http://www.yorku.ca/patientsafety/
Learning to Learn From Patient Safety Events
Knowledge Exchange Workshop, Nov. 2nd, 2010 gWinnipeg Regional Health Authority f
Research funded by the Canadian
Institutes of Health Research
Measuring Learning at the Patient Care
Unit Level
http://www.yorku.ca/patientsafety/
Outline
1. PSE Learning study summary
2. Can we only learn from Catastrophe?
3. Is there variation in learning from PSEs across Ontario hospitals?
4. What factors influence PSE learning?
http://www.yorku.ca/patientsafety/
1. Learning from Patient Safety EventsStudy Background
• 3-year, 2-phase study:– P1. To understand what kind of PSEs are
relevant to staff and managers in daily practice– P1. Develop PSE Learning Instrument– P2. What factors influence learning from PSEs
http://www.yorku.ca/patientsafety/
to err is human
to cover up is unforgivable
to fail to learn is inexcusable-Sir Liam Donaldson
Chief Medical Officer
UK Department of Health

http://www.yorku.ca/patientsafety/
The universe of PSEs
Identification Identify and bring PSEs to the attention of others
The universe of PSEs
Dimensions of PSE LearningRoots: theoretical models of learning from failure (Argote 1999
Analysis
Change
Properly analyze the system-level causes of PSEs
Put corrective strategies in place to reduce PSE reoccurrence; monitor change to ensure it’s sustained
Smaller num
bers of PSEs subject to each stage
of the learning process
Based on Failure-induced learning theory: Sasou, K., and J. Reason. 1999. ‘‘Team Errors: Definition and Taxonomy.’’ Reliability Engineering and System Safety, 65 (1): 1–9. Argote, L. 1999. Organizational Learning: Creating, Retaining and Transferring Knowledge. Norwell: Kluwer.
Dissem-ination
Communicate and disseminate information learned above to others on the unit / in the organization
http://www.yorku.ca/patientsafety/
Matryoshka Dolls Learning from patient safety events takes place in only a very small subset of events

http://www.yorku.ca/patientsafety/
A
1. Safety incidents
2. Recognized safety incidents
3. Recognized and discussed incidents
5. Recognized, and locally investigated
B
C
4. Recognized, discussed and reported:A – in the chartB – to a paper or on-line IR systemC – to person / team with mandate & resources to investigate and make change
Analysis
Change
Dissem
http://www.yorku.ca/patientsafety/
But we learn differently from different types of PSEs…
The following typology: Emerged from focus groups with front-line
staff and managers Describes how these front-line groups
naturally group PSEs Seen as meaningful for understanding
everyday practice
http://www.yorku.ca/patientsafety/
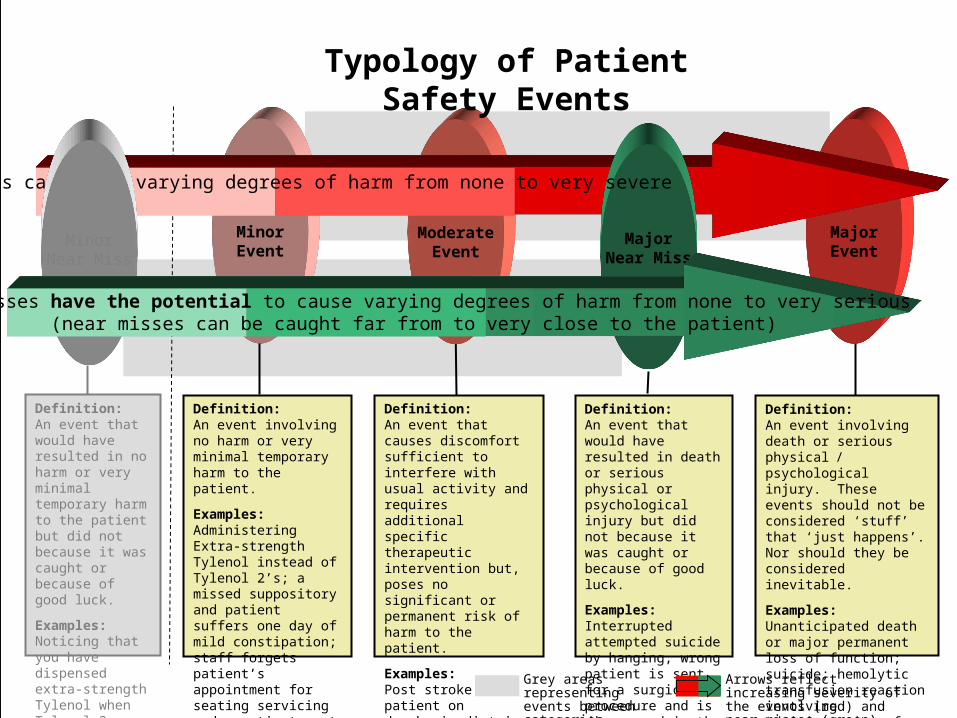
Definition:An event involving no harm or very minimal temporary harm to the patient.
Examples:Administering Extra-strength Tylenol instead of Tylenol 2’s; a missed suppository and patient suffers one day of mild constipation; staff forgets patient’s appointment for seating servicing and a patient must wait another week for a new chair
Definition:An event that causes discomfort sufficient to interfere with usual activity and requires additional specific therapeutic intervention but, poses no significant or permanent risk of harm to the patient.
Examples:Post stroke patient on dysphagic diet is given thin fluids and aspirates resulting in pneumonia, resolves with treatment
Definition:An event involving death or serious physical / psychological injury. These events should not be considered ‘stuff’ that ‘just happens’. Nor should they be considered inevitable.
Examples:Unanticipated death or major permanent loss of function; suicide; hemolytic transfusion reaction involving administration of blood; surgery on the wrong patient or wrong body part.
Definition:An event that would have resulted in death or serious physical or psychological injury but did not because it was caught or because of good luck.
Examples:Interrupted attempted suicide by hanging, wrong patient is sent for a surgical procedure and is discovered in the OR
Definition:An event that would have resulted in no harm or very minimal temporary harm to the patient but did not because it was caught or because of good luck.
Examples:Noticing that you have dispensed extra-strength Tylenol when Tylenol 2 was ordered
MajorEvent
ModerateEvent
MinorEvent
MajorNear Miss
Typology of Patient Safety Events
Events can cause varying degrees of harm from none to very severe
MinorNear Miss
Near Misses have the potential to cause varying degrees of harm from none to very serious
(near misses can be caught far from to very close to the patient)
Grey areas representing events between categories
Arrows reflect increasing severity of the events (red) and near misses (green)
http://www.yorku.ca/patientsafety/
Practically speaking…
• the goal is to grow the size of the smallest matryoshka doll
• and also recognize that we learn differently from different types of PSEs…– For minor events, the largest matryshka doll
(the universe of events) would be enormous and the smallest (Actual learning) would be tiny
http://www.yorku.ca/patientsafety/
The PSE Learning Checklist
• Concrete set of learning behaviours that can function as a checklist following different types of PSEs … that are identified

http://www.yorku.ca/patientsafety/
What learning behaviors do we engage in most often…
least often?
http://www.yorku.ca/patientsafety/
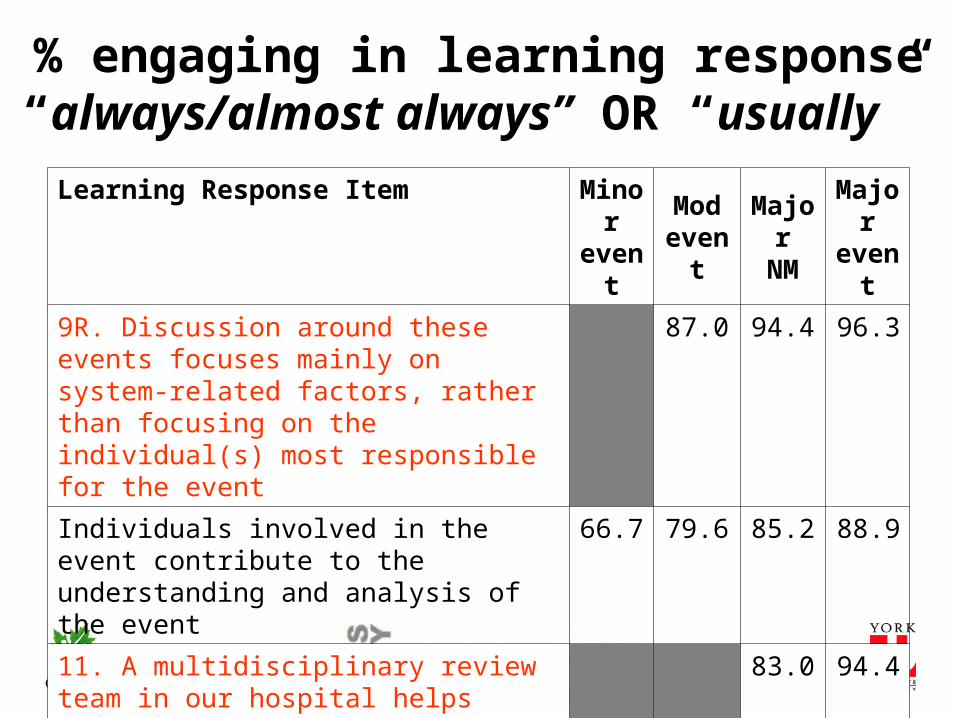
% engaging in learning response “always/almost always” OR “usually”
Learning Response Item Minorevent
Modevent
MajorNM
Majorevent
9R. Discussion around these events focuses mainly on system-related factors, rather than focusing on the individual(s) most responsible for the event
87.0 94.4 96.3
Individuals involved in the event contribute to the understanding and analysis of the event
66.7 79.6 85.2 88.9
11. A multidisciplinary review team in our hospital helps units with the analysis of these kinds of events
83.0 94.4
23. A formal process for disclosure of events to patients/families is followed and this process includes support mechanisms for patients, family, and care/service providers.
88.5
http://www.yorku.ca/patientsafety/
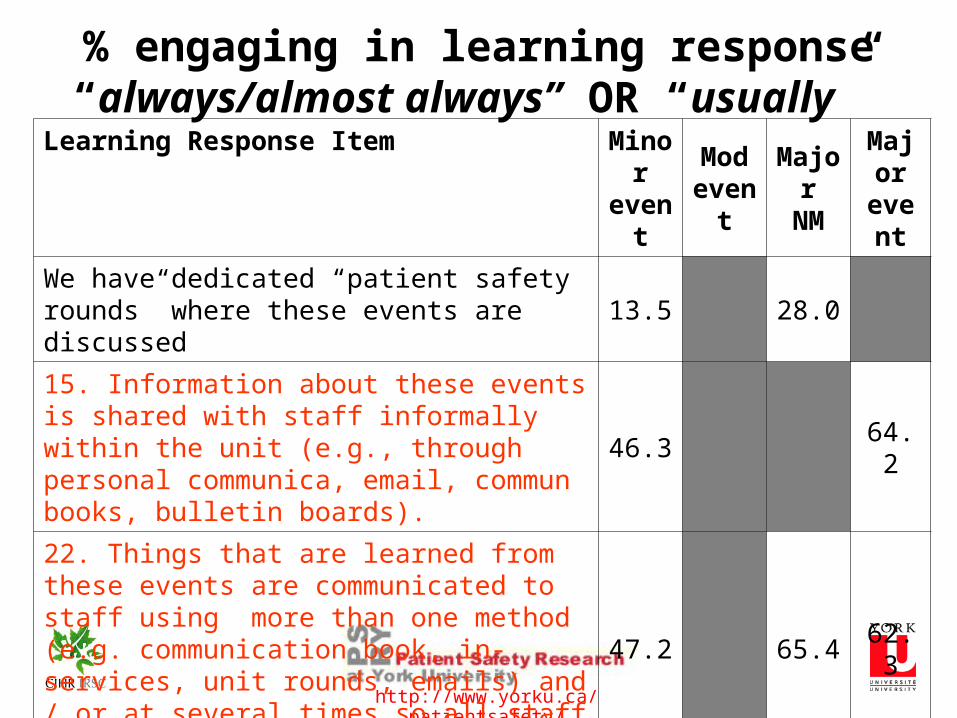
% engaging in learning response “always/almost always” OR “usually”
Learning Response Item Minorevent
Modevent
MajorNM
Majorevent
We have dedicated “patient safety rounds” where these events are discussed 13.5 28.0
15. Information about these events is shared with staff informally within the unit (e.g., through personal communica, email, commun books, bulletin boards).
46.3 64.2
22. Things that are learned from these events are communicated to staff using more than one method (e.g. communication book, in-services, unit rounds, emails) and / or at several times so all staff hear about it
47.2 65.4 62.3
17. Timely responses are provided to those who report these events (e.g., to discuss these events, possible solutions, etc.)
54
N4. The patient and fam are invited to be directly involved in the processes that follow major events (analyzing what occurred & making necessary changes)
33.3
http://www.yorku.ca/patientsafety/
Support at all Levels
- “Squeezed in the middle”- “In our experience, most boards and leaders overestimate the frontline staff’s ability to improve. In such cases, even with sufficient will and great ideas…execution stalls” (Conway, 2008) Single-loop learning – quick fixes Double-loop learning – correcting the underlying causes of a problem
http://www.yorku.ca/patientsafety/
2. Can we only learn from Catastrophe?
http://www.yorku.ca/patientsafety/
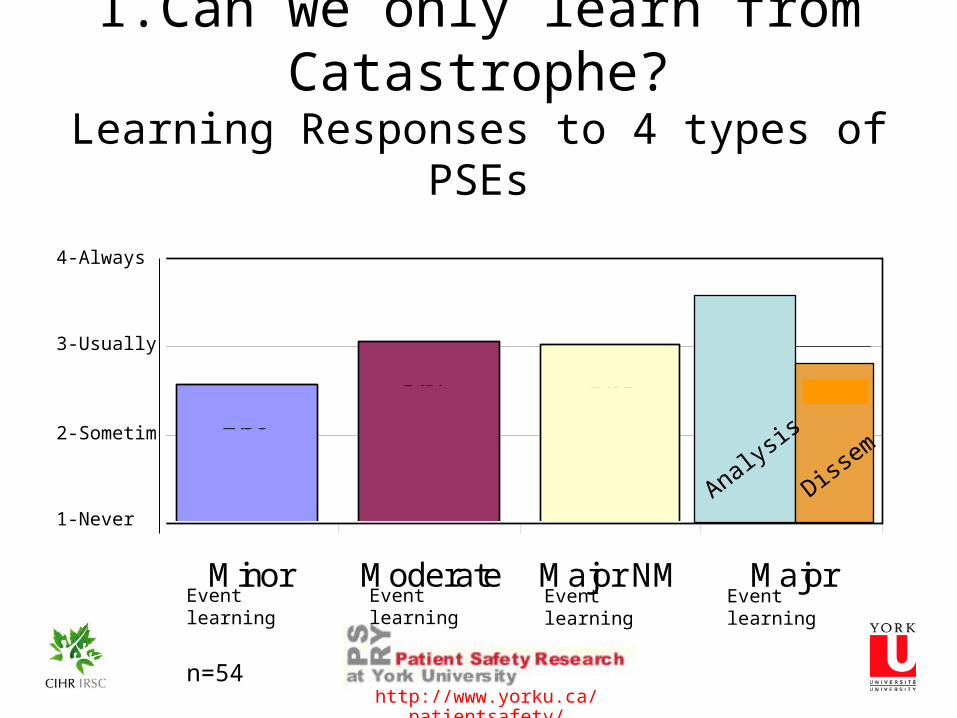
3.383.033.07
2.58
1
2
3
4
Minor Moderate Major NM Major
4-Always
3-Usually
2-Sometim
1-Never
Event learning
n=54
Event learning Event learning Event learning
1.Can we only learn from Catastrophe?Learning Responses to 4 types of PSEs
3.61
2.88
Analysis
Dissem
http://www.yorku.ca/patientsafety/
3. Is there variation in learning from PSEs across
hospitals?
http://www.yorku.ca/patientsafety/
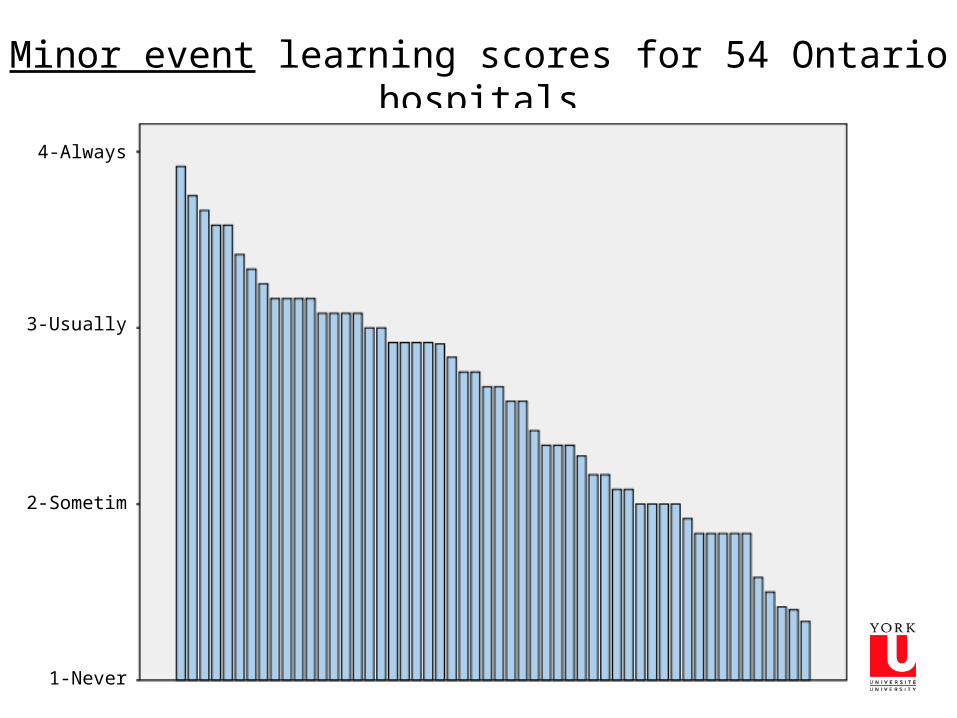
Minor event learning scores for 54 Ontario hospitals
4-Always
3-Usually
2-Sometim
1-Never
http://www.yorku.ca/patientsafety/
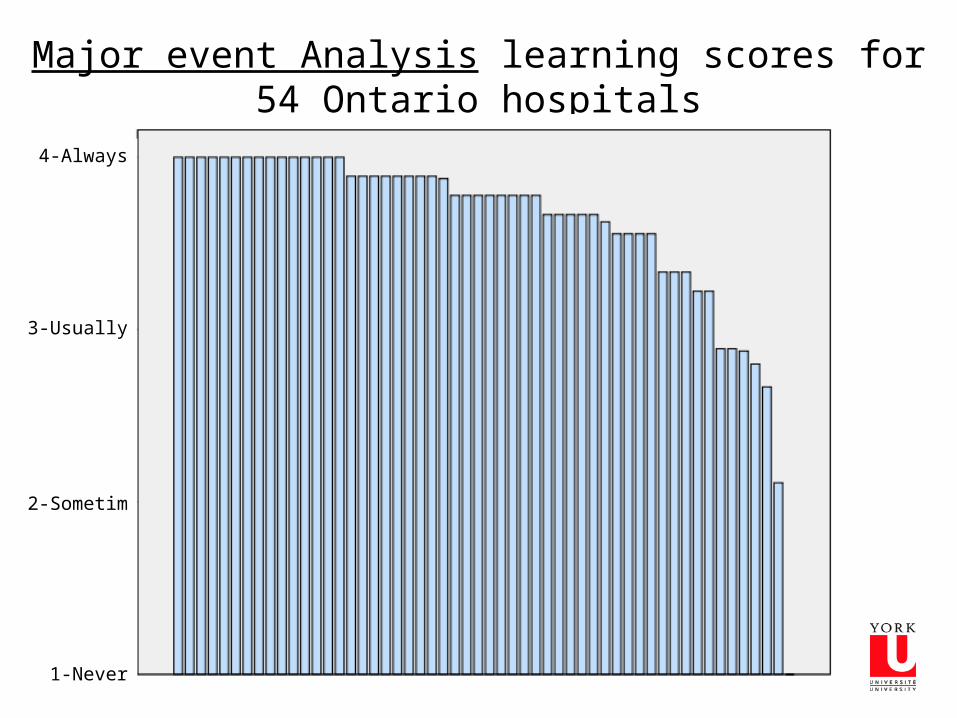
Major event Analysis learning scores for 54 Ontario hospitals
4-Always
3-Usually
2-Sometim
1-Never
http://www.yorku.ca/patientsafety/
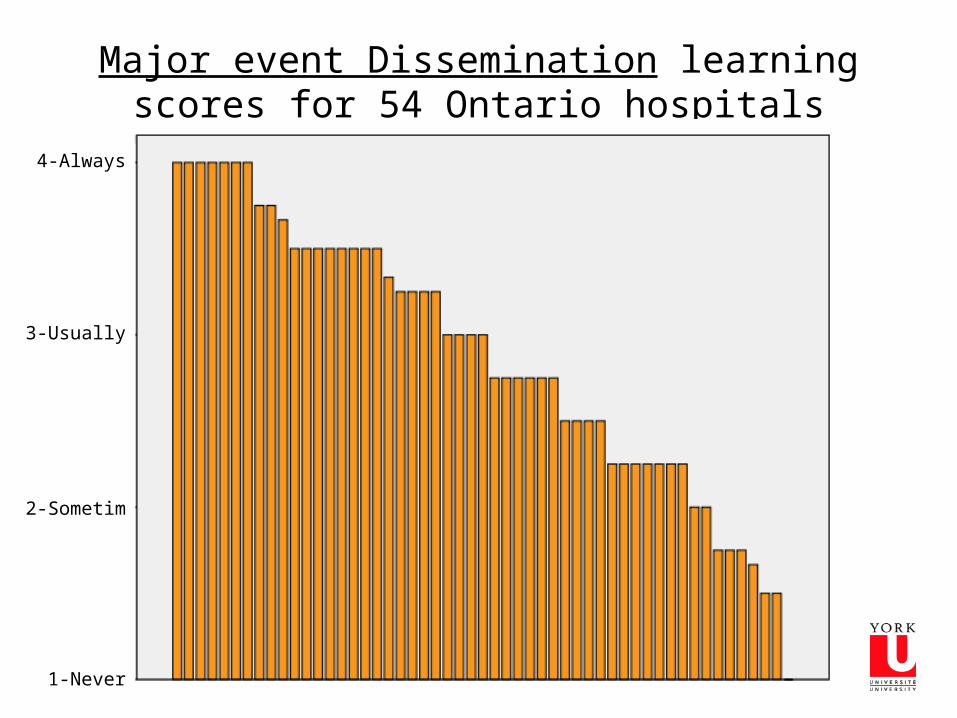
Major event Dissemination learning scores for 54 Ontario hospitals
4-Always
3-Usually
2-Sometim
1-Never

http://www.yorku.ca/patientsafety/
4. What factors influence learning from Patient
Safety Events?

http://www.yorku.ca/patientsafety/
Factors that influence learning from PSEs
• Functional diversity of the unit (invU-shape)• Type of PSEs• Manager PS training• Inter-organizational linkages• Psychological safety & fear of repercussions• Ease of reporting (+ with low fear only)• Formal organizational leadership for PS ++
http://www.yorku.ca/patientsafety/
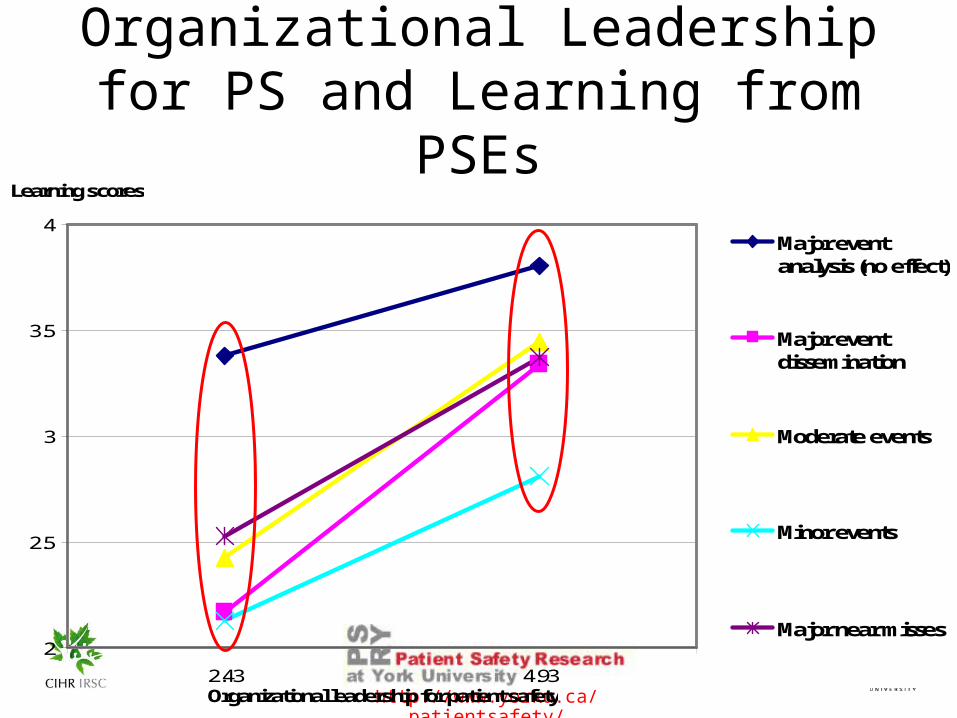
Organizational Leadership for PS and Learning from PSEs
2
2.5
3
3.5
4
2.43 4.93Organizational leadership for patient safety
Learning scores
Major eventanalysis (no effect)
Major eventdissemination
Moderate events
Minor events
Major near misses
http://www.yorku.ca/patientsafety/
So…in 3 years we found out…
• Practically speaking F-L staff and managers think in terms of straightforward, pretty clear cut event types
• There are a series of concrete learning responses that organizations and units can and should be engaging in to reduce reoccurrence of PSEs
• But the complete learning process is found only in the smallest Matryoshka doll
• We do more in response to catastrophes• But some organizations do a lot more than others• And we can identify some factors that → learning
http://www.yorku.ca/patientsafety/
… Using PSE Learning Checklist
• Comparison over time• Starting conversations
– Do the PSE learning instrument with the right people: assess current practice
– Take the results (and process?) up and down the organization: goal setting
• Getting CEOs involved through an in-depth PSE case study (Conway, 2008)
• PSE Learning instrument concrete tool to reduce the knowing-doing gap (Pfeffer & Sutton, 2000): action reduces this gap
http://www.yorku.ca/patientsafety/
ReferencesGinsburg, L., Y. Chuang, P.G. Norton, W. Berta, D. Tregunno, P. Ng, J.
Richardson. (2010). The relationship between organizational leadership for safety and learning from patient safety failure events. Health Services Research. [Epub ahead of print]
Ginsburg, L., Y. Chuang, P.G. Norton, W. Berta, D. Tregunno, P. Ng, J. Richardson. (2009) “Development of a Measure of Patient Safety Event Learning Responses”. Health Services Research. 44(6): 2123-2147..
Ginsburg, L.R., Y. Chuang, J. Richardson, P.G. Norton, W. Berta, D. Tregunno, P. Ng. Categorizing Errors and Adverse Events for Learning: The provider perspective. (2009) Healthcare Quarterly, 12:154-160.
Chuang, Y., Ginsburg, L., Berta, W. (2007). Learning from preventable adverse events in health care organizations: development of a multilevel model of learning and propositions. Health Care Management Review, 32(4).
http://www.yorku.ca/patientsafety/
Recommended

















