IMMEDIATE (UNDELAYED) MUSCULOCUTANEOUS ISLAND CROSS LEG FLAPS
By MIGUEL ORTICOCHEA, M.D.* School of Medicine, Montevideo University, Urugua_v
MUSCULOCUTANEOUS flaps are successful transplants because in many cases the skin overlying a muscle is supplied by branches of the vessels supplying the muscle. Where the blood vessels supplying the muscle are limited to I or 2 vascular pedicles, the musculocutaneous flap is analogous to an axial pattern flap and may be similarly trans- planted.
Much work has been and is being carried out to define suitable and reliable combinations of muscles and overlying skin (Olivari, 1976; McGraw and Dibbell, 1977). I have previously described the uses of the gracilis musculocutaneous flap (Orticochea, 1972a, 1972b) and I now wish to describe a musculocutaneous flap based on the sartorius muscle and one on the gastrocnemius muscle. Both were used as “island flaps”; they were completely detached, apart from the vascular pedicle. Both, too, were used as cross leg flaps; their great advantage over conventional cross leg flaps is that they may be reliably transposed without needing any previous delay.
Most of the technique will be obvious from the illustrations (Figs. I to 15) but 2 additional points are stressed.
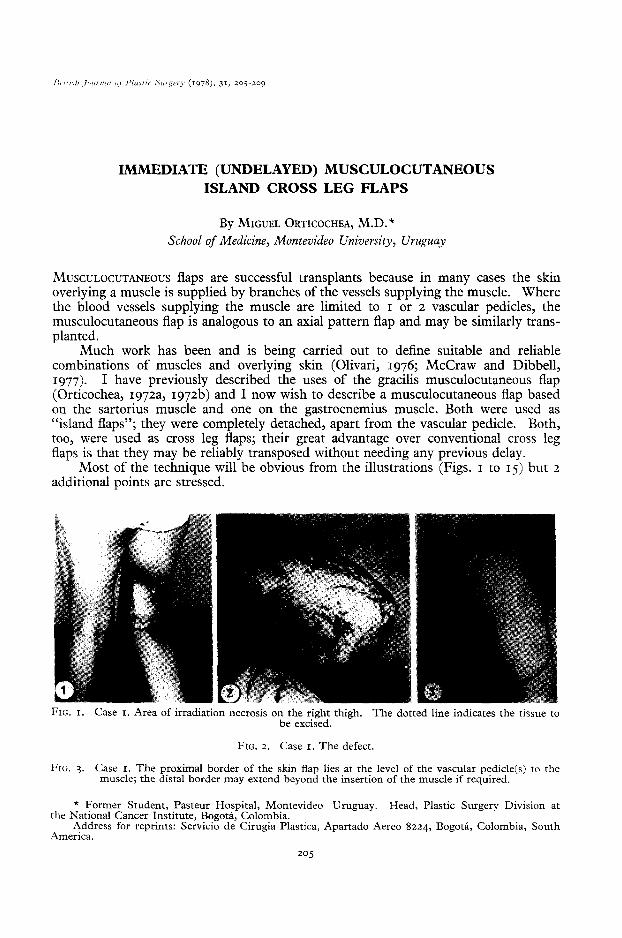
FIG. I. Case I. Area of irradiation necrosis on the right thigh. The dotted line indicates the tissue to be excised.
FIG. 2. Case I. The defect.
FIG. 3. Case I. The proximal border of the skin flap lies at the level of the vascular pedicle(s) to the muscle; the distal border may extend beyond the insertion of the muscle if required.
* Former Student, Pasteur Hospital, Montevideo Uruguay. the National Cancer Institute, Bogota, Colombia.
Head, Plastic Surgery Division at
Address for reprints: Servicio de Cirugia Plastica, Apartado Aereo 8224, Bogota, Colombia, South America.
205

206 BRITISH JOURNAL OF PLASTIC SURGERY
FIG. 4. Case I. The flap has been incised and tfer+;;torius muscle (I) dissected and divided above and
FXG. 5. Case I. The 2 vascular pedicles to the sartorius muscle from the profunda femoris vessels are displayed (3, 3).
FIG. 6. Case I. Only the blood vessels attach the musculocutaneous flap to its original site. The cut ends of the sartorius muscle are shown (I and 2). The flap may readily be rotated through 90” without
occluding the vessels. Suture of the flap to the defect in the other leg has begun.
FIG. 7. Case I. Insertion of the flap is complete.

MUS~~LOCUTANEOUS ISLAND CROSS LEG FLAPS 207
FIG. 8. Case I. Four weeks later, prior to dividing the pedicle of sartorius muscle (I).
FIG. 9. Case I. A and B. Final result. The musculocutaneous flap (I) and the split skin grafted donor area (2).
FIG. IO. Case 2. Area of radionecrosis to be excised. Because of the contraction in the popliteal region the patient could not extend the leg.
FIG. I I. Case 2. The proximal margin of the skin is again at the level where the blood vessels enter the gastrocnemius. The incision to permit exposure of the 2 heads of the muscle is also shown.
208 BRITISH JOURNAL OF PLASTIC SURGERY
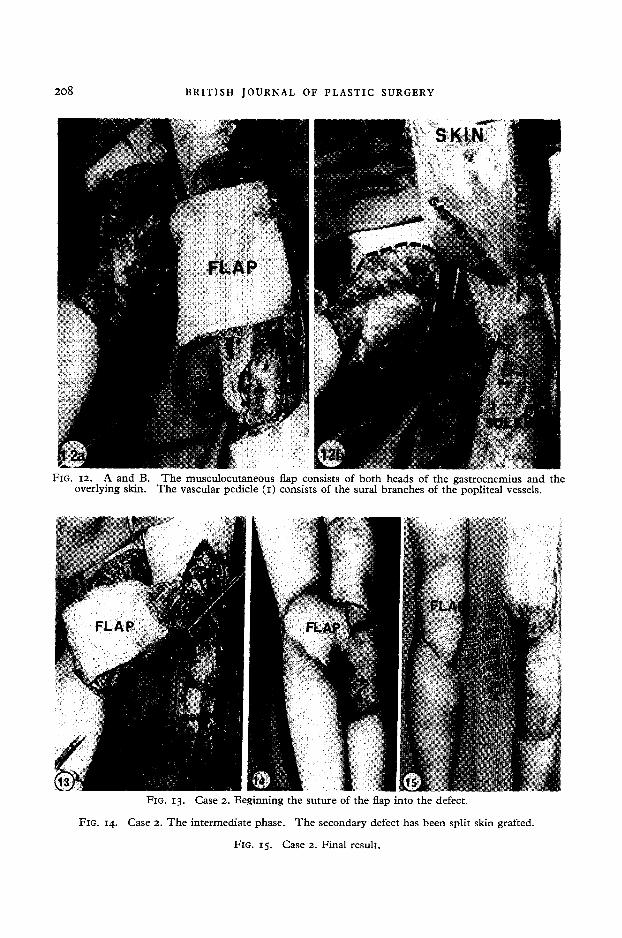
FIG. 12. A and B. The musculocutaneous flap consists of both heads of the gastrocnemius and the overlying skin. The vascular pedicle (I) consists of the sural branches of the popliteal vessels.
FIG. 13. Case 2. Beginning the suture of the flap into the defect.
FIG. 14. Case 2. The intermediate phase. The secondary defect has been split skin grafted.
FIG. 15. Case 2. Final result.

.MlJSCULOCUTANEOUS ISLAND CROSS LEG FLAPS 209
The proximal edge of the cutaneous part of the flap should overlie the vascular pedicle to the muscle. In other words the area supplied by the vascular pedicles is distal to their site of entry into the muscle.
Secondly, the skin is often attached to the muscle by a tenuous layer of superficial fascia. The small perforating blood vessels pass through this layer and may easily be damaged if any shearing stress is imparted to the skin during the operation. When the muscle is divided therefore the ends should be sutured with catgut to the overlying fat.
REFERENCES
IMCCRAW, J. B. and DIBBELL, D. G. (1977). Experimental definition of independent myocutaneous vascular territories. Plastic atzd Reconstructive Surger_v, 60, ZIZ.
OLIVARI, N. (1976). The latissimus flap. British 3ournal of Plastic Surgery, 29, 126. ORTICOCHEA, M. (1972~). The musculo-cutaneous flap method: an immediate and heroic
substitute for the method of delay. British 3011rr2al of Plastic Surgery, 25, 106. ORTICOCHEA, M. (1972b). A new method of total reconstruction of the penis. British
Jowxal of Plastic Surgery, 25, 347.
313-c
Recommended

















