Drug Therapy for Hypercholesteromia &
Dyslipidemia
URVI KOLHATKAR
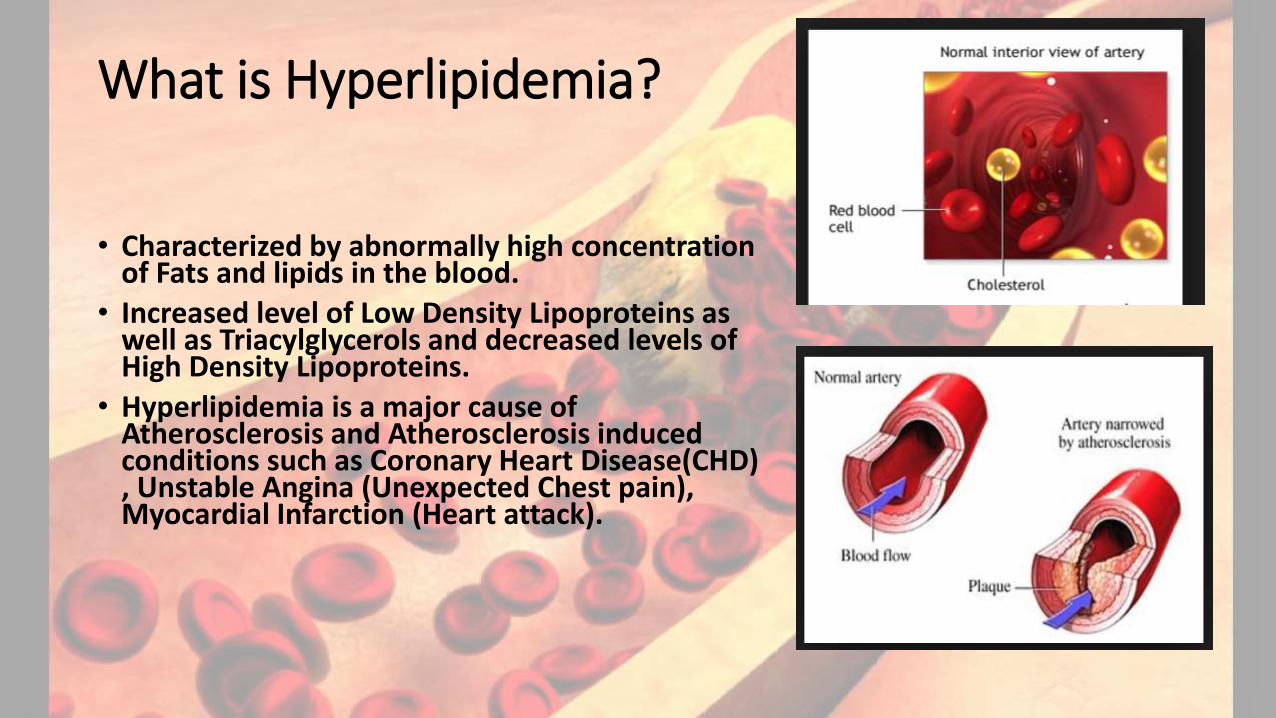
What is Hyperlipidemia?
• Characterized by abnormally high concentration of Fats and lipids in the blood.
• Increased level of Low Density Lipoproteins as well as Triacylglycerols and decreased levels of High Density Lipoproteins.
• Hyperlipidemia is a major cause of Atherosclerosis and Atherosclerosis induced conditions such as Coronary Heart Disease(CHD) , Unstable Angina (Unexpected Chest pain), Myocardial Infarction (Heart attack).
Causes of Hyperlipidemia
• Diet or change in Lifestyle.
• Obesity
• Pregnancy
• Acute Hepatitis
• Diabetes Mellitus
• Nephrotic Syndrome
• Obstructive Liver Disease
• Single Inherited Gene defect in Lipoproteins metabolism.
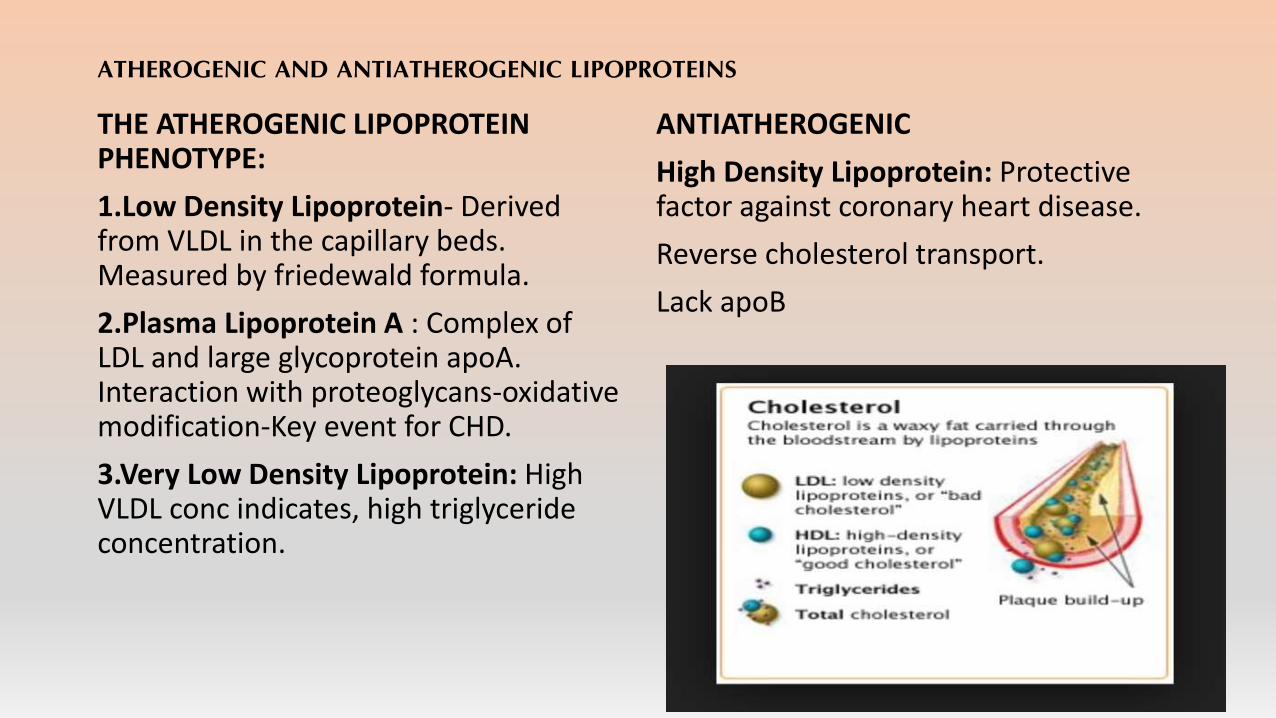
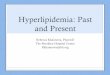
ATHEROGENIC AND ANTIATHEROGENIC LIPOPROTEINS
THE ATHEROGENIC LIPOPROTEIN PHENOTYPE:
1.Low Density Lipoprotein- Derived from VLDL in the capillary beds. Measured by friedewald formula.
2.Plasma Lipoprotein A : Complex of LDL and large glycoprotein apoA. Interaction with proteoglycans-oxidative modification-Key event for CHD.
3.Very Low Density Lipoprotein: High VLDL conc indicates, high triglyceride concentration.
ANTIATHEROGENIC
High Density Lipoprotein: Protective factor against coronary heart disease.
Reverse cholesterol transport.
Lack apoB
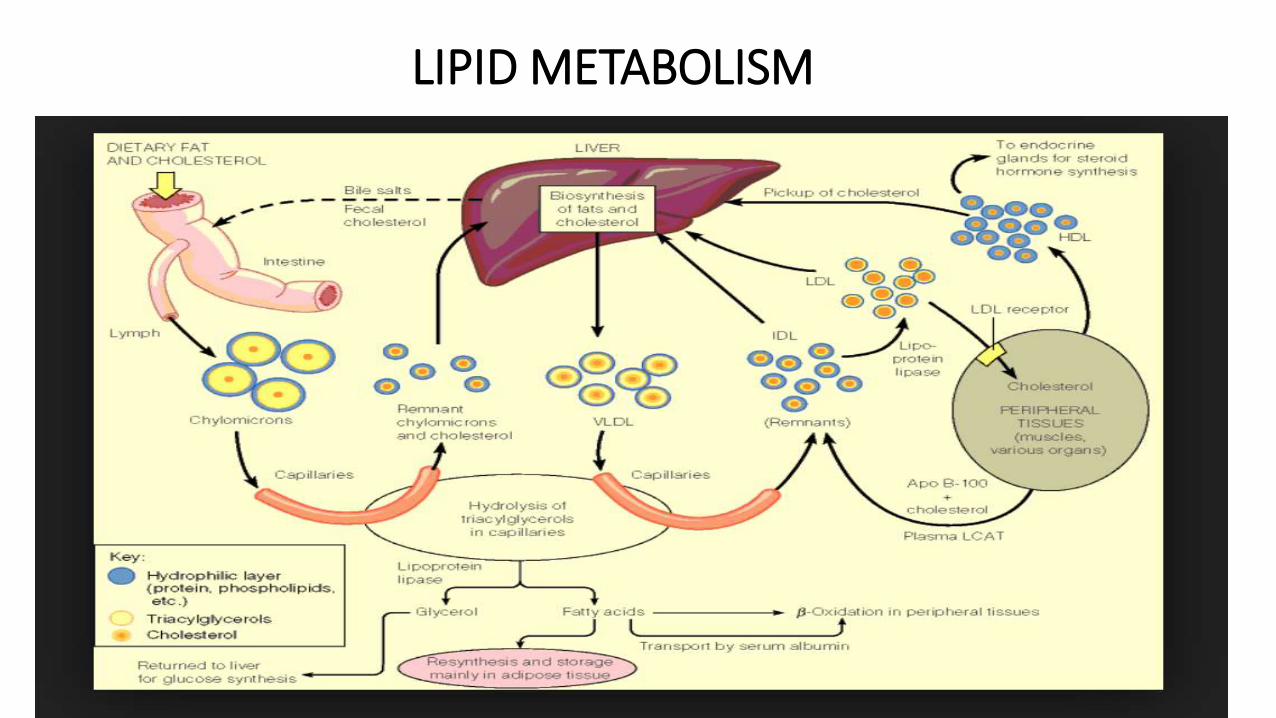
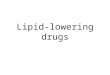
LIPID METABOLISM
DRUG THERAPY OF DYSLIPIDEMIA
1.STATINS :Competitive Inhibitors of (3-Hydroxy-3-methylglutaryl) HMG-CoA reductase, which lowers LDL by inhibiting an early rate-limiting step in cholesterol synthesis.•Drugs under this class are:Lovastatin,pravastatin,simvastatin,Atorvastatin,fluvastatin,rosuvastatin and pitavastatin.
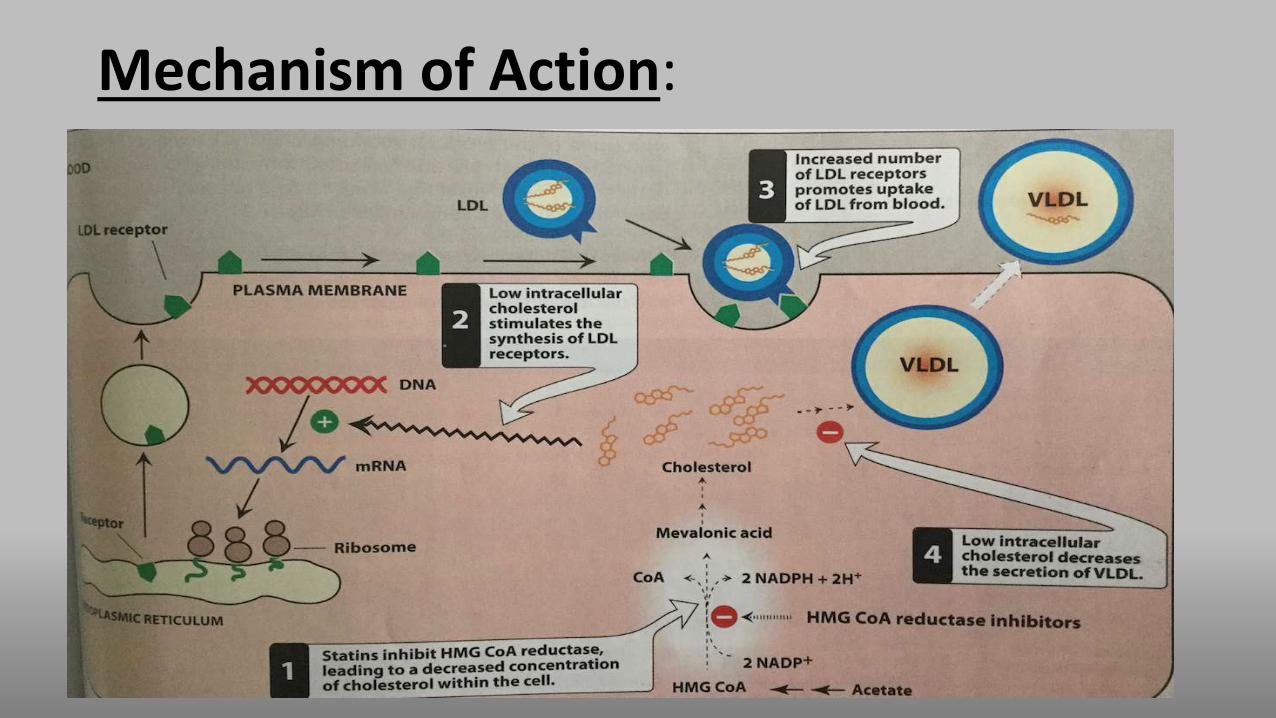
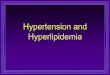
Mechanism of Action:
By reducing the conversion of HMG CoA reductase to Mevalonate, Statins inhibit an early rate-limiting step in cholesterol biosynthesis.
By reducing the hepatic cholesterol synthesis, they also lead to an increased expression of LDL receptor gene.
Statin therapy leads to enhanced production of vasodilator Nitric oxide, contributing to an improved endothelial function.
• Statins lead to plaque stabilization and modulate cellularity of the artery wall.
• Statins decreased the levels of CRP, thus they lower the risk of CHD and inhibit the inflammatory processes.
• Statins prevent susceptibility of Lipoprotein to oxidation.
• Statins repurposed for increasing the bone cell volume and to bolster the bones, this could be a new therapeutic breakthrough for treatment of Osteoporosis.
Ref:http://www.ncbi.nlm.nih.gov/pubmed/10583956
Therapeutic Uses:
• Effective in all types of hyperlipidemias
• Patients with homozygous familial hypercholesteromia benefit less with this drug class.
Adverse Effects:a.Liver:
• Hepatotoxicity.
• Hepatic Insufficiency can cause drug accumulation.
b.Muscle:
• Muscle myopathy and rhabdomyolysis has also been reported rarely.
Drug Interactions:
• The HMG CoA reductase inhibitors could increase warfarin levels.
Contraindications:Statins are contraindicated during pregnancy and for nursing mothers.
Why are statins administered before bedtime or evening?
Hepatic cholesterol synthesis is maximal between midnight and 2:00 AM, thus statins with a t1/2 of 4 hours should be administered in the evening with a recommended dose of 20 mg.
2.The Fibrates:
• This drug class includes Fenofibrate and gemfibrozil.
• These drugs are derivative of fibric acid and they execute the lipid lowering action by decreasing the serum triacylglycerols and by increasing the serum HDL levels.
Mechanism of Action: Lipid lowering action by interaction with peroxisome proliferator-activated receptors (PPARs). This receptor supergene family regulates the Lipid Metabolism.
Fibrate mediated PPAR gene expression leads to decreased triglycerolconcentration by increasing the expression of lipoprotein lipase and decreasing apolipoprotein C II concentration.
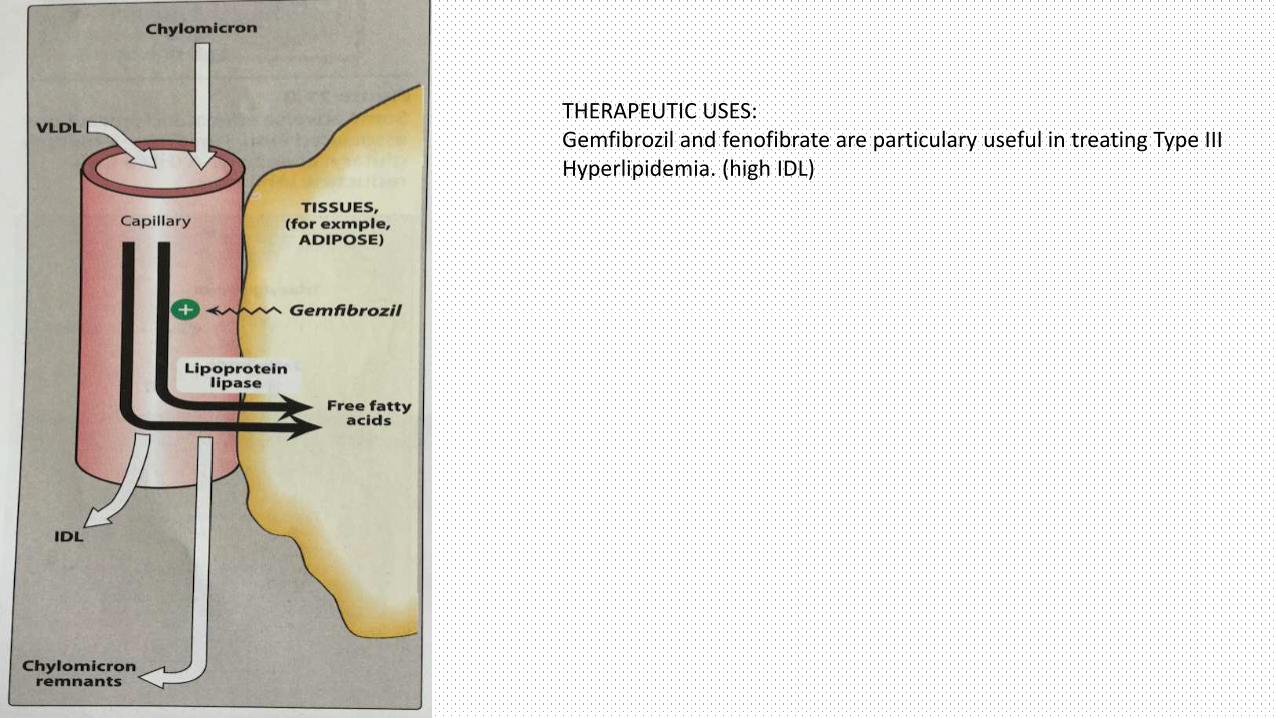
THERAPEUTIC USES:Gemfibrozil and fenofibrate are particulary useful in treating Type III Hyperlipidemia. (high IDL)
Adverse Effects:
• Gastrointestinal Disturbances
• Increased lithogenecity of bile
• Myopathy syndrome
• Myositis
Contraindications: Their safety has not been established for pregnant or lactating women. Patients with renal or hepatic insufficiency or pre-existing gall bladder disease should not be administered with this class of hyperlipidemic drugs.
Drug Interactions: Compete with coumarin anti-coagulants for binding sites on plasma proteins, hence INR should be monitored.
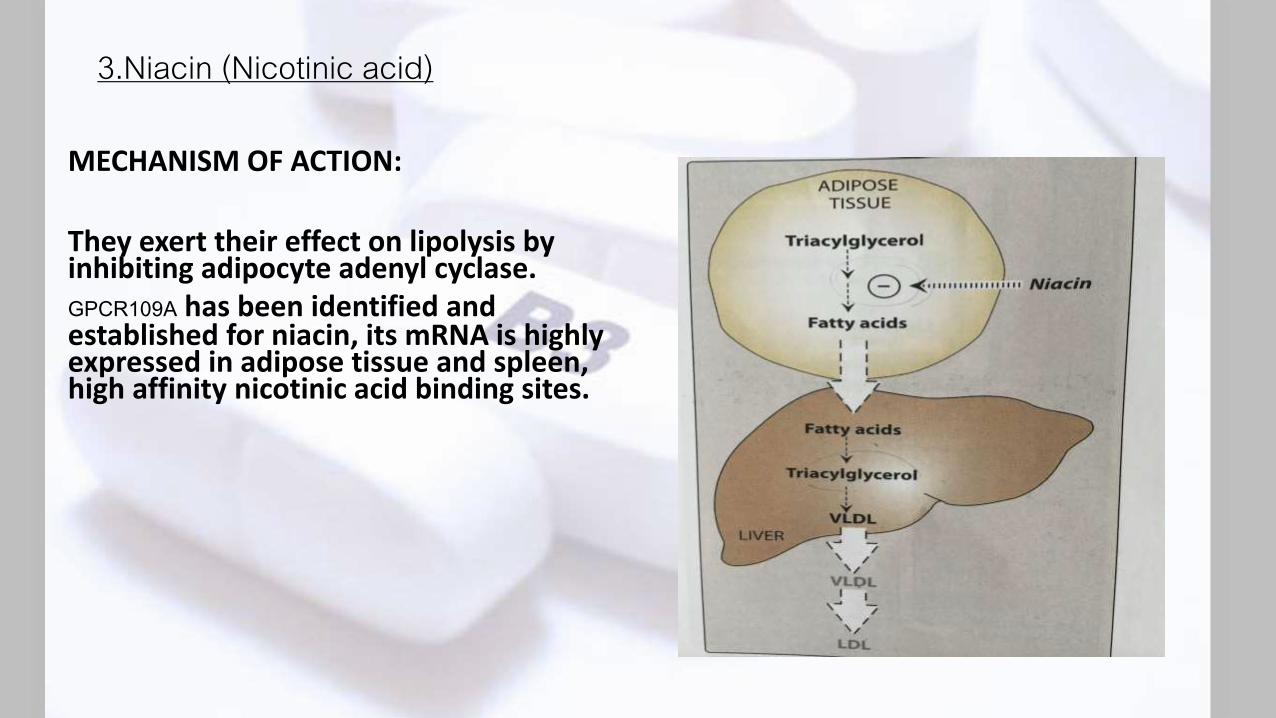
3.Niacin (Nicotinic acid)
MECHANISM OF ACTION:
They exert their effect on lipolysis by inhibiting adipocyte adenyl cyclase.GPCR109A has been identified and established for niacin, its mRNA is highly expressed in adipose tissue and spleen, high affinity nicotinic acid binding sites.
Pharmacokinetics :• Niacin is biotransformed to nicotinamide, which is incorporated
in its cofactor NAD+. These metabolites excreted in the urine.
Adverse Effects: Cutaneous Flush, Pruritus, hyperuricemia, and Gout. Impaired Glucose tolerance and hepatotoxicity are also rarely observed.
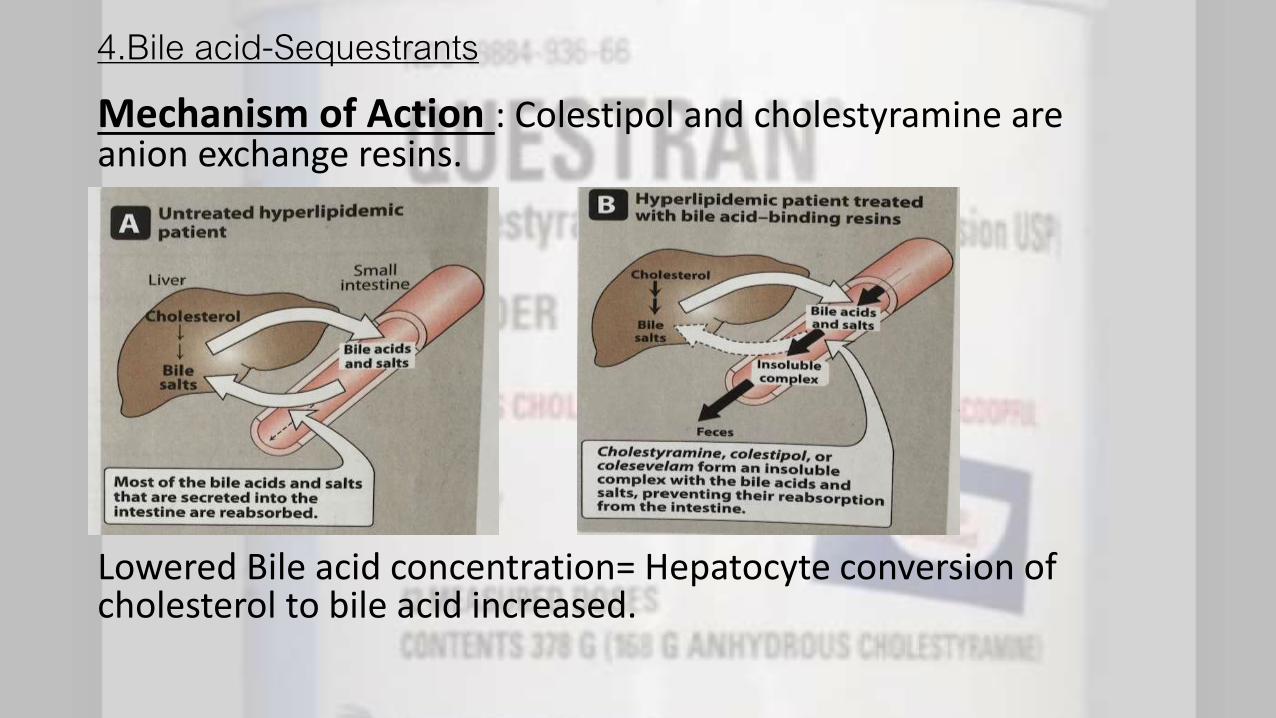
4.Bile acid-SequestrantsMechanism of Action : Colestipol and cholestyramine are anion exchange resins.
Lowered Bile acid concentration= Hepatocyte conversion of cholesterol to bile acid increased.
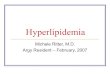
5.EZETIMIBE (Cholesterol Absorption Inhibitor)
• Selectively inhibits absorption of Dietary and biliary cholesterol in the small intestine.
• Blockade of sterol transporter on the brush border membrane of Intestinal epithelial cells.
• Thus decreases delivery of cholesterol to the liver & increases expression of LDL receptors.
• Cholesterol content of atherogenic particles also decreases.
• Niemann-Pick C1 Like 1 Protein transporter has been discovered that appears to be critical for intestinal cholesterol absorption.
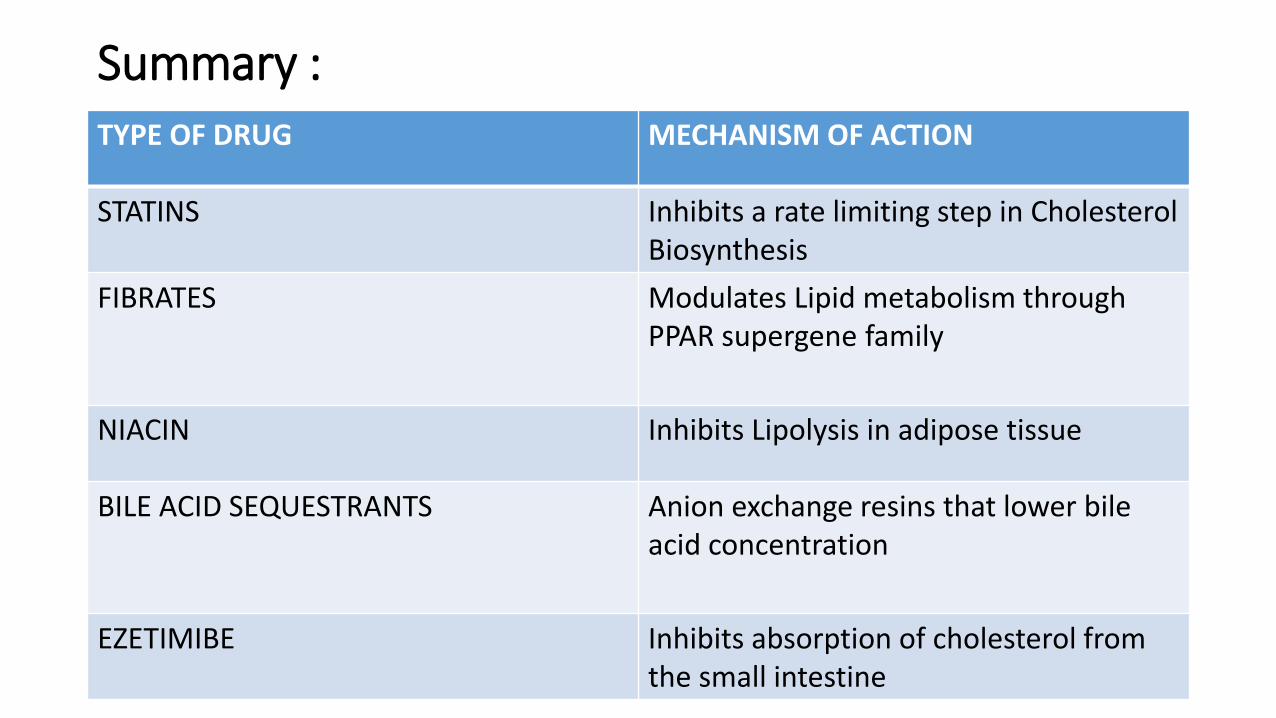
Summary :TYPE OF DRUG MECHANISM OF ACTION
STATINS Inhibits a rate limiting step in Cholesterol Biosynthesis
FIBRATES Modulates Lipid metabolism through PPAR supergene family
NIACIN Inhibits Lipolysis in adipose tissue
BILE ACID SEQUESTRANTS Anion exchange resins that lower bile acid concentration
EZETIMIBE Inhibits absorption of cholesterol from the small intestine
Study Questions:
1. Which of the following drug decreases de-novo cholesterol synthesis by inhibiting the enzyme 3-hydroxy-3-methylglutaryl coenzyme A reductase?
a)Fenofibrate
b)Niacin
c)Lovastatin
d)Gemfibrozil
2.Which one of the following drug causes decrease in liver triacylglycerol synthesis by limiting available free fatty acids needed as building blocks for this pathway?
a)Niacin
b)Fenofibrate
c)Cholestyramine
d)Gemfibrozil
3.Which of the following drugs binds bile acids in the intestine, thus preventing their return to the liver via the enterohepatic circulation?
a)Niacin
b)Fluvastatin
c)Cholestyramine
d)Lovastatin
REFERENCES:
• The NEW ENGLAND JOURNAL OF MEDICINE: http://www.nejm.org/doi/full/10.1056/nejm199506013322207
• http://science.sciencemag.org/content/193/4258/1094.short
• NCBI : Ref:http://www.ncbi.nlm.nih.gov/pubmed/10583956
• Lippincott’s illustrated Reviews
• Prevalence and treatment of hyperlipidemia in patients with chronic hepatitis C infection:
http://www.ncbi.nlm.nih.gov/pubmed/19398918
• Goodman & Gilman’s The Pharmacological Basics of Therapeutics
Thank You.
Recommended