid to the transporter. Once inside the cell, fatty acids are conjugated with coenzyme A by acyl-CoA syn-thases (ACS) maintaining a constant gradient for free fatty acid to fl ow from the outside to the inside of the cells. In the cytoplasm, free fatty acids attach to fatty-acid-binding proteins (FABPc) or acyl-CoA-binding proteins (ACBP). FA : fatty acid; CPT-1: carnitine palmitoyl transferase 1; CPT-2: carnitine palmitoyl transferase 2; CACT: carnitine-acylcarnitine translocase
acyl-CoA dehydrogenase (MCAD), and short-chain acyl-CoA dehydrogenase (SCAD)) introduce a double bond between C2 and C3. A trifunctional protein (TFP) adds water and cleaves two carbon atoms from the long-chain fatty acid. This is done through the sequential action of a hydratase (enoyl-CoA hydratase), a dehy-drogenase (long-chain 3-OH-acyl-CoA dehydrogenase, LCHAD), and a thiolase (acyl-CoA acetyltransferase). The two carbon units generated can be completely oxidized in the muscle to CO
2 or generate ketone bodies in the liver that can be
exported to provide energy to other organs. Defi ciency in any of these steps will lead to impaired energy production, in most
cases aggravated by fasting or catabolic state. The characteristics of disorders of the carnitine cycle and of fatty acid oxidation included in the core panel of conditions to be screened in the newborns are discussed in more detail below. Table 8.4 lists selected disorders of fatty acid oxidation identifi able by newborn screening and the strategy for confi rming or excluding the diagnosis.

186 M. Pasquali and N. Longo
Tabl
e 8.
4 D
iagn
ostic
str
ateg
y an
d D
NA
test
ing
in s
elec
ted
diso
rder
of
fatty
aci
d ox
idat
ion
and
the
carn
itine
cyc
le id
entifi
abl
e by
new
born
scr
eeni
ng
Dis
ease
G
ene
New
born
sc
reen
ing
Bio
chem
ical
fi nd
ings
E
nzym
e as
say
Firs
t-lin
e D
NA
te
stin
g A
dditi
onal
DN
A
test
ing
Car
nitin
e up
take
def
ect/
carn
itine
tran
spor
t def
ect
(CU
D)
SLC
22A
5
C0
C
0, C
3, C
16 (
free
and
to
tal c
arni
tine,
ac
ylca
rniti
nes)
Fibr
obla
sts
Full
gene
se
quen
cing
D
elet
ions
/du
plic
atio
ns
Ver
y-lo
ng-c
hain
acy
l-C
oA
dehy
drog
enas
e de
fi cie
ncy
(VL
CA
D)
AC
AD
VL
�
C14
:1
� C
14:1
(ac
ylca
rniti
nes)
C
an b
e no
rmal
Fi
brob
last
s (fl
uxe
s,
oxid
atio
n,
acyl
carn
itine
)
Full
gene
se
quen
cing
D
elet
ions
/du
plic
atio
ns
Lon
g-ch
ain
L-3
hyd
roxy
acyl
-C
oA d
ehyd
roge
nase
de
fi cie
ncy
(LC
HA
D)
HA
DH
A
� C
16-O
H
� C
18:1
-OH
�
C16
-OH
, C18
:1-O
H,
and
othe
r lo
ng-c
hain
ac
ylca
rniti
nes
Fibr
obla
sts
Targ
eted
m
utat
iona
l an
alys
is
Full
gene
se
quen
cing
Tri
func
tiona
l pro
tein
defi
-ci
ency
(T
FP)
HA
DH
A
HA
DH
B
� C
16-O
H
� C
18:1
-OH
�
C16
-OH
, C18
:1-O
H,
and
othe
r lo
ng-c
hain
ac
ylca
rniti
nes
Fibr
obla
sts
Full
gene
se
quen
cing
N
A
Med
ium
-cha
in a
cyl-
CoA
de
hydr
ogen
ase
defi c
ienc
y (M
CA
D)
AC
AD
M
� C
8 �
C8,
C6,
C10
:1
(acy
lcar
nitin
es)
� H
exan
oylg
lyci
ne
(UO
A, a
cylg
lyci
nes)
Fibr
obla
sts
Targ
eted
m
utat
iona
l an
alys
is
Full
gene
se
quen
cing
UO
A u
rine
org
anic
aci
ds, a
cylc
arni
tine
s pl
asm
a ac
ylca
rniti
ne p
rofi l
e, a
cylg
lyci
nes
urin
e ac
ylgl
ycin
e pr
ofi le

1878 Newborn Screening for Metabolic Disorders
Carnitine Uptake Defect (CUD)
Carnitine uptake defect or primary carnitine defi ciency (OMIM 212140) is an auto-somal recessive disorder of the carnitine cycle affecting fatty acid oxidation. It is due to the lack of functional OCTN2 carnitine transporter. Primary carnitine defi -ciency has a frequency of about 1:40,000 newborns in the general population, but it has a much higher incidence in the Faroe Islands (1:720) [ 87 ] . The lack of the plasma-membrane carnitine transporter results in urinary carnitine wasting, low serum carnitine concentrations (0–5 m M, normal 25–50 m M), and decreased intrac-ellular carnitine accumulation. Patients with primary carnitine defi ciency lose car-nitine in urine, resulting in decreased plasma concentration and subsequent tissue defi ciency. Patients can present with hepatic encephalopathy or cardiomyopathy triggered by fasting or infection. Some patients have been completely asymptomatic for all of their lives and have been diagnosed following the birth of an affected child [ 88 ] . Routine laboratory studies can show hypoglycemia with minimal or no ketones in urine, hyperammonemia with variably elevated liver function tests and, some-times, elevated creatine kinase. Newborn screening can identify reduced free carni-tine (C0) in blood spots. Low carnitine concentrations are also seen in infants of mothers with low carnitine due to carnitine uptake defect or secondary to an undi-agnosed organic acidemia or fatty acid oxidation defect. Diagnosis is further sus-pected by fi nding extremely reduced plasma concentration of free, total, and acylated carnitine (free carnitine < 9 m M, normal 25–50 m M) and relatively increased urinary excretion of free and total carnitine, with unremarkable urine organic acids. Diagnosis is confi rmed by demonstrating reduced carnitine transport (<10% of nor-mal) in skin fi broblasts or two mutations in the SLC22A5 gene encoding the OCTN2 carnitine transporter. Therapy consists of lifelong carnitine (100–300 mg/kg/day) supplementation.
DNA Testing
Heterogeneous mutations have been reported in different patients, and full gene sequencing is the recommended procedure for diagnosis. In some patients, DNA sequencing fails to identify the causative mutation, and measurement of carnitine transport remains the preferred procedure for diagnosis.
Very-Long-Chain Acyl-CoA Dehydrogenase Defi ciency
Very-long-chain acyl-CoA dehydrogenase (VLCAD) catalyzes the fi rst step of the fatty acid beta-oxidation spiral with optimal specifi city toward fatty acids with chains of 12–18 carbon atoms. Patients with VLCAD defi ciency can present in infancy with cardiomyopathy, cardiac arrest, hypoglycemia, and other hepatic symptoms.

188 M. Pasquali and N. Longo
This form is rapidly fatal. Older children can present with hypoketotic hypoglycemia and hepatomegaly with or without cardiomyopathy triggered by fasting, stress, and fever. The milder form presents in adolescents or adults with muscle weakness and pain, without cardiac and hepatic involvement, usually associated with exercise [ 89 ] . Routine laboratory testing during acute episodes reveals hypoketotic hypoglycemia and elevation of creatine kinase and transaminases. Elevated concentration of C14:1-carnitine in the fi rst newborn screen blood spot is often the only abnormality detected, and it may no longer be present in subsequent screens or diagnostic tests (plasma acylcarnitine profi le). For this reason, in all infants with elevated C14:1 carnitine on the newborn screening, the diagnosis of VLCAD defi ciency needs to be confi rmed or excluded by specifi c enzyme assay or fatty acid oxidation studies in vitro and/or by molecular genetic analysis of the ACADVL gene (encoding VLCAD) [ 90 ] . Therapy for this condition consists of avoidance of fasting, prompt treatment of infections, and a low-fat diet with medium-chain triglycerides providing most of the calories from lipids. Low-dose carnitine supplements (25 mg/kg/day) are sometimes given.
DNA Testing
Since there is no reliable biochemical indicator of the disease (plasma acylcarnitine profi le often normalizes in children not acutely stressed such as shortly after birth), DNA testing is essential to confi rm or exclude the diagnosis, especially in children identifi ed by newborn screening. The identifi cation of two mutations previously associated with VLCAD defi ciency or null alleles confi rms the diagnosis. In a few cases, mutations are found in cis on the same allele. For this reason, parental geno-typing is essential for diagnostic confi rmation. In other cases, variations of unknown signifi cance are identifi ed on one allele with a specifi c mutation on the other allele. In these cases, fatty acid oxidation fl uxes, oxidation, or acylcarnitine profi ling can determine the signifi cance of the novel variant and whether the child needs treatment or not. The severity of the phenotype correlates with the genotype [ 91 ] with earlier and more severe presentation observed in patients with the most severe defi ciency.
Trifunctional Protein and Long-Chain 3-Hydroxy-Acyl-CoA Dehydrogenase Defi ciencies
The trifunctional protein (TFP) is a heterooctamer containing four alpha- and four beta-subunits encoded by two different genes [ 92 ] . The alpha-subunit harbors the activities of the second and third steps of fatty acid beta-oxidation, long-chain enoyl-CoA hydratase (LCEH), and long-chain 3-hydroxy-acyl-CoA dehydrogenase (LCHAD). The beta-subunit harbors long-chain 3-ketoacyl-CoA dehydrogenase

1898 Newborn Screening for Metabolic Disorders
(LCKAT), which catalyzes the last step in beta-oxidation of long-chain fatty acids. There are three clinical phenotypes: (a) a severe neonatal presentation with cardio-myopathy, Reye-like symptoms, and early death; (b) a hepatic form with recurrent hypoketotic hypoglycemia; and (c) a milder, later-onset neuromyopathic phenotype with episodic myoglobinuria. Maternal HELLP syndrome can occur in mothers independent of the fetal phenotype [ 93 ] . Patients with LCHAD/TFP defi ciencies may also develop pigmentary retinopathy and a peripheral neuropathy, whose pathophysiology remains obscure. In addition, mothers of these patients can have signifi cant complications with acute fatty liver of pregnancy or hemolysis, elevated liver enzymes, and low platelets (HELLP) syndrome [ 94 ] .
Newborn screening can identify elevated C16:OH- and C18:1-OH-carnitines in blood spots of infants with LCHAD/TFP defi ciency. Plasma acylcarnitine profi le can identify the same abnormalities with the elevation of additional long-chain acyl-carnitines. Urine organic acids collected at the time of an acute episode can show hypoketotic C6-C10 dicarboxylic aciduria and C6-C14 3-hydroxydicarboxylic aci-duria with prominent unsaturated species. The urine organic acids rapidly normalize with therapy and are normal in asymptomatic patients. Therapy for these conditions consists of avoidance of fasting, prompt treatment of infections, a low-fat diet with medium-chain triglycerides providing most of the calories from lipids. Low-dose carnitine supplements (25 mg/kg/day) may be given.
DNA Testing
Mutations in either the HADHA or HADHB genes may cause complete TFP defi -ciency and a prevalent mutation in the HADHA gene encoding the alpha-subunit (c.1528 G>C, p.E474Q) causes isolated LCHAD defi ciency [ 93 ] . In this case, only part of the reaction occurs, and the intermediates that accumulate are toxic for the body. A genotype-phenotype correlation has also emerged for TFP defi ciency, with residual enzyme activity being associated with a milder, later-onset phenotype. In general, targeted mutation analysis is fi rst performed in a patient with an elevation of long-chain hydroxylated acylcarnitines, followed by full gene sequencing of the two genes to confi rm trifunctional protein defi ciency if the fi rst testing is normal. Unlike VLCAD defi ciency, abnormal acylcarnitines are almost always present in this condition, unless the child is under optimal treatment.
Medium-Chain Acyl-CoA Dehydrogenase Defi ciency
Medium-chain acyl-CoA dehydrogenase (MCAD) defi ciency is the most common disorder of fatty acid oxidation, with an estimated frequency of 1:6,000 to 1:10,000 Caucasian births [ 95, 96 ] . The symptoms of the disease are variable, from completely

190 M. Pasquali and N. Longo
asymptomatic to hypoglycemia, lethargy, coma, and sudden death; they are usually triggered by prolonged fasting or illness. Although the majority of patients present in the fi rst year of life, clinical symptoms can occur at any time, and patients can even die in the newborn period before diagnosis [ 97 ] . Patients with MCAD defi -ciency are identifi ed by MS/MS newborn screening because of the characteristic acylcarnitine profi le, with increased concentration of C6- (hexanoyl), C8- (octanoyl), and C10:1- (decenoyl) carnitine and elevated C8/C2 and C8/C10 ratios. Urine organic acids and urine acylglycines analyses during metabolic crisis show increased excretion of dicarboxylic acids (adipic, suberic, sebacic), saturated and unsaturated, little or absent ketones, and increased excretion of hexanoylglycine and suberylgly-cine. When patients are metabolically stable, the urinary concentration of these ana-lytes is greatly reduced, although hexanoylglycine and suberylglycine usually remain detectable. The abnormal plasma acylcarnitine profi le is almost always pres-ent. The treatment consists of avoidance of fasting, low-fat diet, carnitine supple-mentation, and institution of an emergency plan in case of illness or other metabolic stress. Early diagnosis through newborn screening and early initiation of treatment leads to improved outcome.
DNA Testing
The diagnosis can be confi rmed by DNA analysis. Among patients presenting with clinical symptoms, 98% carry at least one copy of the common mutation K304E (also known as p.K329E), with 80% being homozygous for this mutation [ 98 ] . In newborns detected prospectively by newborn screening, the Y42H (also known as p.Y67H) mutation has been found frequently in association with K304E [ 98 ] . The Y42H mutation has not yet been reported in patients with clinical symptoms [ 98 ] and is associated with lower concentrations of diagnostic metabolites in blood and urine [ 99 ] . In the presence of the characteristic abnormal acylcarnitine profi le and the absence of the two mutations above, DNA sequencing can usually identify both causative mutations.
Galactosemia
Galactosemia is a disorder of carbohydrate metabolism that results in the accumula-tion of galactose in blood. In theory, galactosemia can result in the defi ciency of one of three enzymes: galactose-1-phosphate-uridyltransferase defi ciency (GALT), galactokinase defi ciency (GALK), and epimerase defi ciency (GALE) (Fig. 8.5 ). Usually, we refer to GALT defi ciency as classic galactosemia, with inability to metabolize galactose to glucose [ 1 ] . Galactose derives from lactose in milk. This is digested by disaccharidases in the brush border of intestinal cells to generate glu-cose and galactose that enter cells by the action of the sodium-dependent glucose transport SGLT1. Galactose is then phosphorylated to galactose-1-phosphate by the

1918 Newborn Screening for Metabolic Disorders
action of galactokinase (GALK). Galactose-1-phosphate uridyl transferase (GALT) then transforms galactose-1-phosphate and UDP glucose to glucose-1-phosphate and UDP galactose. Finally, the epimerase (uridine diphosphate galactose-4-epim-erase, GALE) converts UDP galactose to UDP glucose. In classic galactosemia, elevated levels of galactose-1-phosphate are toxic for cells. Affected infants present at 3–14 days of age with poor feeding, vomiting, diarrhea, jaundice, lethargy pro-gressing to coma, and abdominal distension with hepatomegaly usually followed by progressive liver failure. Patients with galactosemia are also at increased risk for E. coli or other gram-negative neonatal sepsis. Diagnosis is made by measuring GALT enzyme activity in red blood cells. Treatment consists of the removal of galactose from the diet. Early identifi cation and intervention prevents most early and serious complications, although even with treatment some children develop speech dyspraxia and learning disabilities; girls may experience ovarian failure with primary amenorrhea or early menopause.
DNA Testing
The diagnosis of galactosemia is confi rmed by enzyme assay that can be performed in red blood cells. This is ideally integrated with concomitant DNA testing for com-mon mutations (p.Q188R, p.S135L, p.K285N, p.T138M, p.L195P, p.Y209C, and IVS2-2 A>G) and two variants (p.N314D and p.L218L). DNA testing is essential in distinguishing people who have Duarte-variant galactosemia, a condition in which there is signifi cant residual enzyme activity that usually requires no treatment or treatment for only the fi rst year of life [ 100 ] . These patients have the p.N314D vari-ant in association with a deletion in the promoter region of the gene markedly reducing gene expression and enzyme activity. The same p.N314D variant has been found in
DIET Galactitol+Galactonate
Galactose + ATP
Gal-1-P + UDPGlu Glu-1-P + UDPGal
Gal-1-P + ADP
Endogenous production
UDPGalactose UDPGlucose
uridine diphosphategalactose-4-epimerase
(GALE)
galactose-1-phosphateuridyl transferase (GALT)
galactokinase(GALK)
Galactose dehydrogenaseAldose reductase
Fig. 8.5 Galactose metabolism. Galactose is obtained from the diet or endogenous production. Galactokinase ( GALK ), galactose-1-phosphate uridyl transferase ( GALT ), and uridine diphosphate galactose-4-epimerase ( GALE ) are required for converting galactose into glucose

192 M. Pasquali and N. Longo
association with increased enzyme activity (in cis with the L218L variant and normal promoter activity, Los Angeles variant) and rarely in cis with mutations abolishing enzyme activity. For this reason, measurement of enzyme activity is essential to the correct interpretation of DNA testing. Full gene sequencing can identify mutations in patients with markedly reduced enzyme activity but no com-mon mutations.
Biotinidase Defi ciency
Biotinidase defi ciency is a disorder of biotin recycling that can cause seizures, hypotonia, ataxia, breathing problems, hearing loss, optic atrophy, developmental delay, skin rash, and alopecia. The clinical expression of the disorder is variable, with onset from weeks to several years of age. Therapy consists of the administra-tion of oral biotin for life. Biotinidase defi ciency can be identifi ed by newborn screening, using a colorimetric method. The disease is confi rmed by measurement of enzyme activity in serum.
DNA Testing
Biotinidase defi ciency can be complete or partial. In the complete defi ciency syn-drome, biotinidase activity is reduced to less than 10% of normal. This complete impairment is associated with mutations that completely abolish enzyme activity. Targeted mutation analysis (c.98_104del7ins3 (G98d7i3), p.Q456H, p.R538C, and the double mutation p.A171T:p.D444H) can identify a good percentage of the caus-ative mutations [ 101 ] . Partial biotinidase defi ciency is associated with signifi cant residual enzyme activity. In most cases, patients carry at least one copy of the p.D444H mutation that, without another change in cis, is associated with partial defi -ciency. Full gene sequencing can identify mutations in all other patients with absent enzyme activity and only one mutation detected by the common panel.
References
1. Guthrie R, Susi A. A simple phenylalanine method for detecting phenylketonuria in large populations of newborn infants. Pediatrics. 1963;32:338–43.
2. Chace DH. Mass spectrometry in newborn and metabolic screening: historical perspective and future directions. J Mass Spectrom. 2009;44(2):163–70.
3. Chace DH, Kalas TA. A biochemical perspective on the use of tandem mass spectrometry for newborn screening and clinical testing. Clin Biochem. 2005;38(4):296–309.
4. Newborn screening: toward a uniform screening panel and system. Genet Med. 2006;8 Suppl 1:1S–252S.

1938 Newborn Screening for Metabolic Disorders
5. SCID added to national newborn screening standards. Am J Med Genet A . 2010;152A(8):ix.
6. Ko DH, Jun SH, Park KU, Song SH, Kim JQ, Song J. Newborn screening for galactosemia by a second-tier multiplex enzyme assay using UPLC-MS/MS in dried blood spots. J Inherit Metab Dis. 2011;34(2):409–14.
7. Ko DH, Jun SH, Park HD, et al. Multiplex enzyme assay for galactosemia using ultraperfor-mance liquid chromatography-tandem mass spectrometry. Clin Chem. 2010;56(5):764–71.
8. Jensen UG, Brandt NJ, Christensen E, Skovby F, Norgaard-Pedersen B, Simonsen H. Neonatal screening for galactosemia by quantitative analysis of hexose monophosphates using tandem mass spectrometry: a retrospective study. Clin Chem. 2001;47(8):1364–72.
9. Phenylketonuria (PKU): screening and management. NIH Consens Statement . 2000;17(3):1–33.
10. Verkerk PH, van Spronsen FJ, van Houten M, Smit GP, Sengers RC. Predictors of mean phenylalanine levels during the fi rst fi ve years of life in patients with phenylketonuria who were treated early. Dutch National PKU Steering Committee. Acta Paediatr Suppl. 1994;407:70–2.
11. Viau KS, Wengreen HJ, Ernst SL, Cantor NL, Furtado LV, Longo N. Correlation of age-specifi c phenylalanine levels with intellectual outcome in patients with phenylketonuria. J Inherit Metab Dis. 2011;34(4):963–71.
12. Koch R, Trefz F, Waisbren S. Psychosocial issues and outcomes in maternal PKU. Mol Genet Metab. 2010;99 Suppl 1:S68–74.
13. Widaman KF, Azen C. Relation of prenatal phenylalanine exposure to infant and childhood cognitive outcomes: results from the International Maternal PKU Collaborative Study. Pediatrics. 2003;112(6 Pt 2):1537–43.
14. Koch R, Azen C, Friedman E, et al. Research design, organization, and sample characteristics of the Maternal PKU Collaborative Study. Pediatrics. 2003;112(6 Pt 2):1519–22.
15. Longo N. Disorders of biopterin metabolism. J Inherit Metab Dis. 2009;32(3):333–42. 16. Dobrowolski SF, Heintz C, Miller T, et al. Molecular genetics and impact of residual in vitro
phenylalanine hydroxylase activity on tetrahydrobiopterin responsiveness in Turkish PKU population. Mol Genet Metab. 2011;102(2):116–21.
17. Koch R, Moseley K, Guttler F. Tetrahydrobiopterin and maternal PKU. Mol Genet Metab. 2005;86 Suppl 1:S139–41.
18. Aguado C, Perez B, Garcia MJ, et al. BH4 responsiveness associated to a PKU mutation with decreased binding affi nity for the cofactor. Clin Chim Acta. 2007;380(1–2):8–12.
19. Desviat LR, Perez B, Belanger-Quintana A, et al. Tetrahydrobiopterin responsiveness: results of the BH4 loading test in 31 Spanish PKU patients and correlation with their genotype. Mol Genet Metab. 2004;83(1–2):157–62.
20. Scott CR. The genetic tyrosinemias. Am J Med Genet C Semin Med Genet. 2006;142C(2):121–6.
21. Magera MJ, Gunawardena ND, Hahn SH, et al. Quantitative determination of succinylace-tone in dried blood spots for newborn screening of tyrosinemia type I. Mol Genet Metab. 2006;88(1):16–21.
22. Schlump JU, Mayatepek E, Spiekerkoetter U. Signifi cant increase of succinylacetone within the fi rst 12 h of life in hereditary tyrosinemia type 1. Eur J Pediatr. 2010;169(5):569–72.
23. Turgeon C, Magera MJ, Allard P, et al. Combined newborn screening for succinylacetone, amino acids, and acylcarnitines in dried blood spots. Clin Chem. 2008;54(4):657–64.
24. Arranz JA, Pinol F, Kozak L, et al. Splicing mutations, mainly IVS6–1(G>T), account for 70% of fumarylacetoacetate hydrolase (FAH) gene alterations, including 7 novel mutations, in a survey of 29 tyrosinemia type I patients. Hum Mutat. 2002;20(3):180–8.
25. Dreumont N, Poudrier JA, Bergeron A, Levy HL, Baklouti F, Tanguay RM. A missense mutation (Q279R) in the fumarylacetoacetate hydrolase gene, responsible for hereditary tyrosinemia, acts as a splicing mutation. BMC Genet. 2001;2:9.
26. Grompe M, al-Dhalimy M. Mutations of the fumarylacetoacetate hydrolase gene in four patients with tyrosinemia, type I. Hum Mutat. 1993;2(2):85–93.

194 M. Pasquali and N. Longo
27. Grompe M, St-Louis M, Demers SI, al-Dhalimy M, Leclerc B, Tanguay RM. A single mutation of the fumarylacetoacetate hydrolase gene in French Canadians with hereditary tyrosinemia type I. N Engl J Med. 1994;331(6):353–7.
28. St-Louis M, Leclerc B, Laine J, Salo MK, Holmberg C, Tanguay RM. Identifi cation of a stop mutation in fi ve Finnish patients suffering from hereditary tyrosinemia type I. Hum Mol Genet. 1994;3(1):69–72.
29. Orendac M, Zeman J, Stabler SP, et al. Homocystinuria due to cystathionine beta-synthase defi ciency: novel biochemical fi ndings and treatment effi cacy. J Inherit Metab Dis. 2003;26(8):761–73.
30. Mudd SH. Hypermethioninemias of genetic and non-genetic origin: a review. Am J Med Genet C Semin Med Genet. 2011;157(1):3–32.
31. Gan-Schreier H, Kebbewar M, Fang-Hoffmann J, et al. Newborn population screening for classic homocystinuria by determination of total homocysteine from Guthrie cards. J Pediatr. 2010;156(3):427–32.
32. Zschocke J, Kebbewar M, Gan-Schreier H, et al. Molecular neonatal screening for homo-cystinuria in the Qatari population. Hum Mutat. 2009;30(6):1021–2.
33. Watkins D, Rosenblatt DS. Inborn errors of cobalamin absorption and metabolism. Am J Med Genet C Semin Med Genet. 2011;157(1):33–44.
34. Tortorelli S, Turgeon CT, Lim JS, et al. Two-tier approach to the newborn screening of meth-ylenetetrahydrofolate reductase defi ciency and other remethylation disorders with tandem mass spectrometry. J Pediatr. 2010;157(2):271–5.
35. Clarke R, Lewington S. Homocysteine and coronary heart disease. Semin Vasc Med. 2002;2(4):391–9.
36. Steegers-Theunissen RP, Boers GH, Trijbels FJ, Eskes TK. Neural-tube defects and derange-ment of homocysteine metabolism. N Engl J Med. 1991;324(3):199–200.
37. Danner DJ, Doering CB. Human mutations affecting branched chain alpha-ketoacid dehydro-genase. Front Biosci. 1998;3:d517–24.
38. Fernhoff PM, Lubitz D, Danner DJ, et al. Thiamine response in maple syrup urine disease. Pediatr Res. 1985;19(10):1011–6.
39. Chuang DT, Chuang JL, Wynn RM. Lessons from genetic disorders of branched-chain amino acid metabolism. J Nutr. 2006;136(1 Suppl):243S–9.
40. Bhattacharya K, Khalili V, Wiley V, Carpenter K, Wilcken B. Newborn screening may fail to identify intermediate forms of maple syrup urine disease. J Inherit Metab Dis. 2006;29(4):586.
41. Fernandez-Guerra P, Navarrete R, Weisiger K, et al. Functional characterization of the novel intronic nucleotide change c.288+9C>T within the BCKDHA gene: understanding a variant presentation of maple syrup urine disease. J Inherit Metab Dis. Published online 30 Apr. 2010.
42. Flaschker N, Feyen O, Fend S, Simon E, Schadewaldt P, Wendel U. Description of the muta-tions in 15 subjects with variant forms of maple syrup urine disease. J Inherit Metab Dis. 2007;30(6):903–9.
43. Quental S, Macedo-Ribeiro S, Matos R, et al. Molecular and structural analyses of maple syrup urine disease and identifi cation of a founder mutation in a Portuguese Gypsy commu-nity. Mol Genet Metab. 2008;94(2):148–56.
44. Rodriguez-Pombo P, Navarrete R, Merinero B, Gomez-Puertas P, Ugarte M. Mutational spec-trum of maple syrup urine disease in Spain. Hum Mutat. 2006;27(7):715.
45. Palmieri F. Diseases caused by defects of mitochondrial carriers: a review. Biochim Biophys Acta. 2008;1777(7–8):564–78.
46. Cavicchi C, Malvagia S, la Marca G, et al. Hypocitrullinemia in expanded newborn screening by LC-MS/MS is not a reliable marker for ornithine transcarbamylase defi ciency. J Pharm Biomed Anal. 2009;49(5):1292–5.
47. Smith W, Kishnani PS, Lee B, et al. Urea cycle disorders: clinical presentation outside the newborn period. Crit Care Clin. 2005;21(4 Suppl):S9–17.

1958 Newborn Screening for Metabolic Disorders
48. Nassogne MC, Heron B, Touati G, Rabier D, Saudubray JM. Urea cycle defects: manage-ment and outcome. J Inherit Metab Dis. 2005;28(3):407–14.
49. Scaglia F, Lee B. Clinical, biochemical, and molecular spectrum of hyperargininemia due to arginase I defi ciency. Am J Med Genet C Semin Med Genet. 2006;142C(2):113–20.
50. Kobayashi K, Saheki T. Citrin defi ciency. In: Pagon RA, Bird TD, Dolan CR, Stephens edi-tors. Gene Reviews. Seattle (WA): University of Washington, Seattle; 1993–2005 [updated 2008 June 01].
51. Saheki T, Inoue K, Tushima A, Mutoh K, Kobayashi K. Citrin defi ciency and current treat-ment concepts. Mol Genet Metab. 2010;100 Suppl 1:S59–64.
52. Fukushima K, Yazaki M, Nakamura M, et al. Conventional diet therapy for hyperammonemia is risky in the treatment of hepatic encephalopathy associated with citrin defi ciency. Intern Med. 2010;49(3):243–7.
53. Dimmock D, Kobayashi K, Iijima M, et al. Citrin defi ciency: a novel cause of failure to thrive that responds to a high-protein, low-carbohydrate diet. Pediatrics. 2007;119(3):e773–7.
54. Ohura T, Kobayashi K, Tazawa Y, et al. Clinical pictures of 75 patients with neonatal intrahe-patic cholestasis caused by citrin defi ciency (NICCD). J Inherit Metab Dis. 2007;30(2):139–44.
55. Tazawa Y, Kobayashi K, Abukawa D, et al. Clinical heterogeneity of neonatal intrahepatic cholestasis caused by citrin defi ciency: case reports from 16 patients. Mol Genet Metab. 2004;83(3):213–9.
56. Tamamori A, Fujimoto A, Okano Y, et al. Effects of citrin defi ciency in the perinatal period: feasibility of newborn mass screening for citrin defi ciency. Pediatr Res. 2004;56(4):608–14.
57. Salek J, Byrne J, Box T, Longo N, Sussman N. Recurrent liver failure in a 25-year-old female. Liver Transpl. 2010;16(9):1049–53.
58. Deodato F, Boenzi S, Santorelli FM, Dionisi-Vici C. Methylmalonic and propionic aciduria. Am J Med Genet C Semin Med Genet. 2006;142C(2):104–12.
59. Desviat LR, Perez B, Perez-Cerda C, Rodriguez-Pombo P, Clavero S, Ugarte M. Propionic acidemia: mutation update and functional and structural effects of the variant alleles. Mol Genet Metab. 2004;83(1–2):28–37.
60. Perez B, Angaroni C, Sanchez-Alcudia R, et al. The molecular landscape of propionic aci-demia and methylmalonic aciduria in Latin America. J Inherit Metab Dis. 2010;33 Suppl 2:S307–14.
61. Bikker H, Bakker HD, Abeling NG, et al. A homozygous nonsense mutation in the methyl-malonyl-CoA epimerase gene (MCEE) results in mild methylmalonic aciduria. Hum Mutat. 2006;27(7):640–3.
62. Dobson CM, Gradinger A, Longo N, et al. Homozygous nonsense mutation in the MCEE gene and siRNA suppression of methylmalonyl-CoA epimerase expression: a novel cause of mild methylmalonic aciduria. Mol Genet Metab. 2006;88(4):327–33.
63. Vockley J, Ensenauer R. Isovaleric acidemia: new aspects of genetic and phenotypic hetero-geneity. Am J Med Genet C Semin Med Genet. 2006;142C(2):95–103.
64. Gallardo ME, Desviat LR, Rodriguez JM, et al. The molecular basis of 3-methylcrotonylg-lycinuria, a disorder of leucine catabolism. Am J Hum Genet. 2001;68(2):334–46.
65. Baumgartner MR, Almashanu S, Suormala T, et al. The molecular basis of human 3-methyl-crotonyl-CoA carboxylase defi ciency. J Clin Invest. 2001;107(4):495–504.
66. Sweetman L, Williams JC. Branched chain organic acidurias, vol. 2. 7th ed. New York: McGraw-Hill; 2001.
67. Holzinger A, Roschinger W, Lagler F, et al. Cloning of the human MCCA and MCCB genes and mutations therein reveal the molecular cause of 3-methylcrotonyl-CoA: carboxylase defi -ciency. Hum Mol Genet. 2001;10(12):1299–306.
68. Dantas MF, Suormala T, Randolph A, et al. 3-Methylcrotonyl-CoA carboxylase defi ciency: mutation analysis in 28 probands, 9 symptomatic and 19 detected by newborn screening. Hum Mutat. 2005;26(2):164.

196 M. Pasquali and N. Longo
69. Koeberl DD, Millington DS, Smith WE, et al. Evaluation of 3-methylcrotonyl-CoA carboxylase defi ciency detected by tandem mass spectrometry newborn screening. J Inherit Metab Dis. 2003;26(1):25–35.
70. Bannwart C, Wermuth B, Baumgartner R, Suormala T, Weismann UN. Isolated biotin-resistant defi ciency of 3-methylcrotonyl-CoA carboxylase presenting as a clinically severe form in a newborn with fatal outcome. J Inherit Metab Dis. 1992;15(6):863–8.
71. Bartlett K, Bennett MJ, Hill RP, Lashford LS, Pollitt RJ, Worth HG. Isolated biotin-resistant 3-methylcrotonyl CoA carboxylase defi ciency presenting with life-threatening hypoglycaemia. J Inherit Metab Dis. 1984;7(4):182.
72. Baykal T, Gokcay GH, Ince Z, et al. Consanguineous 3-methylcrotonyl-CoA carboxylase defi ciency: early-onset necrotizing encephalopathy with lethal outcome. J Inherit Metab Dis. 2005;28(2):229–33.
73. Visser G, Suormala T, Smit GP, et al. 3-methylcrotonyl-CoA carboxylase defi ciency in an infant with cardiomyopathy, in her brother with developmental delay and in their asymptomatic father. Eur J Pediatr. 2000;159(12):901–4.
74. Roschinger W, Millington DS, Gage DA, et al. 3-Hydroxyisovalerylcarnitine in patients with defi ciency of 3-methylcrotonyl CoA carboxylase. Clin Chim Acta. 1995;240(1):35–51.
75. van Hove JL, Rutledge SL, Nada MA, Kahler SG, Millington DS. 3-Hydroxyisovalerylcarnitine in 3-methylcrotonyl-CoA carboxylase defi ciency. J Inherit Metab Dis. 1995;18(5):592–601.
76. Menao S, Lopez-Vinas E, Mir C, et al. Ten novel HMGCL mutations in 24 patients of different origin with 3-hydroxy-3-methyl-glutaric aciduria. Hum Mutat. 2009;30(3):E520–9.
77. Suzuki Y, Yang X, Aoki Y, Kure S, Matsubara Y. Mutations in the holocarboxylase syn-thetase gene HLCS. Hum Mutat. 2005;26(4):285–90.
78. Fukao T, Scriver CR, Kondo N. The clinical phenotype and outcome of mitochondrial ace-toacetyl-CoA thiolase defi ciency (beta-ketothiolase or T2 defi ciency) in 26 enzymatically proved and mutation-defi ned patients. Mol Genet Metab. 2001;72(2):109–14.
79. Fukao T, Yamaguchi S. 3-ketoacyl-CoA thiolase defi ciency. Nippon Rinsho. 2002;60 Suppl 4:738–42.
80. Fukao T, Nakamura H, Nakamura K, et al. Characterization of six mutations in fi ve Spanish patients with mitochondrial acetoacetyl-CoA thiolase defi ciency: effects of amino acid sub-stitutions on tertiary structure. Mol Genet Metab. 2002;75(3):235–43.
81. Mrazova L, Fukao T, Halovd K, et al. Two novel mutations in mitochondrial acetoacetyl-CoA thiolase defi ciency. J Inherit Metab Dis. 2005;28(2):235–6.
82. Fukao T, Zhang GX, Sakura N, et al. The mitochondrial acetoacetyl-CoA thiolase (T2) defi -ciency in Japanese patients: urinary organic acid and blood acylcarnitine profi les under stable conditions have subtle abnormalities in T2-defi cient patients with some residual T2 activity. J Inherit Metab Dis. 2003;26(5):423–31.
83. Zhang GX, Fukao T, Rolland MO, et al. Mitochondrial acetoacetyl-CoA thiolase (T2) defi -ciency: T2-defi cient patients with “mild” mutation(s) were previously misinterpreted as normal by the coupled assay with tiglyl-CoA. Pediatr Res. 2004;56(1):60–4.
84. Hedlund GL, Longo N, Pasquali M. Glutaric acidemia type 1. Am J Med Genet C Semin Med Genet. 2006;142C(2):86–94.
85. Tortorelli S, Hahn SH, Cowan TM, Brewster TG, Rinaldo P, Matern D. The urinary excretion of glutarylcarnitine is an informative tool in the biochemical diagnosis of glutaric acidemia type I. Mol Genet Metab. 2005;84(2):137–43.
86. Longo N, Amat di San Filippo C, Pasquali M. Disorders of carnitine transport and the carni-tine cycle. Am J Med Genet C Semin Med Genet. 2006;142C(2):77–85.
87. Lund AM, Joensen F, Hougaard DM, et al. Carnitine transporter and holocarboxylase syn-thetase defi ciencies in The Faroe Islands. J Inherit Metab Dis. 2007;30(3):341–9.
88. Schimmenti LA, Crombez EA, Schwahn BC, et al. Expanded newborn screening identifi es maternal primary carnitine defi ciency. Mol Genet Metab. 2007;90(4):441–5.
89. Gregersen N, Andresen BS, Corydon MJ, et al. Mutation analysis in mitochondrial fatty acid oxidation defects: exemplifi ed by acyl-CoA dehydrogenase defi ciencies, with special focus on genotype-phenotype relationship. Hum Mutat. 2001;18(3):169–89.

1978 Newborn Screening for Metabolic Disorders
90. Boneh A, Andresen BS, Gregersen N, et al. VLCAD defi ciency: pitfalls in newborn screening and confi rmation of diagnosis by mutation analysis. Mol Genet Metab. 2006;88(2):166–70.
91. Andresen BS, Olpin S, Poorthuis BJ, et al. Clear correlation of genotype with disease pheno-type in very-long-chain acyl-CoA dehydrogenase defi ciency. Am J Hum Genet. 1999;64(2):479–94.
92. Carpenter K, Pollitt RJ, Middleton B. Human liver long-chain 3-hydroxyacyl-coenzyme A dehydrogenase is a multifunctional membrane-bound beta-oxidation enzyme of mito-chondria. Biochem Biophys Res Commun. 1992;183(2):443–8.
93. Spiekerkoetter U, Sun B, Khuchua Z, Bennett MJ, Strauss AW. Molecular and phenotypic heterogeneity in mitochondrial trifunctional protein defi ciency due to beta-subunit mutations. Hum Mutat. 2003;21(6):598–607.
94. Strauss AW, Bennett MJ, Rinaldo P, et al. Inherited long-chain 3-hydroxyacyl-CoA dehydro-genase defi ciency and a fetal-maternal interaction cause maternal liver disease and other pregnancy complications. Semin Perinatol. 1999;23(2):100–12.
95. Derks TG, Boer TS, van Assen A, et al. Neonatal screening for medium-chain acyl-CoA dehydrogenase (MCAD) defi ciency in The Netherlands: the importance of enzyme analysis to ascertain true MCAD defi ciency. J Inherit Metab Dis. 2008;31(1):88–96.
96. Horvath GA, Davidson AG, Stockler-Ipsiroglu SG, et al. Newborn screening for MCAD defi ciency: experience of the fi rst three years in British Columbia, Canada. Can J Public Health. 2008;99(4):276–80.
97. Iafolla AK, Thompson Jr RJ, Roe CR. Medium-chain acyl-coenzyme A dehydrogenase defi ciency: clinical course in 120 affected children. J Pediatr. 1994;124(3):409–15.
98. Andresen BS, Dobrowolski SF, O’Reilly L, et al. Medium-chain acyl-CoA dehydrogenase (MCAD) mutations identifi ed by MS/MS-based prospective screening of newborns differ from those observed in patients with clinical symptoms: identifi cation and characterization of a new, prevalent mutation that results in mild MCAD defi ciency. Am J Hum Genet. 2001;68(6):1408–18.
99. Waddell L, Wiley V, Carpenter K, et al. Medium-chain acyl-CoA dehydrogenase defi ciency: genotype-biochemical phenotype correlations. Mol Genet Metab. 2006;87(1):32–9.
100. Ficicioglu C, Thomas N, Yager C, et al. Duarte (DG) galactosemia: a pilot study of biochemi-cal and neurodevelopmental assessment in children detected by newborn screening. Mol Genet Metab. 2008;95(4):206–12.
101. Pindolia K, Jordan M, Wolf B. Analysis of mutations causing biotinidase defi ciency. Hum Mutat. 2010;31(9):983–91.
Recommended