See discussions, stats, and author profiles for this publication at: https://www.researchgate.net/publication/318840523
Molecular bases of anorexia nervosa, bulimia nervosa and binge eating
disorder: shedding light on the darkness
Article in Journal of Neurogenetics · August 2017
DOI: 10.1080/01677063.2017.1353092
CITATIONS
3READS
760
4 authors, including:
Some of the authors of this publication are also working on these related projects:
DIAMANTE View project
Novel Antiproliferative Drugs View project
Claude Everaerts
French National Centre for Scientific Research
89 PUBLICATIONS 920 CITATIONS
SEE PROFILE
Leticia G León
Erasmus MC
144 PUBLICATIONS 1,584 CITATIONS
SEE PROFILE
Angel Acebes
Universidad de La Laguna
45 PUBLICATIONS 871 CITATIONS
SEE PROFILE
All content following this page was uploaded by Leticia G León on 30 October 2017.
The user has requested enhancement of the downloaded file.

Full Terms & Conditions of access and use can be found athttp://www.tandfonline.com/action/journalInformation?journalCode=ineg20
Download by: [University of La Laguna Vicerrectorado] Date: 01 August 2017, At: 07:00
Journal of Neurogenetics
ISSN: 0167-7063 (Print) 1563-5260 (Online) Journal homepage: http://www.tandfonline.com/loi/ineg20
Molecular bases of anorexia nervosa, bulimianervosa and binge eating disorder: shedding lighton the darkness
Germán Cuesto, Claude Everaerts, Leticia G. León & Angel Acebes
To cite this article: Germán Cuesto, Claude Everaerts, Leticia G. León & Angel Acebes (2017):Molecular bases of anorexia nervosa, bulimia nervosa and binge eating disorder: shedding light onthe darkness, Journal of Neurogenetics
To link to this article: http://dx.doi.org/10.1080/01677063.2017.1353092
Published online: 01 Aug 2017.
Submit your article to this journal
View related articles
View Crossmark data

REVIEW ARTICLE
Molecular bases of anorexia nervosa, bulimia nervosa and binge eating disorder:shedding light on the darkness
Germ�an Cuestoa, Claude Everaertsb, Leticia G. Le�onc and Angel Acebesa
aCentre for Biomedical Research of the Canary Islands, Institute of Biomedical Technologies, University of La Laguna, Tenerife, Spain; bCentredes Sciences du Gout et de l'Alimentation, UMR 6265 CNRS, UMR 1324 INRA, Universit�e de Bourgogne Franche-Comt�e, Dijon, France;cCancer Pharmacology Lab, AIRC Start Up Unit, University of Pisa, Pisa, Italy
ABSTRACTEating-disorders (EDs) consequences to human health are devastating, involving social, mental, emo-tional, physical and life-threatening aspects, concluding on impairment and death in cases of extremeanorexia nervosa. It also implies that people suffering an ED need to find psychiatric and psychologicalhelp as soon as possible to achieve a fully physical and emotional recovery. Unfortunately, to date,there is a crucial lack of efficient clinical treatment to these disorders. In this review, we present anoverview concerning the actual pharmacological and psychological treatments, the knowledge of cells,circuits, neuropeptides, neuromodulators and hormones in the human brain- and other organs- under-lying these disorders, the studies in animal models and, finally, the genetic approaches devoted to facethis challenge. We will also discuss the need for new perspectives, avenues and strategies to be devel-oped in order to pave the way to novel and more efficient therapeutics.
ARTICLE HISTORYReceived 9 May 2017Revised 26 June 2017Accepted 5 July 2017
KEYWORDSEating disorders;pharmacology; neuromodu-lators; genetic approaches
Introduction
Eating-disorders (EDs) as anorexia nervosa (AN), bulimianervosa (BN) and binge-eating disorder (BED), have both adeep social impact and an enormous cost to public health-care systems (Keski-Rahkonen & Mustelin, 2016). Theexample of Europe is extremely illustrative: besides a veryhigh risk of premature mortality, more than 2/3 of thoseEDs patients had at least some role impairment in at leastone domain (Preti et al., 2009). In fact, the prevalence ofEDs has increased across time, particularly in the secondhalf of the twentieth century (Bulik et al., 2006). In the USA,20 million women and 10 million men had suffered from aclinically significant ED at some time in their life(Samnaliev, Noh, Sonneville, & Austin, 2015) with 7300worldwide deaths in 2010 (Lozano et al., 2012) resulting in2.2� 106 disability-adjusted life years (DALYs) (Murrayet al., 2012).
Anorexia nervosa is defined as an association of anabnormally low body weight, an intense fear of gainingweight and a distorted cognition regarding weight, shape,and drive for thinness. AN is a disorder but also a symptomof other disorders, as depression, bipolar disorder, anxietydisorders (obsessive–compulsive disorder, panic disorder,social phobias, and post-traumatic stress disorder) and sub-stance abuse (O’Brien & Vincent, 2003; Woodside & Staab,2006). In turn, BN is characterized by episodes of binge eat-ing – defined itself as ‘recurrent periods of uncontrolledovereating’ – in which big amounts of high-sugar,
carbohydrates and fat food are consumed in a very short-time period, followed by 1 or more compensatory purgebehaviours (vomiting, laxatives, fasting, etc… ). That takesplace on average a minimum of twice weekly for three ormore months, or, in extreme cases, several times a day. BNis divided into two subtypes: the above-mentioned purging-type and the lesser-common non-purging type, characterisedby fasting or excessive exercise trying to compensate for thecalories obtained from the previous binge. Besides, thereexist comorbidities between BN and other disorders as sub-stance abuse, affective disorders, and attention disorders(Altman & Shankman, 2009; Hatsukami, Eckert, Mitchell, &Pyle, 1984). Finally, Binge eating disorder (BED) patientsshow also repetitive and uncontrolled episodes of over con-sumption of larger amounts of food in a discrete period, but,unlike BN and AN they do not show recurrent compensa-tory purging, fasting and excessive exercise behaviours(American Psychiatric Association, 2013). As for AN andBN, BED has been associated with medical and psychiatriccomorbidities, as mood (anxiety) and substance use disor-ders (Becker & Grilo, 2015). Interestingly, BED is the mostprevalent among all eating disorders, being higher in womenthan in men, and also the most underdiagnosed and under-treated, due to insufficient diagnostic criteria and lack ofavailable treatment options [see Section 2 below and alsoKornstein, Kunovac, Herman, & Culpepper (2016)].
Eating-disorders have been long considered as severe psy-chiatric disorders of unknown aetiology. As previously
CONTACT Angel Acebes [email protected] Centre for Biomedical Research of the Canary Islands, Institute of Biomedical Technologies, Department of BasicMedical Sciences, Faculty of Medicine, University of La Laguna, 38071 La Laguna, Tenerife, Spain; Leticia G. Le�on [email protected] CancerPharmacology Lab, University of Pisa, Ospedale di Cisanello, Edificio 6, via Paradisa, 2. 56124 Pisa, Italy� 2017 Informa UK Limited, trading as Taylor & Francis Group
JOURNAL OF NEUROGENETICS, 2017https://doi.org/10.1080/01677063.2017.1353092
Dow
nloa
ded
by [
Uni
vers
ity o
f L
a L
agun
a V
icer
rect
orad
o] a
t 07:
00 0
1 A
ugus
t 201
7

mentioned, BN and BED are closely related to affective,attention, emotional and mood disorders. Social cognitionencompass the psychological processes endowing individualsto observe, process, store and retrieve information obtainedfrom conspecifics in social interactions (Frith, 2008). Poorrecognition of emotions in others is documented in ANpatients and facial emotion recognition difficulties persist inthem even after recovery (Oldershaw et al., 2011). Besides,brain abnormalities have been described in AN patients,including abnormal neural activation (Uher et al., 2004) andaltered neurotransmitter function (Kaye, Fudge, & Paulus,2009). More research is crucial to establish links betweensocial cognition abnormalities and neurological defaults asso-ciated with AN (Cardi et al., 2015).
Under these grounds, deciphering unambiguously howthe brain controls food intake and satiation mechanisms iscrucial to know how eating-associated pathological disordersare bypassing this control. To date, there is a good know-ledge about the bidirectional communication among exten-sive areas of the nervous system (including the cortex, basalganglia, and the limbic system) with peripheral components(such as gustatory system, gastrointestinal nervous system,pancreas, liver, muscle, and adipose tissue), sustaining anexquisitely well-regulated homeostasis between food intakeand energy expenditure (Lenard & Berthoud, 2008;Mithieux, 2013). In addition to these circuits, the brainendocannabinoid system also acts as a key regulator for foodintake and energy balance (Cardinal et al., 2015; Di Marzoet al., 2001; DiPatrizio & Piomelli, 2012) through food-related olfactory-dependent mechanisms (Soria-Gomez,Bellocchio, & Marsicano, 2014) and is likely involved in thehedonic and emotional aspects of eating. In spite of thesefundamental advances, it is not completely understood howneuronal feeding circuits regulate food intake and hence,after energy repletion, yield to abolish new impulse to eat.The hypothalamus is crucial to integrate metabolic and sen-sorial signals from the periphery, and from higher brainstructures. More precisely, the hypothalamic arcuate nucleus(ARC) harbours two neuronal populations, one participatingto the synthesis of the appetite-stimulating neuropeptide Y(NPY) and Agouti-related peptide (AgRP) and the otherexpressing the two appetite-suppressing peptides proopiome-lanocortin (POMC) and cocaine- and amphetamine-regulated transcript (CART) (see Lenard & Berthoud, 2008).This highlights the importance of neuropeptide-mediatedpathways in the control of food intake and energy balance.Neuropeptides are a group of chemically diverse moleculesmodulating physiological processes and behaviours in mam-mals (van den Pol, 2012) and invertebrates (Taghert &Nitabach, 2012). Particularly relevant is the case of NPY,synthesized and released by many unrelated groups of neu-rons from different human brain regions and activating mul-tiple different receptors in target neurons (van den Pol,2012).
The brain homeostatic control of feeding involves neuralcircuits located in the hypothalamus (hunger signals, initiat-ing feeding behaviour) and the brainstem (satiation signals,limiting meal size) generating appropriate integratedresponses (Adan, Vanderschuren, & la Fleur, 2008; Woods,
Seeley, Porte, & Schwartz, 1998). Single neuropeptides con-tribute to feeding behaviours in mammals (Dailey &Bartness, 2009), and their roles in the neuronal circuitsunderlying these behaviours have been intensively studied.NPY/AgRP peptidergic neurons increase feeding intake byinhibiting POMC/CART system which stimulates anorexi-genic neurons in the lateral hypothalamus (LH) area, andstimulating orexigenic neurons in the paraventricular nucleus(PVN) (Aponte, Atasoy, & Sternson, 2011; Atasoy, Betley,Su, & Sternson, 2012; Wu, Boyle, & Palmiter, 2009).Together, these neuropeptides translates the feeding behav-iour in appetite as well as adaptive responses (Borglandet al., 2009).
Interestingly, several pieces of evidence indicate thatneurobiological mechanisms underlying ED might involve anoverreaction of the immune system, generating, in turn, adysfunction of neuropeptide signalling. Thus, reactiveImmunoglobulins (Igs) bind to food-intake neuropeptides(named peptide autoantibodies) and are identified in theserum of AN/BN patients, predominantly bound to a-MSHin hypothalamic neurons (Fetissov et al., 2005). In addition,the enterobacteria Caseinolytic protease B protein ClpB alsoact as an a-MSH-mimetic protein, triggering production ofIgs against a-MSH, reducing its anorexigenic effects(Tennoune et al., 2014). Interestingly, these circulating auto-antibodies might be purified in order to be employed aspharmacological tools in AN and BN (Smitka et al., 2013).
In addition to the gastrointestinal-brain communication,gut microbiota plays an important role on nutrimentsabsorption and energy expenditure. Likewise, the brain-gut-microbiota axis allows a bidirectional communicationbetween gut microbes and the brain through endocrine,neural, immune and metabolic pathways (Dinan & Cryan,2017). Moreover, modifications of the gut microbiota havealso been described in AN patients (Armougom, Henry,Vialettes, Raccah, & Raoult, 2009). It is also well character-ized that the gut microbiome contributes to the pathogenesisof malnutrition through nutrient metabolism and immunefunction (Krajmalnik-Brown, Ilhan, Kang, & DiBaise, 2012).Besides, chronic constipation, a common feature in ANpatients, is present prior to weight loss and causes changesin gut microbiota, increasing Methanobrevibacter smithii le-vels (Kim et al., 2012). More interestingly, elevated plasmaconcentrations of the ClpB have been detected in femalepatients with AN, BN, and BED when compared withhealthy individuals (Breton et al., 2016). These findings openthe possibility to manipulate gut microbiota (by using antibi-otics) helping to improve nutritional therapy for ED patients.Clearly, more research is needed at this point.
Pharmacology and pharmacotherapy tools in eatingdisorders
Current treatments of the EDs are substantially multidimen-sional and include psychotherapy, nutritional rehabilitation,drug treatment and even light therapy, but unfortunatelyoften they have shown limited efficacy in ameliorating symp-toms not fully normalizing eating behaviours (Halmi, 2005).To date, psychotherapies such as cognitive behavioural
2 GERM�AN CUESTO ET AL.
Dow
nloa
ded
by [
Uni
vers
ity o
f L
a L
agun
a V
icer
rect
orad
o] a
t 07:
00 0
1 A
ugus
t 201
7

therapy (CBT), cognitive analytic therapy (CAT), dialecticalbehavioural therapy (DBT) or family-based therapy (FBT),remain the main treatments of EDs, even though some drugtherapies have been employed for some specific EDs. Themost demanded pharmacotherapy of EDs should induce aremission of symptoms in the acute phase of the disease,prevent relapse over time and be appropriate to treat fre-quent associated comorbidities. Nowadays, there are noeffective drugs to overcome all these clinical features, exceptfluoxetine and lisdexamfetamine, the only drugs approved bythe international regulatory agencies for the treatment oftwo EDs (respectively BN and BED). Furthermore, numer-ous drugs used in psychiatric clinic (i.e. antipsychotics, anti-depressants, mood stabilizers, and selective norepinephrineand/or serotonin reuptake inhibitors) were also tested totreat clinical manifestations of EDs, showing variable results.In this review, we will highlight the main positive clinicalresults.
Anorexia nervosa
AntipsychoticsAntipsychotic drugs act by blocking dopamine receptors(Miller, 2009). While antipsychotics are known to increaseappetite and weight gain in patients with major psychiatricdisorders (schizophrenia or bipolar disorder; Hay &Claudino, 2012), most of them are paradoxically not usefulfor weight recovery in AN patients (McKnight & Park,2010). However, they are able to reduce AN psychologicalcomorbidities (body image alteration, pathological focus onweight and food, fear of gaining weight, obsessive–compul-sive symptoms, hyperarousal and agitation; see Powers &Santana, 2004).
The first-generation of antipsychotics, pimozide and sul-piride, did not demonstrated sufficient capacity to favourweight gain (Vandereycken, 1984), whereas second-gener-ation antipsychotics are proved more useful, in particularolanzapine, a D2/5HT2 antagonist. This second generationfavours an increase in weight, leads to a significant reductionin the ‘anorexic ruminations’ and depressive symptoms butalso an improvement in obsessive–compulsive symptoms(Brewerton, 2012; Flament, Bissada, & Spettigue, 2012).Other second-generation antipsychotics, such as risperidone,quetiapine, aripiprazole, and ziprasidone, have not been soextensively studied in the treatment of AN (Powers & Bruty,2009). While olanzapine is efficient in reducing psychiatricsymptoms associated with the AN promoting weight recov-ery, its side effects, such as extrapyramidal symptoms andcardiac troubles (QT prolongation), are dangerous for anor-exic patients. All the main international guidelines classifythe use of these second-generation antipsychotics just assecondary possibilities for AN treatment (Aigner, Treasure,Kaye, Kasper, & WFSBP Task Force On Eating Disorders,2011).
Finally, the azapirone derivative tandospirone, also knownas metanopirone, is a selective serotonin-1A (5-HT1A)receptor partial agonist (Tanaka et al., 1995) known toshown enhanced cholinergic and dopaminergic
neurotransmission in hippocampus and cortex (Koyama,Nakajima, Fujii, & Kawashima, 1999; Rasmusson, Goldstein,Deutch, Bunney, & Roth, 1994). Tandospirone is an anti-psychotic and anxiolytic drug clinically used to treat schizo-phrenia in China and Japan (Sumiyoshi et al., 2007), butalso induces improvement in weight gain and psychopath-ology of the AN patients (Okita, Shiina, Nakazato, & Iyo,2013).
AntidepressantsWhile the use of antidepressant in the treatment of EDswould appear logical due to the high rates of comorbidity(greater than 50%) between EDs and mood depression(Mischoulon et al., 2011), the effectiveness of antidepressantsin the treatment of AN patients is weak. Thus, while tricyclicantidepressants (TCA) have not shown significant benefits(Halmi, Eckert, LaDu, & Cohen, 1986), the most recent sero-tonin reuptake inhibitors (SSRIs – fluoxetine) have shownvery little effectiveness in promoting weight regain in ANpatients (Walsh et al., 2006).
Bulimia nervosa
AntipsychoticsSecond-generation antipsychotics used in AN treatmentinduce or exacerbate the crisis of binge eating in patientswith EDs (McElroy, Guerdjikova, Mori, & O’Melia, 2012).
AntidepressantsContrarily to what is described for AN, antidepressants(including TCAs, SSRIs, Serotonin-norepinephrine reuptakeinhibitors (SNRIs), and monoamine oxidase inhibitors,MAOIs) are the mainstay of pharmacological treatment forBN, by reducing the dopamine crisis of binge eating andpurging phenomena, improving anxiety moods (Capasso,Petrella, & Milano, 2009). However, although quite effective,both the clinical use of TCA and MAOIs are not recom-mended for their frequent adverse events. Desipramine (aTCA also known as desmethylimipramine) inhibits thereuptake of norepinephrine and, to a minor extent, sero-tonin. Both imipramine and desipramine were demonstratedto reduce binge eating and to improve the comorbidities inshort-term treatments (Barlow, Blouin, Blouin, & Perez,1988; Walsh, Hadigan, Devlin, Gladis, & Roose, 1991).However, their side effects make them inadequate for BNlong-term treatments (Agras et al., 1992; Leitenberg et al.,1994). In turn, SSRIs (fluoxetine, citalopram, sertraline andfluvoxamine) were shown to reduce BN main symptoms(Bacaltchuk & Hay, 2001; McElroy et al., 2003; Milano,Petrella, Sabatino, & Capasso, 2004). Among them,Fluoxetine has been the most studied being – since 1997 –the only drug approved by the FDA for the treatment of BN,at a dose of 60mg/day. Although BN is a chronic diseasewith frequent relapses, most trials lasted only several months(Martiadis, Castaldo, Monteleone, & Maj, 2007). However, a58-week study has demonstrated the efficacy of fluoxetine inreducing binge and purging episodes, obsessive–compulsive
JOURNAL OF NEUROGENETICS 3
Dow
nloa
ded
by [
Uni
vers
ity o
f L
a L
agun
a V
icer
rect
orad
o] a
t 07:
00 0
1 A
ugus
t 201
7

symptoms and the frequency of relapses (Romano, Halmi,Sarkar, Koke, & Lee, 2002). Finally, milnacipran is a dualacting antidepressant which inhibits the reuptake of bothserotonin and noradrenaline (SNRI) being efficient in theshort-term treatment of patients with BN (El-Giamal et al.,2003) and leading to a significant reduction in weekly bingeeating and vomiting frequency.
Anticonvulsant mood stabilizersMany drugs described as ‘mood stabilizers’ are categorizedas anticonvulsants, and the term ‘anticonvulsant moodstabilizers’ is sometimes used to describe them as a class.Since the early 2000s, antiepileptic drugs (AEDs) have beenuseful in the treatment of psychiatric disorders related toEDs, such as headache, substance abuse, and bipolar, anxietyor personality disorders. Furthermore, many AEDs interactwith glutamatergic, GABAergic, serotonergic and dopamin-ergic systems in the regulation of appetite, food intake andweight (Gao & Horvath, 2008; Meister, 2007). For example,topiramate and zonisamide are associated with appetite andweight decrease (McElroy et al., 2009).
Numerous human clinical studies, and preclinical studiesin animals, have demonstrated the utility of topiramate(TPM) in neuroprotection against ischemia and brain inju-ries, body weight loss in obese subjects, mitigation of alcoholconsumption, drug addiction, post-traumatic stress disorder,BN and BED. Its efficiency in the treatment of EDs associ-ated with obesity – BN and BED – could be related to itseffect on kainite/AMPA glutamate receptors (Hettes et al.,2003). Thus, TPM improves multiple behavioural aspects ofBN: binge and purge symptoms are reduced, while self-esteem, eating attitudes, anxiety, body weight and bodyimage are also ameliorated (Nickel et al., 2005). Beside itsefficiency, TPM has some recognized several adverse events(paraesthesia, metabolic acidosis, nephrolithiasis, acute cog-nitive impairment, and acute myopia among others (Shank& Maryanoff, 2008) that must be taken into account in thecommon clinical practice.
Binge eating disorder
AmphetamineDue to their weak efficacy and severe side effects, the use ofdrugs to treat BED was limited until lisdexamfetamine dime-sylate (L-lysine-dextroamphetamine, LDX) was approved bythe US food and drug administration (FDA) to treat moder-ate to severe BED in adults (50–70mg/day, US FDA, 2015).Nowadays, it is the only drug currently approved for thetreatment of BED, and the second medication of any ED,after fluoxetine (approved for BN in 1997). LDX is an effica-cious treatment for BED by regulating dopamine (DA), nor-epinephrine (NE) and serotonin neurotransmitters involvedin the modulation of appetite, hunger and eating behaviours(Guerdjikova, Mori, Casuto, & McElroy, 2016).
AntipsychoticsMemantine is a non-competitive antagonist of N-methyl-D-aspartate receptors (NMDARs). Memantine therapy in
schizophrenic patients improves mainly negative symptoms(Velligan, Alphs, Lancaster, Morlock, & Mintz, 2009) show-ing also promising results in the treatment of generalizedanxiety disorder (Schwartz, Siddiqui, & Raza, 2012), atten-tion deficit hyperactivity disorder ADHD (Hosenbocus &Chahal, 2013) and obsessive compulsive disorder (Haghighiet al., 2013). Memantine has been proved effective in reduc-ing the frequency of binge days and episodes (Brennanet al., 2008; Hermanussen & Tresguerres, 2005).
AntidepressantsThe antidepressants are also useful in the treatment of BEDboth decreasing the binge seizure frequency and improvingsymptoms of depression and anxiety often present in BED.SSRIs seem to favour a significant reduction in binge crisishaving a modest effect in reducing the body weight of thepatients (Reas & Grilo, 2008; Stefano, Bacaltchuk, Blay, &Appolin�ario, 2008). Although the effect of fluoxetine is con-troversial in humans (Arnold et al., 2002; Grilo, Crosby,Wilson, & Masheb, 2012), this drug (as TPM and sibutr-amine) was reported to reduce binge eating in animal mod-els (Cifani, Polidori, Melotto, Ciccocioppo, & Massi, 2009).
Two other drugs acting similar to antidepressants, duloxe-tine and sibutramine, two serotonin re-uptake inhibitors(SNRIs), have shown the ability to reduce both the frequencyof binge episodes crisis, body weight, and depressive symp-toms in patients with BED (Appolinario et al., 2003;Guerdjikova et al., 2012; Milano et al., 2005). However, since2010, sibutramine has been withdrawn from European andUSA markets due to cardiovascular risks. Venlafaxine isanother SNRI that at low-dose (75mg/day) also acts as aweak inhibitor of norepinephrine re-uptake (Smith,Dempster, Glanville, Freemantle, & Anderson, 2002). Inaddition, Venlafaxine may be an effective treatment for BEDassociated with overweight or obesity in reducing of weeklybinge frequency, severity of binge-eating and mood symp-toms (McElroy et al., 2012). These effects can be related toits activity against impulse control disorders (ICD;Camardese, Picello, & Bria, 2008).
Finally, atomoxetine is a selective norepinephrinereuptake inhibitor (NRI) indicated for patients with atten-tion-deficit hyperactivity disorder and narcolepsy (Garnock-Jones & Keating, 2009). Although in 2007 McElroy’s teamhave shown preliminary evidence for the efficacy of atomo-xetine in BED (McElroy et al., 2007), no newer studies hasbeen devoted to this drug.
Anticonvulsant mood stabilizersIn studies in BED with obesity, Citalopram-treated patientsdisplayed a 94% reduction of binge eating and significantweight loss (McElroy et al., 2003). In turn, zonisamide is asulfonamide anticonvulsant approved for use as an adjunc-tive therapy in adults with partial-onset seizures and infantilespasm (Brodie, Ben-Menachem, Chouette, & Giorgi, 2012;Holder & Wilfong, 2011). Together with the CBT, zonisa-mide has proved useful in the treatment of obesity associatedBED, in a one-year trial, with reduction of the binge
4 GERM�AN CUESTO ET AL.
Dow
nloa
ded
by [
Uni
vers
ity o
f L
a L
agun
a V
icer
rect
orad
o] a
t 07:
00 0
1 A
ugus
t 201
7

manifestations and weight loss (Ricca, Castellini, Lo Sauro,Rotella, & Faravelli, 2009). However, it presents substantiallythe same adverse effects as TPM.
Anti-obesity drugsThe serotonin releaser fenfluramine, also known as 3-tri-fluoromethyl-N-ethylamphetamine, is a highly effective ano-rectic agent in both laboratory animals and humans (Davis& Faulds, 1996; McGuirk, Goodall, Silverstone, & Willner,1991). This drug reduced the frequency of seizures in BEDobese patients, without weight loss (Stunkard, Berkowitz,Tanrikut, Reiss, & Young, 1996). However, fenfluramineworks only while it is taken and binge eating returns to pre-vious levels after medication. Fenfluramine was removedfrom its clinical use after reports of heart valve disease in1997 (Rothman & Baumann, 2002). In turn, orlistat is agastrointestinal lipase inhibitor that reduces the absorptionof dietary fat, indicated for weight loss and maintenance,being designed to treat obesity (Padwal & Majumdar, 2007).It has been used in individuals with BED primarily targetingweight loss rather than binge eating frequency (Grilo,Masheb, & Salant, 2005). It must be noted that orlistat mis-uses were reported in patients with BED and BN(Fern�andez-Aranda et al., 2001; Hagler Robinson, 2009).
Anti-addiction drugsThe urge to consume food and the lack of control in BEDpatients resemble the strong impulse to consume alcoholand the absence of control found in Alcohol Use Disorder(AUD) patients (Pelchat, 2009). Indeed, BED and AUDshare similar neural substrates (Volkow, Wang, & Baler,2011) activating the mesolimbic dopaminergic ‘reward’ sys-tem (Koob & Volkow, 2010; Umberg, Shader, Hsu, &Greenblatt, 2012). Therefore, almost all AUD medicationshave been tested in BED patients, with insignificant results,except disulfiram, the oldest medication approved for AUD(McElroy et al., 2012; Suh, Pettinati, Kampman, & O’Brien,2006). Disulfiram is a carbamate derivative discovered in the1920s, and used since the 1950s to support the treatment ofchronic alcoholism by producing an acute sensitivity to etha-nol by inhibiting the aldehyde dehydrogenase (ALDH)involved in alcohol metabolism (Hald & Jacobsen, 1948).Disulfiram also inhibits the dopamine b-hydroxylase (DbH),responsible for converting dopamine to noradrenaline innoradrenergic neurons (Barth & Malcolm, 2010). Used astreatment of BED, disulfiram effectively reduced the fre-quency of binge eating episodes in BED patients, and thiseffect is also considered to be due, at least in part, to DbHinhibition, as for cocaine use disorder (Farci et al., 2015).However, the use of disulfiram in the BED treatment may belimited by side effects or by the risk of exacerbation ofpsychotic disorders in BED patients.
In summary, the pharmacological treatment of EDs is inits early stages. Nowadays, no drug was especially designedto treat ED suffering patients, and current ED pharmaco-therapy is only the adaptation of some drugs previously used
in psychiatric clinic, showing generally undesirable sideeffects.
Neuropeptides, neurotransmitters and hormonesinvolved in EDs
Role of neuropeptides in EDs
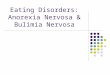
Hunger signals results from internally generated metabolicdeficits yielding the animals to feed (Saper, Chou, &Elmquist, 2002). Feeding behaviour remains critical forrestoring metabolic homeostasis and, consequently, survival.Animals have evolved refined feedback mechanisms to regu-late energy expenditure and food consumption, rectifyingpossible imbalances and modifying feeding thresholds con-sidering both internal needs and food availability (Morton,Cummings, Baskin, Barsh, & Schwartz, 2006). How the ner-vous system integrates internal physiological state to generatea response triggering feeding behaviours is insufficientlydocumented and, hence, understood. However, in this scen-ario, the crosstalk of neuropeptides within the nervous sys-tem and peripheral circulating hormones appears to beextremely relevant. Figure 1 shows a schematic summary ofthe information highlighted in this section. Indeed, neuro-peptides affect different complex behaviours at system, cellu-lar, and molecular levels in an age-dependent andhormonally modulated manner (Figure 1).
Research evidences point directly to defaults in neuropep-tide levels and/or function in ED pathogeny. In this review,we have highlighted the most relevant:
NPY/AgRPNeuropeptide Y and Agouti-related peptide are both pro-duced mainly in the ventromedial part of the ARC hypotha-lamus by NPY/AgRP neurons (Broberger, Johansen,Johansson, Schalling, & H€okfelt, 1998; Chronwall et al.,1985). Both neuropeptides exert an orexigenic signal overhypothalamic–pituitary–adrenocortical axis, increasing theACTH, cortisol and prolactin release and have been involvedin appetite regulation. Cerebral injections of NPY induce thefood intake (Clark, Kalra, Crowley, & Kalra, 1984) and highlevels of NPY are associated with high food intake but lowphysical activity (Schwartz et al., 1996). Recent studies indi-cates AN patients are unable to up-regulate NPY system toadapt their energy demand when exposed to chronic under-nutrition, whereas the satisfaction for rapid food is due tothe triggered a-melanocyte-stimulating hormone (a-MSH)response occurred during lunchtime (Galusca et al., 2015).Besides, an abnormal increase of NPY have been found inAN and BN patients after consumption of high-carbohydrateand high-protein breakfast, suggesting alterations in regula-tion of gut–brain axis peptides and indicating that NPYplasma levels represent a good indicator for EDs (Sedlackovaet al., 2012). In an indirect manner, the anti-stress effects ofNPY are also relevant to ameliorate psychiatric conditions ofboth AN and BN patients. In turn, AgRP has been involvedin appetite regulation since passive stress prevents AgRP and
JOURNAL OF NEUROGENETICS 5
Dow
nloa
ded
by [
Uni
vers
ity o
f L
a L
agun
a V
icer
rect
orad
o] a
t 07:
00 0
1 A
ugus
t 201
7

orexin upregulation in response to activity in an anorexia ratmodel (Boersma et al., 2016).
OrexinsOrexins, also known as hypocretins, are orexigenic neuralhormones expressed and secreted in the LH nucleus, but arealso expressed in peripheral tissues such as kidney, adrenalglands, pancreas, placenta, stomach, ileum, colon and colo-rectal epithelial cells (Nakabayashi et al., 2003). Orexinsinteract with leptin either directly regulating neural orexi-genic pathways (Muroya et al., 2004) or indirectly, modulat-ing the activity of orexigenic neurons in the LH (Louis,Leinninger, Rhodes, & Myers, 2010). Interestingly, neuropep-tides as orexins, but also melanin-concentrating hormone(MCH) and 26RFa are up-regulated in AN patients. Toexplain this finding, two different hypotheses have been for-mulated. In the first one, this up-regulation might resultfrom an adaptive mechanism to increase food intake againstunder nutrition. In the second, a chronic increase of orexi-genic neurons could reinforce dopamine-induced anxiety inthe reward system (see dopamine section below) of ANpatients, increasing their aversion to eat (Gorwood et al.,2016). Orexins are also involved in endocrine system regula-tion, playing an important role in insulin, glucagon and lep-tin secretion in response to glucose (Park et al., 2015).Interestingly, alterations in orexin signalling could be relatedwith eating disorders at different levels: either by regulatingdirectly the appetite, but also regulating the reward systemand controlling anxiety levels. For this reason, orexin could
be the link between physiological and psychological compo-nents, since most of the eating disorders are caused by cul-tural pressure to thinness. This pressure often canalizes asfrustration by predisposed people, triggering development ofanxiety and behavioural related disorders.
Proopiomelanocortin (POMC) and CARTProopiomelanocortin is a precursor polypeptide synthesizedmainly in the anterior pituitary, expressed as pre-proopiome-lanocortin and cleaved by the convertase prohormones 1 and2 generating a-MSH, ACTH, and the opioids beta-endorphinand Met-enkephalin. POMC is an anorexigenic peptide atthe hypothalamic ARC. Indeed, re-feeding after fasting indu-ces the activation of POMC neurons in ARC, promotingsatiety (Fekete et al., 2012). Leptin is the key activating regu-lator of the CNS POMC system, which is involved in appe-tite but also regulation of sexual behaviour, lactation,reproductive cycle, central cardiovascular control, melaninproduction in the skin, addictive behaviours and stress ma-nagement (Millington, 2007; Zhou & Kreek, 2015). POMCmRNA level increases after stress exposition and POMCneurons activate rapidly under emotional stressing condi-tions (J. Liu et al., 2007). These evidences define the role ofPOMC as a key communication link between brain feedingcontrol centre and stress systems (Ryan et al., 2014). In ad-dition, a-MSH, a POMC-derived peptide, is involved inmanifestation of affective disorders like anxiety and depres-sion via MC4R response in the PVN and ARC nuclei,among others (Kokare, Dandekar, Singru, Gupta, &
Figure 1. The neuropeptide, neurotransmitter and hormonal control of food intake. This schematic picture shows the interrelationships among different modulators,brain areas and other body organs. Dotted lines indicate modulatory actions exerted outside the hypothalamus. Pointed arrows indicate activation and blunt arrowsindicate repression. Dopaminergic actions are shown in blue, whereas serotonergic actions are represented in orange. Abnormal levels reported on Eating disordersare indicated with yellow squares.
6 GERM�AN CUESTO ET AL.
Dow
nloa
ded
by [
Uni
vers
ity o
f L
a L
agun
a V
icer
rect
orad
o] a
t 07:
00 0
1 A
ugus
t 201
7

Subhedar, 2010). Finally, intracerebroventricular injection ofMC4R agonists activates the hypothalamo–pituitary–adrenal(HPA) axis, increased anxiety and reduced food intake(Klenerova, Sery, & Hynie, 2008).
In turn, cocaine and amphetamine regulated transcript(CART) is an anorectic peptide widely expressed in bothcentral and peripheral nervous system, playing an importantrole in the hypothalamus (Keller et al., 2006). As for POMC,CART hypothalamic secretion is regulated by leptin (Eliaset al., 1998) and it has been related with addictive beha-viours and stress responses (Bakhtazad, Vousooghi, Garmabi,& Zarrindast, 2016). The intracerebroventricular CARTadministration reduces appetite and increases energyexpenditure, but, under specific circumstances, hypothalamicCART has been considered also as orexigenic (Murphy,2005). An increase in CART expression has been alsoreported in the nucleus accumbens (NAc), mediating thehyperactivity in AN induced by activation of serotonin 5-HT4 receptor (Jean et al., 2007).
OxytocinOxytocin is a peptidic hormone involved in social, sexualand parental behaviours, among others (Ross & Young,2009). Several evidences connect oxytocin signalling andEDs. Indeed, recently, oxytocin treatment has been proposedagainst obesity (Altirriba, Poher, & Rohner-Jeanrenaud,2015), whereas oxytocin antagonist increases body weightgain (Zhang & Cai, 2011). The release of oxytocin to blood-stream has been associated with the inhibition of appetite(Herisson, Brooks, Waas, Levine, & Olszewski, 2014) and therelease, through the action of prolactin-releasing peptide, ofthe satiety signal cholecystokinin (CKK) (Yamashita et al.,2013). Actually, four-week chronic oxytocin treatmentreduces body weight in rhesus monkeys by decreasing foodintake and increasing energy expenditure and lipolysis(Blevins et al., 2015). This anorectic effect involves partiallythe inhibition of reward circuits (Peters, Bowen, Bohrer,McGregor, & Neumann, 2017), is accompanied by a reduc-tion of gastric empting and is blocked by an oxytocin recep-tor antagonist in rats (Wu, Doong, & Wang, 2008).According to this, circulating oxytocin levels has been foundaltered in AN patients, but not in BN (Monteleone,Scognamiglio, Volpe, Di Maso, & Monteleone, 2016).Interestingly, oxytocin treatments decreased caloric intake inBN patients but not in AN (Kim, Eom, Yang, Kang, &Treasure, 2015). Despite these contradictory findings, oxyto-cinergic system has been suggested to be involved in mecha-nisms underlying BN and eating disorders, since specificoxytocin receptor genes polymorphisms have been recentlyfound (Acevedo, Valencia, Lutter, & McAdams, 2015; Kim,Kim, Kim, Shin, & Treasure, 2015). The oxitocinergic systemshows a higher regulation level, involving some other neuro-peptides like leptin, which has been reported to decreaseoxytocin release (Kutlu et al., 2010). In addition, AN andBN patients present lower serum activity of the prolyl-endo-peptidase, an enzyme involved in oxytocin cleavage (Maeset al., 2001).
Role of neurohormones in EDs: the ghrelin/leptin system
GhrelinGhrelin, the ‘hunger hormone’, is a peptidic hormoneexpressed in humans by P/D sub 1 gland cells of the sto-mach (Rindi et al., 2002), with lower expression in pancreas,gallbladder, colon, liver, colon and lungs (Kojima, Hosoda,& Kangawa, 2001). Ghrelin is also expressed in the brain(Cowley et al., 2003), where it exerts a paracrine effect by acti-vating orexigenic NPY/AgRP neurons and inhibiting anorexi-genic POMC neurons, increasing appetite [reviewed inKageyama, Takenoya, Shiba, & Shioda (2010)]. However, newstudies do not indicate ghrelin central nervous system synthe-sis (Cabral, L�opez Soto, Epelbaum, & Perell�o, 2017). In anycase, ghrelin main secretion starts when the stomach is empty(Williams, Cummings, Grill, & Kaplan, 2003). Ghrelinincreases gastric secretion and gastrointestinal motility to pre-pare the body for food intake [reviewed in Kirsz & Zieba(2011)]. The ghrelin/growth hormone secretagogue receptor(GHSR) is the only ghrelin receptor known, being located inthe same brain areas than the leptin receptor (Perello et al.,2012). Its activation triggers the synthesis of NPY, increasingappetite albeit ghrelin treatment was ineffective as a singleappetite stimulatory treatment in AN patients (Miljic et al.,2006). Furthermore, the effects of ghrelin also involve thereward system activation throughout dopaminergic pathways,(see Dopamine section below and also Perello & Dickson,2015). It also exerts a neurogenic action in the hippocampus,facilitating learning and memory (Kim, Kim, & Park, 2017),and acts on the central nucleus of amygdala, where modulatesemotional arousal and feeding (Alvarez-Crespo et al., 2012).Surprisingly, several studies have reported elevated ghrelinlevels in AN patients (Blauwhoff-Buskermolen et al., 2017;Nakai et al., 2003; Tolle et al., 2003).
LeptinLeptin, the ‘satiety hormone’, is an adipocyte-derived hor-mone involved in the regulation of energy balance at bothlong- and short-term (Blundell, Goodson, & Halford, 2001).Leptin activity is exerted in the hypothalamic ARC, stimulat-ing anorexigenic neurons expressing POMC and cortico-tropin-release factor (CRF), and inhibiting orexigenic NPY/AgRP neurons (Baver et al., 2014; Flak & Myers, 2016). Theexistence of low levels of plasma leptin in cerebrospinal fluid(hypoleptinemia) is a key endocrinological feature of AN(F€ocker et al., 2011; Hebebrand et al., 1997). Hence, altera-tions in leptin homeostasis could be crucial in eating disor-ders. Indeed, reduced plasma circulating leptin levels werereported in AN and BN patients, but not in overweight BEDpatients. Interestingly, the inverse correlation was foundwhen measuring plasma-circulating levels of leptin receptorin the same groups. Conversely, an increased concentration ofNPY correlates to body mass deficiency coexisting with highconcentrations of leptin, suggesting disturbances in the regu-latory axis (Monteleone, Fabrazzo, Tortorella, Fuschino, &Maj, 2002). Reduced circulating leptin plasma levels but nor-mal leptin concentrations in subcutaneous adipose tissue werealso reported in acute ill AN girls (Dost�alov�a et al., 2005).
JOURNAL OF NEUROGENETICS 7
Dow
nloa
ded
by [
Uni
vers
ity o
f L
a L
agun
a V
icer
rect
orad
o] a
t 07:
00 0
1 A
ugus
t 201
7

In summary, data obtained from ghrelin and leptin indi-cate that an alteration in hormonal milieu is relevant in theprogression of eating disorders, highlighting the role ofphysiological compensatory mechanisms trying to minimisethe pathology extent.
Other appetite regulatorsIn addition to the peptides and hormones described above,other regulators play a role on appetite regulation, and theiralterations have been linked to EDs onset and progression.Cholecystokinin (CCK) is a peptidic hormone of the gastro-intestinal system that promotes satiety, but has been alsorelated with anxiety, panic and even hallucinations (Lenka,Arumugham, Christopher, & Pal, 2016; Zwanzger,Domschke, & Bradwejn, 2012). In a recent study, CCKexhibits similar plasma levels in AN patients compared tocontrol group both prior to and after a meal suggesting ahormonal adaptation (Cuntz et al., 2013). Inconsistently, inolder studies, plasma measurements performed in ANpatients showed a postprandial increase in CKK levels, sug-gesting an implication in this ED (Tomasik, Sztefko, &Starzyk, 2004). More data are clearly necessary to solve thisambiguity. In turn, Glucagon like peptide 1 (GLP-1) is abrain-gut peptide that exerts a hormone-neurotransmitteraction inhibiting food intake, energetic expenditure andinsulin levels (Richard et al., 2014; Shah & Vella, 2014). As asatiety inductor, GLP-1 interacts with the leptin and ghrelinsystem to induce satiation (Zhu et al., 2002), probably bydecreasing gastric emptying and acting on the brain to pro-duce a conditional taste aversion (Monteleone, Castaldo, &Maj, 2008). In AN patients, whereas GLP-1 was significantlydecreased compared with normal individuals, insulin andglucagon levels were increased, indicating an alteration inglucose homeostasis (Tomasik, Sztefko, Starzyk, Rogatko, &Szafran, 2005). In addition, punctual GLP-1 secretorydecrease was also found in BN patients compared to healthycontrols, being this concurrence limited to bingeing andvomiting events (Brambilla, Monteleone, & Maj, 2009).Other gut peptide, Peptide tyrosine tyrosine (PYY) belongsto NPY family and is secreted in ileum and colon with ananorexigenic role (Karra, Chandarana, & Batterham, 2009).PYY plasma concentrations increases within 15min after eat-ing and lasts approximately 90min (Batterham & Bloom,2003). Serum levels of PYY hormone are decreased inBN/BED compared with AN (Eddy et al., 2015). Finally,concerning opioid peptides, anandamide, also known asN-arachidonoylethanolamine (AEA), plays an important rolein feeding behaviour generating motivation and pleasure infood consumption (Fuss et al., 2015; Mahler, Smith, &Berridge, 2007). Anandamide and hence, the endocannabi-noid system, shows a therapeutic relevance in EDs. The can-nabinoid agonists can alleviate anorexia and nausea, whereasthe AEA mono-unsaturated analogue oleoylethanolamide(OEA) decreases food intake and body weight through acannabinoid receptor-independent mechanism (S Gaetani,Kaye, Cuomo, & Piomelli, 2008). In the same study, plasmalevels of anandamide were down-regulated in AN patients.As anandamide, other opioid peptides as hypothalamic
b-endorphin and dynorphin-A shown level changes in EDsanimal models (see Animal models section).
Dopamine and serotonin in EDs
Dopamine role in EDsDopamine is the most important regulator of reward behav-iours, including feeding and reproduction. These rewardbehaviours are conserved along phyla. In Drosophila, a smallgroup of dopaminergic neurons in the protocerebral anteriormedial (PAM) cluster send axons to the mushroom bodies(MBs), where appetitive olfactory associative memory isformed. After sugar ingestion, PAM dopaminergic neuronsare activated, generating a reward effect. These neuronsbecome overactivated under starving conditions (Liu et al.,2012). In mammals, abnormal function of mesocorticolimbicdopaminergic circuits impairs severely motivation andreward behaviours, contributing to pathological conditionssuch as depression, addictions, compulsive moods andapathy [reviewed in Castrioto, Thobois, Carnicella, Maillet,& Krack (2016)]. As an example, reward system responsive-ness is heightened in adolescent suffering AN when under-weight and after weight restoration (DeGuzman, Shott,Yang, Riederer, & Frank, 2017). These mesocorticolimbicdopaminergic alterations correlate with an abnormally highphysical activity in AN and BN patients (Hebebrand et al.,2003) and can trigger a dopamine-dependent stress response(Kalyanasundar et al., 2015). This convergence betweendopamine levels, physical activity pattern alterations and eat-ing disorders points out towards a dysfunction in the dopa-minergic neuromodulatory system. In addition, it exists aclear association between dopaminergic pathways and eatingdisorders with psychiatric comorbidities including depres-sion, anxiety, compulsive disorders and even aggressivebehaviours (Jennings, Wildes, & Coccaro, 2017; Martinussenet al., 2016). In the last years, neuroimaging has reporteddopaminergic alterations in ED patients (Berner, Winter,Matheson, Benson, & Lowe, 2017). As examples, positronemission tomography (PET) shows a [11C]raclopride bind-ing increase in ventral striatum in recovered AN patients(Frank et al., 2005), whereas AN patients display a poor acti-vation in prefrontal cortex (PFC) (Nagamitsu et al., 2011).Finally, nigrostriatal pathway is also involved in food intakeregulation, since the restoration of dopamine expression indopamine deficient mice causes hypophagia and bradykinesia(Hnasko et al., 2006).
Ghrelin, leptin and the dopamine-reward system: physio-logical roles and therapeutic potentialMany studies have been carried out to demonstrate thetherapeutic use of ghrelin in EDs with contradictory results:whereas some of them described that ghrelin administrationwas ineffective to increase the appetite in AN patients-prob-ably due to the high circulating ghrelin levels found in thesesubjects- (Miljic et al., 2006; Otto et al., 2001), others sug-gested that a ghrelin long-term treatment was efficient totreat AN patients (Hotta et al., 2009; Kawai et al., 2017). Inrodents, ghrelin injection increases food intake and triggers
8 GERM�AN CUESTO ET AL.
Dow
nloa
ded
by [
Uni
vers
ity o
f L
a L
agun
a V
icer
rect
orad
o] a
t 07:
00 0
1 A
ugus
t 201
7

dopamine release (Abizaid et al., 2006; Kawahara et al.,2009). It also prevents the development of activity basedanorexia in mice, confirming its role in the mesocorticolim-bic dopaminergic pathway (Legrand et al., 2016).
In turn, leptin is also involved in hedonic and rewardfeeding behaviour through mesocorticolimbic dopaminergicpathways, including NAc and ventral tegmental area (VTA).Whereas orexin coming from LH orexigenic neurons acti-vates VTA dopaminergic neurons, leptin reduces the LHorexin activation, lowers dopaminergic mesolimbic neuronsactivation, and decreases dopamine release in NAc, allthrough the activity of the neuropeptide galanin (Laqueet al., 2015). Thereby, leptin negatively modulates reward-related behaviour suppressing feeding (Leinninger et al.,2009). According to these findings, leptin antagonism mayrepresent a viable therapeutic strategy in ED.
Taken all these evidences together, the VTA to NAcdopaminergic projections can be considered as essential ele-ments of both ghrelin and leptin responsive circuits control-ling food reward behaviour, highlighting the complexity ofsignal integration within the VTA and locating this brainarea as a crucial target for therapeutically actions tacklingEDs (Skibicka et al., 2013).
Serotonin function in EDSerotonin (5-hydroxitriptamin or 5-HT) is a monoamineneurotransmitter produced in the brain by neurons locatedin the dorsal and median raphe nuclei projecting to corticaland striatal limbic regions. Serotonergic projections to hypo-thalamus are responsible of the satiety signal (Haleem &Haider, 1996) whereas projections to hippocampus, striatum,amygdala and frontal cortex are responsible of the moodregulation (Lambe, Fillman, Webster, & Shannon Weickert,2011; Mineur et al., 2015; Sumiyoshi, Kunugi, & Nakagome,2014). Serotonin modulates hunger, sleep, sex, emotions, andalso several endocrine processes (Haleem, 2012).Additionally, depressive, anxious, impulsive and obsessionalbehaviours, commonly related to ED, have been extensivelyrelated with serotonergic functions (Brewerton, 1992; Kaye,1997). AN and BN patients develop an egosyntonic personal-ity, implying that they do not perceive anything wrong withtheir acts. They consider their actions as reasonable andappropriate, perceiving their dysfunctional cognition regard-ing to their own weight and shape as perfectionism(Aardema, 2007). This particular trait shared between EDand other psychiatric diseases, taken together with the factthat medications acting over 5-HT pathways have somedegree of efficacy over AN and BN patients, suggests animportant role of serotonergic system dysfunction in EDonset and progression (Kaye, Bailer, Frank, Wagner, &Henry, 2005). Some authors directly assign to the serotoner-gic system the psychiatric symptomatic deteriorationobserved in AN and BN due to malnutrition, since trypto-phan (TRP), an essential amino acid only available in dietand precursor of 5-HT, is reduced in their diet (Haleem &Haider, 1996). The fact that re-feeding increases TRP plasmalevels in AN patients correlating with a decrease in depres-sive symptoms supports their theory (Gauthier et al., 2014).
Animal models employed on EDs research
A striking parallelism to the existence of brain neuropeptider-gic circuits controlling mechanisms of food intake/metabolismhomeostasis is found in other vertebrates as rodents but alsoin insects (Pool & Scott, 2014). Indeed, whereas NPY/AgRPneurons were proved to be involved in food intake stimulationin rats (Stanley, Kyrkouli, Lampert, & Leibowitz, 1986;Zarjevski, Cusin, Vettor, Rohner-Jeanrenaud, & Jeanrenaud,1993), energy expenditure decrement (Billington, Briggs,Grace, & Levine, 1991) and hedonic feeding (Pandit, la Fleur,& Adan, 2013), a homologue of the mammalian NPY wasdescribed in the insect model Drosophila melanogaster, theDrosophila NPF (Brown et al., 1999). Like NPY, DrosophilaNPF is expressed in only a small set of neurons in the fly brainmodulating neuronal circuits related to feeding behaviours,stress responses, metabolism, energy homeostasis, ethanolconsumption and also reproduction (Krashes et al., 2009;N€assel & Winther, 2010). In addition, the neuropeptide hugin,homologous to mammalian NeuromedinU, inhibits feedingbehaviour (Melcher & Pankratz, 2005). Subtypes of hugin neu-rons connect chemosensory to endocrine neurons producingthe Diuretic hormone 44 neuropeptide (Dh44), a homologueof the mammalian corticotropin-releasing hormone (CRH),responsible of the regulation of gut motility and excretion(Dus et al., 2015), and Drosophila insulin-like peptides(DILPs) (Kannan & Fridell, 2013). In turn, whereas dimin-ished signalling of DILPs affects food intake in flies, drosulfa-kinins (DSKs), cholecystokinin-like peptides, regulates satietyin Drosophila (S€oderberg, Carlsson, & N€assel, 2012).Interestingly, insulin-producing cells of the fly brain co-expresses both DILPs and DSKs, and each peptide affects thetranscript levels of the other suggesting a feedback regulationbetween two signalling pathways (S€oderberg et al., 2012).
With the help of the Drosophila sophisticated genetictoolkits and the deep knowledge of their sensory and centralnervous system circuitry, it is possible to further investigateand characterize neuropeptide function in food intake,energy balance and diet restriction, among other processes.Besides, the short life-cycle of Drosophila helps to assess therole of precocious aspects on food intake control.Furthermore, some recent methods developed in Drosophilahad made possible to precisely quantify food intake, facilitat-ing advances on the genetic, neural, and environmental fac-tors modulating food consumption (Deshpande et al., 2014).This knowledge will be crucial not only to delineate the gen-etic and neural mechanisms of metabolism and disordersconnected with food consumption, but also to identify evolu-tionarily conserved candidate genes and pathways relevant tohuman biology [see next section and Garlapow, Huang,Yarboro, Peterson, & Mackay (2015)].
Research using EDs animal models has also been highlyvaluable in the study of brain neurotransmitters and circuitryunderlying aberrant feeding behaviours. To date, somereward-related brain dysfunctions have been described onrodent animal models of AN, BN and BED, by affectingdopamine (DA), serotonin and acetylcholine (ACh) neuro-transmitters but also opioid levels (Avena & Bocarsly, 2012).Thus, in an AN rodent model based on activity, the activity-
JOURNAL OF NEUROGENETICS 9
Dow
nloa
ded
by [
Uni
vers
ity o
f L
a L
agun
a V
icer
rect
orad
o] a
t 07:
00 0
1 A
ugus
t 201
7

based anorexia (ABA) model (Routtenberg & Kuznesof,1967), a restricted access to food increases the reinforcingeffects of DA when the rat finally eat, suggesting alterations inmesolimbic DA and also serotonin as a result of starvation.In addition, b-endorphin levels are high in plasma fromABA rats, due to rises in hypothalamic b-endorphin anddynorphin-A (Aravich, Rieg, Lauterio, & Doerries, 1993).Likewise, eating palatable food releases DA in a BN model,whereas purge behaviour attenuates a signal of satietydependent on ACh release. In this BN model, binge eating iscombined with gastric sham feeding in the rat to incorporateboth bingeing behaviour and purging component aspects(Avena, Rada, Moise, & Hoebel, 2006). With respect to BED,several animal models are available, by offering limitedaccess to a palatable high-fat or high-sugar food, providingad libitum access to standard rodent chow for several weeks,by alternating cyclic periods of food deprivation and feedingor even by using foot-shocks to generate binge eating beha-viour in rats. Data generated from BED animal models haveyielded important insights to concomitant physiological andneurochemical alterations associated to binge. Thus, bingeeating of a 10% sucrose solution causes a repeated release ofDA in the NAc similar to changes observed with drugdependency and obesity and have also unveiled a role forNAc ACh in binge eating behaviour (Avena, Rada, &Hoebel, 2008; Rada, Avena, & Hoebel, 2005). Concerningthe opioid system, the use of opioid antagonists as naltre-xone or naloxone (among others) was able to decrease intakeof preferred fat and sucrose diets and also to suppress pala-table food intake (Boggiano et al., 2005; Naleid, Grace,Chimukangara, Billington, & Levine, 2007). Moreover, in arat BED model, memantine treatment fully blocked the com-pulsivity associated with the intake of the highly palatablefood, confirming the potential therapeutic role of this drugin curing aspects of BED in humans (Popik, Kos, Zhang, &Bisaga, 2011; Smith et al., 2015).
In addition, rat animal models shared characteristics withhuman patient psychopathologies, including EDs co-morbi-dities, helping to find novel preventions or treatments (Lutzet al., 1998). As an example, many representative featuresfound in AN patients can be mimicked in a rat model of com-bined food restriction and increased physical activity (theabovementioned ABA model). Food restricted rats exhibitedthis hyperactivity and low leptin levels seem to contribute tothe phenotype of these AN rats because hyperactivity can bereduced by leptin supplementation (Dixon, Ackert, & Eckel,2003; Hebebrand et al., 2003). Additionally, a rat model ofBED combines the use of intermittent food restriction withfrustration stress (Micioni Di Bonaventura et al., 2014) assess-ing stress-induced food-reward behaviours that are crucial inthe development of eating disorders in humans. Moreover, ratstrains can be used to study reward-driven mechanisms byinvolving progressive tests where animals needs to gain theirfood (i.e. by pressing a lever), being more active to obtain pal-atable food sources. In this context, reward-deficit syndromescan also be studied in rats whose dopamine synthesis or dopa-mine receptor signalling is disturbed (Gaetani et al., 2016).Remarkably, clinical findings and data obtained through neu-roimaging and pharmacotherapy studies of human
populations have supported and enhanced the informationderived from rat models.
Genetic approaches
Genetically, EDs are aggregated in families (Zerwas & Bulik,2011). Twins studies have provided an irrefutable proof,showing that the heritability of these disorders is 33–84% forAN, 28–83% for BN and 41–57% for BED (Munn-Chernoff& Baker, 2016). In 2003, Gorwood, Kipman, & Foulon(2003) published the first study indicating family burdenwithin these disorders, followed by others (Clarke, Weiss, &Berrettini, 2012; Helder & Collier, 2011; Thornton, Mazzeo,& Bulik, 2011; Treasure et al., 2015). Several works describedspecifically the family aggregation (Hudson et al., 2006;Lilenfeld, Ringham, Kalarchian, & Marcus, 2008; Munn-Chernoff & Baker, 2016). All of them confirm that EDs havea family burden. However, family studies are unable toaddress whether family-related factors are genetic and/orenvironmental (Zerwas & Bulik, 2011).
Genome-wide association studies
Genetic epidemiology transforms the way we look into theinfluence of genes and environmental factor in EDs.Genome-wide association studies (GWAS) show large scalegenetic studies of EDs that measure simultaneously hundredsof thousands of genetic variants scattered throughout thehuman genome. In the case of those specific for EDs,research focuses on single nucleotide polymorphisms (SNPs),traits, occurring more frequently in people with AN, BN orBED than in healthy people. Each study can look at hun-dreds or thousands of SNPs in several tentative traits at thesame time. GWAS represent a promising way to study com-plex, common diseases in which many genetic variationscontribute to a person’s risk, allowing effect-size estimatesfor specific genetic variants, testing shared genetics by loo-king for correlations in effect-sizes across traits and notrequiring measurements of multiple traits per individual.The most common methods in this type of studies isMendelian randomisation, which uses significantly associatedSNPs as instrumental variables to attempt quantify causalrelationships between risk factors and disease (Bulik-Sullivanet al., 2015). A complementary approach is to estimate gene-tic correlation, which includes the effects of all SNPs, includ-ing those that do not reach genome-wide significance.
Talking about EDs, one point is to demonstrate the familyburden of those disorders and something crucially differentis to establish – by GWAS studies – the relationshipsbetween those disorders with genetic traits. To date, thereare not significant genes associated with EDs. In early stud-ies, it was thought that a question of sample size could bethe problem for the lack of significance, but nowadays eventhe most powerful set of data in AN, by far the ED withmore genetic available studies, could not get any significantrelation with any genetic trait (Boraska et al., 2014).
As an example, Root et al. (2011) defined seven differentphenotypes which are known to be associated with AN
10 GERM�AN CUESTO ET AL.
Dow
nloa
ded
by [
Uni
vers
ity o
f L
a L
agun
a V
icer
rect
orad
o] a
t 07:
00 0
1 A
ugus
t 201
7

(drive for thinness, concern over mistakes, among others).They tried to correlate those phenotypes with 5151 SNPS in182 genes, but they were unable to significantly associate anySNPs with EDs psychological traits despite the huge samplesize: 1085 EDs participants and 677 controls (Root et al.,2011). However, in despite the fact that they fail to makeany significant association, they described two SNPS withpotential interest in future studies: (i) rs17719880 in KCNN3(potassium calcium activated channel), an important gene inneuronal excitability that could be related with schizophreniaand bipolar disorders and (ii) rs12744840 in HCRTR1,an orexin receptor gene (Sakurai et al., 1998).
Another genetic study was performed on 1533 twinAmerican women focusing in the analysis of 15 polymor-phisms in HTR2A, a gene implicated in appetite process andsatiety in BED (Koren et al., 2014). In this study, theauthors describe three main polymorphism for HTR2A:(i)� 1438G/A (rs6311) which have been associated withpoor treatment response in BN patients but the authorsfailed to find a significant genetic association with EDs char-acteristics and (ii) two other polymorphisms, rs6561333 andrs2296972, associated with less likelihood of BED. However,when those polymorphisms were corrected for multiple test-ing they were no longer significant; with only rs2296972remain significant as trend level (Koren et al., 2014).Likewise, the authors did not find any comorbidity betweenMDD (Mayor Depressive Disorder) and EDs.
Some cross-trait studies (Hinney et al., 2017) obtained asignificant genetic relationship with AN and body massindex (BMI) using a ‘cross-talking’ with two big GWAS, onefor AN (Boraska et al., 2014) and one for BMI (Locke et al.,2015), demonstrating the existence of gender correlationbetween the trait and those diseases. Indeed, in AN, 90% ofthe people affected are females (Yilmaz, Hardaway, & Bulik,2015) and BN is also gender specific, affecting mainly femalepopulation. Remarkably, there are almost no EDs studiesconducted with men (Munn-Chernoff & Baker, 2016).
As stated previously, Hinney et al. (2017) describedthree significantly altered loci correlating AN risk withincreased BMI. The genes associated to those loci areCTBP2, CCNE1, CARF and NBEAL1 but their relevance inAN risk mechanisms or BMI increases are still uncertain.Other comorbid interesting study with significant results isthe one performed by Munn-Chernoff and Baker (2016).They associate EDs to substance use disorders (SUD),describing a possible unbalance in the system and loss ofcontrol (negative valence domain). This loss control is acore feature of BED as well as SUD and could be influ-enced by dopamine. In addition, a recent study describethat AN patients could present an unbalance in the rewardsystem involving dopamine circuits (see dopamine section),describing a marginally genetic association between AN andexcessive exercise, a rs17030795 located in PPP3CA(Gorwood et al., 2016). By their side, OPRD1 (opioid deltareceptor) and HTR1D (1D serotonin receptor) are beenassociated with AN by Bergen et al. (2003) and Wanggroups (Wang et al., 2011) confirming this association,although not backed by significant results. Other geneshave been under the spot light and come out in GWAS
studies, but they fail to get significance. They are: (i)DRD2/ANKK1 gene and SNPs Val58Met in COMT gene,implicated in dopamine (Munn-Chernoff & Baker, 2016);(ii) 5-HTTLPR in 5HTT transporter and HTR2A receptorgene in serotonin path (Munn-Chernoff & Baker, 2016;Yilmaz et al., 2015) and (iii) SOX2 gene, in this case thestudy with a comorbidity of EDs and bipolar disorder(Bulik, Kleiman, & Yilmaz, 2016).
Finally, Munn-Chernoff et al. (2015) review deeply thepossible genetic overlap between alcohol use disorder (AUD)and bulimic behaviour, not obtaining statistical significancetowards EDs. Although specific genetic mechanism underly-ing comorbidity are unclear, at minimum, individuals withAUD should be screened for individual and family history ofEDs and vice versa, regardless of race. Even when the studyis unable to provide any statistically significant data, it isclear that AUD and bulimic behaviour share environmentalinfluences.
There could be several explanations for the lack of signifi-cance concerning GWAS studies in EDs. One is the potentialpopulation stratification, probably because we are not usingthe appropriate phenotypes to separate the patients. Theother one could be the sample size. As an example, inSchizophrenia studies, only a sample size of 5000 partici-pants allowed to obtain differences in genes with statisticalsignificance. Finally, it is necessary to consider the study ofEDs as comorbid with other disorders; alcohol abuse, sub-stance abuse, bipolar disorder, emotional instability, andobesity (Yilmaz et al., 2015).
Epigenetic studies
Epigenetic refers to heritable patterns of gene expression thatoccur without changes in the DNA sequence, that is, changesin phenotype not involving changes in genotype. Epigeneticshave a major role in genomic regulation, as a natural processwhich silence specific genes during development. At leastthree systems; DNA methylation, histone modification andnon-coding RNA (ncRNA)-associated gene silencing havebeen currently considered to initiate and sustain epigeneticchange (Brown et al., 2007; Campbell, Mill, Uher, &Schmidt, 2011; Egger, Liang, Aparicio, & Jones, 2004). Thefield of epigenetics is quickly growing and with it the under-standing that both the environment and individual lifestylecan also directly interact with the genome. For example,human epidemiological studies have provided evidence thatprenatal and early postnatal environmental factors influencethe adult risk of developing various chronic diseases andbehavioural disorders (Jirtle & Skinner, 2007; Pjetri,Schmidt, Kas, & Campbell, 2012).
Epigenetics changes play a role in causation of complexadult psychiatric and neurodegenerative disorders, with rear-rangements in DNMT (DNA-methyltransferase) genes.Recent evidence supports the idea that epigenetic mechanismmay help initiate and maintain EDs (Strober, Peris, &Steiger, 2014), for example AN has been genetically corre-lated with Schizophrenia (Bulik-Sullivan et al., 2015).Epigenetics modifications have a key role in the genetic
JOURNAL OF NEUROGENETICS 11
Dow
nloa
ded
by [
Uni
vers
ity o
f L
a L
agun
a V
icer
rect
orad
o] a
t 07:
00 0
1 A
ugus
t 201
7

bases of the EDs owing to early life events, or familiar envir-onment (Munn-Chernoff & Baker, 2016). Epigenetic mech-anism also occurs during pregnancy, for example maternaldepression have been linked to specific increases in methyla-tion of offspring glucocorticoid receptor (NR3C1) gene,yielding to altered cortisol responses and increased stressreactivity in the offspring (Steiger & Thaler, 2016).
As mentioned previously, there is an imbalance in thedopamine reward circuit in EDs. Some epigenetics changescould be related with this mechanism. Indeed, Frieling et al.(2010) described higher levels of methylation in the promo-tors of DAT1 (dopamine active transporter 1) and DRD2(dopamine receptor D2) in AN patients compared withhealthy controls, indicating an increase in the expression ofthe DAT1 and a decrease in the expression of the DRD2.Other studies linked AN weight loss to hypermethylationand reduced expression of POMC (proopiomelanocortin)gene (Ehrlich et al., 2010; Steiger & Thaler, 2016). In add-ition, several studies carried out in BN women patientsassessed the methylation status of specific genes showing: (i)hypermethylation in exon 1C region of the glucocorticoidreceptor (GR) with comorbid BN and suicidal records; (ii)hypermethylation of the DRD2 promoter region with BN
and Borderline Personality Disorder and (iii) hypermethyla-tion of specific CpG sites in the BDNF gene promoter regionwith BN, with and without childhood abuse (Groleau et al.,2014; Steiger, Labont�e, Groleau, Turecki, & Israel, 2013;Thaler et al., 2014).
Recently, several studies have investigated directly gen-ome-wide (GW) methylation in patients with EDs (Saffrey,Novakovic, & Wade, 2014; Tremolizzo et al., 2014). Thus,Booij and colleagues reported that a group of AN patientshad higher mean and median global methylation level whencompared to normal eaters. In this study, they also describedsignificant group differences in 2 CpGs associated withNR1H3 gene and 3 CpGs associated with PXDNL gene, bothgenes involved in dopamine and glutamate signallingrespectively and, hence, in reward dependence, mood andanxiety (Booij et al., 2015).
Transcriptome studies
Expression studies have been used mainly to confirm epigen-etic imbalances, or SNPs detected. Using transcriptomics, arecent study has shown how binge eating resulted in thedownregulation of a set of genes involved in decreased
Table 1. Genetic studies on eating disorders.
Study Type Disorder Results
Bergen et al. (2003) GWAS AN OPRD1, HTR1DBrown et al. (2007) SNPs AN OPRD1, HTR1DWang et al. (2011) GWAS AN OPRD1, HTR1D, CNV, the only oneBoraska et al. (2014) GWAS AN No statistical significant dataTremolizzo et al. (2014) Epigenetics AN No significant data, but less methylated DNA in
fasting patient vs control. Correlating withplasma leptin and steroid hormone
Frieling et al. (2010) Epigenetics AN Hypermethylation in DAT1 (high express), DRD2(low express)
Kern et al. (2012) Mouse models AN Mouse wt and ghrelin-/- treated with DRD2inhibitors develop anorexia
Krajmalnik-Brown et al. (2012) Metagenomics Obesity & Anorexia Microbioma study (obesity vs undernutrition)Scott-Van Zeeland et al. (2014) Targeted sequencing AN EPHX2 variants related with susceptibility to ANCui et al. (2013) Targeted sequencing,
(WGS and WES)AN and BN Mutations in ESRRA and HDAC4 increase the
risk of EDsBooij et al. (2015) Epigenetics AN AN have higher methylation level than controls:
(NR1H3 and PXDNL)Wade et al. (2013) GWAS EDs No significant but important genes: CLEC5A,
LOC136242, TSHZ1, SYTL5 for AN NT5C1B forBN and ATP8A2 for BED
Boraska et al. (2012) GWAS ED general Not significant but important: RUFY1, CCNL1,SEMA6D, SHC4, DLGAP1, SDPR, TRPS1 in EDsphenotypes
Munn-Chernoff and Baker (2016) GWAS EDs(BN) & SUD DRD2/ANKK1, and SNPs Val58Met in COMTYilmaz et al. (2015) GWAS AN DRD2/ANKK1, and SNPs Val58Met in COMTBulik et al. (2016) GWAS AN SOX2Munn-Chernoff et al. (2015) GWAS AUD & BN No statistical significant genesRoot et al. (2011) GWAS EDs psychological phenotypes No significant association, but important:
KCNN3, HCRTR1Koren et al. (2014) GWAS BED No significant when FDR correction is applied,
HTR2AHinney et al. (2017) Meta-analysis GWAS AN and BMI CTBP2, CCNE1, CARF and NBEAL1Gorwood et al. (2016) GWAS AN & excessive exercise PPP3CA, DRD2Steiger & Thaler (2016) Epigenetics EDs Hypermethylation NR3C1, POMC (low
expression)Ehrlich et al. (2010) Epigenetic AN Hypermethylation POMC (low expression)Groleau et al. (2014) Epigenetics BN and suicidality history Hypermethylation in exon 1C region of GRSteiger et al. (2013) Epigenetics BN and Border Line personality Hypermethylation of DRD2 promoterThaler et al. (2014) Epigenetics BN and childhood abuse Hypermethylation in CpG sites in the BDNF
promoterClarke et al. (2016) Targeted Sequencing AN No significant, but important mutation in BDNF
This table summarizes most of the genetics studies carried out in EDs. Columns show respectively authors, the type of genetic approach employed and the mainresults obtained.
12 GERM�AN CUESTO ET AL.
Dow
nloa
ded
by [
Uni
vers
ity o
f L
a L
agun
a V
icer
rect
orad
o] a
t 07:
00 0
1 A
ugus
t 201
7

myelination as well as oligodendrocyte differentiation andexpression (Kirkpatrick et al., 2017).
To conclude, even though there is an absence of signifi-cant correlation between EDs phenotypic characteristics andspecific genetic trait, it is obvious that there exist a geneticimbalance which leads first to a pathway disparity, finallyending in an aberrant eating behaviour. Table 1 summarisesmost of the studies devoted to EDs, describing the type ofgenetic approach employed and the main result of the study.Undoubtedly, more epigenetic studies of those disorderswhich are crucially influenced by environmental circumstan-ces during early childhood development are mandatory foruncover the origins of these diseases.
Wrap-up and synthesis: towards a global approach
This review focused on three illnesses responsible of a high-increasing and extremely frequent phenomenon related toour daily way of living: pathologies associating to feedingdysfunctions. Besides, these EDs are complexes, affecting notonly nutritional and physiological features but also socialcognitive processes, psychological, mental and clinicalaspects, reducing the life-quality of millions of worldwideinhabitants and generating a profound social impact. In spiteof this fact, EDs tend to be exclusively considered as psychi-atric disorders, existing nowadays a profound imbalancebetween psychological and biological therapies. In addition,psychological help is not effective to achieve a fully physicaland emotional recovery in most of the cases (Halmi, 2013).Concerning clinical treatment, unfortunately, to date, onlytwo drugs (fluoxetine and lisdexamfetamine, respectively forBN and BED treatment) have been approved by the FDAand the international regulatory agencies for the treatmentof EDs. Furthermore, there is a major lack of pharmacother-apy studies and treatments in children and teenagers suffer-ing from EDs. Under these grounds, a scientificmultidisciplinary effort is mandatory to overcome this chal-lenge. The combination of genomics and epigenomics toidentify new genes and biomarkers, the involvement of bio-informatics analysis to provide an integrative overview andgenerate a network interaction between SNPs and epigeneticmodulation and the deep characterization of the neuropepti-des, neurotransmitters and hormones involved will allow abetter understanding of EDs. In parallel, computational dataand the creation of new databases will allow the develop-ment of molecules targeting specifically neuromodulators-and hormones-mediated signalling pathways involved inthese illnesses. Finally, tailor medicine approaches based ongenetic individual differences must be also applied in EDspatients. Indeed, an accurate diagnosis should include a gen-etic and epigenetic study accompanied by a family retro-spective revision, to understand the specific circumstances ineach case and the possible genetic imbalance, identifying alist of genes as a first option to check for SNPs or epigeneticderegulation. This genetic imbalance would affect the regula-tion and function of neuromodulators and hormones in thebrain and/or other organs, ultimately generating abnormal-ities in eating behaviours. For all these reasons, we stronglybelieve that it is urgent to develop a different way of
approach those disorders, which affects not only the patientsbut also the families and their environmental influences.
Acknowledgements
We appreciate the help of Dr. Cristina Martin-Higueras and laboratorymembers for their critical comments. This publication was supportedby the Spanish National Programme for Research aimed at theChallenges of Society [DPI2015–66458-C2–2-R, MINECO] to AA andGC, an AIRC-iCARE Fellowship co-funded by European Communityto LG and the CNRS, INRA, Burgundy Regional Council (PARI2012and 2014) and University of Bourgogne Franche-Comt�e to CE.
Disclosure statement
No potential conflict of interest was reported by the authors.
Funding
This publication was supported by the Spanish National Programmefor Research aimed at the Challenges of Society [DPI2015–66458-C2–2-R, MINECO] to AA and GC, an AIRC-iCARE Fellowship co-funded byEuropean Community to LG and the CNRS, INRA, Burgundy RegionalCouncil (PARI2012 and 2014) and University of Bourgogne Franche-Comt�e to CE.
ORCID
Leticia G. Le�on http://orcid.org/0000-0001-8781-7424Angel Acebes http://orcid.org/0000-0003-0020-1913
References
Aardema, F. O. (2007). The menace within: obsessions and the self.International Journal of Cognitive Therapy, 21, 182–197. doi:10.1891/088983907781494573
Abizaid, A., Liu, Z.-W., Andrews, Z.B., Shanabrough, M., Borok, E.,Elsworth, J.D., … Horvath, T.L. (2006). Ghrelin modulates theactivity and synaptic input organization of midbrain dopamine neu-rons while promoting appetite. Journal of Clinical Investigation, 116,3229–3239. doi: 10.1172/JCI29867
Acevedo, S.F., Valencia, C., Lutter, M., & McAdams, C.J. (2015).Severity of eating disorder symptoms related to oxytocin receptorpolymorphisms in anorexia nervosa. Psychiatry Research, 228,641–648. doi: 10.1016/j.psychres.2015.05.040
Adan, R.A.H., Vanderschuren, L.J.M.J., & la Fleur, S.E. (2008). Anti-obes-ity drugs and neural circuits of feeding. Trends in PharmacologicalSciences, 29, 208–217. doi: 10.1016/j.tips.2008.01.008
Agras, W.S., Rossiter, E.M., Arnow, B., Schneider, J.A., Telch, C.F.,Raeburn, S.D., … Koran, L.M. (1992). Pharmacologic and cognitive-behavioral treatment for bulimia nervosa: A controlled comparison.American Journal of Psychiatry, 149, 82–87. doi: 10.1176/ajp.149.1.82
Aigner, M., Treasure, J., Kaye, W., & Kasper, S. & WFSBP Task ForceOn Eating Disorders. (2011). World Federation of Societies ofBiological Psychiatry (WFSBP) guidelines for the pharmacologicaltreatment of eating disorders. World Journal of Biological Psychiatry,12, 400–443. doi: 10.3109/15622975.2011.602720
Altirriba, J., Poher, A.-L., & Rohner-Jeanrenaud, F. (2015). Chronicoxytocin Administration as a treatment against impaired leptin sig-naling or leptin resistance in obesity. Frontiers in Endocrinology, 6,119. doi: 10.3389/fendo.2015.00119
Altman, S.E., & Shankman, S.A. (2009). What is the association betweenobsessive–compulsive disorder and eating disorders? ClinicalPsychology Review, 29, 638–646. doi: 10.1016/j.cpr.2009.08.001
JOURNAL OF NEUROGENETICS 13
Dow
nloa
ded
by [
Uni
vers
ity o
f L
a L
agun
a V
icer
rect
orad
o] a
t 07:
00 0
1 A
ugus
t 201
7

Alvarez-Crespo, M., Skibicka, K.P., Farkas, I., Moln�ar, C.S., Egecioglu, E.,Hrabovszky, E., … Dickson, S.L. (2012). The amygdala as a neurobio-logical target for ghrelin in rats: Neuroanatomical, electrophysiologicaland behavioral evidence. PLoS One, 7, e46321. doi: 10.1371/journal.pone.0046321
American Psychiatric Association. (2013). Diagnostic and statisticalmanual of mental disorders. (5th ed.). Arlington, VA: AmericanPsychiatric Publishing.
Aponte, Y., Atasoy, D., & Sternson, S.M. (2011). AGRP neurons aresufficient to orchestrate feeding behavior rapidly and without train-ing. Nature Neuroscience, 14, 351–355. doi: 10.1038/nn.2739
Appolinario, J.C., Bacaltchuk, J., Sichieri, R., Claudino, A.M., Godoy-Matos, A., Morgan, C., … Coutinho, W. (2003). A randomized,double-blind, placebo-controlled study of sibutramine in the treat-ment of binge-eating disorder. Archives of General Psychiatry, 60,1109–1116. doi: 10.1001/archpsyc.60.11.1109
Aravich, P.F., Rieg, T.S., Lauterio, T.J., & Doerries, L.E. (1993). Beta-endorphin and dynorphin abnormalities in rats subjected to exerciseand restricted feeding: Relationship to anorexia nervosa? BrainResearch, 622, 1–8. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/790218710.1016/0006-8993(93)90794-N
Armougom, F., Henry, M., Vialettes, B., Raccah, D., & Raoult, D. (2009).Monitoring bacterial community of human gut microbiota reveals anincrease in Lactobacillus in obese patients and methanogens in anor-exic patients. PloS One, 4, e7125. doi: 10.1371/journal.pone.0007125
Arnold, L.M., McElroy, S.L., Hudson, J.I., Welge, J.A., Bennett, A.J., &Keck, P.E. (2002). A placebo-controlled, randomized trial of fluoxet-ine in the treatment of binge-eating disorder. Journal of ClinicalPsychiatry, 63, 1028–1033. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/1244481710.4088/JCP.v63n1113
Atasoy, D., Betley, J.N., Su, H.H., & Sternson, S.M. (2012).Deconstruction of a neural circuit for hunger. Nature, 488, 172–177.doi: 10.1038/nature11270
Avena, N.M., & Bocarsly, M.E. (2012). Dysregulation of brain reward sys-tems in eating disorders: Neurochemical information from animalmodels of binge eating, bulimia nervosa, and anorexia nervosa.Neuropharmacology, 63, 87–96. doi: 10.1016/j.neuropharm.2011.11.010
Avena, N.M., Rada, P., & Hoebel, B.G. (2008). Underweight rats haveenhanced dopamine release and blunted acetylcholine response inthe nucleus accumbens while bingeing on sucrose. Neuroscience, 156,865–871. doi: 10.1016/j.neuroscience.2008.08.017
Avena, N.M., Rada, P., Moise, N., & Hoebel, B.G. (2006). Sucrose shamfeeding on a binge schedule releases accumbens dopamine repeatedlyand eliminates the acetylcholine satiety response. Neuroscience, 139,813–820. doi: 10.1016/j.neuroscience.2005.12.037
Bacaltchuk, J., & Hay, P. (2001). Antidepressants versus placebo forpeople with bulimia nervosa. The Cochrane Database of SystematicReviews, CD003391. doi: 10.1002/14651858.CD003391
Bakhtazad, A., Vousooghi, N., Garmabi, B., & Zarrindast, M.R. (2016).CART peptide and opioid addiction: Expression changes in male ratbrain. Neuroscience, 325, 63–73. doi: 10.1016/j.neuroscience.2016.02.071
Barlow, J., Blouin, J., Blouin, A., & Perez, E. (1988). Treatment of buli-mia with desipramine: A double-blind crossover study. CanadianJournal of Psychiatry. Revue Canadienne De Psychiatrie, 33, 129–133.Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/328463010.1177/070674378803300211
Barth, K.S., & Malcolm, R.J. (2010). Disulfiram: An old therapeuticwith new applications. CNS & Neurological Disorders Drug Targets,9, 5–12. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/2020181010.2174/187152710790966678
Batterham, R.L., & Bloom, S.R. (2003). The gut hormone peptide YYregulates appetite. Annals of the New York Academy of Sciences, 994,162–168. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/1285131210.1111/j.1749-6632.2003.tb03176.x
Baver, S.B., Hope, K., Guyot, S., Bjørbaek, C., Kaczorowski, C., &O’connell, K.M.S. (2014). Leptin modulates the intrinsic excitabilityof AgRP/NPY neurons in the arcuate nucleus of the hypothalamus.Journal of Neuroscience, 34, 5486–5496. doi: 10.1523/JNEUROSCI.4861-12.2014
Becker, D.F., & Grilo, C.M. (2015). Comorbidity of mood and sub-stance use disorders in patients with binge-eating disorder:Associations with personality disorder and eating disorder pathology.Journal of Psychosomatic Research, 79, 159–164. doi: 10.1016/j.jpsychores.2015.01.016
Bergen, A.W., van den Bree, M.B.M., Yeager, M., Welch, R., Ganjei,J.K., Haque, K., … Kaye, W.H. (2003). Candidate genes for anorexianervosa in the 1p33-36 linkage region: Serotonin 1D and delta opi-oid receptor loci exhibit significant association to anorexia nervosa.Molecular Psychiatry, 8, 397–406. doi: 10.1038/sj.mp.4001318
Berner, L.A., Winter, S.R., Matheson, B.E., Benson, L., & Lowe, M.R.(2017). Behind binge eating: A review of food-specific adaptations ofneurocognitive and neuroimaging tasks. Physiology & Behavior, 176,59–70. doi: 10.1016/j.physbeh.2017.03.037
Billington, C.J., Briggs, J.E., Grace, M., & Levine, A.S. (1991). Effects ofintracerebroventricular injection of neuropeptide Y on energy metab-olism. American Journal of Physiology, 260(2 Pt 2), R321–R327.Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/1996719
Blauwhoff-Buskermolen, S., Langius, J.A.E., Heijboer, A.C., Becker, A.,de van der Schueren, M.A.E., & Verheul, H.M.W. (2017). Plasmaghrelin levels are associated with anorexia but not cachexia inpatients with NSCLC. Frontiers in Physiology, 8, 119. doi: 10.3389/fphys.2017.00119
Blevins, J.E., Graham, J.L., Morton, G.J., Bales, K.L., Schwartz, M.W.,Baskin, D.G., & Havel, P.J. (2015). Chronic oxytocin administrationinhibits food intake, increases energy expenditure, and producesweight loss in fructose-fed obese rhesus monkeys. American Journalof Physiology, Regulatory, Integrative and Comparative Physiology,308, R431–R438. doi: 10.1152/ajpregu.00441.2014
Blundell, J.E., Goodson, S., & Halford, J.C. (2001). Regulation of appe-tite: Role of leptin in signalling systems for drive and satiety.International Journal of Obesity and Related Metabolic Disorders, 25Suppl 1, S29–S34. doi: 10.1038/sj.ijo.0801693
Boersma, G.J., Liang, N.-C., Lee, R.S., Albertz, J.D., Kastelein, A.,Moody, L.A., … Tamashiro, K.L. (2016). Failure to upregulate Agrpand Orexin in response to activity based anorexia in weight loss vul-nerable rats characterized by passive stress coping and prenatal stressexperience. Psychoneuroendocrinology, 67, 171–181. doi: 10.1016/j.psyneuen.2016.02.002
Boggiano, M.M., Chandler, P.C., Viana, J.B., Oswald, K.D., Maldonado,C.R., & Wauford, P.K. (2005). Combined dieting and stress evokeexaggerated responses to opioids in binge-eating rats. BehavioralNeuroscience, 119, 1207–1214. doi: 10.1037/0735-7044.119.5.1207
Booij, L., Casey, K.F., Antunes, J.M., Szyf, M., Joober, R., Isra€el, M., &Steiger, H. (2015). DNA methylation in individuals with anorexianervosa and in matched normal-eater controls: A genome-widestudy. International Journal of Eating Disorders, 48, 874–882. doi:10.1002/eat.22374
Boraska, V., Davis, O.S.P., Cherkas, L.F., Helder, S.G., Harris, J., Krug,I., … Zeggini, E. (2012). Genome-wide association analysis of eatingdisorder-related symptoms, behaviors, and personality traits.American Journal of Medical Genetics. Part B, NeuropsychiatricGenetics?: The Official Publication of the International Society ofPsychiatric Genetics, 159B, 803–811. doi: 10.1002/ajmg.b.32087
Boraska, V., Franklin, C.S., Floyd, J.A.B., Thornton, L.M., Huckins,L.M., Southam, L., … Bulik, C.M. (2014). A genome-wide associ-ation study of anorexia nervosa. Molecular Psychiatry, 19,1085–1094. doi: 10.1038/mp.2013.187
Borgland, S.L., Chang, S.-J., Bowers, M.S., Thompson, J.L., Vittoz, N.,Floresco, S.B., … Bonci, A. (2009). Orexin A/hypocretin-1 selectivelypromotes motivation for positive reinforcers. Journal of Neuroscience,29, 11215–11225. doi: 10.1523/JNEUROSCI.6096-08.2009
Brambilla, F., Monteleone, P., & Maj, M. (2009). Glucagon-like peptide-1 secretion in bulimia nervosa. Psychiatry Research, 169, 82–85. doi:10.1016/j.psychres.2008.06.040
Brennan, B.P., Roberts, J.L., Fogarty, K.V., Reynolds, K.A., Jonas, J.M.,& Hudson, J.I. (2008). Memantine in the treatment of binge eatingdisorder: An open-label, prospective trial. International Journal ofEating Disorders, 41, 520–526. doi: 10.1002/eat.20541
14 GERM�AN CUESTO ET AL.
Dow
nloa
ded
by [
Uni
vers
ity o
f L
a L
agun
a V
icer
rect
orad
o] a
t 07:
00 0
1 A
ugus
t 201
7

Breton, J., Legrand, R., Akkermann, K., J€arv, A., Harro, J., D�echelotte,P., & Fetissov, S.O. (2016). Elevated plasma concentrations of bacter-ial ClpB protein in patients with eating disorders. InternationalJournal of Eating Disorders, 49, 805–808. doi: 10.1002/eat.22531
Brewerton, T. (1992). Serotonin function in depression: Effects of sea-sonality? American Journal of Psychiatry, 149, 1277. Retrieved fromhttp://www.ncbi.nlm.nih.gov/pubmed/1482444
Brewerton, T.D. (2012). Antipsychotic agents in the treatment of ano-rexia nervosa: neuropsychopharmacologic rationale and evidencefrom controlled trials. Current Psychiatry Reports, 14, 398–405. doi:10.1007/s11920-012-0287-6
Broberger, C., Johansen, J., Johansson, C., Schalling, M., & H€okfelt, T.(1998). The neuropeptide Y/agouti gene-related protein (AGRP)brain circuitry in normal, anorectic, and monosodium glutamate-treated mice. Proceedings of the National Academy of Sciences of theUnited States of America, 95, 15043–15048. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/9844012
Brodie, M.J., Ben-Menachem, E., Chouette, I., & Giorgi, L. (2012).Zonisamide: Its pharmacology, efficacy and safety in clinical trials. ActaNeurologica Scandinavica. Supplementum, 126, 19–28. doi: 10.1111/ane.12016
Brown, K.M.O., Bujac, S.R., Mann, E.T., Campbell, D.A., Stubbins, M.J.,& Blundell, J.E. (2007). Further evidence of association of OPRD1 &HTR1D polymorphisms with susceptibility to anorexia nervosa.Biological Psychiatry, 61, 367–373. doi: 10.1016/j.biopsych.2006.04.007
Brown, M.R., Crim, J.W., Arata, R.C., Cai, H.N., Chun, C., & Shen, P.(1999). Identification of a Drosophila brain-gut peptide related tothe neuropeptide Y family. Peptides, 20, 1035–1042. Retrievedfrom http://www.ncbi.nlm.nih.gov/pubmed/1049942010.1016/S0196-9781(99)00097-2
Bulik-Sullivan, B., Finucane, H.K., Anttila, V., Gusev, A., Day, F.R.,Loh, P.-R. … Neale, (2015). An atlas of genetic correlations acrosshuman diseases and traits. Nature Genetics, 47, 1236–1241. doi:10.1038/ng.3406
Bulik, C.M., Kleiman, S.C., & Yilmaz, Z. (2016). Genetic epidemiologyof eating disorders. Current Opinion in Psychiatry, 29, 383–388. doi:10.1097/YCO.0000000000000275
Bulik, C.M., Sullivan, P.F., Tozzi, F., Furberg, H., Lichtenstein, P., &Pedersen, N.L. (2006). Prevalence, heritability, and prospective riskfactors for anorexia nervosa. Archives of General Psychiatry, 63,305–312. doi: 10.1001/archpsyc.63.3.305
Cabral, A., L�opez Soto, E., Epelbaum, J., & Perell�o, M. (2017). Is ghrelinsynthesized in the central nervous system? International Journal ofMolecular Sciences, 18, 638. doi: 10.3390/ijms18030638
Camardese, G., Picello, A., & Bria, P. (2008). Venlafaxine: Successfultreatment in impulsive disorders. Psychiatry and ClinicalNeurosciences, 62, 241–242. doi: 10.1111/j.1440-1819.2008.01763.x
Campbell, I.C., Mill, J., Uher, R., & Schmidt, U. (2011). Eating disorders,gene-environment interactions and epigenetics. Neuroscience andBiobehavioral Reviews, 35, 784–793. doi: 10.1016/j.neubiorev.2010.09.012
Capasso, A., Petrella, C., & Milano, W. (2009). Pharmacological profileof SSRIs and SNRIs in the treatment of eating disorders. CurrentClinical Pharmacology, 4, 78–83. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/1914950610.2174/157488409787236092
Cardi, V., Corfield, F., Leppanen, J., Rhind, C., Deriziotis, S.,Hadjimichalis, A., … Treasure, J. (2015). Emotional processing, rec-ognition, empathy and evoked facial expression in eating disorders:An experimental study to map deficits in social cognition. PLoS One,10, e0133827. doi: 10.1371/journal.pone.0133827
Cardinal, P., Bellocchio, L., Guzm�an-Quevedo, O., Andr�e, C., Clark, S.,Elie, M., … Cota, D. (2015). Cannabinoid type 1 (CB1) receptorson Sim1-expressing neurons regulate energy expenditure in malemice. Endocrinology, 156, 411–418. doi: 10.1210/en.2014-1437
Castrioto, A., Thobois, S., Carnicella, S., Maillet, A., & Krack, P. (2016).Emotional manifestations of PD: Neurobiological basis. MovementDisorders, 31, 1103–1113. doi: 10.1002/mds.26587
Chronwall, B.M., DiMaggio, D.A., Massari, V.J., Pickel, V.M., Ruggiero,D.A., & O’donohue, T.L. (1985). The anatomy of neuropeptide-Y-containing neurons in rat brain. Neuroscience, 15, 1159–1181.Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/3900805
Cifani, C., Polidori, C., Melotto, S., Ciccocioppo, R., & Massi, M.(2009). A preclinical model of binge eating elicited by yo-yo dietingand stressful exposure to food: effect of sibutramine, fluoxetine, top-iramate, and midazolam. Psychopharmacology, 204, 113–125. doi:10.1007/s00213-008-1442-y
Clarke, J., Ramoz, N., Fladung, A.-K., & Gorwood, P. (2016). Higherreward value of starvation imagery in anorexia nervosa and associ-ation with the Val66Met BDNF polymorphism. TranslationalPsychiatry, 6, e829. doi: 10.1038/tp.2016.98
Clark, J.T., Kalra, P.S., Crowley, W.R., & Kalra, S.P. (1984).Neuropeptide Y and human pancreatic polypeptide stimulate feedingbehavior in rats. Endocrinology, 115, 427–429. doi: 10.1210/endo-115-1-427
Clarke, T.K., Weiss, A.R.D., & Berrettini, W.H. (2012). The genetics ofanorexia nervosa. Clinical Pharmacology and Therapeutics, 91,181–188. doi: 10.1038/clpt.2011.253
Cowley, M.A., Smith, R.G., Diano, S., Tsch€op, M., Pronchuk, N.,Grove, K.L., … Horvath, T.L. (2003). The distribution and mechan-ism of action of ghrelin in the CNS demonstrates a novel hypothal-amic circuit regulating energy homeostasis. Neuron, 37, 649–661.Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/12597862
Cui, H., Moore, J., Ashimi, S.S., Mason, B.L., Drawbridge, J.N., Han, S.,… Lutter, M. (2013). Eating disorder predisposition is associatedwith ESRRA and HDAC4 mutations. The Journal of ClinicalInvestigation, 123, 4706–4713. doi: 10.1172/JCI71400
Cuntz, U., Enck, P., Fr€uhauf, E., Lehnert, P., Riepl, R.L., Fichter, M.M.,& Otto, B. (2013). Cholecystokinin revisited: CCK and the hungertrap in anorexia nervosa. PloS One, 8, e54457. doi: 10.1371/journal.pone.0054457
Dailey, M.J., & Bartness, T.J. (2009). Appetitive and consummatoryingestive behaviors stimulated by PVH and perifornical area NPYinjections. American Journal of Physiology, Regulatory, Integrativeand Comparative Physiology, 296, R877–R892. doi: 10.1152/ajpregu.90568.2008
Davis, R., & Faulds, D. (1996). Dexfenfluramine. An updated review ofits therapeutic use in the management of obesity. Drugs, 52,696–724. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/911881910.2165/00003495-199652050-00007
DeGuzman, M., Shott, M.E., Yang, T.T., Riederer, J., & Frank, G.K.W.(2017). Association of elevated reward prediction error responsewith weight gain in adolescent anorexia nervosa. American Journalof Psychiatry, 174, 557–565. doi: 10.1176/appi.ajp.2016.16060671
Deshpande, S.A., Carvalho, G.B., Amador, A., Phillips, A.M., Hoxha, S.,Lizotte, K.J., & Ja, W.W. (2014). Quantifying Drosophila food intake:comparative analysis of current methodology. Nature Methods, 11,535–540. doi: 10.1038/nmeth.2899
Di Marzo, V., Goparaju, S.K., Wang, L., Liu, J., B�atkai, S., J�arai, Z., …Kunos, G. (2001). Leptin-regulated endocannabinoids are involved inmaintaining food intake. Nature, 410, 822–825. doi: 10.1038/35071088
Dinan, T.G., & Cryan, J.F. (2017). The microbiome–gut–brain axis inhealth and disease. Gastroenterology Clinics of North America, 46,77–89. doi: 10.1016/j.gtc.2016.09.007
DiPatrizio, N.V., & Piomelli, D. (2012). The thrifty lipids:Endocannabinoids and the neural control of energy conservation.Trends in Neurosciences, 35, 403–411. doi: 10.1016/j.tins.2012.04.006
Dixon, D.P., Ackert, A.M., & Eckel, L.A. (2003). Development of, andrecovery from, activity-based anorexia in female rats. Physiology &Behavior, 80, 273–279. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/1463722610.1016/j.physbeh.2003.08.008
Dost�alov�a, I., Kopsk�y, V., Duskov�a, J., Papezov�a, H., Pac�ak, K., &Nedv�ıdkov�a, J. (2005). Leptin concentrations in the abdominal sub-cutaneous adipose tissue of patients with anorexia nervosa assessedby in vivo microdialysis. Regulatory Peptides, 128, 63–68. doi:10.1016/j.regpep.2004.12.029
Dus, M., Lai, J.S.-Y., Gunapala, K.M., Min, S., Tayler, T.D., Hergarden,A.C., … Suh, G.S.B. (2015). Nutrient sensor in the brain directs theaction of the brain–gut axis in Drosophila. Neuron, 87, 139–151. doi:10.1016/j.neuron.2015.05.032
JOURNAL OF NEUROGENETICS 15
Dow
nloa
ded
by [
Uni
vers
ity o
f L
a L
agun
a V
icer
rect
orad
o] a
t 07:
00 0
1 A
ugus
t 201
7

Eddy, K.T., Lawson, E.A., Meade, C., Meenaghan, E., Horton, S.E.,Misra, M., … Miller, K.K. (2015). Appetite regulatory hormones inwomen with anorexia nervosa: Binge-eating/purging versus restrict-ing type. Journal of Clinical Psychiatry, 76, 19–24. doi: 10.4088/JCP.13m08753
Egger, G., Liang, G., Aparicio, A., & Jones, P.A. (2004). Epigenetics inhuman disease and prospects for epigenetic therapy. Nature, 429,457–463. doi: 10.1038/nature02625
Ehrlich, S., Weiss, D., Burghardt, R., Infante-Duarte, C., Brockhaus, S.,Muschler, M.A., … Frieling, H. (2010). Promoter specific DNAmethylation and gene expression of POMC in acutely underweightand recovered patients with anorexia nervosa. Journal of PsychiatricResearch, 44, 827–833. doi: 10.1016/j.jpsychires.2010.01.011
El-Giamal, N., de Zwaan, M., Bailer, U., Strnad, A., Sch€ussler, P., &Kasper, S. (2003). Milnacipran in the treatment of bulimia nervosa: areport of 16 cases. European Neuropsychopharmacology, 13, 73–79.doi: 10.1016/S0924-977X(02)00126-8
Elias, C.F., Lee, C., Kelly, J., Aschkenasi, C., Ahima, R.S., Couceyro,P.R., … Elmquist, J.K. (1998). Leptin activates hypothalamic CARTneurons projecting to the spinal cord. Neuron, 21, 1375–1385.Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/9883730
Farci, A.M.G., Piras, S., Murgia, M., Chessa, A., Restivo, A., Gessa, G.L., &Agabio, R. (2015). Disulfiram for binge eating disorder: An open trail.Eating Behaviors, 16, 84–87. doi: 10.1016/j.eatbeh.2014.10.008
Fekete, C., Zs�eli, G., Singru, P.S., K�ad�ar, A., Wittmann, G., F€uzesi, T.,… Lechan, R.M. (2012). Activation of anorexigenic pro-opiomela-nocortin neurones during refeeding is independent of vagal andbrainstem inputs. Journal of Neuroendocrinology, 24, 1423–1431. doi:10.1111/j.1365-2826.2012.02354.x
Fern�andez-Aranda, F., Amor, A., Jim�enez-Murcia, S., Gim�enez-Mart�ınez, L., Tur�on-Gil, V., & Vallejo-Ruiloba, J. (2001). Bulimianervosa and misuse of orlistat: Two case reports. InternationalJournal of Eating Disorders, 30, 458–461. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/11746308
Fetissov, S.O., Harro, J., Jaanisk, M., J€arv, A., Podar, I., Allik, J., …H€okfelt, T. (2005). Autoantibodies against neuropeptides are associ-ated with psychological traits in eating disorders. Proceedings of theNational Academy of Sciences of the United States of America, 102,14865–14870. doi: 10.1073/pnas.0507204102
Flak, J.N., & Myers, M.G. (2016). Minireview: CNS mechanisms of lep-tin action. Molecular Endocrinology (Baltimore, Md.), 30, 3–12. doi:10.1210/me.2015-1232
Flament, M.F., Bissada, H., & Spettigue, W. (2012). Evidence-based pharma-cotherapy of eating disorders. International Journal ofNeuropsychopharmacology, 15, 189–207. doi: 10.1017/S1461145711000381
F€ocker, M., Timmesfeld, N., Scherag, S., B€uhren, K., Langkamp, M.,Dempfle, A., … Hebebrand, J. (2011). Screening for anorexia nerv-osa via measurement of serum leptin levels. Journal of NeuralTransmission (Vienna, Austria: 1996), 118, 571–578. doi: 10.1007/s00702-010-0551-z
Frank, G.K., Bailer, U.F., Henry, S.E., Drevets, W., Meltzer, C.C., Price,J.C., … Kaye, W.H. (2005). Increased dopamine D2/D3 receptorbinding after recovery from anorexia nervosa measured by positronemission tomography and [11c]raclopride. Biological Psychiatry, 58,908–912. doi: 10.1016/j.biopsych.2005.05.003
Frieling, H., R€omer, K.D., Scholz, S., Mittelbach, F., Wilhelm, J., DeZwaan, M., … Bleich, S. (2010). Epigenetic dysregulation of dopa-minergic genes in eating disorders. International Journal of EatingDisorders, 43, 577–583. doi: 10.1002/eat.20745
Frith, C.D. (2008). Social cognition. Philosophical Transactions of theRoyal Society of London Series B, Biological Sciences, 363, 2033–2039.doi: 10.1098/rstb.2008.0005
Fuss, J., Steinle, J., Bindila, L., Auer, M.K., Kirchherr, H., Lutz, B., &Gass, P. (2015). A runner’s high depends on cannabinoid receptorsin mice. Proceedings of the National Academy of Sciences of theUnited States of America, 112, 13105–13108. doi: 10.1073/pnas.1514996112
Gaetani, S., Kaye, W.H., Cuomo, V., & Piomelli, D. (2008). Role ofendocannabinoids and their analogues in obesity and eating
disorders. Eating and Weight Disorders, 13, e42–e48. Retrieved fromhttp://www.ncbi.nlm.nih.gov/pubmed/19011363
Gaetani, S., Romano, A., Provensi, G., Ricca, V., Lutz, T., & Passani,M.B. (2016). Eating disorders: From bench to bedside and back.Journal of Neurochemistry, 139, 691–699. doi: 10.1111/jnc.13848
Galusca, B., Pr�evost, G., Germain, N., Dubuc, I., Ling, Y., Anouar, Y.,… Chartrel, N. (2015). Neuropeptide Y and a-MSH circadian levelsin two populations with low body weight: Anorexia nervosa andconstitutional thinness. PLoS One, 10, e0122040. doi: 10.1371/journal.pone.0122040
Gao, Q., & Horvath, T.L. (2008). Neuronal control of energy homeosta-sis. FEBS Letters, 582, 132–141. doi: 10.1016/j.febslet.2007.11.063
Garlapow, M.E., Huang, W., Yarboro, M.T., Peterson, K.R., & Mackay,T.F.C. (2015). Quantitative genetics of food intake in Drosophila mela-nogaster. PLoS One, 10, e0138129. doi: 10.1371/journal.pone.0138129
Garnock-Jones, K.P., & Keating, G.M. (2009). Atomoxetine: A reviewof its use in attention-deficit hyperactivity disorder in children andadolescents. Paediatric Drugs, 11, 203–226. doi: 10.2165/00148581-200911030-00005
Gauthier, C., Hassler, C., Mattar, L., Launay, J.-M., Callebert, J.,Steiger, H., … Godart, N. (2014). Symptoms of depression and anx-iety in anorexia nervosa: Links with plasma tryptophan and sero-tonin metabolism. Psychoneuroendocrinology, 39, 170–178. doi:10.1016/j.psyneuen.2013.09.009
Gorwood, P., Blanchet-Collet, C., Chartrel, N., Duclos, J., Dechelotte, P.,Hanachi, M., … Epelbaum, J. (2016). New insights in anorexia nerv-osa. Frontiers in Neuroscience, 10, 256. doi: 10.3389/fnins.2016.00256
Gorwood, P., Kipman, A., & Foulon, C. (2003). The human genetics ofanorexia nervosa. European Journal of Pharmacology, 480, 163–170.Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/1462335910.1016/j.ejphar.2003.08.103
Grilo, C.M., Crosby, R.D., Wilson, G.T., & Masheb, R.M. (2012). 12-month follow-up of fluoxetine and cognitive behavioral therapy forbinge eating disorder. Journal of Consulting and Clinical Psychology,80, 1108–1113. doi: 10.1037/a0030061
Grilo, C.M., Masheb, R.M., & Salant, S.L. (2005). Cognitive behavioraltherapy guided self-help and orlistat for the treatment of binge eatingdisorder: A randomized, double-blind, placebo-controlled trial.Biological Psychiatry, 57, 1193–1201. doi: 10.1016/j.biopsych.2005.03.001
Groleau, P., Joober, R., Israel, M., Zeramdini, N., DeGuzman, R., &Steiger, H. (2014). Methylation of the dopamine D2 receptor(DRD2) gene promoter in women with a bulimia-spectrum disorder:associations with borderline personality disorder and exposure tochildhood abuse. Journal of Psychiatric Research, 48, 121–127. doi:10.1016/j.jpsychires.2013.10.003
Guerdjikova, A.I., McElroy, S.L., Winstanley, E.L., Nelson, E.B., Mori, N.,McCoy, J., … Hudson, J.I. (2012). Duloxetine in the treatment ofbinge eating disorder with depressive disorders: A placebo-controlledtrial. International Journal of Eating Disorders, 45, 281–289. doi:10.1002/eat.20946
Guerdjikova, A.I., Mori, N., Casuto, L.S., & McElroy, S.L. (2016). Novelpharmacologic treatment in acute binge eating disorder – role of lis-dexamfetamine. Neuropsychiatric Disease and Treatment, 12,833–841. doi: 10.2147/NDT.S80881
Haghighi, M., Jahangard, L., Mohammad-Beigi, H., Bajoghli, H.,Hafezian, H., Rahimi, A., … Brand, S. (2013). In a double-blind,randomized and placebo-controlled trial, adjuvant memantineimproved symptoms in inpatients suffering from refractoryobsessive–compulsive disorders (OCD). Psychopharmacology, 228,633–640. doi: 10.1007/s00213-013-3067-z
Hagler Robinson, A. (2009). Orlistat misuse as purging in a patientwith binge-eating disorder. Psychosomatics, 50, 177–178. doi:10.1176/appi.psy.50.2.177
Hald, J., & Jacobsen, E. (1948). A drug sensitizing the organism toethyl alcohol. Lancet (London, England), 2, 1001–1004. Retrievedfrom http://www.ncbi.nlm.nih.gov/pubmed/1810347510.1016/S0140-6736(48)91514-1
Haleem, D. (2012). Serotonin neurotransmission in anorexia nervosa.Behavioural Pharmacology, 23, 478–495. doi: 10.1097/FBP.0b013e328357440d
16 GERM�AN CUESTO ET AL.
Dow
nloa
ded
by [
Uni
vers
ity o
f L
a L
agun
a V
icer
rect
orad
o] a
t 07:
00 0
1 A
ugus
t 201
7

Haleem, D., & Haider, S. (1996). Food restriction decreases serotoninand its synthesis rate in the hypothalamus. Neuroreport, 7,1153–1156. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/881752210.1097/00001756-199604260-00011
Halmi, K.A. (2005). The multimodal treatment of eating disorders.World Psychiatry, 4, 69–73. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/16633511
Halmi, K.A. (2013). Perplexities of treatment resistence in eating disor-ders. BMC Psychiatry, 13, 292. doi: 10.1186/1471-244X-13-292
Halmi, K.A., Eckert, E., LaDu, T.J., & Cohen, J. (1986). Anorexia nerv-osa. Treatment Efficacy of Cyproheptadine and Amitriptyline,Archives of General Psychiatry, 43, 177–181. Retrieved fromhttp://www.ncbi.nlm.nih.gov/pubmed/351187710.1001/archpsyc.1986.01800020087011
Hatsukami, D., Eckert, E., Mitchell, J.E., & Pyle, R. (1984). Affectivedisorder and substance abuse in women with bulimia. PsychologicalMedicine, 14, 701–704. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/659375810.1017/S0033291700015324
Hay, P.J., & Claudino, A.M. (2012). Clinical psychopharmacology of eatingdisorders: A research update. The International Journal ofNeuropsychopharmacology, 15 (2), 209–22. doi: 10.1017/S1461145711000460
Hebebrand, J., Blum, W.F., Barth, N., Coners, H., Englaro, P., Juul, A.,… Remschmidt, H. (1997). Leptin levels in patients with anorexianervosa are reduced in the acute stage and elevated upon short-termweight restoration. Molecular Psychiatry, 2, 330–334. Retrieved fromhttp://www.ncbi.nlm.nih.gov/pubmed/9246674
Hebebrand, J., Exner, C., Hebebrand, K., Holtkamp, C., Casper, R.C.,Remschmidt, H., … Klingenspor, M. (2003). Hyperactivity inpatients with anorexia nervosa and in semistarved rats: Evidence fora pivotal role of hypoleptinemia. Physiology & Behavior, 79, 25–37.Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/12818707
Helder, S.G., & Collier, D.A. (2011). The genetics of eating disorders.Current Topics in Behavioral Neurosciences, 6, 157–175. doi: 10.1007/7854_2010_79
Herisson, F.M., Brooks, L.L., Waas, J.R., Levine, A.S., & Olszewski, P.K.(2014). Functional relationship between oxytocin and appetite forcarbohydrates versus saccharin. Neuroreport, 25, 909–914. doi:10.1097/WNR.0000000000000201
Hermanussen, M., & Tresguerres, J.A.F. (2005). A new anti-obesitydrug treatment: First clinical evidence that, antagonising glutamate-gated Ca2þ ion channels with memantine normalises binge-eatingdisorders. Economics and Human Biology, 3, 329–337. doi: 10.1016/j.ehb.2005.04.001
Hettes, S.R., Gonzaga, J., Heyming, T.W., Perez, S., Wolfsohn, S., &Stanley, B.G. (2003). Dual roles in feeding for AMPA/kainate recep-tors: Receptor activation or inactivation within distinct hypothalamicregions elicits feeding behavior. Brain Research, 992, 167–178.Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/1462505610.1016/j.brainres.2003.08.032
Hinney, A., Kesselmeier, M., Jall, S., Volckmar, A.-L., F€ocker, M.,Antel, J. … Hebebrand, (2017). Evidence for three genetic lociinvolved in both anorexia nervosa risk and variation of body massindex. Molecular Psychiatry, 22, 192–201. doi: 10.1038/mp.2016.71
Hnasko, T.S., Perez, F.A., Scouras, A.D., Stoll, E.A., Gale, S.D., Luquet,S., … Palmiter, R.D. (2006). Cre recombinase-mediated restorationof nigrostriatal dopamine in dopamine-deficient mice reverses hypo-phagia and bradykinesia. Proceedings of the National Academy ofSciences of the United States of America, 103, 8858–8863. doi:10.1073/pnas.0603081103
Holder, J.L., & Wilfong, A.A. (2011). Zonisamide in the treatment ofepilepsy. Expert Opinion on Pharmacotherapy, 12, 2573–2581. doi:10.1517/14656566.2011.622268
Hosenbocus, S., & Chahal, R. (2013). Memantine: A review of possibleuses in child and adolescent psychiatry. Journal of the CanadianAcademy of Child and Adolescent Psychiatry, 22, 166–171. Retrievedfrom http://www.ncbi.nlm.nih.gov/pubmed/23667364
Hotta, M., Ohwada, R., Akamizu, T., Shibasaki, T., Takano, K., &Kangawa, K. (2009). Ghrelin increases hunger and food intake inpatients with restricting-type anorexia nervosa: A pilot study.
Endocrine Journal, 56, 1119–1128. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/1975575310.1507/endocrj.K09E-168
Hudson, J.I., Lalonde, J.K., Berry, J.M., Pindyck, L.J., Bulik, C.M.,Crow, S.J., … Pope, H.G. (2006). Binge-eating disorder as a distinctfamilial phenotype in obese individuals. Archives of GeneralPsychiatry, 63, 313–319. doi: 10.1001/archpsyc.63.3.313
Jean, A., Conductier, G., Manrique, C., Bouras, C., Berta, P., Hen, R.,… Compan, V. (2007). Anorexia induced by activation of serotonin5-HT4 receptors is mediated by increases in CART in the nucleusaccumbens. Proceedings of the National Academy of Sciences of theUnited States of America, 104, 16335–16340. doi: 10.1073/pnas.0701471104
Jennings, K.M., Wildes, J.E., & Coccaro, E.F. (2017). Intermittent explo-sive disorder and eating disorders: Analysis of national comorbidityand research samples. Comprehensive Psychiatry, 75, 62–67. doi:10.1016/j.comppsych.2017.02.011
Jirtle, R.L., & Skinner, M.K. (2007). Environmental epigenomics anddisease susceptibility. Nature Reviews. Genetics, 8, 253–262. doi:10.1038/nrg2045
Kageyama, H., Takenoya, F., Shiba, K., & Shioda, S. (2010). Neuronal cir-cuits involving ghrelin in the hypothalamus-mediated regulation offeeding. Neuropeptides, 44, 133–138. doi: 10.1016/j.npep.2009.11.010
Kalyanasundar, B., Perez, C.I., Luna, A., Solorio, J., Moreno, M.G.,Elias, D., … Gutierrez, R. (2015). D1 and D2 antagonists reversethe effects of appetite suppressants on weight loss, food intake, loco-motion, and rebalance spiking inhibition in the rat NAc shell.Journal of Neurophysiology, 114, 585–607. doi: 10.1152/jn.00012.2015
Kannan, K., & Fridell, Y.-W.C. (2013). Functional implications ofDrosophila insulin-like peptides in metabolism, aging, and dietary restric-tion. Frontiers in Physiology, 4, 288. doi: 10.3389/fphys.2013.00288
Karra, E., Chandarana, K., & Batterham, R.L. (2009). The role of pep-tide YY in appetite regulation and obesity. Journal of Physiology,587, 19–25. doi: 10.1113/jphysiol.2008.164269
Kawahara, Y., Kawahara, H., Kaneko, F., Yamada, M., Nishi, Y.,Tanaka, E., & Nishi, A. (2009). Peripherally administered ghrelininduces bimodal effects on the mesolimbic dopamine systemdepending on food-consumptive states. Neuroscience, 161, 855–864.doi: 10.1016/j.neuroscience.2009.03.086
Kawai, K., Nakashima, M., Kojima, M., Yamashita, S., Takakura, S.,Shimizu, M., … Sudo, N. (2017). Ghrelin activation and neuropep-tide Y elevation in response to medium chain triglyceride adminis-tration in anorexia nervosa patients. Clinical Nutrition ESPEN, 17,100–104. doi: 10.1016/j.clnesp.2016.10.001
Kaye, W. (1997). Anorexia nervosa, obsessional behavior, and sero-tonin. Psychopharmacology Bulletin, 33, 335–344. Retrieved fromhttp://www.ncbi.nlm.nih.gov/pubmed/9550876
Kaye, W.H., Bailer, U.F., Frank, G.K., Wagner, A., & Henry, S.E.(2005). Brain imaging of serotonin after recovery from anorexia andbulimia nervosa. Physiology & Behavior, 86, 15–17. doi: 10.1016/j.physbeh.2005.06.019
Kaye, W.H., Fudge, J.L., & Paulus, M. (2009). New insights into symp-toms and neurocircuit function of anorexia nervosa. Nature Reviews,Neuroscience, 10, 573–584. doi: 10.1038/nrn2682
Keller, P.A., Compan, V., Bockaert, J., Giacobino, J.-P., Charnay, Y.,Bouras, C., & Assimacopoulos-Jeannet, F. (2006). Characterizationand localization of cocaine- and amphetamine-regulated transcript(CART) binding sites. Peptides, 27, 1328–1334. doi: 10.1016/j.peptides.2005.10.016
Kern, A., Albarran-Zeckler, R., Walsh, H.E., & Smith, R.G. (2012).Apo-ghrelin receptor forms heteromers with DRD2 in hypothalamicneurons and is essential for anorexigenic effects of DRD2 agonism.Neuron, 73, 317–332. doi:10.1016/j.neuron.2011.10.038
Keski-Rahkonen, A., & Mustelin, L. (2016). Epidemiology of eating dis-orders in Europe: Prevalence, incidence, comorbidity, course, conse-quences, and risk factors. Current Opinion in Psychiatry, 29,340–345. doi: 10.1097/YCO.0000000000000278
Kim, C., Kim, S., & Park, S. (2017). Neurogenic effects of ghrelin onthe hippocampus. International Journal of Molecular Sciences, 18,588. doi: 10.3390/ijms18030588
JOURNAL OF NEUROGENETICS 17
Dow
nloa
ded
by [
Uni
vers
ity o
f L
a L
agun
a V
icer
rect
orad
o] a
t 07:
00 0
1 A
ugus
t 201
7

Kim, G., Deepinder, F., Morales, W., Hwang, L., Weitsman, S., Chang, C.,… Pimentel, M. (2012). Methanobrevibacter smithii is the predomin-ant methanogen in patients with constipation-predominant IBS andmethane on breath. Digestive Diseases and Sciences, 57, 3213–3218. doi:10.1007/s10620-012-2197-1
Kim, Y.-R., Eom, J.-S., Yang, J.-W., Kang, J., & Treasure, J. (2015). Theimpact of oxytocin on food intake and emotion recognition inpatients with eating disorders: A double blind single dose within-subject cross-over design. PLoS One, 10, e0137514. doi: 10.1371/journal.pone.0137514
Kim, Y.-R., Kim, J.-H., Kim, C.-H., Shin, J.G., & Treasure, J. (2015).Association between the oxytocin receptor gene polymorphism(rs53576) and bulimia nervosa. European Eating Disorders Review,23, 171–178. doi: 10.1002/erv.2354
Kirkpatrick, S.L., Goldberg, L.R., Yazdani, N., Babbs, R.K., Wu, J.,Reed, E.R., … Bryant, C.D. (2017). Cytoplasmic FMR1-interactingprotein 2 is a major genetic factor underlying binge eating. BiologicalPsychiatry, 81, 757–769. doi: 10.1016/j.biopsych.2016.10.021
Kirsz, K., & Zieba, D.A. (2011). Ghrelin-mediated appetite regulation inthe central nervous system. Peptides, 32, 2256–2264. doi: 10.1016/j.peptides.2011.04.010
Klenerova, V., Sery, O., & Hynie, S. (2008). Corticotropin-releasing hor-mone receptor subtypes in the rat anterior pituitary after two typesof restraint stress. Annals of the New York Academy of Sciences,1148, 415–420. doi: 10.1196/annals.1410.043
Kojima, M., Hosoda, H., & Kangawa, K. (2001). Purification and distri-bution of ghrelin: The natural endogenous ligand for the growthhormone secretagogue receptor. Hormone Research, 56 Suppl 1,93–97. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/11786694.
Kokare, D.M., Dandekar, M.P., Singru, P.S., Gupta, G.L., & Subhedar,N.K. (2010). Involvement of alpha-MSH in the social isolation inducedanxiety- and depression-like behaviors in rat. Neuropharmacology, 58,1009–1018. doi: 10.1016/j.neuropharm.2010.01.006
Koob, G.F., & Volkow, N.D. (2010). Neurocircuitry of addiction.Neuropsychopharmacology, 35, 217–238. doi: 10.1038/npp.2009.110
Koren, R., Duncan, A.E., Munn-Chernoff, M.A., Bucholz, K.K.,Lynskey, M.T., Heath, A.C., & Agrawal, A. (2014). Preliminary evi-dence for the role of HTR2A variants in binge eating in youngwomen. Psychiatric Genetics, 24, 28–33. doi: 10.1097/YPG.0000000000000014
Kornstein, S.G., Kunovac, J.L., Herman, B.K., & Culpepper, L. (2016).Recognizing binge-eating disorder in the clinical setting: A review ofthe literature. Primary Care Companion for CNS Disorders, 18. doi:10.4088/PCC.15r01905
Koyama, T., Nakajima, Y., Fujii, T., & Kawashima, K. (1999).Enhancement of cortical and hippocampal cholinergic neurotrans-mission through 5-HT1A receptor-mediated pathways by BAY x3702 in freely moving rats. Neuroscience Letters, 265, 33–36.Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/1032719910.1016/S0304-3940(99)00200-1
Krajmalnik-Brown, R., Ilhan, Z.-E., Kang, D.-W., & DiBaise, J.K.(2012). Effects of gut microbes on nutrient absorption and energyregulation. Nutrition in Clinical Practice, 27, 201–214. doi: 10.1177/0884533611436116
Krashes, M.J., DasGupta, S., Vreede, A., White, B., Armstrong, J.D., &Waddell, S. (2009). A neural circuit mechanism integrating motiv-ational state with memory expression in Drosophila. Cell, 139,416–427. doi: 10.1016/j.cell.2009.08.035
Kutlu, S., Aydin, M., Alcin, E., Ozcan, M., Bakos, J., Jezova, D., &Yilmaz, B. (2010). Leptin modulates noradrenaline release in theparaventricular nucleus and plasma oxytocin levels in female rats: Amicrodialysis study. Brain Research, 1317, 87–91. doi: 10.1016/j.brainres.2009.12.044
Lambe, E.K., Fillman, S.G., Webster, M.J., & Shannon Weickert, C.(2011). Serotonin receptor expression in human prefrontal cortex:Balancing excitation and inhibition across postnatal development.PLoS One, 6, e22799. doi: 10.1371/journal.pone.0022799
Laque, A., Yu, S., Qualls-Creekmore, E., Gettys, S., Schwartzenburg, C.,Bui, K., … M€unzberg, H. (2015). Leptin modulates nutrient reward
via inhibitory galanin action on orexin neurons. MolecularMetabolism, 4, 706–717. doi: 10.1016/j.molmet.2015.07.002
Legrand, R., Lucas, N., Breton, J., Azhar, S., do Rego, J.-C., D�echelotte, P.,… Fetissov, S.O. (2016). Ghrelin treatment prevents development ofactivity based anorexia in mice. European Neuropsychopharmacology,26, 948–958. doi: 10.1016/j.euroneuro.2016.03.010
Leinninger, G.M., Jo, Y.-H., Leshan, R.L., Louis, G.W., Yang, H.,Barrera, J.G., … Myers, M.G. (2009). Leptin acts via leptin receptor-expressing lateral hypothalamic neurons to modulate the mesolimbicdopamine system and suppress feeding. Cell Metabolism, 10, 89–98.doi: 10.1016/j.cmet.2009.06.011
Leitenberg, H., Rosen, J.C., Wolf, J., Vara, L.S., Detzer, M.J., & Srebnik, D.(1994). Comparison of cognitive–behavior therapy and desipraminein the treatment of bulimia nervosa. Behaviour Research and Therapy,32, 37–45. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/813572110.1016/0005-7967(94)90082-5
Lenard, N.R., & Berthoud, H.-R. (2008). Central and peripheral regula-tion of food intake and physical activity: Pathways and genes.Obesity (Silver Spring, Md.), 16 Suppl 3, S11–S22. doi: 10.1038/oby.2008.511
Lenka, A., Arumugham, S.S., Christopher, R., & Pal, P.K. (2016).Genetic substrates of psychosis in patients with Parkinson’s disease:A critical review. Journal of the Neurological Sciences, 364, 33–41.doi: 10.1016/j.jns.2016.03.005
Lilenfeld, L.R.R., Ringham, R., Kalarchian, M.A., & Marcus, M.D.(2008). A family history study of binge-eating disorder.Comprehensive Psychiatry, 49, 247–254. doi: 10.1016/j.comppsych.2007.10.001
Liu, C., Placais, P.-Y., Yamagata, N., Pfeiffer, B.D., Aso, Y., Friedrich,A.B., … Tanimoto, H. (2012). A subset of dopamine neurons sig-nals reward for odour memory in Drosophila. Nature, 488, 512–516.doi: 10.1038/nature11304
Liu, J., Garza, J.C., Truong, H.V., Henschel, J., Zhang, W., & Lu, X.-Y.(2007). The melanocortinergic pathway is rapidly recruited by emo-tional stress and contributes to stress-induced anorexia and anxiety-like behavior. Endocrinology, 148, 5531–5540. doi: 10.1210/en.2007-0745
Locke, A.E., Kahali, B., Berndt, S.I., Justice, A.E., Pers, T.H., Day, F.R.,… Speliotes, E.K. (2015). Genetic studies of body mass index yieldnew insights for obesity biology. Nature, 518, 197–206. doi: 10.1038/nature14177
Louis, G.W., Leinninger, G.M., Rhodes, C.J., & Myers, M.G. (2010).Direct innervation and modulation of orexin neurons by lateralhypothalamic LepRb neurons. Journal of Neuroscience, 30,11278–11287. doi: 10.1523/JNEUROSCI.1340-10.2010
Lozano, R., Naghavi, M., Foreman, K., Lim, S., Shibuya, K., Aboyans, V.,… Memish, Z.A. (2012). Global and regional mortality from 235causes of death for 20 age groups in 1990 and 2010: A systematic ana-lysis for the Global Burden of Disease Study 2010. Lancet (London,England), 380, 2095–2128. doi: 10.1016/S0140-6736(12)61728-0
Lutz, T.A., Senn, M., Althaus, J., Del Prete, E., Ehrensperger, F., &Scharrer, E. (1998). Lesion of the area postrema/nucleus of the soli-tary tract (AP/NTS) attenuates the anorectic effects of amylin andcalcitonin gene-related peptide (CGRP) in rats. Peptides, 19,309–317. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/949386310.1016/S0196-9781(97)00292-1
Maes, M., Monteleone, P., Bencivenga, R., Goossens, F., Maj, M.,van West, D., … Scharpe, S. (2001). Lower serum activity of prolylendopeptidase in anorexia and bulimia nervosa.Psychoneuroendocrinology, 26, 17–26. Retrieved from doi: http://www.ncbi.nlm.nih.gov/pubmed/11070331
Mahler, S.V., Smith, K.S., & Berridge, K.C. (2007). Endocannabinoidhedonic hotspot for sensory pleasure: Anandamide in nucleusaccumbens shell enhances “liking” of a sweet reward.Neuropsychopharmacology, 32, 2267–2278. doi: 10.1038/sj.npp.1301376
Martiadis, V., Castaldo, E., Monteleone, P., & Maj, M. (2007). The roleof psychopharmacology in the treatment of eating disorders. ClinicalNeuropsychiatry, 4, 51–60.
18 GERM�AN CUESTO ET AL.
Dow
nloa
ded
by [
Uni
vers
ity o
f L
a L
agun
a V
icer
rect
orad
o] a
t 07:
00 0
1 A
ugus
t 201
7

Martinussen, M., Friborg, O., Schmierer, P., Kaiser, S., Øvergård, K.T.,Neunhoeffer, A.-L., … Rosenvinge, J.H. (2016). The comorbidity ofpersonality disorders in eating disorders: A meta-analysis. Eatingand Weight Disorders, 22, 201–209. doi: 10.1007/s40519-016-0345-x
McElroy, S., Guerdjikova, A.I., Mori, N., & O’melia, A. (2012).Pharmacological management of binge eating disorder: Currentand emerging treatment options. Therapeutics and ClinicalRisk Management, 8, 219–241. doi: 10.2147/TCRM.S25574
McElroy, S.L., Guerdjikova, A.I., Martens, B., Keck, P.E., Pope, H.G., &Hudson, J.I. (2009). Role of antiepileptic drugs in themanagement of eating disorders. CNS Drugs, 23, 139–156. Retrievedfrom http://www.ncbi.nlm.nih.gov/pubmed/1917337310.2165/00023210-200923020-00004
McElroy, S.L., Guerdjikova, A., Kotwal, R., Welge, J.A., Nelson, E.B.,Lake, K.A., … Hudson, J.I. (2007). Atomoxetine in the treatment ofbinge-eating disorder: A randomized placebo-controlled trial. Journalof Clinical Psychiatry, 68 (3), 390–8. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/17388708
McElroy, S.L., Hudson, J.I., Malhotra, S., Welge, J.A., Nelson, E.B., &Keck, P.E. (2003). Citalopram in the treatment of binge-eating dis-order: A placebo-controlled trial. Journal of Clinical Psychiatry, 64,807–813. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/1293498210.4088/JCP.v64n0711
McGuirk, J., Goodall, E., Silverstone, T., & Willner, P. (1991).Differential effects of d-fenfluramine, l-fenfluramine and d-amphet-amine on the microstructure of human eating behaviour.Behavioural Pharmacology, 2, 113–119. Retrieved fromhttp://www.ncbi.nlm.nih.gov/pubmed/1122405510.1097/00008877-199104000-00004
McKnight, R.F., & Park, R.J. (2010). Atypical antipsychotics and ano-rexia nervosa: A review. European Eating Disorders Review, 18,10–21. doi: 10.1002/erv.988
Meister, B. (2007). Neurotransmitters in key neurons of the hypothalamusthat regulate feeding behavior and body weight. Physiology & Behavior,92, 263–271.doi: 10.1016/j.physbeh.2007.05.021
Melcher, C., & Pankratz, M.J. (2005). Candidate gustatory interneuronsmodulating feeding behavior in the Drosophila brain. PLoS Biology,3, e305. doi: 10.1371/journal.pbio.0030305
Micioni Di Bonaventura, M.V., Ciccocioppo, R., Romano, A., Bossert,J.M., Rice, K.C., Ubaldi, M., … Cifani, C. (2014). Role of bednucleus of the stria terminalis corticotrophin-releasing factor recep-tors in frustration stress-induced binge-like palatable food consump-tion in female rats with a history of food restriction. Journal ofNeuroscience, 34, 11316–11324. doi: 10.1523/JNEUROSCI.1854-14.2014
Milano, W., Petrella, C., Casella, A., Capasso, A., Carrino, S., & Milano,L. (2005). Use of sibutramine, an inhibitor of the reuptake of sero-tonin and noradrenaline, in the treatment of binge eating disorder:A placebo-controlled study. Advances in Therapy, 22, 25–31.Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/1594321910.1007/BF02850181
Milano, W., Petrella, C., Sabatino, C., & Capasso, A. (2004). Treatmentof bulimia nervosa with sertraline: A randomized controlled trial.Advances in Therapy, 21, 232–237. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/1560561710.1007/BF02850155
Miljic, D., Pekic, S., Djurovic, M., Doknic, M., Milic, N., Casanueva,F.F., … Popovic, V. (2006). Ghrelin has partial or no effect onappetite, growth hormone, prolactin, and cortisol release in patientswith anorexia nervosa. Journal of Clinical Endocrinology andMetabolism, 91, 1491–1495. doi: 10.1210/jc.2005-2304
Miller, R. (2009). Mechanisms of action of antipsychotic drugs of differ-ent classes, refractoriness to therapeutic effects of classical neurolep-tics, and individual variation in sensitivity to their actions: PART II.Current Neuropharmacology, 7, 315–330. doi: 10.2174/157015909790031184
Millington, G.W. (2007). The role of proopiomelanocortin (POMC)neurones in feeding behaviour. Nutrition & Metabolism, 4, 18. doi:10.1186/1743-7075-4-18
Mineur, Y.S., Einstein, E.B., Bentham, M.P., Wigestrand, M.B.,Blakeman, S., Newbold, S.A., & Picciotto, M.R. (2015). Expression of
the 5-HT1A serotonin receptor in the hippocampus is required forsocial stress resilience and the antidepressant-like effects induced bythe nicotinic partial agonist cytisine. Neuropsychopharmacology, 40,938–946. doi: 10.1038/npp.2014.269
Mischoulon, D., Eddy, K.T., Keshaviah, A., Dinescu, D., Ross, S.L.,Kass, A.E., … Herzog, D.B. (2011). Depression and eating disorders:Treatment and course. Journal of Affective Disorders, 130, 470–477.doi: 10.1016/j.jad.2010.10.043
Mithieux, G. (2013). Nutrient control of hunger by extrinsic gastro-intestinal neurons. Trends in Endocrinology and Metabolism, 24,378–384. doi: 10.1016/j.tem.2013.04.005
Monteleone, A.M., Scognamiglio, P., Volpe, U., Di Maso, V., &Monteleone, P. (2016). Investigation of oxytocin secretion in ano-rexia nervosa and bulimia nervosa: Relationships to temperamentpersonality dimensions. European Eating Disorders Review, 24,52–56. doi: 10.1002/erv.2391
Monteleone, P., Castaldo, E., & Maj, M. (2008). Neuroendocrine dysre-gulation of food intake in eating disorders. Regulatory Peptides, 149,39–50. doi: 10.1016/j.regpep.2007.10.007
Monteleone, P., Fabrazzo, M., Tortorella, A., Fuschino, A., & Maj, M.(2002). Opposite modifications in circulating leptin and soluble lep-tin receptor across the eating disorder spectrum. MolecularPsychiatry, 7, 641–646. doi: 10.1038/sj.mp.4001043
Morton, G.J., Cummings, D.E., Baskin, D.G., Barsh, G.S., & Schwartz,M.W. (2006). Central nervous system control of food intake andbody weight. Nature, 443, 289–295. doi: 10.1038/nature05026
Munn-Chernoff, M.A., & Baker, J.H. (2016). A primer on the geneticsof comorbid eating disorders and substance use disorders. EuropeanEating Disorders Review, 24, 91–100. doi: 10.1002/erv.2424
Munn-Chernoff, M.A., Grant, J.D., Bucholz, K.K., Agrawal, A.,Lynskey, M.T., Madden, P.A.F., … Duncan, A.E. (2015). Bulimicbehaviors and early substance use: Findings from a Cotwin-controlstudy. Alcoholism, Clinical and Experimental Research, 39,1740–1748. doi: 10.1111/acer.12829
Muroya, S., Funahashi, H., Yamanaka, A., Kohno, D., Uramura, K.,Nambu, T., … Yada, T. (2004). Orexins (hypocretins) directly inter-act with neuropeptide Y, POMC and glucose-responsive neurons toregulate Ca 2þ signaling in a reciprocal manner to leptin: orexigenicneuronal pathways in the mediobasal hypothalamus. EuropeanJournal of Neuroscience, 19, 1524–1534. doi: 10.1111/j.1460-9568.2004.03255.x
Murphy, K.G. (2005). Dissecting the role of cocaine- and amphetamine-regulated transcript (CART) in the control of appetite. Briefings inFunctional Genomics & Proteomics, 4, 95–111. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/1610226710.1093/bfgp/4.2.95
Murray, C.J.L., Vos, T., Lozano, R., Naghavi, M., Flaxman, A.D.,Michaud, C., … Memish, Z.A. (2012). Disability-adjusted life years(DALYs) for 291 diseases and injuries in 21 regions, 1990-2010: Asystematic analysis for the Global Burden of Disease Study 2010.Lancet (London, England), 380, 2197–2223. doi: 10.1016/S0140-6736(12)61689-4
Nagamitsu, S., Araki, Y., Ioji, T., Yamashita, F., Ozono, S., Kouno, M.,… Matsuishi, T. (2011). Prefrontal brain function in children withanorexia nervosa: A near-infrared spectroscopy study. Brain &Development, 33, 35–44. doi: 10.1016/j.braindev.2009.12.010
Nakabayashi, M., Suzuki, T., Takahashi, K., Totsune, K., Muramatsu, Y.,Kaneko, C., … Sasano, H. (2003). Orexin-A expression in humanperipheral tissues. Molecular and Cellular Endocrinology, 205, 43–50.Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/12890566
Nakai, Y., Hosoda, H., Nin, K., Ooya, C., Hayashi, H., Akamizu, T., &Kangawa, K. (2003). Plasma levels of active form of ghrelin duringoral glucose tolerance test in patients with anorexia nervosa.European Journal of Endocrinology, 149, R1–R3. Retrieved fromhttp://www.ncbi.nlm.nih.gov/pubmed/1282486910.1530/eje.0.149R001
Naleid, A.M., Grace, M.K., Chimukangara, M., Billington, C.J., &Levine, A.S. (2007). Paraventricular opioids alter intake of high-fatbut not high-sucrose diet depending on diet preference in a bingemodel of feeding. American Journal of Physiology, Regulatory,Integrative and Comparative Physiology, 293, R99–105. doi: 10.1152/ajpregu.00675.2006
JOURNAL OF NEUROGENETICS 19
Dow
nloa
ded
by [
Uni
vers
ity o
f L
a L
agun
a V
icer
rect
orad
o] a
t 07:
00 0
1 A
ugus
t 201
7

N€assel, D.R., & Winther, A.M.E. (2010). Drosophila neuropeptides inregulation of physiology and behavior. Progress in Neurobiology, 92,42–104. doi: 10.1016/j.pneurobio.2010.04.010
Nickel, C., Tritt, K., Muehlbacher, M., Pedrosa Gil, F., Mitterlehner,F.O., Kaplan, P., … Nickel, M.K. (2005). Topiramate treatment inbulimia nervosa patients: A randomized, double-blind, placebo-con-trolled trial. International Journal of Eating Disorders, 38, 295–300.doi: 10.1002/eat.20202
O’Brien, K.M., & Vincent, N.K. (2003). Psychiatric comorbidity in ano-rexia and bulimia nervosa: Nature, prevalence, and causal relation-ships. Clinical Psychology Review, 23, 57–74. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/12559994
Okita, K., Shiina, A., Nakazato, M., & Iyo, M. (2013). Tandospirone, a5-HT1A partial agonist is effective in treating anorexia nervosa:A case series. Annals of General Psychiatry, 12, 7. doi: 10.1186/1744-859X-12-7
Oldershaw, A., Hambrook, D., Stahl, D., Tchanturia, K., Treasure, J., &Schmidt, U. (2011). The socio-emotional processing stream inAnorexia Nervosa. Neuroscience and Biobehavioral Reviews, 35,970–988. doi: 10.1016/j.neubiorev.2010.11.001
Otto, B., Cuntz, U., Fruehauf, E., Wawarta, R., Folwaczny, C., Riepl,R.L., … Tsch€op, M. (2001). Weight gain decreases elevated plasmaghrelin concentrations of patients with anorexia nervosa. EuropeanJournal of Endocrinology, 145, 669–673. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/11720888
Padwal, R.S., & Majumdar, S.R. (2007). Drug treatments for obesity:Orlistat, sibutramine, and rimonabant. Lancet (London, England),369, 71–77. doi: 10.1016/S0140-6736(07)60033-6
Pandit, R., la Fleur, S.E., & Adan, R.A.H. (2013). The role of melano-cortins and Neuropeptide Y in food reward. European Journal ofPharmacology, 719, 208–214. doi: 10.1016/j.ejphar.2013.04.059
Park, J.-H., Shim, H.-M., Na, A.-Y., Bae, J.-H., Im, S.-S., & Song, D.-K.(2015). Orexin A regulates plasma insulin and leptin levels in atime-dependent manner following a glucose load in mice.Diabetologia, 58, 1542–1550. doi: 10.1007/s00125-015-3573-0
Pelchat, M.L. (2009). Food addiction in humans. Journal of Nutrition,139, 620–622. doi: 10.3945/jn.108.097816
Perello, M., & Dickson, S.L. (2015). Ghrelin signalling on food reward:A salient link between the gut and the mesolimbic system. Journal ofNeuroendocrinology, 27, 424–434. doi: 10.1111/jne.12236
Perello, M., Scott, M.M., Sakata, I., Lee, C.E., Chuang, J.-C., Osborne-Lawrence, S., … Zigman, J.M. (2012). Functional implications oflimited leptin receptor and ghrelin receptor coexpression in thebrain. Journal of Comparative Neurology, 520, 281–294. doi: 10.1002/cne.22690
Peters, S.T., Bowen, M.T., Bohrer, K., McGregor, I.S., & Neumann, I.D.(2017). Oxytocin inhibits ethanol consumption and ethanol-induceddopamine release in the nucleus accumbens. Addiction Biology, 22,702–711. doi: 10.1111/adb.12362
Pjetri, E., Schmidt, U., Kas, M.J., & Campbell, I.C. (2012). Epigeneticsand eating disorders. Current Opinion in Clinical Nutrition andMetabolic Care, 15, 330–335. doi: 10.1097/MCO.0b013e3283546fd3
Pool, A.-H., & Scott, K. (2014). Feeding regulation in Drosophila.Current Opinion in Neurobiology, 29, 57–63. doi: 10.1016/j.conb.2014.05.008
Popik, P., Kos, T., Zhang, Y., & Bisaga, A. (2011). Memantine reducesconsumption of highly palatable food in a rat model of binge eating.Amino Acids, 40, 477–485. doi: 10.1007/s00726-010-0659-3
Powers, P.S., & Bruty, H. (2009). Pharmacotherapy for eating disordersand obesity. Child and Adolescent Psychiatric Clinics of NorthAmerica, 18, 175–187. doi: 10.1016/j.chc.2008.07.009
Powers, P.S., & Santana, C. (2004). Available pharmacological treat-ments for anorexia nervosa. Expert Opinion on Pharmacotherapy, 5,2287–2292. doi: 10.1517/14656566.5.11.2287
Preti, A., Girolamo, G., de Vilagut, G., Alonso, J., Graaf, R., deBruffaerts, R. … ESEMeD-WMH Investigators. (2009). The epi-demiology of eating disorders in six European countries: Results ofthe ESEMeD-WMH project. Journal of Psychiatric Research, 43,1125–1132. doi: 10.1016/j.jpsychires.2009.04.003
Rada, P., Avena, N.M., & Hoebel, B.G. (2005). Daily bingeing on sugarrepeatedly releases dopamine in the accumbens shell. Neuroscience,134, 737–744. doi: 10.1016/j.neuroscience.2005.04.043
Rasmusson, A.M., Goldstein, L.E., Deutch, A.Y., Bunney, B.S., & Roth,R.H. (1994). 5-HT1a agonist þ/�8-OH-DPAT modulates basal andstress-induced changes in medial prefrontal cortical dopamine.Synapse (New York, N.Y.), 18, 218–224. doi: 10.1002/syn.890180307
Reas, D.L., & Grilo, C.M. (2008). Review and meta-analysis of pharma-cotherapy for binge-eating disorder. Obesity (Silver Spring, Md.), 16,2024–2038. doi: 10.1038/oby.2008.333
Ricca, V., Castellini, G., Lo Sauro, C., Rotella, C.M., & Faravelli, C.(2009). Zonisamide combined with cognitive behavioral therapy inbinge eating disorder: A one-year follow-up study. Psychiatry(Edgmont (Pa.: Township)), 6, 23–28. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/20049147
Richard, J.E., Farkas, I., Anesten, F., Anderberg, R.H., Dickson, S.L.,Gribble, F.M., … Skibicka, K.P. (2014). GLP-1 receptor stimulationof the lateral parabrachial nucleus reduces food intake:Neuroanatomical, electrophysiological, and behavioral evidence.Endocrinology, 155, 4356–4367. doi: 10.1210/en.2014-1248
Rindi, G., Necchi, V., Savio, A., Torsello, A., Zoli, M., Locatelli, V., …Solcia, E. (2002). Characterisation of gastric ghrelin cells in man andother mammals: Studies in adult and fetal tissues. Histochemistryand Cell Biology, 117, 511–519. doi: 10.1007/s00418-002-0415-1
Romano, S.J., Halmi, K.A., Sarkar, N.P., Koke, S.C., & Lee, J.S. (2002).A placebo-controlled study of fluoxetine in continued treatment ofbulimia nervosa after successful acute fluoxetine treatment. AmericanJournal of Psychiatry, 159, 96–102. doi: 10.1176/appi.ajp.159.1.96
Root, T.L., Szatkiewicz, J.P., Jonassaint, C.R., Thornton, L.M., Pinheiro,A.P., Strober, M., … Bulik, C.M. (2011). Association of candidategenes with phenotypic traits relevant to anorexia nervosa. EuropeanEating Disorders Review, 19, 487–493. doi: 10.1002/erv.1138
Ross, H.E., & Young, L.J. (2009). Oxytocin and the neural mechanismsregulating social cognition and affiliative behavior. Frontiers inNeuroendocrinology, 30, 534–547. doi: 10.1016/j.yfrne.2009.05.004
Rothman, R.B., & Baumann, M.H. (2002). Therapeutic and adverseactions of serotonin transporter substrates. Pharmacology &Therapeutics, 95, 73–88. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/1216312910.1016/S0163-7258(02)00234-6
Routtenberg, A., & Kuznesof, A.W. (1967). Self-starvation of ratsliving in activity wheels on a restricted feeding schedule. Journal ofComparative and Physiological Psychology, 64, 414–421. Retrievedfrom http://www.ncbi.nlm.nih.gov/pubmed/608287310.1037/h0025205
Ryan, K.K., Mul, J.D., Clemmensen, C., Egan, A.E., Begg, D.P.,Halcomb, K., … Ulrich-Lai, Y.M. (2014). Loss of melanocortin-4receptor function attenuates HPA responses to psychological stress.Psychoneuroendocrinology, 42, 98–105. doi: 10.1016/j.psyneuen.2014.01.010
Saffrey, R., Novakovic, B., & Wade, T.D. (2014). Assessing global andgene specific DNA methylation in anorexia nervosa: A pilot study.International Journal of Eating Disorders, 47, 206–210. doi: 10.1002/eat.22200
Sakurai, T., Amemiya, A., Ishii, M., Matsuzaki, I., Chemelli, R.M.,Tanaka, H., … Yanagisawa, M. (1998). Orexins and orexin recep-tors: a family of hypothalamic neuropeptides and G protein-coupledreceptors that regulate feeding behavior. Cell, 92, 573–585.Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/9491897
Samnaliev, M., Noh, H.L., Sonneville, K.R., & Austin, S.B. (2015). Theeconomic burden of eating disorders and related mental healthcomorbidities: An exploratory analysis using the U.S. MedicalExpenditures Panel Survey. Preventive Medicine Reports, 2, 32–34.doi: 10.1016/j.pmedr.2014.12.002
Saper, C.B., Chou, T.C., & Elmquist, J.K. (2002). The need to feed:Homeostatic and hedonic control of eating. Neuron, 36, 199–211.Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/1238377710.1016/S0896-6273(02)00969-8
Schwartz, M.W., Baskin, D.G., Bukowski, T.R., Kuijper, J.L., Foster, D.,Lasser, G., … Weigle, D.S. (1996). Specificity of leptin action on ele-vated blood glucose levels and hypothalamic neuropeptide Y gene
20 GERM�AN CUESTO ET AL.
Dow
nloa
ded
by [
Uni
vers
ity o
f L
a L
agun
a V
icer
rect
orad
o] a
t 07:
00 0
1 A
ugus
t 201
7

expression in ob/ob mice. Diabetes, 45, 531–535. Retrieved fromhttp://www.ncbi.nlm.nih.gov/pubmed/8603777
Schwartz, T.L., Siddiqui, U.A., & Raza, S. (2012). Memantine as an aug-mentation therapy for anxiety disorders. Case Reports in Psychiatry,2012, 749796. doi: 10.1155/2012/749796
Scott-Van Zeeland, A.A., Bloss, C.S., Tewhey, R., Bansal, V.,Torkamani, A., Libiger, O., … Schork, N. J. (2014). Evidence for therole of EPHX2 gene variants in anorexia nervosa. MolecularPsychiatry, 19, 724–732. doi: 10.1038/mp.2013.91
Sedlackova, D., Kopeckova, J., Papezova, H., Hainer, V., Kvasnickova, H.,Hill, M., & Nedvidkova, J. (2012). Comparison of a high-carbohydrateand high-protein breakfast effect on plasma ghrelin, obestatin, NPYand PYY levels in women with anorexia and bulimia nervosa.Nutrition & Metabolism, 9, 52. doi: 10.1186/1743-7075-9-52
Shah, M., & Vella, A. (2014). Effects of GLP-1 on appetite and weight.Reviews in Endocrine & Metabolic Disorders, 15, 181–187. doi:10.1007/s11154-014-9289-5
Shank, R.P., & Maryanoff, B.E. (2008). Molecular pharmacodynamics,clinical therapeutics, and pharmacokinetics of topiramate. CNSNeuroscience & Therapeutics, 14, 120–142. doi: 10.1111/j.1527-3458.2008.00041.x
Skibicka, K.P., Shirazi, R.H., Rabasa-Papio, C., Alvarez-Crespo, M.,Neuber, C., Vogel, H., & Dickson, S.L. (2013). Divergent circuitryunderlying food reward and intake effects of ghrelin: DopaminergicVTA-accumbens projection mediates ghrelin’s effect on food rewardbut not food intake. Neuropharmacology, 73, 274–283. doi: 10.1016/j.neuropharm.2013.06.004
Smith, D., Dempster, C., Glanville, J., Freemantle, N., & Anderson, I.(2002). Efficacy and tolerability of venlafaxine compared with select-ive serotonin reuptake inhibitors and other antidepressants: A meta-analysis. British Journal of Psychiatry, 180, 396–404. Retrieved fromhttp://www.ncbi.nlm.nih.gov/pubmed/1198363510.1192/bjp.180.5.396
Smith, K.L., Rao, R.R., Vel�azquez-S�anchez, C., Valenza, M., Giuliano, C.,Everitt, B.J., … Cottone, P. (2015). The uncompetitive N-methyl-D-aspartate antagonist memantine reduces binge-like eating, food-seek-ing behavior, and compulsive eating: Role of the nucleus accumbensshell. Neuropsychopharmacology, 40, 1163–1171. doi: 10.1038/npp.2014.299
Smitka, K., Papezova, H., Vondra, K., Hill, M., Hainer, V., &Nedvidkova, J. (2013). The role of “mixed” orexigenic and anorexi-genic signals and autoantibodies reacting with appetite-regulatingneuropeptides and peptides of the adipose tissue-gut-brain axis:Relevance to food intake and nutritional status in patients with ano-rexia nervosa. International Journal of Endocrinology, 2013, 483145.doi: 10.1155/2013/483145
S€oderberg, J.A.E., Carlsson, M.A., & N€assel, D.R. (2012). Insulin-pro-ducing cells in the drosophila brain also express satiety-inducingcholecystokinin-like peptide, drosulfakinin. Frontiers inEndocrinology, 3, 109. doi: 10.3389/fendo.2012.00109
Soria-Gomez, E., Bellocchio, L., & Marsicano, G. (2014). New insightson food intake control by olfactory processes: The emerging role ofthe endocannabinoid system. Molecular and Cellular Endocrinology,397, 59–66. doi: 10.1016/j.mce.2014.09.023
Stanley, B.G., Kyrkouli, S.E., Lampert, S., & Leibowitz, S.F. (1986).Neuropeptide Y chronically injected into the hypothalamus: Apowerful neurochemical inducer of hyperphagia and obesity.Peptides, 7, 1189–1192. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/347071110.1016/0196-9781(86)90149-X
Stefano, S.C., Bacaltchuk, J., Blay, S.L., & Appolin�ario, J.C. (2008).Antidepressants in short-term treatment of binge eating disorder:Systematic review and meta-analysis. Eating Behaviors, 9, 129–136.doi: 10.1016/j.eatbeh.2007.03.006
Steiger, H., Labont�e, B., Groleau, P., Turecki, G., & Israel, M. (2013).Methylation of the glucocorticoid receptor gene promoter in bulimicwomen: Associations with borderline personality disorder, suicidal-ity, and exposure to childhood abuse. International Journal of EatingDisorders, 46, 246–255. doi: 10.1002/eat.22113
Steiger, H., & Thaler, L. (2016). Eating disorders, gene-environmentinteractions and the epigenome: Roles of stress exposures and
nutritional status. Physiology & Behavior, 162, 181–185. doi: 10.1016/j.physbeh.2016.01.041
Strober, M., Peris, T., & Steiger, H. (2014). The plasticity of develop-ment: How knowledge of epigenetics may advance understanding ofeating disorders. International Journal of Eating Disorders, 47,696–704. doi: 10.1002/eat.22322
Stunkard, A., Berkowitz, R., Tanrikut, C., Reiss, E., & Young, L. (1996).d-Fenfluramine treatment of binge eating disorder. American Journalof Psychiatry, 153, 1455–1459. doi: 10.1176/ajp.153.11.1455
Suh, J.J., Pettinati, H.M., Kampman, K.M., & O’brien, C.P. (2006). Thestatus of disulfiram. A half of a century later. Journal of ClinicalPsychopharmacology, 26, 290–302. doi: 10.1097/01.jcp.0000222512.25649.08
Sumiyoshi, T., Higuchi, Y., Matsui, M., Arai, H., Takamiya, C.,Meltzer, H.Y., & Kurachi, M. (2007). Effective adjunctive use oftandospirone with perospirone for enhancing verbal memory andquality of life in schizophrenia. Progress in Neuro-Psychopharmacology & Biological Psychiatry, 31, 965–967. doi:10.1016/j.pnpbp.2007.02.017
Sumiyoshi, T., Kunugi, H., & Nakagome, K. (2014). Serotonin anddopamine receptors in motivational and cognitive disturbances ofschizophrenia. Frontiers in Neuroscience, 8, 395. doi: 10.3389/fnins.2014.00395
Taghert, P.H., & Nitabach, M.N. (2012). Peptide neuromodulation ininvertebrate model systems. Neuron, 76, 82–97. doi: 10.1016/j.neuron.2012.08.035
Tanaka, H., Tatsuno, T., Shimizu, H., Hirose, A., Kumasaka, Y., &Nakamura, M. (1995). Effects of tandospirone on second messengersystems and neurotransmitter release in the rat brain. GeneralPharmacology, 26, 1765–1772. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/874516710.1016/0306-3623(95)00077-1
Tennoune, N., Chan, P., Breton, J., Legrand, R., Chabane, Y.N.,Akkermann, K., … Fetissov, S.O. (2014). Bacterial ClpB heat-shockprotein, an antigen-mimetic of the anorexigenic peptide a-MSH, atthe origin of eating disorders. Translational Psychiatry, 4, e458. doi:10.1038/tp.2014.98
Thaler, L., Gauvin, L., Joober, R., Groleau, P., de Guzman, R.,Ambalavanan, A., … Steiger, H. (2014). Methylation of BDNF inwomen with bulimic eating syndromes: Associations with childhoodabuse and borderline personality disorder. Progress in Neuro-Psychopharmacology & Biological Psychiatry, 54, 43–49. doi: 10.1016/j.pnpbp.2014.04.010
Thornton, L.M., Mazzeo, S.E., & Bulik, C.M. (2011). The heritability ofeating disorders: Methods and current findings. Current Topics inBehavioral Neurosciences, 6, 141–156. doi: 10.1007/7854_2010_91
Tolle, V., Kadem, M., Bluet-Pajot, M.-T., Frere, D., Foulon, C., Bossu, C.,… Estour, B. (2003). Balance in ghrelin and leptin plasma levels inanorexia nervosa patients and constitutionally thin women. Journal ofClinical Endocrinology and Metabolism, 88, 109–116. doi: 10.1210/jc.2002-020645
Tomasik, P.J., Sztefko, K., & Starzyk, J. (2004). Cholecystokinin, glucosedependent insulinotropic peptide and glucagon-like peptide 1 secre-tion in children with anorexia nervosa and simple obesity. Journal ofPediatric Endocrinology & Metabolism, 17, 1623–1631. Retrievedfrom http://www.ncbi.nlm.nih.gov/pubmed/1564569610.1515/JPEM.2004.17.12.1623
Tomasik, P.J., Sztefko, K., Starzyk, J., Rogatko, I., & Szafran, Z. (2005).Entero-insular axis in children with anorexia nervosa.Psychoneuroendocrinology, 30, 364–372. doi: 10.1016/j.psyneuen.2004.10.003
Treasure, J., Zipfel, S., Micali, N., Wade, T., Stice, E., Claudino, A., …Wentz, E. (2015). Anorexia nervosa. Nature Reviews. DiseasePrimers, 1, 15074. doi: 10.1038/nrdp.2015.74
Tremolizzo, L., Conti, E., Bomba, M., Uccellini, O., Rossi, M.S.,Marfone, M., … Nacinovich, R. (2014). Decreased whole-blood glo-bal DNA methylation is related to serum hormones in anorexianervosa adolescents. World Journal of Biological Psychiatry, 15,327–333. doi: 10.3109/15622975.2013.860467
Uher, R., Murphy, T., Brammer, M.J., Dalgleish, T., Phillips, M.L.,Ng, V.W., … Treasure, J. (2004). Medial prefrontal cortex activity
JOURNAL OF NEUROGENETICS 21
Dow
nloa
ded
by [
Uni
vers
ity o
f L
a L
agun
a V
icer
rect
orad
o] a
t 07:
00 0
1 A
ugus
t 201
7

associated with symptom provocation in eating disorders. AmericanJournal of Psychiatry, 161, 1238–1246. doi: 10.1176/appi.ajp.161.7.1238
Umberg, E.N., Shader, R.I., Hsu, L.K.G., & Greenblatt, D.J. (2012).From disordered eating to addiction: The “food drug”. in BulimiaNervosa. Journal of Clinical Psychopharmacology, 32, 376–389. doi:10.1097/JCP.0b013e318252464f
van den Pol, A.N. (2012). Neuropeptide transmission in brain circuits.Neuron, 76, 98–115. doi: 10.1016/j.neuron.2012.09.014
Vandereycken, W. (1984). Neuroleptics in the short-term treatment ofanorexia nervosa. A double-blind placebo-controlled study with sul-piride. British Journal of Psychiatry, 144, 288–292. Retrieved fromhttp://www.ncbi.nlm.nih.gov/pubmed/636787610.1192/bjp.144.3.288
Velligan, D.I., Alphs, L., Lancaster, S., Morlock, R., & Mintz, J. (2009).Association between changes on the negative symptom assessmentscale (NSA-16) and measures of functional outcome in schizophre-nia. Psychiatry Research, 169, 97–100. doi: 10.1016/j.psychres.2008.10.009
Volkow, N.D., Wang, G.-J., & Baler, R.D. (2011). Reward, dopamineand the control of food intake: Implications for obesity. Trends inCognitive Sciences, 15, 37–46. doi: 10.1016/j.tics.2010.11.001
Wade, T.D., Gordon, S., Medland, S., Bulik, C.M., Heath, A.C.,Montgomery, G.W., & Martin, N.G. (2013). Genetic variants associ-ated with disordered eating. The International Journal of EatingDisorders, 46, 594–608. doi: 10.1002/eat.22133
Walsh, B.T., Hadigan, C.M., Devlin, M.J., Gladis, M., & Roose, S.P.(1991). Long-term outcome of antidepressant treatment for bulimianervosa. American Journal of Psychiatry, 148, 1206–1212. doi:10.1176/ajp.148.9.1206
Walsh, B.T., Kaplan, A.S., Attia, E., Olmsted, M., Parides, M., Carter,J.C., … Rockert, W. (2006). Fluoxetine after weight restoration inanorexia nervosa: A randomized controlled trial. JAMA, 295,2605–2612. doi: 10.1001/jama.295.22.2605
Wang, K., Zhang, H., Bloss, C.S., Duvvuri, V., Kaye, W., Schork, N.J. …Price Foundation Collaborative Group. (2011). A genome-wide associ-ation study on common SNPs and rare CNVs in anorexia nervosa.Molecular Psychiatry, 16, 949–959. doi: 10.1038/mp.2010.107
Williams, D.L., Cummings, D.E., Grill, H.J., & Kaplan, J.M. (2003).Meal-related ghrelin suppression requires postgastric feedback.Endocrinology, 144, 2765–2767. doi: 10.1210/en.2003-0381
Woods, S.C., Seeley, R.J., Porte, D., & Schwartz, M.W. (1998). Signalsthat regulate food intake and energy homeostasis. Science (New York,N.Y.), 280, 1378–1383. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/960372110.1126/science.280.5368.1378
Woodside, B.D., & Staab, R. (2006). Management of psychiatric comor-bidity in anorexia nervosa and bulimia nervosa. CNS Drugs, 20,655–663. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/1686327010.2165/00023210-200620080-00004
Wu, C.-L., Doong, M.-L., & Wang, P.S. (2008). Involvement ofcholecystokinin receptor in the inhibition of gastrointestinal motilityby oxytocin in ovariectomized rats. European Journal ofPharmacology, 580, 407–415. doi: 10.1016/j.ejphar.2007.11.024
Wu, Q., Boyle, M.P., & Palmiter, R.D. (2009). Loss of GABAergic sig-naling by AgRP neurons to the parabrachial nucleus leads to starva-tion. Cell, 137, 1225–1234. doi: 10.1016/j.cell.2009.04.022
Yamashita, M., Takayanagi, Y., Yoshida, M., Nishimori, K., Kusama, M.,& Onaka, T. (2013). Involvement of prolactin-releasing peptide in theactivation of oxytocin neurones in response to food intake. Journal ofNeuroendocrinology, 25, 455–465. doi: 10.1111/jne.12019
Yilmaz, Z., Hardaway, J.A., & Bulik, C.M. (2015). Genetics and epigen-etics of eating disorders. Advances in Genomics and Genetics, 5,131–150. doi: 10.2147/AGG.S55776
Zarjevski, N., Cusin, I., Vettor, R., Rohner-Jeanrenaud, F., &Jeanrenaud, B. (1993). Chronic intracerebroventricular neuropeptide-Y administration to normal rats mimics hormonal and metabolicchanges of obesity. Endocrinology, 133, 1753–1758. doi: 10.1210/endo.133.4.8404618
Zerwas, S., & Bulik, C.M. (2011). Genetics and epigenetics of eatingdisorders. Psychiatric Annals, 41, 532–538. Retrieved fromhttp://www.ncbi.nlm.nih.gov/pubmed/2622921110.3928/00485713-20111017-06
Zhang, G., & Cai, D. (2011). Circadian intervention of obesity develop-ment via resting-stage feeding manipulation or oxytocin treatment.American Journal of Physiology, Endocrinology and Metabolism, 301,E1004–E1012. doi: 10.1152/ajpendo.00196.2011
Zhou, Y., & Kreek, M.J. (2015). Persistent increases in rathypothalamic POMC gene expression following chronic withdrawalfrom chronic “binge” pattern escalating-dose, but not steady-dose,cocaine. Neuroscience, 289, 63–70. doi: 10.1016/j.neuroscience.2014.12.078
Zhu, Y., Yamanaka, A., Kunii, K., Tsujino, N., Goto, K., & Sakurai, T.(2002). Orexin-mediated feeding behavior involves both leptin-sensi-tive and -insensitive pathways. Physiology & Behavior, 77, 251–257.Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/1241940110.1016/S0031-9384(02)00843-0
Zwanzger, P., Domschke, K., & Bradwejn, J. (2012). Neuronalnetwork of panic disorder: The role of the neuropeptidecholecystokinin. Depression and Anxiety, 29, 762–774. doi: 10.1002/da.21919
22 GERM�AN CUESTO ET AL.
Dow
nloa
ded
by [
Uni
vers
ity o
f L
a L
agun
a V
icer
rect
orad
o] a
t 07:
00 0
1 A
ugus
t 201
7
View publication statsView publication stats
Recommended