Endoscopic Endoscopic Mucosal Mucosal
Resection (EMR)Resection (EMR)
Clinical Professor of MedicineClinical Professor of MedicineSt. Louis UniversitySt. Louis University
Midwest Therapeutic Endoscopy ConsultantsMidwest Therapeutic Endoscopy ConsultantsSt. Louis, Missouri, USA St. Louis, Missouri, USA
Clinical Professor of MedicineClinical Professor of MedicineSt. Louis UniversitySt. Louis University
Midwest Therapeutic Endoscopy ConsultantsMidwest Therapeutic Endoscopy ConsultantsSt. Louis, Missouri, USA St. Louis, Missouri, USA
Giuseppe Aliperti, MD, Giuseppe Aliperti, MD, FACPFACP
Giuseppe Aliperti, MD, Giuseppe Aliperti, MD, FACPFACP

Endoscopic Mucosal Resection Endoscopic Mucosal Resection (EMR)(EMR)
Major advance in minimally invasive surgery Major advance in minimally invasive surgery of the GI tract based on the following of the GI tract based on the following realities:realities: Endoscopy provides visualization/access to GI Endoscopy provides visualization/access to GI
mucosa, where most cancers originatemucosa, where most cancers originate Resection/retrieval of tissue allows pathologic Resection/retrieval of tissue allows pathologic
examination (as opposed to ablation)examination (as opposed to ablation)
First perfected in Japan for resection of First perfected in Japan for resection of superficial gastric cancer, very high in that superficial gastric cancer, very high in that Country unlike the West, where colon Country unlike the West, where colon cancer (arising in polyps) is much more cancer (arising in polyps) is much more commoncommon

Most gastric cancers begin in slightly Most gastric cancers begin in slightly elevated, flat, or slightly depressed mucosal elevated, flat, or slightly depressed mucosal dysplastic lesions, difficult to grasp with a dysplastic lesions, difficult to grasp with a simple wire snare.simple wire snare.
Most mucosal polyps, by projecting into the Most mucosal polyps, by projecting into the lumen, are easy to grasp with wire snares at lumen, are easy to grasp with wire snares at the polyp base for resection with the polyp base for resection with electrocauteryelectrocautery
Endoscopic Mucosal Resection Endoscopic Mucosal Resection (EMR)(EMR)

Japanese endoscopists have adapted and Japanese endoscopists have adapted and perfected methods to raise the neoplastic perfected methods to raise the neoplastic mucosal area in order to allow snaring or mucosal area in order to allow snaring or dissection with sharp-tipped instrumentsdissection with sharp-tipped instruments
Most use fluid injection into the Most use fluid injection into the submucosal layer to elevate the mucosa submucosal layer to elevate the mucosa and allow it to be grasped with the snareand allow it to be grasped with the snare
Some use specially fitted scope caps that Some use specially fitted scope caps that lift the lesion by suctionlift the lesion by suction
Endoscopic Mucosal Resection Endoscopic Mucosal Resection (EMR)(EMR)

The success of EMR in the stomach The success of EMR in the stomach prompted endoscopists to expand the prompted endoscopists to expand the method to the:method to the: EsophagusEsophagus, where early cancer and , where early cancer and
premalignant dysplasia also tends to be non-premalignant dysplasia also tends to be non-polypoid and flatpolypoid and flat
ColonColon, where some neoplastic lesions are flat , where some neoplastic lesions are flat or sessile or sessile
DuodenumDuodenum Major papillaMajor papilla
Endoscopic Mucosal Resection Endoscopic Mucosal Resection (EMR)(EMR)

EMR: techniquesEMR: techniques
Special caps designed to fit the tip Special caps designed to fit the tip of the endoscope allow of the endoscope allow endoscopic suction to lift the endoscopic suction to lift the mucosa to be ensnared mucosa to be ensnared
Removal of large lesions in 1 piece Removal of large lesions in 1 piece ((en blocen bloc) is achieved with ) is achieved with electrocautery wire-knives of electrocautery wire-knives of different shapes that dissect different shapes that dissect around and under the diseased around and under the diseased mucosamucosa

High-Grade Dysplasia (HGD), High-Grade Dysplasia (HGD), Superficial Cancer in Barrett's Superficial Cancer in Barrett's
EsophagusEsophagus Incresed detection rates with Incresed detection rates with
screening/surveillancescreening/surveillance Difficult area in clinical decision making – HGD Difficult area in clinical decision making – HGD
difficult to distinguish histologically from difficult to distinguish histologically from invasive adenocarcinoma intra-(T1m) or sub-invasive adenocarcinoma intra-(T1m) or sub-mucosal (T1sm)mucosal (T1sm)
In specimens of esophagectomy for HGD >30% In specimens of esophagectomy for HGD >30% harbor invasive cancerharbor invasive cancer
Esophagectomy has a high morbidity/mortality Esophagectomy has a high morbidity/mortality (2-7% in expert centers, 20% in others – (2-7% in expert centers, 20% in others – age/comorbidities in older patients where HGD is age/comorbidities in older patients where HGD is more frequent)more frequent)

Endoscopic Ablative Endoscopic Ablative Therapies (non-resective) Therapies (non-resective)
methods based on rates of lymph node metastasis: methods based on rates of lymph node metastasis: absent in HGD, very low in confined invasive cancers absent in HGD, very low in confined invasive cancers 1-2-31-2-3
photodynamic therapyphotodynamic therapyargon plasma coagulationargon plasma coagulation
Both successfulBoth successful4-54-5, but cannot assure:, but cannot assure:Confinement to the mucosa – Confinement to the mucosa – T1m vs. T1smT1m vs. T1smRemoval of the entire lesion - Removal of the entire lesion - there is there is nono
specimenspecimen
EUS accuracy, excellent for invasion beyond EUS accuracy, excellent for invasion beyond submucosa and lymph node detection - is only 75-submucosa and lymph node detection - is only 75-85% in distinguishing between mucosal [T1m] and 85% in distinguishing between mucosal [T1m] and submucosal [T1sm] diseasesubmucosal [T1sm] disease

EMR for Staging in Barrett's EMR for Staging in Barrett's Esophagus:Esophagus:
General ConceptsGeneral Concepts
EMR allows removal of large pathology EMR allows removal of large pathology specimens extending into the mid-specimens extending into the mid-submucosa, a big staging advantage over submucosa, a big staging advantage over ablative methods ablative methods 66
Depth of cancer invasion can be made Depth of cancer invasion can be made with great accuracywith great accuracy
Disease confined to mucosa with clear Disease confined to mucosa with clear margins is considered curedmargins is considered cured
Patients with submucosal invasion (T1sm) Patients with submucosal invasion (T1sm) are usually referred for surgery/chemoare usually referred for surgery/chemo
Ell et al Gastroenterol 2000;118:670-677

EMR performed to stage patients with HGD/T1m EMR performed to stage patients with HGD/T1m (confined to mucosa) CA by EUS (confined to mucosa) CA by EUS 77
48 pts, 8 to surgery for submucosal (T1sm) 48 pts, 8 to surgery for submucosal (T1sm) disease by EUS: 7/8 T1sm, one T1m, overstageddisease by EUS: 7/8 T1sm, one T1m, overstaged
40 with T1m by EUS: 25 had HGD, 15 had 40 with T1m by EUS: 25 had HGD, 15 had adenoCA - All underwent EMR for definitive adenoCA - All underwent EMR for definitive staging (no complications)staging (no complications)
EMR changed the staging in 30%:EMR changed the staging in 30%: 19/25 with apparent HGD by EUS were T1m1, 19/25 with apparent HGD by EUS were T1m1,
4/25 T1m2, 2/25 T1m34/25 T1m2, 2/25 T1m3 6/15 with T1m CA were T1sm (submucosal 6/15 with T1m CA were T1sm (submucosal
invasion) instead and were sent to surgeryinvasion) instead and were sent to surgeryadditional therapy required for residual/recurrent additional therapy required for residual/recurrent
HGD, CAHGD, CA
EMR for Staging in Barrett's EMR for Staging in Barrett's EsophagusEsophagus
Lightdale et al Gastrointest Endosc. 2004;59:AB90

Post-EMR Endoscopic Post-EMR Endoscopic SurveillanceSurveillance
240 EMR 1996-2003 240 EMR 1996-2003 88
accurate assessment of invasion depthaccurate assessment of invasion depthneoplastic lesions neoplastic lesions notnot resected completely resected completely
in most, required additional biopsies and f-uin most, required additional biopsies and f-u
72 EMR compared with 66 surgery for T1m/T1sm 72 EMR compared with 66 surgery for T1m/T1sm CA EMR patients older, smaller tumors, less LN CA EMR patients older, smaller tumors, less LN mets mets 99
EMR: fewer complications, shorter hospital EMR: fewer complications, shorter hospital staystay
EMR: higher risk of tumor recurrence.EMR: higher risk of tumor recurrence.
Lewis et al, Mayo, GIE 2004;59:AB101Bhave et al, MGH/UCH,MGH/UCH, GIE 2004;59:AB254

Post-EMR Endoscopic Post-EMR Endoscopic SurveillanceSurveillance
79 patients, 38 with HGD/T1m CA 79 patients, 38 with HGD/T1m CA 1010
EMR alone satisfactory in 60% pts; T1sm EMR alone satisfactory in 60% pts; T1sm invasion in 18% required surgery/chemoinvasion in 18% required surgery/chemo
Complete resection, clear margins not Complete resection, clear margins not always possiblealways possible
EMR in 38 pts with HGD/T1m EMR in 38 pts with HGD/T1m 1111
changed pretreatment diagnosis in 10 changed pretreatment diagnosis in 10 (26%)(26%)
negligible complicationsnegligible complications careful endoscopic surveillance was careful endoscopic surveillance was
recommendedrecommendedPonchon et al, France, GIE 2004;59:AB255 Conio et al, Italy, GIE 2004;59:AB253

EMR performed for focal lesions or for EMR performed for focal lesions or for complete removal of short-segment complete removal of short-segment Barrett'sBarrett's
EMR good for superficial cancer EMR good for superficial cancer treatment, low complicationstreatment, low complications
Impossible to determine clear margins in Impossible to determine clear margins in piecemeal resectionspiecemeal resections
After EMR, careful follow-up is required After EMR, careful follow-up is required for residual or metachronous diseasefor residual or metachronous disease
EMR for Barrett's Esophagus: EMR for Barrett's Esophagus: ConclusionsConclusions

Circumferential EMR in Circumferential EMR in Barrett's EsophagusBarrett's Esophagus
All Barrett's tissue removed with special stiff All Barrett's tissue removed with special stiff monofilament snare in 22 patients with monofilament snare in 22 patients with HGD/IMCA HGD/IMCA 1212
Tissue removed piecemeal, median length 3cm Tissue removed piecemeal, median length 3cm (1.2-10)(1.2-10)
Four had residual Barrett's epithelium (1 Four had residual Barrett's epithelium (1 beneath new squamous epithelium), 6 beneath new squamous epithelium), 6 developed strictures responding to dilationdeveloped strictures responding to dilation
Circumferential piecemeal EMR with modified Circumferential piecemeal EMR with modified multiple variceal band ligator, then multiple snare multiple variceal band ligator, then multiple snare resections without removing scope in between resections without removing scope in between 1313
greater efficiency then cap-assisted EMR for greater efficiency then cap-assisted EMR for larger resectionslarger resections
Seewald et al, Germany, GIE 2004;59:AB101 Soehendra, Germany, DDW 2004

EMR Combined With Ablation EMR Combined With Ablation TherapyTherapy
Used to treat residual neoplastic tissue after EMR Used to treat residual neoplastic tissue after EMR Photodynamic therapy (PDT) with laser after light-Photodynamic therapy (PDT) with laser after light-
sensitizing drugs successful method of ablation sensitizing drugs successful method of ablation after EMR after EMR 1414
Combination of EMR and PDT Combination of EMR and PDT 1515
local remission in 26/28 pts, mean f-u 15.2 molocal remission in 26/28 pts, mean f-u 15.2 mo local recurrence common, further treated with local recurrence common, further treated with
EMREMR++PDTPDTCombination of EMR and PDT Combination of EMR and PDT 1616
local remission in 18 of 22 pts over 10.6 local remission in 18 of 22 pts over 10.6 monthsmonths
no complicationsno complicationsPacifico et al, Clin Gastr Hepatol. 2003;1:252-257Peters et al, The Netherlands GIE 2004;59:AB251Haringsma et al, The Netherlands GIE 2004;59:AB252

EMR Combined With Ablation EMR Combined With Ablation TherapyTherapy
Combination EMR/PDT for focal neoplastic Combination EMR/PDT for focal neoplastic lesions followed with thermal ablation by APC lesions followed with thermal ablation by APC 1717 Complete eradication of all of the Barrett's Complete eradication of all of the Barrett's
and all neoplastic tissue was achieved in and all neoplastic tissue was achieved in 85/88 patients, mean f-u 30 months; 2 85/88 patients, mean f-u 30 months; 2 patients died of progressive diseasepatients died of progressive disease
Complications included 1 bleed after EMR, Complications included 1 bleed after EMR, 20 symptomatic strictures, 10 "sunburns," 2 20 symptomatic strictures, 10 "sunburns," 2 episodes of atrial fibrillation after PDTepisodes of atrial fibrillation after PDT
Rahmani et al (IU) GIE 2004;59:AB250

EMR for Other Esophageal EMR for Other Esophageal TumorsTumors
EMR for SCCA of esophagus is widely used in EMR for SCCA of esophagus is widely used in Japan, less in the West, where early detection Japan, less in the West, where early detection is uncommon. is uncommon.
EMR on 39 pts with early SCCA EMR on 39 pts with early SCCA 1818
10 pts CA in situ, 19 T1m, 10 T1sm 10 pts CA in situ, 19 T1m, 10 T1sm (inoperable)(inoperable)
9/10 with CA in situ, 19/19 patients with T1m 9/10 with CA in situ, 19/19 patients with T1m with complete remission at mean f-u 29.7 mowith complete remission at mean f-u 29.7 mo
3 minor bleeding, 3 mild strictures3 minor bleeding, 3 mild stricturesEMR (band ligation then snare) for submucosal EMR (band ligation then snare) for submucosal
benign tumors <3cm benign tumors <3cm 1919
17 pts: 11 granular cell tumors, 3 17 pts: 11 granular cell tumors, 3 leiomyomas, 1 lipoma, 2 stromal leiomyomas, 1 lipoma, 2 stromal
7 bleeding, no transfusions (1 to surgery for 7 bleeding, no transfusions (1 to surgery for residual)residual) Pech et al, Germany GIE 2004;59:AB256
Wehrmann et al, Germany GIE 2004;59:AB241

Variation of EMR in which large resections are Variation of EMR in which large resections are performed for accurate determination of margins performed for accurate determination of margins and depthand depth
Hyaluronic acid is injected to maintain long-lasting Hyaluronic acid is injected to maintain long-lasting submucosal elevationsubmucosal elevation
Dissection is performed with different shape Dissection is performed with different shape devices through the endoscope operating channeldevices through the endoscope operating channel
Experts are Dr. Haruhiro InoueExperts are Dr. Haruhiro Inoue20 20 who uses a who uses a triangle-tipped knife Dr. Hiroyuki Onotriangle-tipped knife Dr. Hiroyuki Ono21 21 who uses an who uses an insulated-tip knifeinsulated-tip knife
Dissections are lengthy, sometimes taking hours, Dissections are lengthy, sometimes taking hours, and have significant perforation rates of 5-10%, and have significant perforation rates of 5-10%, most are managed endoscopically with clipsmost are managed endoscopically with clips
Endoscopic Endoscopic SubSub--mucosal mucosal DissectionDissection
Inoue, Japan, DDW 2004Ono, Japan, DDW 2004

Adjustable thin-wire snare or a flex-Adjustable thin-wire snare or a flex-knife knife 2222
9 pts with GE-junction, cardia tumors9 pts with GE-junction, cardia tumors mean lesion size 20.8 mm, mean mean lesion size 20.8 mm, mean
specimen size 35.2 mmspecimen size 35.2 mm no significant bleeding, 1 stricture no significant bleeding, 1 stricture
responding to dilationresponding to dilation 1 pt with submucosal invasion, all others 1 pt with submucosal invasion, all others
without recurrence at mean f-u 8 mo.without recurrence at mean f-u 8 mo.
Endoscopic Endoscopic SubSub--mucosal mucosal DissectionDissection
Yahagi et al, Japan, GIE 2004;59:AB171

Hook knife in left-sided colonic lesions Hook knife in left-sided colonic lesions 2323
14 pts. mean diameter of 32.7 mm. 14 pts. mean diameter of 32.7 mm. En blocEn bloc resection in 10/14 (71%) ptsresection in 10/14 (71%) pts
1 microperforation with a 60mm flat rectal 1 microperforation with a 60mm flat rectal adenoma, managed with endoscopic clips adenoma, managed with endoscopic clips and antibioticsand antibiotics
Endoscopic Endoscopic SubSub--mucosal mucosal DissectionDissection
Hotta et al, Japan GIE 2004;59:AB273

Removal of adenomas of the major papilla 2424
Patients underwent biopsy, snare polypectomy, dual sphincterotomy with dual stent placement
Nd:YAG laser ablation or Argon Plasma Coagulation were used if the resection was felt to be incomplete
Endoscopy repeated at 4 to 8 weeks for stent exchange/removal with further ablation/biopsies until complete resection accomplished
Patients then followed with endoscopy/biopsies every 6 months and, if negative for recurrence, yearly
Ampullectomy: ProtocolAmpullectomy: Protocol
Husain, Sawhney, Aliperti GIE 2001;53(5):3402

Ampullectomy: ResultsAmpullectomy: Results
Twelve pts 72 + 2.3 y (r 59-83) with jaundice/abnormal LFTs (58.2%), biliary colic (16.6%), Fe-def. anemia (16.6%)
Lesions between 2 and 5 cm (mean 2.5 cm) and normal cholangiography, except for dilatation
Median of 3 endoscopic sessions (range 2-4 ) for complete adenoma ablation
50 % required Nd:YAG laser or APC
Husain, Sawhney, Aliperti GIE 2001;53(5):3402

Ampullectomy: ResultsAmpullectomy: Results
At 40 mo (r 6-84 mo) recurrent adenomas in 6 (50%). Two with foci of adenoCA had Whipple; 4 had repeat endoscopic resection; disease free at 12, 21, 48 and 84 mo
Six (50%) patients had no disease recurrence. Two died of unrelated causes at 33 and 48 mo. The other four remain disease-free at 6, 22, 37 and 48 mo
On multivariate analysis: age, size, use of laser/APC not different between pts with and without recurrence
One pt developed cholangitis following stent occlusion and was successfully treated with antibiotics and stent exchange
No other endoscopy-related complications
Husain, Sawhney, Aliperti GIE 2001;53(5):3402

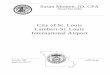
During healing, after stent removal
After mucosectomy,during laser ablation
Duodenal wall extensionAdenoma before resection
#2762
Ampullectomy: Ampullectomy: ConclusionsConclusions
For patients with ampullary adenomas who are poor surgical candidates or refuse surgery:
Endoscopic resection with periodic surveillance is a safe and effective alternative
After endoscopic resection, age, size of adenoma and use of thermal therapy are not reliable predictors of recurrence

EMR of Choledochal CystEMR of Choledochal Cyst
Not reported, so far…Not reported, so far… Three cases, presenting with intermittant Three cases, presenting with intermittant
biliary obstruction (pain, LFTs)biliary obstruction (pain, LFTs) Complete resection, no complicationsComplete resection, no complications
Aliperti, Unpublished

ConclusionsConclusions
EMR is now firmly established as an important EMR is now firmly established as an important minimally invasive therapy for the treatment of minimally invasive therapy for the treatment of mucosal cancer and premalignant lesions of mucosal cancer and premalignant lesions of the gastrointestinal tract. the gastrointestinal tract.
The techniques for EMR are still in evolution. The techniques for EMR are still in evolution. However, current methods involving However, current methods involving submucosal fluid injection followed by submucosal fluid injection followed by electrocautery excision, or cap-assisted EMR electrocautery excision, or cap-assisted EMR using endoscopic suction to achieve mucosal using endoscopic suction to achieve mucosal lifting, have been highly safe and effective. lifting, have been highly safe and effective.
Endoscopic submucosal dissection allows large Endoscopic submucosal dissection allows large en blocen bloc resections of larger superficial tumors, resections of larger superficial tumors, and this method has been proven safe and and this method has been proven safe and effective in effective in expertexpert hands. hands.
Recommended