British Journal of Industrial Medicine 1992;49:545-555
Effects ofoccupational exposure to mercury vapour onthe central nervous system
S Langworth, 0 Almkvist, E Soderman, B-0 Wikstrom
AbstractPossible effects of mercury on the centralnervous system (CNS) were examined in agroup of chloralkali workers exposed to mer-cury (n = 89) and compared with a controlgroup (n = 75), by registration of subjectivesymptoms, personality changes, forearmtremor, and performance on six computerisedpsychometric tests in the two groups. Thegroups were similar in age, education, verbalcomprehension, and work tasks. In thechloralkali group, median blood mercury con-centration (B-Hg) was 55 nmol/l, serum mer-cury concentration (S-Hg) 45 nmol/l, and urinemercury concentration (U-Hg) 14-3 nmol/mmol creatinine (25-4 pg/g creatinine). Corre-sponding concentrations in the control groupwere 15 nmol/l, 4 nmol/l, and 1P1 nmol/mmolcreatinine (19 pg/g creatinine) respectively.The number of self reported symptoms, thescores for tiredness and confusion in the profileof mood states (POMS), and the degree ofneuroticism in the Eysenck personality inven-tory (EPI), were significantly higher in themercury exposed group compared with thecontrols. Performance on the psychometrictests and tremor frequency spectra did notdiffer significantly between the two groups.Dose-response calculations showed weak butstatistically significant relations betweensymptom prevalence and current mercuryconcentrations in both blood and urine. Theperformance on three of the psychometrictests was negatively correlated with earlierpeak exposures. The findings indicate a slightmercury induced effect on the CNS among thechloralkali workers.
Department of Occupational Medicine, HuddingeHospital, S-141 86 Huddinge, SwedenS Langworth, E SodermanDepartment of Geriatric Medicine, HuddingeHospital, S-141 86 Huddinge, Sweden0 AlmkvistDivision of Technical Work Physiology, NationalInstitute of Occupational Health, S-171 84 Solna,SwedenB-O Wikstrom
The central nervous system (CNS) is the criticalorgan for exposure to mercury (Hg) vapour' andoccupational exposure exceeding 100 Mg Hg/m3 airmay cause clinical symptoms such as fatigue, anxiety,shyness, insomnia, loss of appetite, weight loss, andtremor." Studies of workers with low exposure haveshown both increased frequency of symptoms anddisturbances in various psychological tests related tothe degree ofexposure to mercury.' The studies are,however, difficult to compare, because of discrepan-cies in study design (for example, selection ofexposure indicators, test types, etc). Thus a safethreshold, below which effects on the CNS can beexcluded, has not yet been established. In 1980, theWorld Health Organisation Study Group recom-mended an exposure limit of 25 Mg Hg/m' air (timeweighted average, TWA) for long term occupationalexposure to mercury vapour, and a biologicalthreshold concentration of 50 jg Hg/g creatinine inurine.'
In Sweden, the exposure limit (TWA) for mercuryvapour is 50 jg Hg/m' air. The average exposure inthe Swedish chloralkali industry has decreased con-siderably during the past decades7 and is today about25 jg Hg/m' air. Cases of chronic mercury poisoningare rare. Despite this, there has been debate concern-ing possible effects on the CNS of long term, lowexposure to inorganic mercury, and the exposurelimit (50 pg/m') has been questioned. The purpose ofthe present study was to examine health effects oflong term, low level exposure to mercury vapour. Wedescribe a survey of possible effects on the CNS ofmercury exposure among Swedish chloralkaliworkers, examined by registration of subjective sym-ptoms, personality changes, forearm tremor, andperformance on psychometric tests. Renal andimmunological effects of the workers' exposure tomercury were described in an earlier publication.8
Material and methodsSUBJECTSA group of96 chloralkali workers exposed to mercuryand from five plants located in three different geogra-phic regions in Sweden (the west coast, the centralregion, and the east coast) and a control group of 80industrial workers from two chemical industries,from a paper factory, and from a saw mill located in
545
on March 11, 2020 by guest. P
rotected by copyright.http://oem
.bmj.com
/B
r J Ind Med: first published as 10.1136/oem
.49.8.545 on 1 August 1992. D
ownloaded from

Langworth, Almkvist, Sdderman, Wikstrom
the same regions were requested to participate in thestudy on a voluntary basis.As the major objective of the study was to detect
possible health effects of exposure to mercury,chloralkali workers with repeatedly raised bloodmercury concentrations (>75 nmol/l) on routinetests during the past three years were selectedtogether with workers judged to have high currentexposure to mercury. Only workers with a minimumof one year of employment at the plants were
included. Workers from nearby industries as similaras possible in age, educational level, and type ofworkwere selected as controls. Criteria for exclusion fromthe study were exposure to other heavy metals (forexample, lead, cadmium, manganese) or organicsolvents, chronic neurological or renal disease, andexcessive alcohol intake. Selection and rejection ofsubjects were based on the judgement of the com-
pany physicians and one of us (SL).Due to sick leave that was not related to exposure
to mercury (four cases) and to unwillingness toparticipate (three cases), the final mercury exposedgroup included 89 workers. Their duration ofexposure varied from one to 45 years (mean 13 5 (SD8-7) years). Because of sick leave (two cases),unwillingness to participate (two cases), and suspec-ted previous exposure to mercury (one case), the finalcontrol group numbered 75 workers. There were 25shift workers in the mercury exposed group and 27 inthe control group. Table 1 presents the data concern-ing the workers age, education, verbal comprehen-sion, alcohol consumption, and smoking.
STUDY DESIGN AND METHODSA cross sectional study was performed during theperiod 1985-6. All examinations were carried out atthe factories during ordinary work days. About eightpersons were examined each day. All subjects under-went a clinical examination by a physician (SL),including an interview that focused on history ofexposure, previous health state, and currentsymptoms.
Special attention was paid to previous neurologicaldiseases including concussion of the brain. Data on
smoking (smoker or non-smoker), alcohol intake(average weekly intake of beer, wine, and spirits) and
fish consumption (number of meals per week andtype of fish) were registered by means of a question-naire and then checked at the interview. The currentuse of medicines was also registered. Odontologicalstate was recorded by a dentist. The total number ofamalgam fillings and the number of amalgam sur-
faces (each tooth was taken to constitute zero to fivesurfaces covered with amalgam) were registered. Theclinical examination also included collection of ven-ous blood samples for mercury analyses.
Immediately after clinical examination thesubjects were instructed to complete questionnairesconcerning subjective symptoms, mood state, andpersonality. A test of verbal comprehension (synon-yms) was included to assess the premorbidintelligence of the workers.9 This was followed byregistration of forearm tremor, and finally a com-
puter administered psychometric test in the presenceof a psychologist (OA).
REGISTRATION OF SYMPTOMS, MOOD STATE, ANDPERSONALITYAs well as the interview, three self administeredquestionnaires: (1) questionnaire 16 (Q16), (2) profileof mood state (POMS), and (3) Eysenck personalityinventory (EPI), were used to survey the prevalenceof subjective symptoms, current mood state, andpersonality changes. Questionnaire Q16 is a symp-
tom questionnaire developed as a screening ins-trument for symptoms among workers exposed tosolvents; it has been used in many epidemiologicalstudies.'" A higher proportion of positive answers inQ16 has been related to decreased psychometric testperformance in groups exposed to lead" and organicsolvents.'0 12
The mood state questionnaire was based on theprofile of mood states described by McNair et al,3and was adapted from a computer administeredmood questionnaire.'4 The 25 items were translatedinto Swedish by one of us (OA), and were used to
measure the degree of tiredness, depression, anger,
tension, and confusion.The Eysenck personality inventory was used to
evaluate the grade ofneuroticism and extroversion orintroversion.'5 This questionnaire is widely used, andhas been validated on groups exposed to mercury
vapour.'6
Table 1 Background characteristics of the mercury exposed and control workers
Exposed (n= 89) Controls (n = 75)
Median Range Median Range
Age (y) 42 22- 64 43 21-64Education (y) 8 4- 13 8 6-14Synonyms (score) 21 1- 29 19 0-28Alcohol (cl/week) 10 0-100 10 0-75Fish (meals/week) 1 0- 3 1 0- 3Amalgam (surfaces) 21 0- 46 28 0-54Smoking (frequency) 44% 40%
546
on March 11, 2020 by guest. P
rotected by copyright.http://oem
.bmj.com
/B
r J Ind Med: first published as 10.1136/oem
.49.8.545 on 1 August 1992. D
ownloaded from

Effects of occupational exposure to mercury vapour on the central nervous system
PSYCHOMETRIC TEST BATTERYPsychomotor performance, attention, and short termmemory were tested using six computerised tests,which were selected and adapted from the neurobe-havioural evaluation system.4 17A personal computerequipped with a joystick and a special button panelwas used. All test sessions were performed in a quietroom under guidance of the same test leader (OA).The test conditions were standardised as much aspossible. Exposed subjects and controls were testedin a randomised order, and could not be identified bythe test leader. In all tests the first trial was a practicerun. The six tests are:
(1) Hand-eye coordination (HEC) -This is a visualmotor coordination test executed with a joystick. Thetask was to move a cursor as close as possible to acurved line on the screen. The average deviationfrom the line (mean absolute error based on a graphicmeasure) during five tests was used as test parameter.
(2) Finger tapping-Motor speed function wastested by finger tapping with (a) dominant hand, (b)non-dominant hand, and (c) alternating hands. Thesubjects were instructed to tap a button with theindex finger as fast as possible for 10 seconds. Theaverage number of taps during five trials for eachcondition was used as test parameter.
(3) Simple reaction time-In this attention test thesubjects were required to press a button with theindex finger of the preferred hand as quickly aspossible when a symbol (a large "0") appeared on thedisplay. Twelve stimuli were presented per minutewith randomised time intervals between 2-5 and fiveseconds. The average reaction time (ms) and stan-dard deviation (SD) during six minutes were cal-culated and used as test parameters.
(4) Symbol-digit-In this test of perceptual speedthe task was to combine symbols with correspondingdigits presented in random order in a row. The key tothis coding was given by a row with paired symbolsand digits from one to nine. Each trial consisted ofnine pairs of symbols and digits and a total of fivetrials were presented. The average answering time (s)was used as test parameter.
(5) Digit span-This is a traditional test of shortterm memory capacity. Series from three to ninedigits were presented on the screen and the task wasto reproduce the series on the key board. Dependingon the correctness ofthe answer, the number ofdigitsin the next series either increased or decreased. Fivetrials were performed, and each trial started with aseries of three digits and was terminated after fiveincorrect answers. The average maximum level (lon-gest digit span) in the five trials was used as testparameter.
(6) The Sternberg task-This is another short termmemory test. A set of two, three, or four randomlyselected digits was presented on the display and thetest subject was asked to remember this set. A digit
was then displayed on the screen and the subject wasordered to respond with a yes button if the digit wasincluded in the previous set (positive), or with a nobutton if the digit was not included (negative). Eachset of digits was tested twice and in total 12 positiveand 12 negative presentations were made for eachcondition. The regression coefficients for positiveand negative answers were calculated according toStemnberg's theory of processing time."8
REGISTRATION OF FOREARM TREMORThe frequency spectrum ofthe physiological forearmtremor was investigated with an accelerometer usingthe technique described by Fawer et al."9 The subjectwas seated with the right elbow resting on the arm ofthe chair and with a 900 elbow angle, the forearmunsupported and the hand supine. An accelerometer(Bruel and Kjaer 4384, weight 10 g) was tightly fixedon the dorsum of the wrist with a cuff. The electricalsignals were amplified (Bruel and Kjaer 2626) andrecorded on an FM tape recorder (Tandberg 100).Measurements were carried out first without loadduring 90 seconds, and then with a load of 1000 gattached to the hand for 90 seconds. The signals werecontinuously controlled on an oscilloscope. Tremorspectra were analysed with a spectrum analyser(Bruel and Kjaer 2032). Two peak frequencies andcorresponding accelerations were registered in eachspectrum. The middle 60 second periods were usedfor the spectra analyses.
EXPOSURE INDICATORSThe exposure indicators used in the chloralkali groupwere: (1) current concentration of mercury in wholeblood (B-Hg), serum (S-Hg), and urine (U-Hg); (2)average B-Hg during the past five years (samplescollected at each factory and analysed at the samelaboratory as the current samples); (3) duration ofemployment (number of years worked at thechloralkali plant); (4) intensity ofexposure (based onthe subjects' type ofwork, their exposure to mercurywas graded as low, medium, or high, as judged by oneof the researchers together with the companyphysicians); (5) peak exposures (relative frequency ofB-Hg values > 150 nmol/l during the past five years).The relative frequency was used as a control bloodsample was always requested for subjects with B-Hgabove 150 nmol/l at the routine controls. Subjectswith B-Hg persistently above 150 nmol/l were susp-ended from mercury exposed work for two or threeweeks and a new blood sample was taken after thisperiod.
In the control group, current concentrations ofmercury in whole blood, serum, and urine were usedas measures of current exposure to mercury. In bothgroups, fish consumption and amalgam burden wereused as indicators ofbackground exposure to methyl-mercury and inorganic mercury respectively.
547
on March 11, 2020 by guest. P
rotected by copyright.http://oem
.bmj.com
/B
r J Ind Med: first published as 10.1136/oem
.49.8.545 on 1 August 1992. D
ownloaded from

Langworth, Almkvist, Soderman, Wikstrom
Table 2 Current B-Hg, S-Hg, and U-Hg among chloralkali workers and controls
Exposed (n= 89) Controls (n = 75)
Median Range Median Range
B-Hg (nmol/1) 55 15 -299 15 1-65S-Hg (nmol/1) 45 1 -255 4 1-25U-Hg (nmol/mmol creatinine) 14 3 03- 46 9 1 1 0- 4-3
Samples for B-Hg analyses were collected in metalfree, heparinised, Venoject tubes (Terumo EuropeNV, Leuven, Belgium); samples for S-Hg analyseswere collected in metal free Venoject tubes andcentrifuged to separate the blood cells. Morningurine samples were collected at home by each subjectin 250 ml acid washed, polyethylene bottles andimmediately delivered to the company's health care
units. The B-Hg, S-Hg, and U-Hg were analysed inthe laboratory of the Division of Medical Chemistryat the Swedish National Institute of OccupationalHealth. A version of the cold vapour atomic absorp-tion spectrophotometry (CVAAS) technique des-cribed by Einarson et al 0 was used. The accuracy ofthe mercury analyses had earlier been tested andfound to be comparable with that obtained in otherlaboratories using CVAAS and neutron activationanalyses (NAA). Standard blood and urine sampleswith known concentrations ofmercury were analysedin every analytical series. For details relating toquality control of the mercury analyses see Lang-worth et al." The U-Hg was adjusted for creatinineexcretion measured with Jaffe's method using picricacid.
STATISTICAL ANALYSISBackground data, clinical parameters, testparameters (from questionnaires, psychometrictests, and tremor registrations), and mercury concen-
trations in the biological samples were comparedbetween the exposed and the control groups withStudent's t test, Mann-Whitney's U test, or the x2
test (smoking). Two *sided p values are giventhroughout.
In both groups dose-effect relations were studiedusing Pearson's correlation coefficient, Spearman'srank correlation coefficient (for skewed parameters),and multiple regression. The influence of back-ground factors such as age, smoking, and alcoholconsumption was tested in both groups.
The 90th percentiles of the test parameters in thecontrol group were regarded as upper normal values,and values above these among the exposed subjectswere considered abnormal. The prevalence ofabnor-mal values of test parameters in the chloralkali groupwas then related to the exposure parameters men-tioned previously and to three levels of current U-Hg: (a) low (<10 nmol Hg/mmol creatinine); (b)middle (10-25 nmol Hg/mmol creatinine); and (c)
high (> 25 nmol Hg/mmol creatinine). Theprevalence of abnormal test parameters in the sub-groups was then compared by x2 test or with Fisher'sexact test. Minitab data analyses software, release7.2, Minitab Inc, USA, were used for all analysesexcept Fisher's test.
ResultsWe found no significant differences between the twogroups for age, years of education, performance onthe verbal test (synonyms), smoking, alcohol con-sumption (cl of liquor per week), or fish intake (table1). The average number of amalgam surfaces wasslightly higher in the control group (table 1), but thegroup difference was not statistically significant(p = 0 09).The interviews showed that 14 chloralkali workers
and 10 controls had experienced earlier mild concus-sion of the brain. Eight chloralkali workers and sevencontrols were on regular medication because ofhypertension. Two chloralkali workers and one con-trol worker took tablets for diabetes. One chloralkaliworker was taking a neuroleptic drug because ofsleepdisturbances and anxiety. None of the subjects usedtranquillisers regularly.The physical examination showed that 17
chloralkali workers and 13 controls had slight fingertremor (17 of 89 v 13 of 75, non-significant). Fivechloralkali workers and three controls had slightlyimpaired tactile sensibility in feet or hands. Therewere no notable group differences in either systolic ordiastolic blood pressure.Table 2 presents results for current B-Hg, S-Hg,
and U-Hg for the two groups. Table 3 presents thefigures for the other indicators of exposure used inthe chloralkali group. Mercury concentrations in thebiological media were significantly higher in the
Table 3 Characteristics of some of the exposure indicatorsused in the chloralkali group
No Mean (SD) Median Range
Duration (y) 89 13 5 (8 7) 12 1- 45B-Hgl (nmol/l) 89 79 (34) 75 25-176B-Hg5 (nmol/l) 65 81 (37) 77 28-182B-Hg peaks (%) 89 24 (24) 20 0- 96
Duration = number of years worked at the plant, B-Hgl = meanB-Hg during the past year, B-Hg5 = mean B-Hg during the pastfive years, B-Hg peaks = frequency of B-Hg peaks > 150 nmol/lduring the past five years.
548
on March 11, 2020 by guest. P
rotected by copyright.http://oem
.bmj.com
/B
r J Ind Med: first published as 10.1136/oem
.49.8.545 on 1 August 1992. D
ownloaded from

Effects of occupational exposure to mercury vapour on the central nervous system
Loss of appetite
Hand tremor
Poor concentration
GI disturbance
Nervousness
Sleep disturbance
Memory disturbance
Tiredness
0 5
|ff3 Exposed z Control
10 15
Frequency (%)
20 25
Figure I Symptomfrequency in exposed and control groups.
mercury exposed group than in the control group.The concentrations were significantly related toestimated intensity ofexposure but not to duration ofemployment. In the control group the strongestpredictor for B-Hg and S-Hg was fish consumption,whereas the number of amalgam surfaces was thebest predictor for U-Hg (see Langworth et al").The number of symptoms reported at interview
was significantly higher in the mercury exposedgroup compared with the control group (p < 0001).Figure 1 shows the frequency of the eight mostreported symptoms (relevant to effects ofmercury onthe CNS) in the two study groups. All symptomsexcept hand tremor were more frequent in theexposed group, and statistically significant higher
frequencies were seen for tiredness (p = 0O002) andmemory disturbance (p = 0-013). Within the mer-
cury exposed group there were no significantdifferences in frequency of symptoms between daytime workers and shift workers. Dose-effect calcula-tions showed weak but statistically significant rela-tions between the total number of symptoms andcurrent B-Hg (r = 0-25, p = 0 02), current U-Hg/creatinine (r = 0-24, p = 0-04), average B-Hg dur-ing the past year (r = 0-32, p = 0-003), and average
B-Hg during the past five years (r = 0-28, p = 0-02).Furthermore, the frequency of all symptoms excepthand tremor and loss of appetite was higher in thesubgroup with estimated high exposure to mercurythan in the subgroup with estimated low exposure.
Table 4 Questionnaire scores in the chloralkali and control groups
Exposedgroup Controlgroupp-Value
Mean SD Mean SD (two-sided)
Q16 (n = 89) 3 03 2-85 1-63 1-84 00002
POMS (n = 88)*
Tiredness 2-70 0-88 2 40 0-75 0-018Confusion 2 40 0-62 2-18 0 55 0-045Depression 1-62 0-52 1-64 0-61 0-82Anger 1-60 0 59 1-50 0-58 0 30Tension 2-11 0-80 2-01 0-80 0 44
EPI-N (n = 87)t 6-55 3-88 4-99 3-42 0-007
Two sample t test was used for group comparisons.*One subject and ttwo subjects were excluded because of incomplete answers.
..........................I
.................................
............................................. .I
7r..
...........................................:.......i.............. ........
I
I............................ ...........................:
............................ .............. ............................ ................
III ..........L L.
549
on March 11, 2020 by guest. P
rotected by copyright.http://oem
.bmj.com
/B
r J Ind Med: first published as 10.1136/oem
.49.8.545 on 1 August 1992. D
ownloaded from

Langworth, Almkvist, Soderman, Wikstrom
Hand-eye coordination
I4 11
100
Ue
Cuco00z
90 -
80 -
60
Finger tapping(alternating)
I
Symbol-digit
I
T{ ' {a
450 -
425 -
400-a)Ez 375-0.)X 350-tr
325 -
II
I s S
Digit span (STM)
31I Il
20-35 36-50 51-65
Age classes
This increase was statistically significant for tired-ness (p = 0-013) and nervousness (p = 0 008). Inneither of the two groups was earlier concussion orcurrent medication correlated to prevalence ofsymp-toms.Table 4 shows the scores for the questionnaires
Reaction time (RT) -
I I
20-35 36-50 51-65
Age classes
Figure 2 Psychometric test performance in exposed (U)and control groups (LO). Mean values and SDs areindicated.
(Q16, POMS, and EPI). The number of yes answersin the Q16 was significantly higher in the chloralkaligroup than in the control group, and the prevalenceof five or more yes answers (regarded as the upperlimit in a normal population) was also significantlyhigher among exposed workers than among controls(p = 0-02, x2 test). Scores for tiredness and con-fusion in the POMS were significantly higher in thechloralkali group than in the control group, as wasthe score for neuroticism in EPI (EPI-N), whereasthe degree of extroversion or introversion did notdiffer between the two groups.The relations between the questionnaire scores
and different exposure indicators (used in thechloralkali group) were weak. Only the score forneuroticism in EPI showed a statistically significantrelation with average B-Hg during the past year(r = 0-24, p = 0-026).
Figure 2 gives the results of the psychometric tests
9 -
7-
5-
t',
04-
co
a)0
3-
45 -
40 -
35 -C',
0 30-
25 -
20 -
I0
97
8 -1
Cl,
0)
00z
7
6
5
550
I
-IZA
on March 11, 2020 by guest. P
rotected by copyright.http://oem
.bmj.com
/B
r J Ind Med: first published as 10.1136/oem
.49.8.545 on 1 August 1992. D
ownloaded from

Effects of occupational exposure to mercury vapour on the central nervous system
regression coefficient for negative sets on the Stern-Positive sets berg task was also correlated with the current S-Hg
and U-Hg (r = 0 35, p = 0-001; r = 0-28,p = 0-009 respectively).The prevalence of abnormal results for the psy-
chometric tests (poorer performance than the 90thpercentile of the control group) was compared for
,'/ different subgroups of the mercury exposed group(different exposure indicators were tested). No nota-ble dose-response relations were found. Neither wasthere any significant correlation between fish con-
. I| | sumption or amalgam burden and performance ofthe2 3 4 psychometric tests.
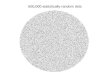
We found a large variance in the tremor frequencyspectra. Four people in the chloralkali group and sixcontrols were excluded due to large divergences in
Negative setsthe spectra. Figure 4 summarises the results of thetremor registrations. At rest (without load), a highpeak frequency (HPF, the frequency correspondingto the highest acceleration) of about 6 Hz was foundin both groups. In 31 exposed subjects and in 27
, - / controls a second HPF of about 10 Hz was seen.During load (1000 g) a first HPF was seen at about 4Hz and a secondHPF (for 85 exposed subjects and 72controls) at about 10 Hz. The exposed subjectstended to have higher acceleration amplitudes com-pared with the controls, but the differences were not
E E statistically significant.2 3 4 In both groups, a statistically significant negative
correlation existed between age and the second HPFRegression lines for positive and negative sets of during load (p < 001). Alcohol consumption and
iberg task in exposed (-) and control (---) smoking did not significantly affect the tremorparameters.
Finally, the relations between the different effectparameters were tested. These calculations showed
for the Stemnberg task). On four of the tests significant (p < 0-001) correlations between the1-digit, alternating finger tapping, reaction number of self reported symptoms and the scores inLd digit span) the average performance was both Q16 and POMS (except for anger). The scoresidentical in the two groups. On the hand-eye in POMS (except for confusion) were also correlatediation test the mercury exposed workers (p < 0 05) with the grade of neuroticism in EPI.slightly better results than the controls Performance on the psychometric tests did not
08). The test performance was age depen- correlate significantly with the other effecttarticularly in the symbol-digit test and in parameters.
alternating finger tapping. Test performance was notcorrelated with earlier concussion or with currentmedication in either group.
Figure 3 shows the regression lines for the positiveand negative sets in the Stemnberg test. The mercuryexposed workers performed slightly better than thecontrols.
In the chloralkali group the performance of thehand-eye coordination test, alternating finger tap-ping, and the Sternberg task for negative sets (theregression coefficient for negative sets), showed astatistically significant negative correlation with therelative number ofB-Hg peaks ( 150 nmol/l) duringthepastfiveyears(r = 0-24,p = 0-022;r = -0-28,p = 0-009; r = 0-25, p = 0-017 respectively). The
DiscussionSeveral investigations have shown that occupationalexposure to high concentrations of mercury vapourmay cause effects on both the CNS and the peripheralnervous system. In 1970, Smith et al' reported a doserelated increase in frequency of symptoms among567 chloralkali workers, particularly in subgroupswith exposure concentrations exceeding 100 jg Hg/m' air. Miller et al' found raised prevalences ofneurological signs, alterations in forearm tremorfrequency, --and impaired performance on psy-chomotor tests in a group of mercury exposedchloralkali workers with raised U-Hg (> 50 yg/l).
In more recent studies, increased prevalence of
900
800
700
0)E0-,
0)c4)
cc
900
800
700
Figure 3the Sterngroups.
(except(symbo]time analmost icoordinshowed(p = 0-1dent, p
551
on March 11, 2020 by guest. P
rotected by copyright.http://oem
.bmj.com
/B
r J Ind Med: first published as 10.1136/oem
.49.8.545 on 1 August 1992. D
ownloaded from

Langworth, Almkvist, Soderman, Wikstrom
Exposed group
No load20
(n
EE10
Load 1 kg
0 5 10 15 20 25 0 5 10 15 20 25Hz Hz
Control group
No load20 [
10 [
20U)
E
E 10E
Load 1 kg
0 5 10 15 20 25 0 5 10 15 20 25Hz Hz
Figure 4 Mean tremor spectra in exposed group (n = 85) and control group (n = 69).
subjective symptoms and impairment of cognitivefunctions have been shown at lower mercuryexposure. Smith et al" reported a dose related mer-cury effect on short term memory (assessed by 50%threshold for correct serial recall on the digit spantest) in two groups of chloralkali workers with anaverage U-Hg during the past 12 months of 195 pg/land 108 pg/l respectively. In a study by Roels and co-workers4 a dose related effect ofmercury was seen onboth psychomotor tests (eye-hand coordination,arm-hand steadiness) and on parameters of renaldysfunction, among mercury exposed workers withan average U-Hg of96 pg/g creatinine and an averageB-Hg of 29 jg/l. A Finnish study23 showed reducedperformance on the Santa Ana coordination testamong 36 chloralkali workers compared with mat-ched controls. Average U-Hg in the chloralkali groupwas about 58 pg/l and average B-Hg was about 20 Mg/1. In a later study, Roels and co-workers,24 reportedan increased prevalence of subjective symptoms, butnormal performance on various psychological tests(simple reaction time, critical flicker fusion, colourdiscrimination, short term memory) among mercuryexposed workers compared with controls. The auth-ors judged the registered increase in symptomprevalence as possible overreporting, however, dueto expected adverse effects among the mercury
exposed workers. Rosenman et al25 reportedincreased prevalence ofsymptoms correlated with U-Hg in a mercury exposed group of workers withaverage U-Hg between 28 and 50 pg/l and average B-Hg between 100 and 150 pg/l. A number of studieswere negative. Schuckmann et al"6 did not find anysignificant group differences in finger tremor, hand-eye coordination, or reaction time for 39 controls and39 chloralkali workers with a mean U-Hg of 108 pg/land a mean B-Hg of 20 pg/l. Bunn and co-workers27examined 101 chloralkali workers and nine controlsover a period of several years. Mercury concentra-tions in air varied from 50 pg to about 100 pg/m'. Theresearchers found no signs indicative of chronicmercury intoxication. In a recent study, Piikivi andHanninen'2 found no impairment of performance inpsychological tests, but an increase in self reportedmemory disturbance in a group of 60 Finnishchloralkali workers with a mean U-Hg of 17 pg/l anda mean B-Hg of about 10 pg/l. The memory distur-bance correlated strongest with shift work.
Alterations of hand or forearm tremor spectrainduced by mercury have been described by severalauthors."9 29 Fawer et all'9 reported a subclinicalincrease in forearm tremor frequency at an averageexposure of about 26 pg Hg/mi air (TWA), andrecently Chapman and co-workers described altera-
en
EE
enENU)
EE
0
552
on March 11, 2020 by guest. P
rotected by copyright.http://oem
.bmj.com
/B
r J Ind Med: first published as 10.1136/oem
.49.8.545 on 1 August 1992. D
ownloaded from

Effects of occupational exposure to mercury vapour on the central nervous system
tions in finger tremor in otherwise asymptomaticmercury exposed workers.'
In summary, many studies show effects on theCNS among mercury exposed workers; however, thereports are difficult to compare as different estimatesof exposure and various types of effect parametershave been used. No clearly established thresholdsexist below which effects of exposure to mercury onthe CNS can be safely excluded. Results from someof the most reliable studies indicate that chronicexposure to mercury concentrations below 50 pg/m'air seldom lead to increased prevalence of subjectivesymptoms or impaired test performance. The mostimportant indicator of biological exposure seems tobe U-Hg, and the biological threshold of 50 ug/gcreatinine (corresponding to about 28 nmol/mmolcreatinine) proposed by Roels and co-workers24appears, from these other studies, to be reasonable.
In our current study, efforts were made to obtaintwo groups as similar as possible for background datasuch as age, education, and type of work. Theequivalent results on the synonym test suggest thatverbal knowledge within the two groups was similar,a fact that may have been underestimated in some ofthe other studies mentioned.Our chosen indicators of exposure were a combin-
ation of current and long term estimates. Peakexposure was included because correlations betweenpeak exposures of mercury and effects on the CNShave been described in earlier studies.223" This wasthe only estimate of exposure that correlated withimpaired performance in some of the psychologicaltests. Theoretically, repeated peak exposures may bemore dangerous for the CNS than chronic lowexposure, because concentrations of free mercuryvapour in blood become much higher at peakexposures, and the amount ofmercury that passes theblood brain barrier is dependent on the concentrationof unoxidized mercury vapour in the blood.'During the past decades, technical improvements
and encouragement ofpersonal hygiene at work havesignificantly reduced the exposure to mercury inSwedish chloralkali factories.7 At the time of thisstudy the average mercury concentration in air wasestimated to be about 25 pg/m' based onmeasurements made by the company's health careunits and by our own random measurements perfor-med with a goldfilm sniffer (model Jerome 411,Jerome Inc, USA). The random samples showedlarge fluctuations in concentration, however, withpeaks up to 150 pg/m' air.The selection of symptom questionnaires and
psychological tests was also an object ofdiscussion. Itis well known that symptom questionnaires may leadto overreporting of subjective symptoms. To preventthis, our symptom questionnaire (Q16) was com-bined with an interview and two questionnairesaimed to detect early changes in mood state and
personality (POMS and EPI). The last two question-naires are regarded as less sensitive to overreportingthan a common symptom questionnaire.The raised prevalence of symptoms in the
chloralkali group may still be a result of overreport-ing. The concomitant increase in the scores fortiredness, confusion (POMS), and neuroticism(EPI), together with the registered correlation bet-ween the prevalence of symptoms and questionnairescores, mitigates against this, however. Furthermore,the dose-effect relations seen in all three question-naires, although weak, indicate that a real effect ofmercury on subjective wellbeing exists, at leastamong the workers with highest exposure to mer-cury.The selection of psychometric tests was based on
experiences from earlier studies ofeffects on the CNScaused by mercury and various neurotoxic agents.The computerised test battery developed by Bakerand co-workers,'7 has shown high stability over timeand strong correlations with other standardisedtests.'4Our test battery did not show any significant
differences in performance between the two groups,and dose-effect relations were weak. We found atendency toward poorer performance among subjectswith increased frequency of earlier peak exposures,whereas a long term indicator such as duration ofemployment did not correlate with test performance.The strong correlation between age and test perfor-mance indicates that the selected tests were sensitivefor the detection of effects on the CNS.Our findings are in agreement with earlier studies
in which exposures were also low.2324 ' The lack ofdecreased performance on the psychometric tests,together with increase in prevalence of symptoms(Q16, POMS) and degree of neuroticism (EPI)registered in the chloralkali group, points to symp-toms as more sensitive indicators of effects of mer-cury on the CNS than the psychometric tests.The choice oftremor registration was based on the
report by Fawer et al,'9 in which alterations in tremorspectra (higher HPFs related to exposure duration)were described at comparatively low exposure.These results are supported by newly publishedfindings of Chapman et al.' In a recent study,however, Roels et al"2 compared three differentmethods of hand tremor registration (accelerometerregistration, hand-eye coordination, and handsteadiness), without finding any significant differen-ces between a mercury exposed group (with medianU-Hg 63 pg/g creatinine and median B-Hg 24 pg/l)and a control group.Our results showed tendencies towards higher
HPF and higher accelerations, especially duringload, in the chloralkali group, but group differenceswere not statistically significant.The amount of mercury released from dental
553
on March 11, 2020 by guest. P
rotected by copyright.http://oem
.bmj.com
/B
r J Ind Med: first published as 10.1136/oem
.49.8.545 on 1 August 1992. D
ownloaded from

Langworth, Almkvist, Soderman, Wikstrom
amalgam fillings is normally low,"' far lower thanoccupational exposure to mercury in the chloralkaliindustry. Despite this, there has been debate concer-ning possible toxic effects of mercury released fromdental fillings. We therefore tested the relationbetween the number of amalgam surfaces and someof the effect parameters. These calculations showedno significant correlations between the number ofamalgam surfaces and questionnaire scores or perfor-mance on the psychometric tests in either group.We regard our results as representative for mer-
cury exposed chloralkali workers in Sweden. Eightynine out of a total of about 250 exposed workers wereexamined. The selection criteria selected mainlyworkers subjected to high exposure, thus the risk ofunderestimating the adverse effects of the workers'exposure seems to have been small.
ConclusionsOur results suggest a slight effect on the CNS due tothe present low mercury exposure. The registereddose-effect relations, although weak, indicate that thiseffect is best related to current exposure to mercuryand to earlier peak exposures. None ofthe parametersofeffect were related to duration ofemployment. Thefinding of suspected effects on the CNS at this lowexposure suggests that the Swedish exposure limitfor metallic mercury vapour of 50 Mg Hg/m' air is toohigh. The exposure limit of 25 pg/mi (TWA) recom-mended by the World Health organisation6 seemsmore accurate.
We thank all personnel at the companies' health careunits for excellent collaboration, and Dr Carl-GustafElinder and Dr Carl-Johan Gothe for general scien-tific support. Mercury analyses were carried out byMrs Kerstin Roxstrom and Mrs Siw Siljerud and weappreciate their help. Financial support was obtainedfrom the Swedish Work Environment Fund.
Requests for reprints to: Dr S Langworth, Depart-ment ofOccupational Medicine, Huddinge Hospital,S-141 86 Huddinge, Sweden.
1 Berlin M. Mercury. In: Friberg L, Nordberg GF, Vouk VB, eds.Handbook on the toxicology of metals. Vol II. Amsterdam:Elsevier, 1986:387-445.
2 Smith RG, Vorwald AJ, Patil LS, Mooney TF. Effects ofexposure to mercury in the manufacture of chlorine. Am IndHyg Ass J 1970;31:687-700.
3 Miller JM, Chaffin DB, Smith RG. Subclinical psychomotorand neuromuscular changes in workers exposed to inorganicmercury. Am Ind Hyg Assoc J 1975;36:725-33.
4 Roels H, Lauwerys R, Buchet JP, Bernard A, Barthels A,Oversteyns M, Gaussin J. Comparison of renal function andpsychomotor performance in workers exposed to elementalmercury. Int Arch Occup Environ Health 1982;50:77-93.
5 Triebig G, Schaller KH. Neurotoxic effects in mercury-exposedworkers. Neurobehav Toxicol Teratol 1982;4:717-20.
6 World Health Organisation. Recommended health-based limitsin occupational exposure to heavy metals. Geneva: WVHO,1980. (WHO technical reports series, No 647.)
7 Sallsten G, Barregard L, Jarvholm B. Mercury in the Swedishchloralkali industry-An evaluation of the exposure and thepreventive measures over 40 years. Ann Occup Hyg1990;34:205-14.
8 Langworth S, Elinder C-G, Sundkvist K-G, Vesterberg 0.Renal and immunological effects of occupational exposure toinorganic mercury. Br J Ind Med 1992;49:394-401.
9 Lezak M. Neuropsychological assessment. New York: OxfordUniversity Press, 1983.
10 Hogstedt C, Andersson K, Hane M. A questionnaire approach tothe monitoring of early disturbances in central nervousfunctions. In: Aito A, Ruhimaki V, Vainio H, eds. Biologicalmonitoring and surveillance of workers exposed to chemicals.Washington: Hemisphere Publishing Corporation, 1984:257-87.
11 Hogstedt C, Hane M, Agrell A, Bodin L. Neuropsychologicaltest results and symptoms among workers with well-definedlong-term exposure to lead. Br J Ind Med 1983;40:99-105.
12 Fidler AT, Baker EL, Letz RE. Neurobehavioural effects ofoccupational exposure to organic solvents among constructionpainters. Br J Ind Med 1987;44:292-308.
13 McNair DM, Lorr M, Droppleman LF. EITS Manual-Profileofmood states. San Diego: Educational and Industrial TestingService, 1971.
14 Baker EL, Letz RE, Fidler AT, Shalar S, Plantamura D,Lyndon M. A computer-based neurobehavioural evaluationsystem for occupational and environmental epidemiology:Methodology and validation studies. Neurobehav ToxicolTeratol 1985;7:369-77.
15 Eysenck H. The Maudsley personality inventory. London:University of London Press Ltd, 1959.
16 Forzi M, Cassito MG, Bulgheroni C, Foa V. Psychologicalmeasures in workers occupationally exposed to mercuryvapours: a validation study. In: Horvath M, ed. Adverse effectsofenvironmental chemicals andpsychotropic drugs. Amsterdam:Elsevier, 1976:165-71.
17 Baker EL, Letz RE, Fidler AT. A computer-administeredneurobehavioural evaluation system. J Occup Med1985;27:206-12.
18 Stemnberg S. Memory scanning: mental processes revealed byreaction time experiments. American Scientist 1969;57:421-57.
19 Fawer RF, de Ribaupierre Y, Guillemin MP, Berode M, Lob M.Measurement of hand tremor induced by industrial exposureto metallic mercury. Br J Ind Med 1983;40:204-8.
20 Einarsson 0, Lindstedt G, Bergstrom T. A computerizedautomatic apparatus for determination of mercury inbiological samples. J Automat Chm 1984;2:74-9.
21 Langworth S, Elinder C-G, Gothe C-J, Vesterberg 0. Biologicalmonitoring of occupational and environmental exposure tomercury. Int Arch Occup Environ Health 1991;63:161-7.
22 Smith PJ, Langolf GD, Goldberg J. Effects of occupationalexposure to elemental mercury on short-term memory. Br JInd Med 1983;40:413-9.
23 Piikivi L, Hanninen H, Martelin T, Mantere P. Psychologicalperformance and long-term exposure to mercury vapors.Scand J Work Environ Health 1984;10:35-41
24 Roels H, Gennart JP, Lauwerys R, Buchet JP, Malchaire J,Bernard A. Surveillance of workers exposed to mercuryvapour: Validation of a previously proposed biological thre-shold limit value for mercury concentration in urine. Am J IndMed 1985;7:45-71.
25 Rosenman KD, Valciukas JA, Glickman L, Meyers HR, CinottiA. Sensitive indicators of inorganic mercury toxicity. ArchEnviron Health 1986;41:208-15.
26 Schuckmann F. Study ofpreclinical changes in workers exposedto inorganic mercury in chloralkali plants. Int Arch OccupEnviron Health 1979;44:193-200.
27 Bunn WB, McGill CM, Barber TE, Cromer JWJ, GoldwaterLJ. Mercury exposure in chloralkali plants. Am IndHyg AssocJ 1986;47:249-54.
28 Piikivi L, Hanninen H. Subjective symptoms and psychologicalperformance ofchlorine-alkali workers. ScandJ Work EnvironHealth 1989;15:69-74.
29 VerberkMM, Salle HJA, Kemper CM. Tremor in workers withlow exposure to metallic mercury. Am Ind Hyg Assoc J1986;47:559-62.
30 Chapman LJ, Sauter SL, Henning RA, Dodson VN, ReddanWG, Matthews CG. Differences in frequency offinger tremorin otherwise asymptomatic mercury workers. Br J Ind Med1990;47:838-43.
31 LangolfGD, Chaffin DB, Henderson R, Whittle HP. Evaluationof workers exposed to elemental mercury using quantitative
554
on March 11, 2020 by guest. P
rotected by copyright.http://oem
.bmj.com
/B
r J Ind Med: first published as 10.1136/oem
.49.8.545 on 1 August 1992. D
ownloaded from

Effects of occupational exposure to mercury vapour on the central nervous system
tests of tremor and neuromuscular functions. Am Ind HygAssoc J 1978;39:976-84.
32 Roels H, Abdeladim S, Braun M, Malchaire J, Lauwerys R.Detection of hand tremor in workers exposed to mercuryvapor: A comparative study of three methods. Environ Res1989;45: 152-65.
33 Langworth S, Kolbick K-G, Akesson A. Mercury exposurefrom dental fillings. II. Release and absorption. Swed Dent J
1988;12:71-2.34 Mackert JR Jr. Factors affecting estimation of dental amalgam
mercury exposure from measurements of mercury vapourlevels in intra-oral and expired air. J Dent Res 1987;66:1775-80.
Accepted 6 January 1992
Vancouver style
All manuscripts submitted to the Br J Ind Medshould conform to the uniform requirements formanuscripts submitted to biomedical joumals(known as the Vancouver style).The Br J Ind Med, together with many other
international biomedical journals, has agreed toaccept articles prepared in accordance with theVancouver style. The style (described in full in BrMed J, 24 February 1979, p 532) is intended tostandardise requirements for authors.
References should be numbered consecutivelyin the order in which they are first mentioned inthe text by Arabic numerals above the line on eachoccasion the reference is cited (Manson' confirmedother reports' . . .). In future references to paperssubmitted to the Br JlndMed should include: the
names of all authors if there are six or less or, ifthere are more, the first three followed by et al; thetitle of journal articles or book chapters; the titlesof journals abbreviated according to the style ofIndexMedicus;andthefirstandfinalpagenumbersof the article or chapter.
Excamples ofcommon forms of references are:
1 International Steering Committee of Medical Editors.Uniform requirements for manuscripts submitted tobiomedical journals. Br Mcd J 1979;1:532-5.
2 Soter NA, Wasserman SI, Austen KF. Cold urticaria:release into the circulation of histamine and eosino-philchemotactic factor of anaphylaxis during cold challenge.N Engl JMed 1976;294:687-90.
3 Weinstein L, Swartz MN. Pathogenic properties ofinvadingmicro-organisms. In: Sodeman WA Jr, Sodeman WA,eds. Pathologicphysiology: mechanisms ofdisease. Philadel-phia: W B Saunders, 1974:457-72.
555
on March 11, 2020 by guest. P
rotected by copyright.http://oem
.bmj.com
/B
r J Ind Med: first published as 10.1136/oem
.49.8.545 on 1 August 1992. D
ownloaded from
Recommended