
Improving Adult VaccinationProtecting our Most Vulnerable
Dale W. Bratzler, DO, MPHPrincipal Clinical Coordinator
Do the vaccines work?
Myth: Vaccines don’t work in hospitalized patients.
3
Missed Opportunities
• Influenza vaccine is immunogenic in hospitalized patients and patients with chronic renal failure
• Pneumococcal vaccine approximately 50-75% effective preventing invasive disease
Berry BB et al. Vaccine. 2001;19:3493-3498.
Brydak LB et al. Vaccine. 2000;18:3280-3286.
Christenson B, et al. Lancet. 2001;357:1008-1011.
Nichol KL, et al. Arch Intern Med. 1999;159:2437-2442.
Nichol KL. Vaccine. 1991;17(suppl 1):S91-S93.

4
Influenza VaccinationReductions in Hospitalization and Death
2 yr study of elderly members of 3 HMO’s- 1998-99 & 1999-00 seasons with > 140,000 persons in each year’s cohort
Nichol KL, et al. N Engl J Med. 2003;348:1322-1332.
19% 16%32%
48%23%

5 Benefits of Pneumococcal Vaccinations
Group Effectiveness / Cost Savings
All Elderly Persons 1
Bacteremias 75% (57% to 85%)Cost savings $8.27 per person
Elderly w/ Chronic Lung Disease 2
Hospitalizations for pneumonia 43% (16% to 62%)
Deaths 29% (9% to 44%)Cost savings $294 per person
1 Sisk J. JAMA 1997; 278: 1333.2 Nichol KL. Arch Intern Med 1999; 159: 2437.
6 Effectiveness of Pneumococcal Vaccination in Older Adults:The VSD Cohort Study
• 3 year cohort study of 47,365 members of Group Health Coop (Seattle)
• PPV was associated with lower rates of bacteremia:• HR 0.56 (95% CI 0.33 – 0.93)
• PPV was not associated with lower rates of community acquired pneumonia• HR 1.07 (95% CI 0.99 – 1.14)
HR = hazard ratio. Jackson LA, et al. NEJM 2003; 348: 1747.
7
Do the vaccines work??
• All agree, we need more effective vaccines
• Influenza vaccines that can be produced more rapidly after identification of a viral strain

What about immunosuppressed patients?
Myth: We shouldn’t vaccinate immunosuppressed patients.

9
Missed Opportunities
• Immunocompromised persons• PPV
• HIV, leukemia, lymphoma, Hodgkins ds, multiple myeloma, malignancy, those receiving immunosuppressive chemotherapy, and those who have received an organ or bone marrow transplant
• Influenza• Immunosuppression caused by medications or
by HIVCDC. MMWR. 1997;46(RR-8):1-24.
CDC. MMWR. 2003;52(RR-8):1-36.

Is Vaccination Safe?
Myth: Vaccination is not safe for patients in the hospital. (vaccination
can make me sick)
11 Missed OpportunitiesMyth: Hospital Vaccination is Not Safe
• Many hospital and emergency department-based vaccination programs have been safely and effectively implemented with no evidence of significant risk
Klein RS, et al. Arch Intern Med. 1983;143:1878-1881. (hospital pneumococcal vaccine)
Magnussen CR, et al. Arch Intern Med. 1984;144:1755-1757. (hospital and ambulatory pneumococcal vaccine)
Bloom HG, et al. J Am Geriat Soc. 1988;36:897-901. (hospital influenza and pneumococcal vaccines)
Crouse BJ, et al. J Fam Pract. 1994;38:258-261. (hospital-based influenza vaccination)
Nichol KL, et al. Am J Med. 1998;105:385-392. (10-year experience with inpatient influenza and pneumococcal vaccination)
Rodriquez RM, et al. Ann Emerg Med. 1993;22:1729-1732. (ER-based influenza and pneumococcal vaccination)
Slobodkin D, et al. Vaccine. 1998;16:1795-1802. (Inner-city ER-based influenza and pneumococcal vaccination)
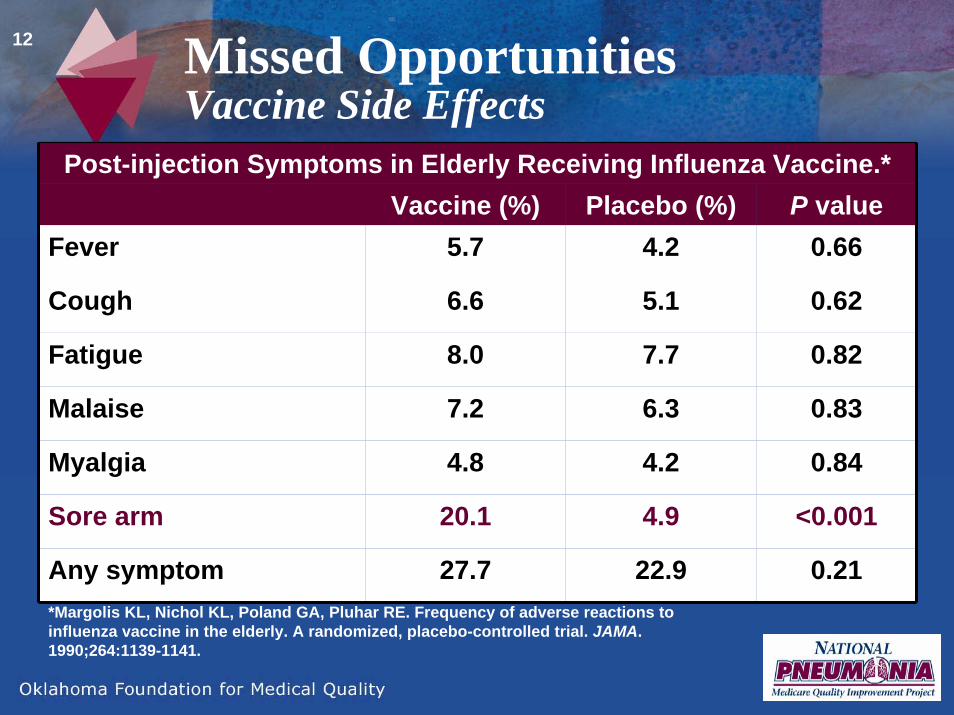
12 Missed OpportunitiesVaccine Side Effects
Post-injection Symptoms in Elderly Receiving Influenza Vaccine.*Vaccine (%) Placebo (%) P value
Fever 5.7 4.2 0.66
Cough 6.6 5.1 0.62
Fatigue 8.0 7.7 0.82
Malaise 7.2 6.3 0.83
Myalgia 4.8 4.2 0.84
Sore arm 20.1 4.9 <0.001
Any symptom 27.7 22.9 0.21*Margolis KL, Nichol KL, Poland GA, Pluhar RE. Frequency of adverse reactions to influenza vaccine in the elderly. A randomized, placebo-controlled trial. JAMA. 1990;264:1139-1141.

13 Missed OpportunitiesVaccine Side Effects
Systemic Symptoms Experienced Before and After Pneumococcal Vaccination.*
Pre-vaccination (%) Post-vaccination (%) P valueFever 2.6 1.9 0.37Rash 4.8 0.7 <0.01Myalgias 11 1.4 <0.01
Fatigue 18.2 3.5 <0.01Malaise 8.3 2.6 <0.01
Headache 4.6 0.9 <0.01
Overall health (same as usual)
90.1 97.9 <0.01
*Nichol KL, Mac Donald R, Hauge M. Side effects associated with pneumococcal vaccination. Am J Infect Control. 1997;25:223-228.

14 Vaccination Reality in the USThe Why…..
Despite the fact that influenza and pneumococcal vaccines are:• clinically effective
• cost effective
• safe, and
• free to most elderly patients
They are under-utilized!

Why should we vaccinate hospitalized patients?
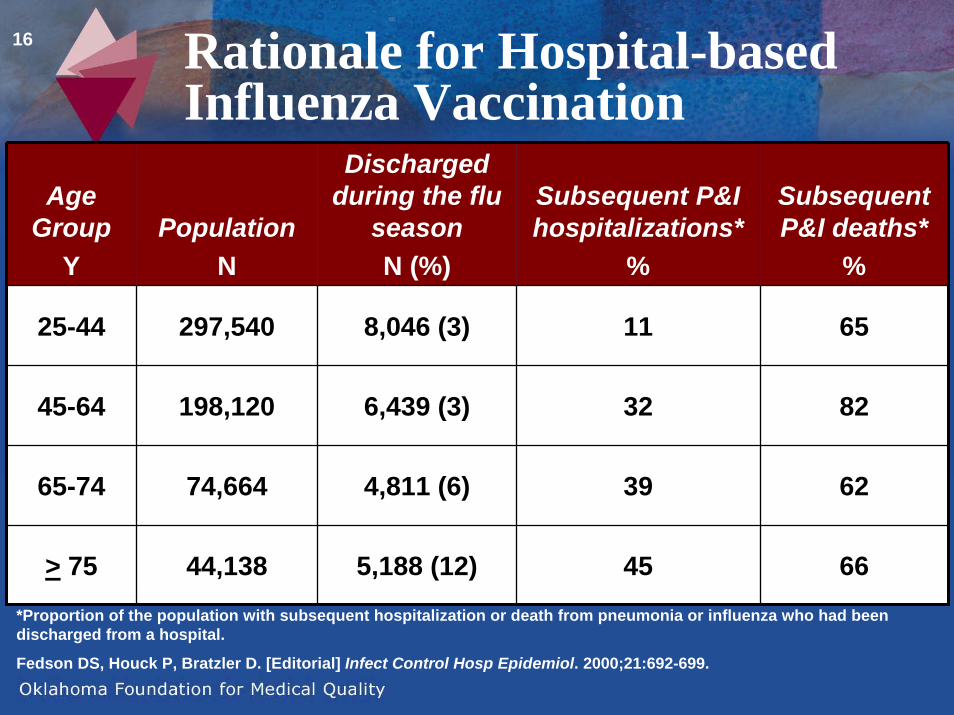
16 Rationale for Hospital-based Influenza Vaccination
Age Group
YPopulation
N
Discharged during the flu
seasonN (%)
Subsequent P&I hospitalizations*
%
Subsequent P&I deaths*
%
25-44 297,540 8,046 (3) 11 65
45-64 198,120 6,439 (3) 32 82
65-74 74,664 4,811 (6) 39 62
> 75 44,138 5,188 (12) 45 66*Proportion of the population with subsequent hospitalization or death from pneumonia or influenza who had been discharged from a hospital.
Fedson DS, Houck P, Bratzler D. [Editorial] Infect Control Hosp Epidemiol. 2000;21:692-699.

17 Missed OpportunitiesBackground
Fedson DS, et al. Infect Control Hosp Epidemiol. 2000;21:692-699.

18
Why give them in the hospital?
• Failure to vaccinate hospitalized patients is a missed opportunity• Hospitalized patients may be at
particularly risk of subsequent complications of influenza and pneumococcal disease
19 Is Hospital-based Vaccination the Standard of Care?
• CMS and JCAHO have adopted influenza and pneumococcal vaccination of inpatients as measures of hospital quality
• PPV written into the MMA as a publicly reported measure of quality
• Hospital Compare• Recommended by ACIP, IDSA, and
others
20 PN-2: Pneumococcal Vaccination
• Numerator• Patients with pneumonia, age 65 and older, who
were screened for pneumococcal vaccine status and were vaccinated prior to discharge, if indicated
• Denominator• Pneumonia patients 65 years of age and older
• Key Exclusions• Transfers from another acute care facility, no
working diagnosis of pneumonia on admission, patients receiving comfort care only, expired in hospital, left AMA, discharged to hospice care, transferred to another hospital

21
PN-7: Influenza Vaccination• Numerator
• Patients discharged during October through February with pneumonia, age 50 and over, who were screened for influenza vaccine status and were vaccinated prior to discharge, if indicated
• Denominator• Pneumonia patients 50 years and older
• Key Exclusions• Transfers from another acute care facility, no working
diagnosis of pneumonia on admission, patients receiving comfort care only, expired in hospital, left AMA, discharged to hospice care, diagnosis of influenza, transferred to another acute care hospital
22
Additional Measure Notes
• We exclude patients who have had a bone marrow transplantation within the past year and patients actively receiving chemotherapy or radiation therapy
• Influenza vaccine not available – this variable is only allowed when there is a national shortage of vaccine

23 ResultsInfluenza
Take home – still no documentation in 61% of patients!
0
5
10
15
20
25
30
35
40
45
10/2000-02/2001 01/2002-02/2002 10/2002-02/2003 10/2003-02/2004
Perc
ent
Vaccinated Prior to Arrival Contraindicated Refused
Proportion of Medicare patients discharged with a discharge diagnosis of pneumonia that were screened for or vaccinated prior to discharge.
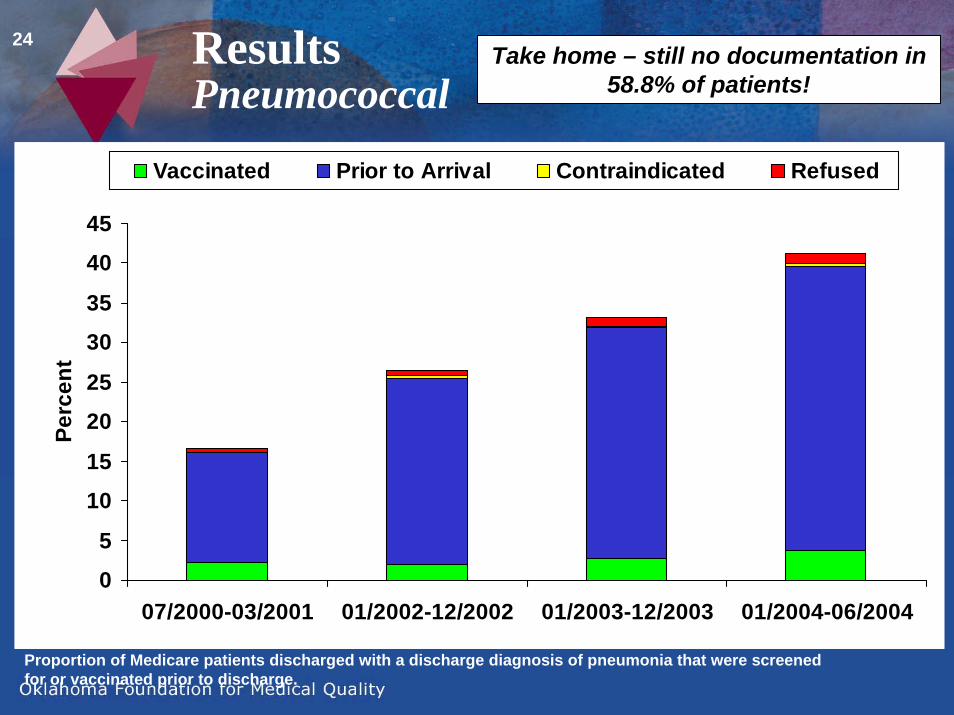
24 ResultsPneumococcal
Take home – still no documentation in 58.8% of patients!
0
5
10
15
20
25
30
35
40
45
07/2000-03/2001 01/2002-12/2002 01/2003-12/2003 01/2004-06/2004
Perc
ent
Vaccinated Prior to Arrival Contraindicated Refused
Proportion of Medicare patients discharged with a discharge diagnosis of pneumonia that were screened for or vaccinated prior to discharge.

25
Where are we at now?
• Targeted efforts to measure performance and promote quality improvement on hospital-based vaccination have resulted in improved documentation of patient vaccination status……………

26
Where are we at now?
…….However• Overall rates of inpatient vaccination
have only marginally improved
• There is no information on vaccination status for more than half of the Medicare patients discharged from the hospital
27
Where are we at now?
• Refusals and contraindications accounted for a small proportion of the improvement in vaccination/screening documentation in Medicare patients
28
Where’s the greater risk of liability??
29
Where is the liability risk?
• Liability cases in three states• Very consistent theme
• Young males who have previously had a splenectomy (no documentation of PPV)
• Subsequently hospitalized (in some, multiple times) –not given PPV
• At least one case had visits to primary care physicians and an emergency department – not given PPV
• All three developed purpura fulminans (two with significant amputations, one with menigitis and renal failure, one death)

30
Amsden said the jury's verdict would send a message to the hospital that it is focusing on the wrong areas for cost savings. Jordan's last day at the hospital
cost $18,000 - the vaccine would have cost $25.
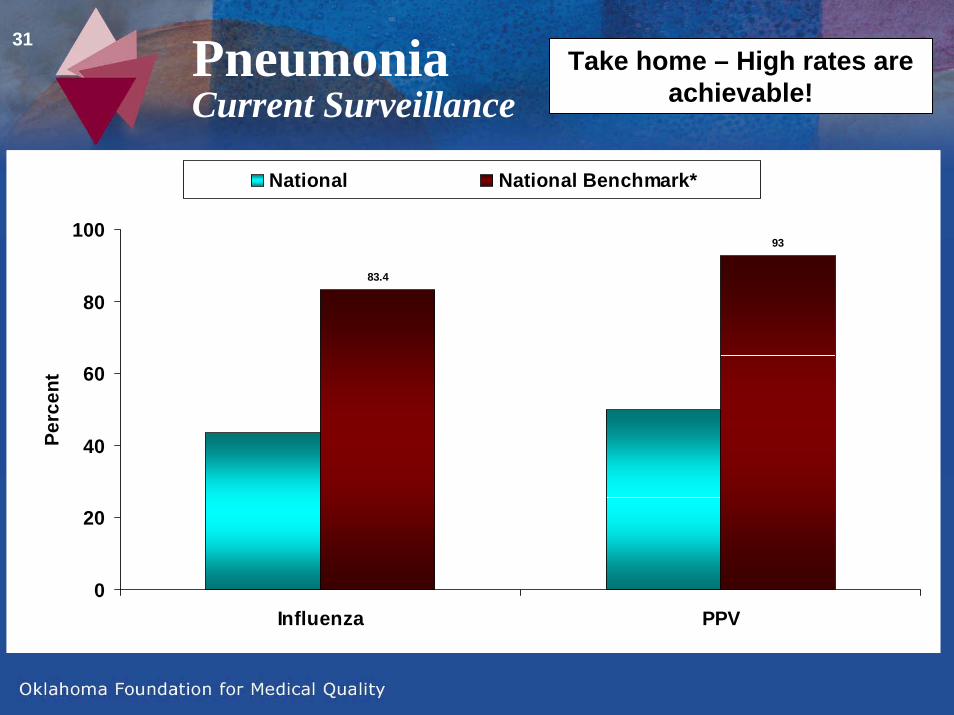
31 PneumoniaCurrent Surveillance
Take home – High rates are achievable!
83.4
93
0
20
40
60
80
100
Influenza PPV
Perc
ent
National National Benchmark*

32
Where Should We Vaccinate?
Anywhere that we find chronically ill or elderly
patients!
33 Systems-based StrategiesInstitutional Vaccination
• Strategies to improve vaccination rates• Organizational change• Provider reminders• Patient financial incentives• Provider financial incentives• Patient reminders• Provider education• Patient education• Assessment and feedback
RAND. Evidence Report and Evidence-based Recommendations: Interventions that increase utilization of Medicare-funded Preventive Services for Persons Age 65 and Older. US Dept of Health and Human Services. Health Care Financing Administration. Contract No. 500-98-0281. September 30, 1998.
Task Force on Community Preventive Services. Guide to Community Preventive Services. Am J Prev Med. 2000;18(1S):S97-140.
34
Standing Orders Programs
Standing orders programs authorize nurses or pharmacists to administer vaccinations according to an institution- or physician-approved protocol without a physician’s examination

35 Standing Orders are Among the Most Effective Strategies
• Non-physicians offer and administer vaccinations without direct doctor involvement at the time of the visit
• Established through approved policies & protocols
• Locations: clinics, hospitals & nursing homes
36
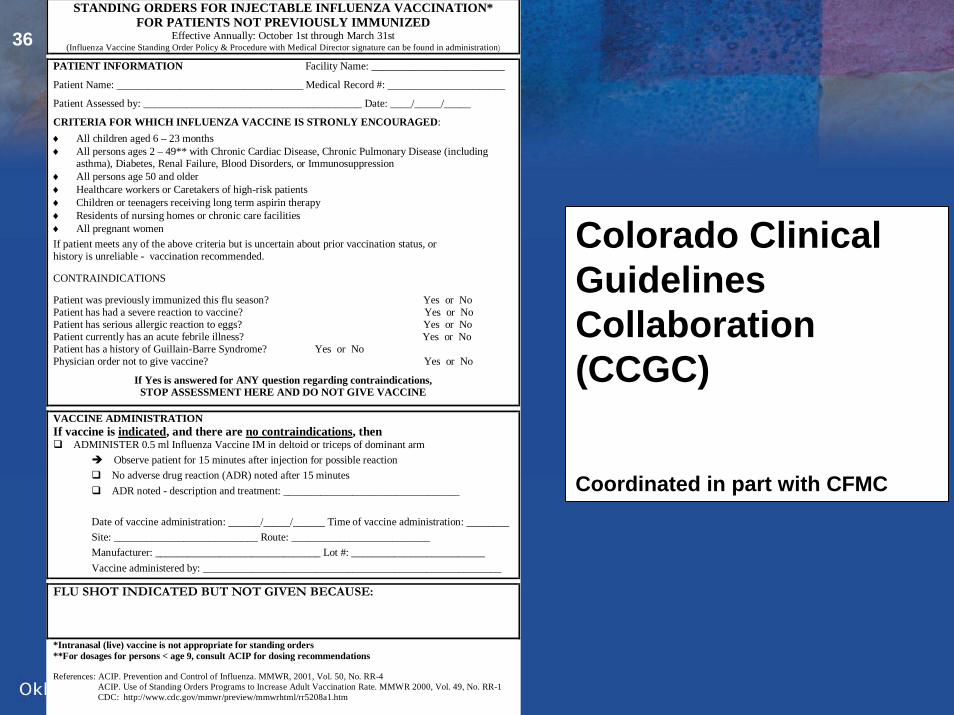
STANDING ORDERS FOR INJECTABLE INFLUENZA VACCINATION* FOR PATIENTS NOT PREVIOUSLY IMMUNIZED
Effective Annually: October 1st through March 31st (Influenza Vaccine Standing Order Policy & Procedure with Medical Director signature can be found in administration)
PATIENT INFORMATION Facility Name: _________________________
Patient Name: ___________________________________ Medical Record #: ______________________
Patient Assessed by: _________________________________________ Date: ____/_____/_____
CRITERIA FOR WHICH INFLUENZA VACCINE IS STRONLY ENCOURAGED: ♦ All children aged 6 – 23 months ♦ All persons ages 2 – 49** with Chronic Cardiac Disease, Chronic Pulmonary Disease (including
asthma), Diabetes, Renal Failure, Blood Disorders, or Immunosuppression ♦ All persons age 50 and older ♦ Healthcare workers or Caretakers of high-risk patients ♦ Children or teenagers receiving long term aspirin therapy ♦ Residents of nursing homes or chronic care facilities ♦ All pregnant women If patient meets any of the above criteria but is uncertain about prior vaccination status, or history is unreliable - vaccination recommended.
CONTRAINDICATIONS
Patient was previously immunized this flu season? Yes or No Patient has had a severe reaction to vaccine? Yes or No Patient has serious allergic reaction to eggs? Yes or No Patient currently has an acute febrile illness? Yes or No Patient has a history of Guillain-Barre Syndrome? Yes or No Physician order not to give vaccine? Yes or No
If Yes is answered for ANY question regarding contraindications, STOP ASSESSMENT HERE AND DO NOT GIVE VACCINE
VACCINE ADMINISTRATION If vaccine is indicated, and there are no contraindications, then ADMINISTER 0.5 ml Influenza Vaccine IM in deltoid or triceps of dominant arm
Observe patient for 15 minutes after injection for possible reaction No adverse drug reaction (ADR) noted after 15 minutes ADR noted - description and treatment: _________________________________
Date of vaccine administration: ______/_____/______ Time of vaccine administration: ________ Site: ___________________________ Route: __________________________ Manufacturer: _______________________________ Lot #: _________________________ Vaccine administered by: ________________________________________________________
FLU SHOT INDICATED BUT NOT GIVEN BECAUSE:
*Intranasal (live) vaccine is not appropriate for standing orders **For dosages for persons < age 9, consult ACIP for dosing recommendations References: ACIP. Prevention and Control of Influenza. MMWR, 2001, Vol. 50, No. RR-4
ACIP. Use of Standing Orders Programs to Increase Adult Vaccination Rate. MMWR 2000, Vol. 49, No. RR-1 CDC: http://www.cdc.gov/mmwr/preview/mmwrhtml/rr5208a1.htm
Colorado Clinical Guidelines Collaboration (CCGC)
Coordinated in part with CFMC

37 Comparison of Florida PPVRates* to Vaccination Process
* Hospital-submitted data in CMS Warehouse
Courtesy FMQAI.
38 Institutional VaccinationConditions of Participation
• Federal Register, Vol. 67, No. 191 (October 2, 2002)“All orders for drugs and biologicals must be in
writing and signed by the practitioner or practitioners responsible for the care of the patient as specified under 482.12(c) with the exception of influenza and pneumococcal polysaccharide vaccines, which may be administered per physician-approved facility policy after an assessment for contraindications.”
• Includes similar provisions for nursing homes and home health agencies
39 Opportunities for Cross-setting Initiatives
• Hospitals and home health agencies
• Nursing homes and home health agencies
• Mass vaccinators
40
Annual influenza vaccination is recommended for all persons who work in any medical care facility or
at increased risk of influenza or complications of influenza.
provide care in any setting to persons

41 Deaths Due to Vaccine Preventable Diseases - US, 1989-1998
77486Tetanus6553,634Pertussis214412Rubella724,075Mumps
13260,189Measles9694146,644Hepatitis B1013282,650Hepatitis A
~ 120,000(millions)Pneumococcal~ 510,000 (millions)Influenza
Deaths (all ages)CasesDisease*~ 630k(90% in elderly)
11k (reported cases though the actual number is likely 5-10 times higher)
VPD = vaccine preventable diseases.MMWR 2001; 48 (RR-53); Thompson et al. JAMA 2003; 289: 179; Feikin DR, et al. Am J Public Health 2000; 90: 223-9.
42
Poland GA. Clin Infect Dis. 2002;35:378-380.
43
Summary
• Vaccination rates for our most vulnerable are unacceptably low
• Vaccination in these settings is effective!
• Systems-based interventions are the best way to improve vaccination rates
Recommended

















