Diuretics
Diuretics
Agents that promote natriuresis (salt loss) and diuresis (water loss)
Used to treat hypertension and fluid retention
Salt & Water Balance
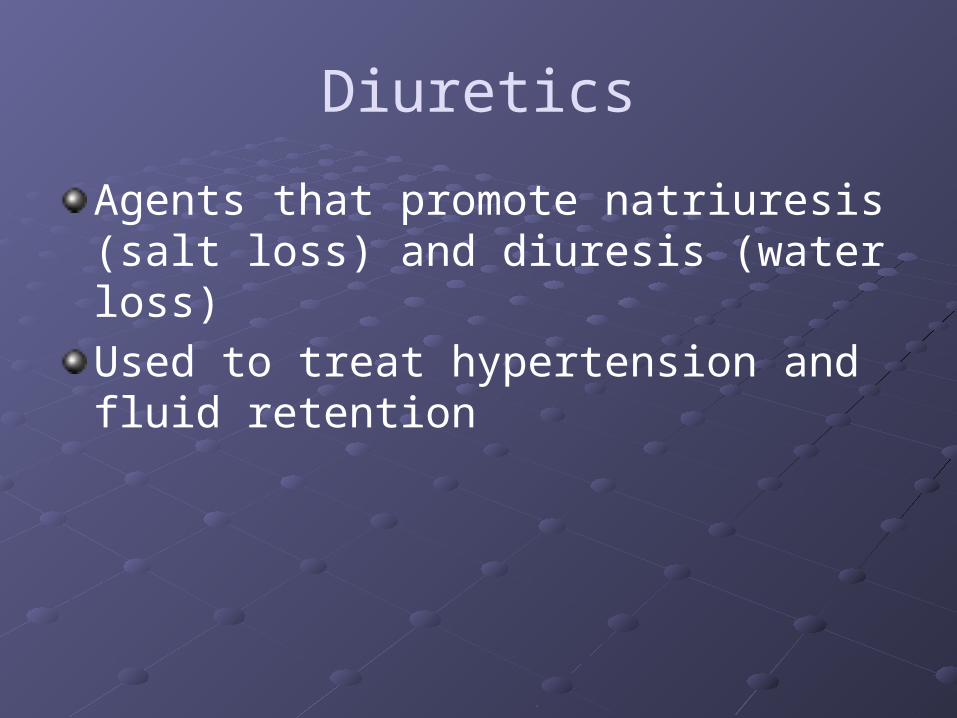
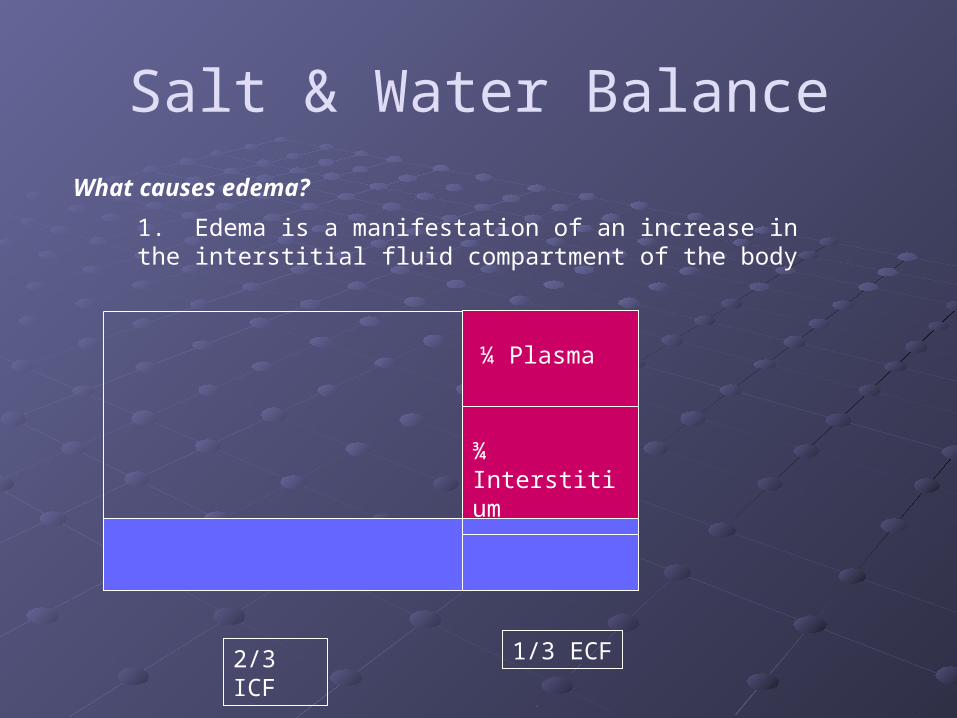
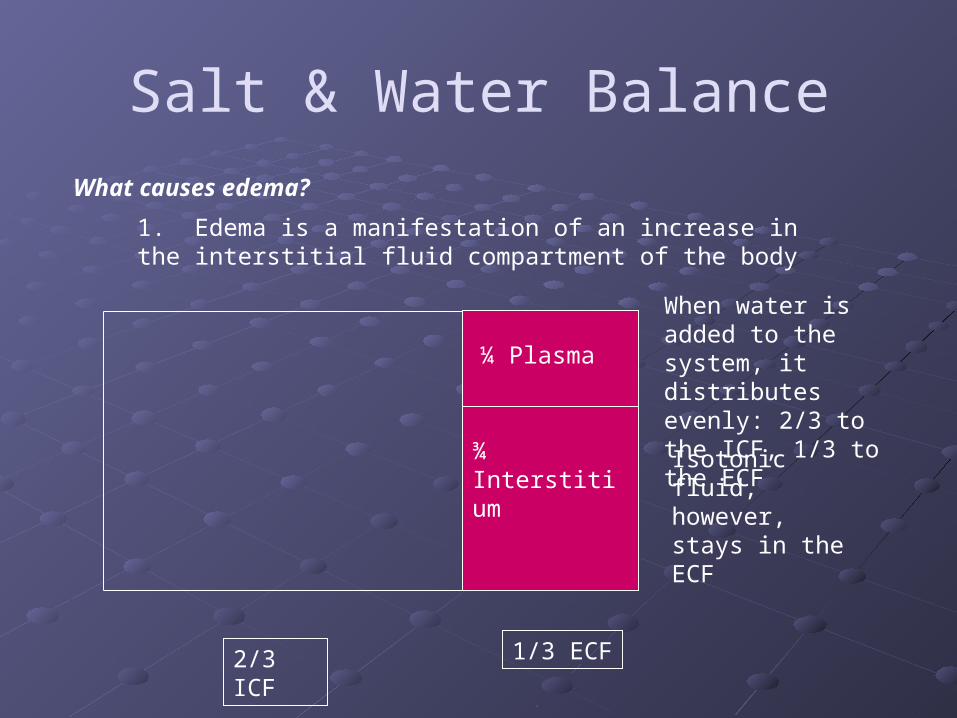
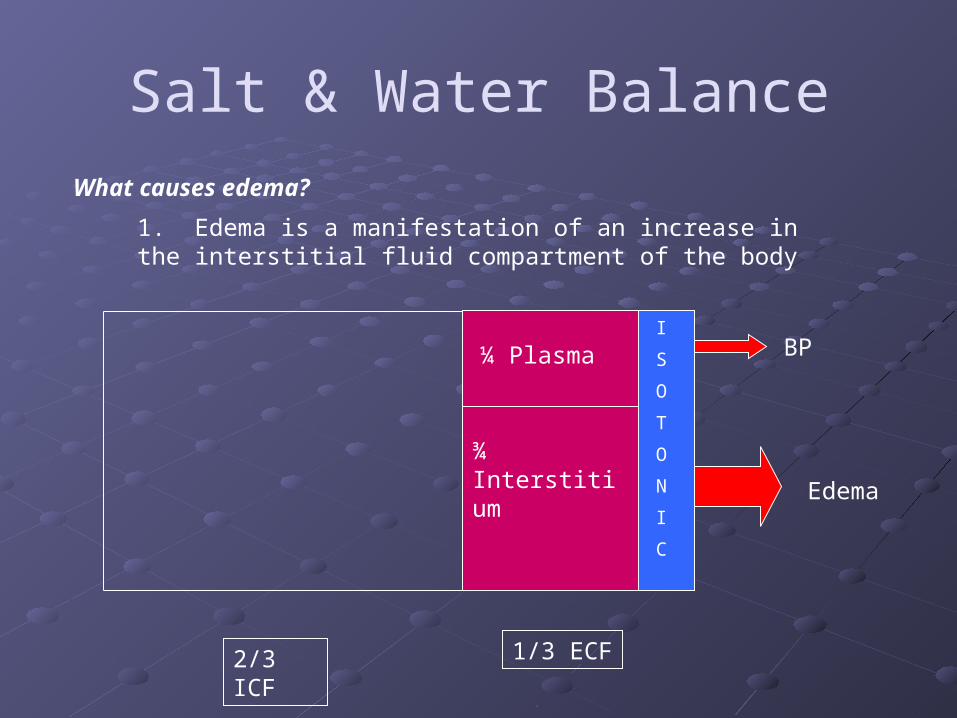
2/3 ICF 1/3 ECF
What causes edema?
¼ Plasma
¾ Interstitium
1. Edema is a manifestation of an increase in the interstitial fluid compartment of the body
Salt & Water Balance
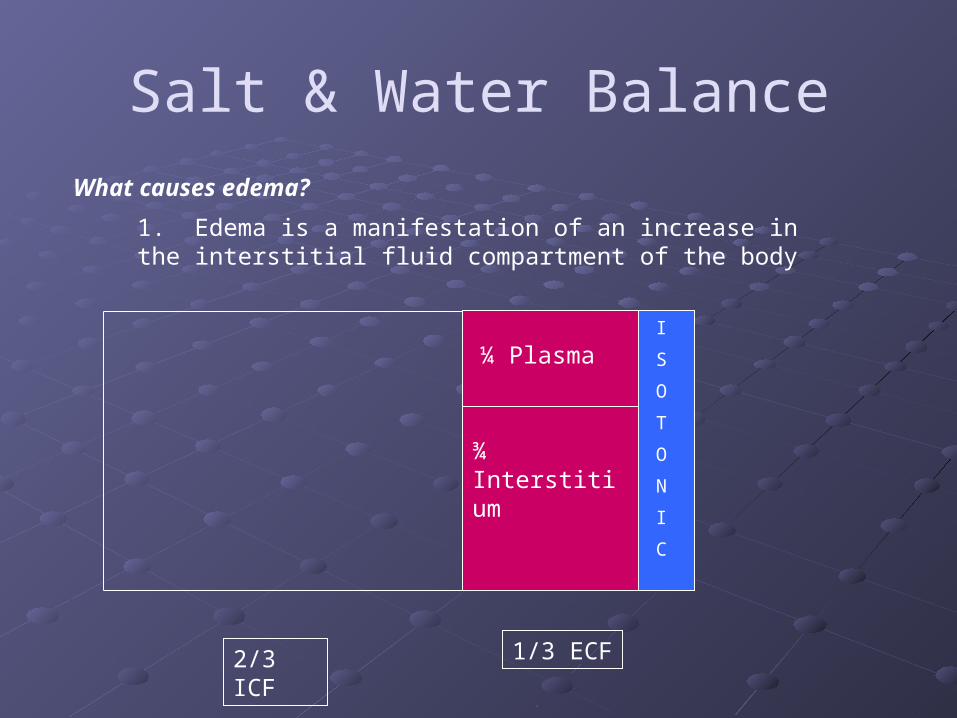
2/3 ICF 1/3 ECF
What causes edema?
¼ Plasma
¾ Interstitium
1. Edema is a manifestation of an increase in the interstitial fluid compartment of the body
When water is added to the system, it distributes evenly: 2/3 to the ICF, 1/3 to the ECFIsotonic fluid, however, stays in the ECF
Salt & Water Balance
2/3 ICF 1/3 ECF
I
S
O
T
O
N
I
C
What causes edema?
¼ Plasma
¾ Interstitium
BP
Edema
1. Edema is a manifestation of an increase in the interstitial fluid compartment of the body
Salt & Water Balance
2/3 ICF 1/3 ECF
I
S
O
T
O
N
I
C
What causes edema?
¼ Plasma
¾ Interstitium
1. Edema is a manifestation of an increase in the interstitial fluid compartment of the body
Salt & Water Balance
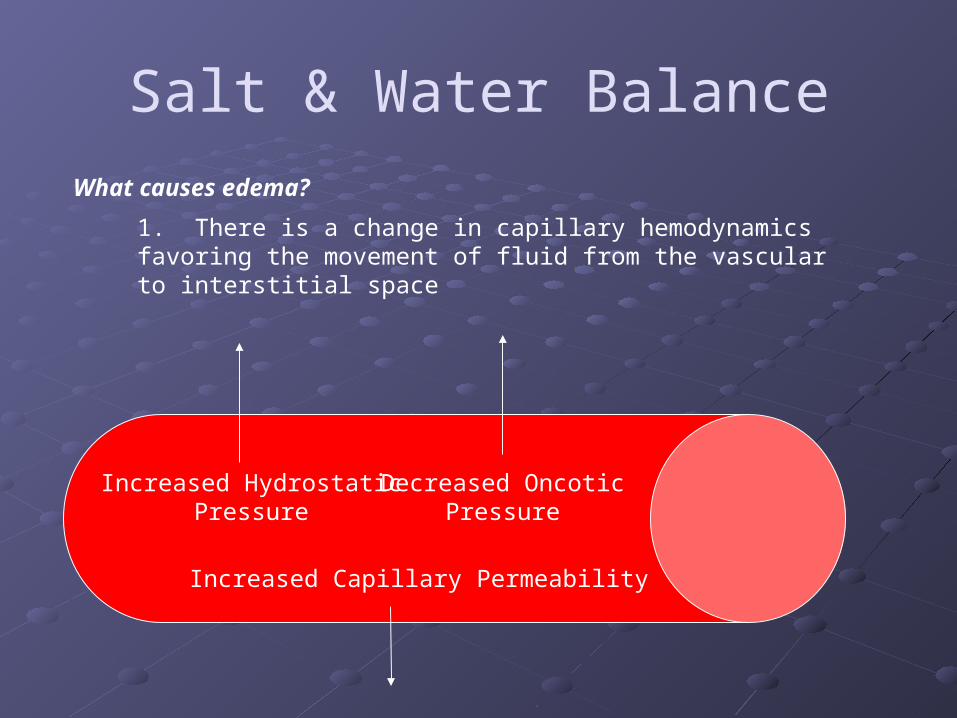
What causes edema?
1. There is a change in capillary hemodynamics favoring the movement of fluid from the vascular to interstitial space
Increased Hydrostatic Pressure
Decreased Oncotic Pressure
Increased Capillary Permeability
Diuretics
Diuretics have profound clinical implicationsThey allow physicians to manipulate salt and water excretion in impaired states of volume/solute regulationLike all great therapeutic interventions, they have the potential to make patients better, and, when not considered carefully, the potential to make patients worse
Diuretics
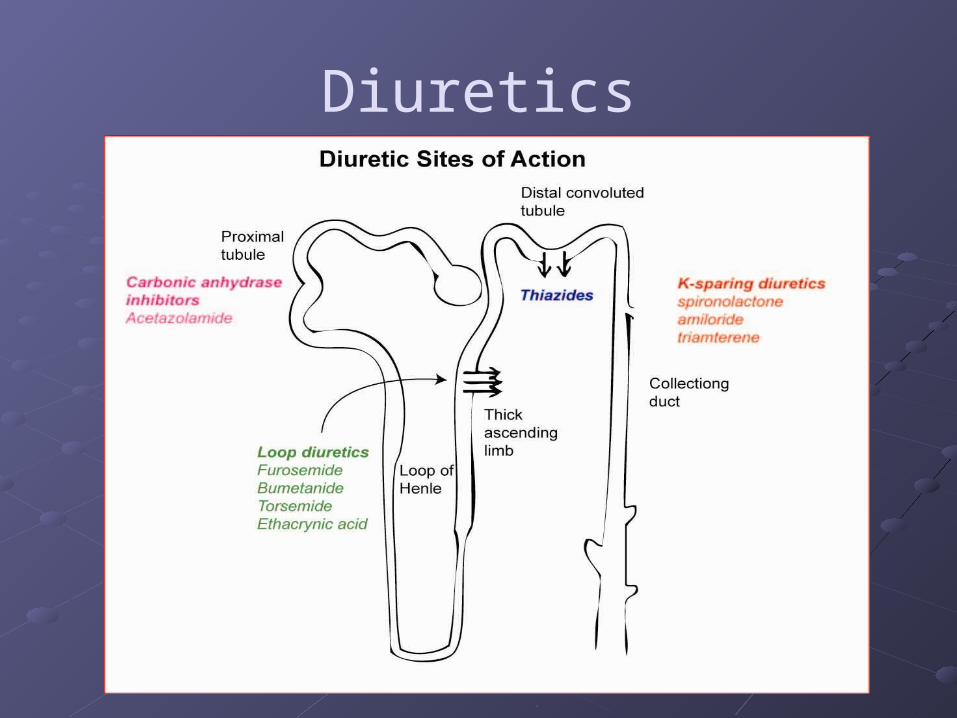
Act primarily by inhibiting Na channels in the renal tubular system
To reach the tubular lumen, these drugs must be… Ingested and absorbed Effectively circulated Secreted into the renal tubular lumen Bound to the target transporter
Question 1
All of the following are potential obstacles in the diuretic’s migration from pill bottle to apical transporter EXCEPT: A. Low Albumin States B. Pt non compliance C. Renal Failure D. All of these are obstacles to effective
diuresis
Question 2
In patients with nephrotic syndrome, oral diuretics: A. Are not effective, since these patients have
volume retention due to low albumin states and not salt retention
B. Are absorbed more efficiently in the gut C. May bind albumin in the urine instead of
their targeted apical transporters D. Are unable to reach the apical transporters
due to impaired glomerular permeability
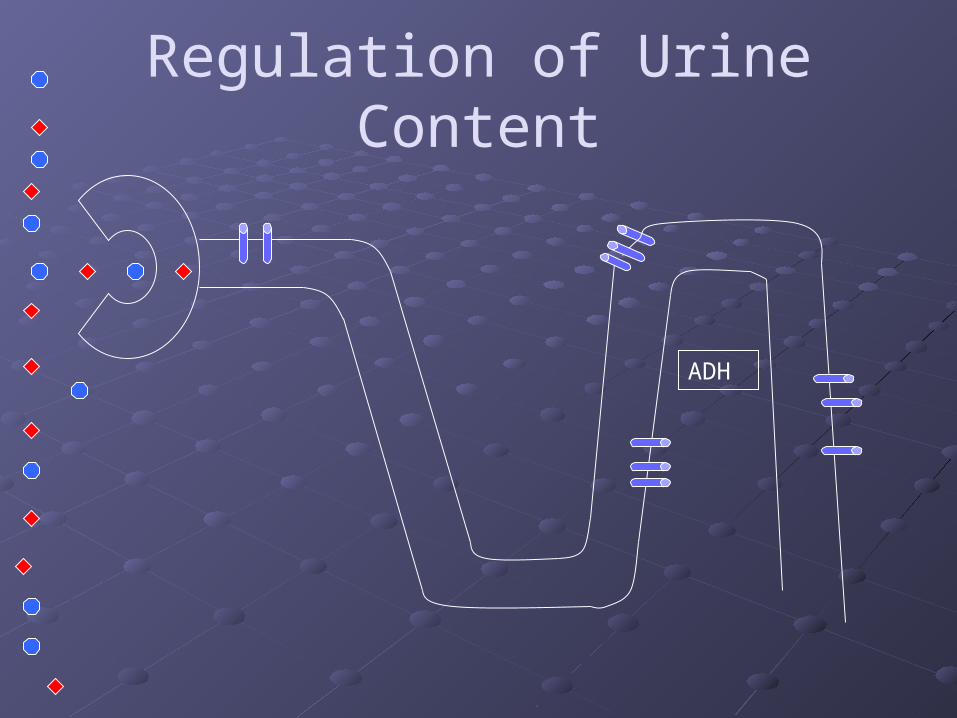
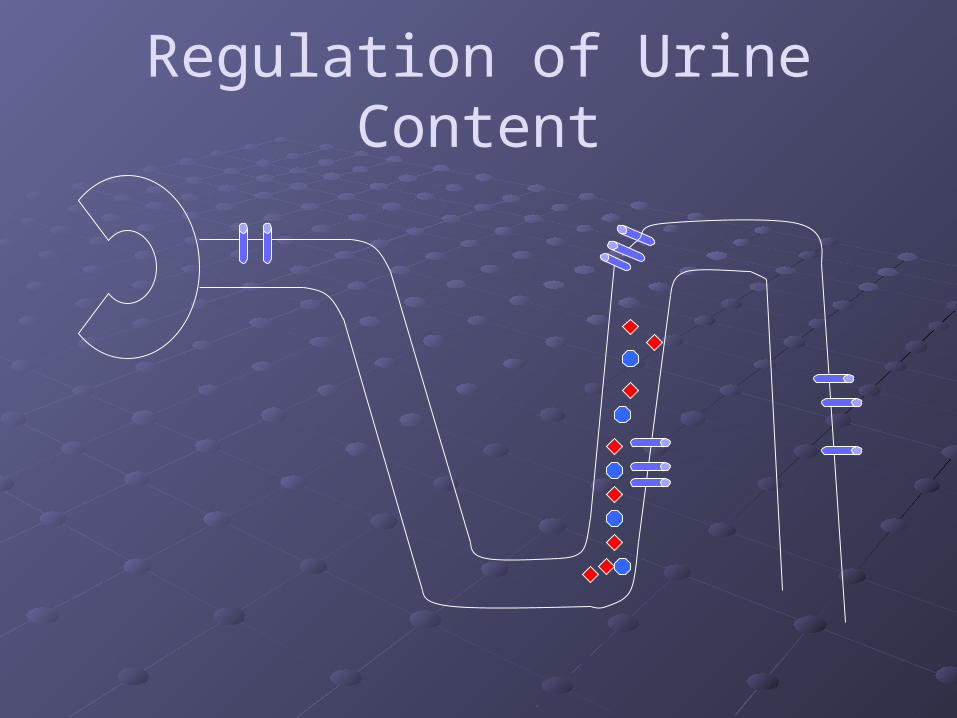
Regulation of Urine Content
ADH
Diuretics
Diuretics
Are all diuretics pretty much the same?
Well, they all cause people to pee
But recognize the difference based on the channels being blocked
Favorite test questions focus on “Why is one diuretic better than another in a particular context?”
Diuretics
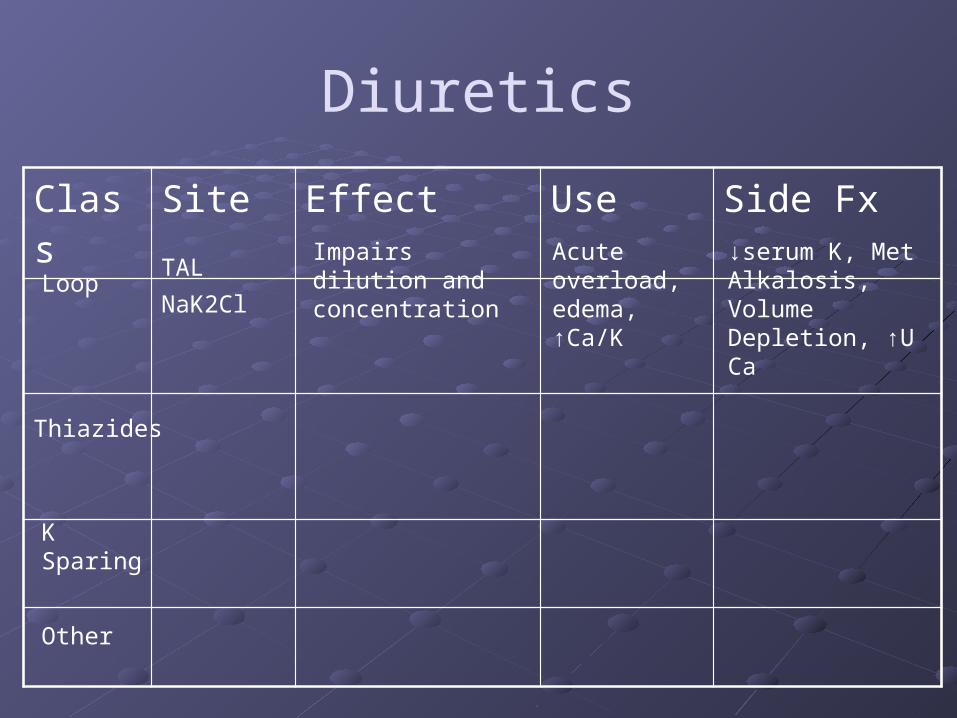
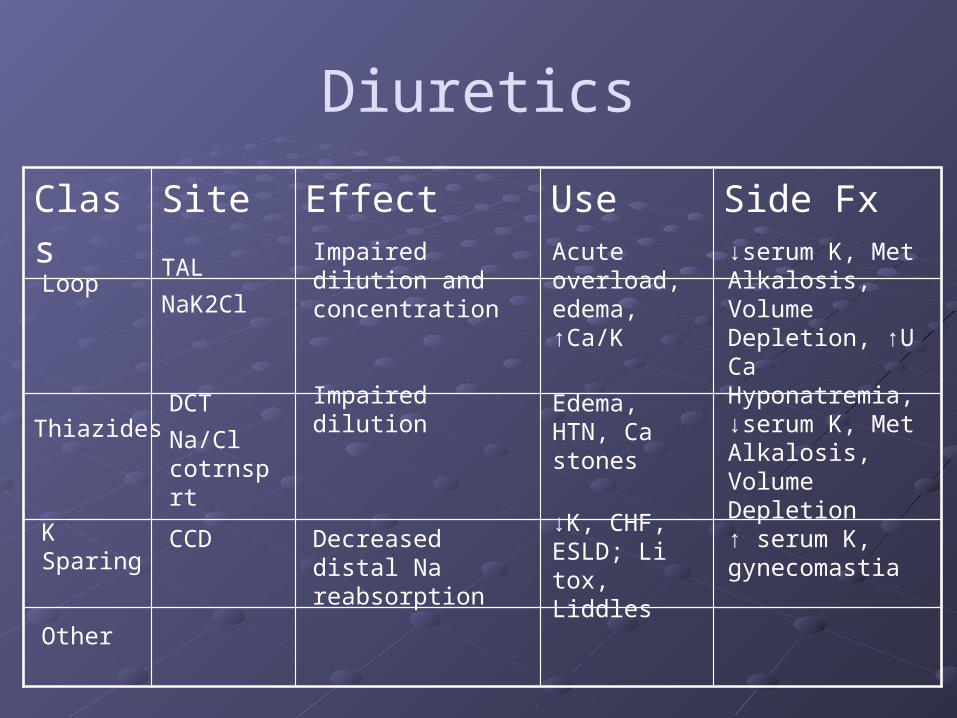
Class Site Effect Use Side Fx
Thiazides
Loop
K Sparing
Other
Diuretics
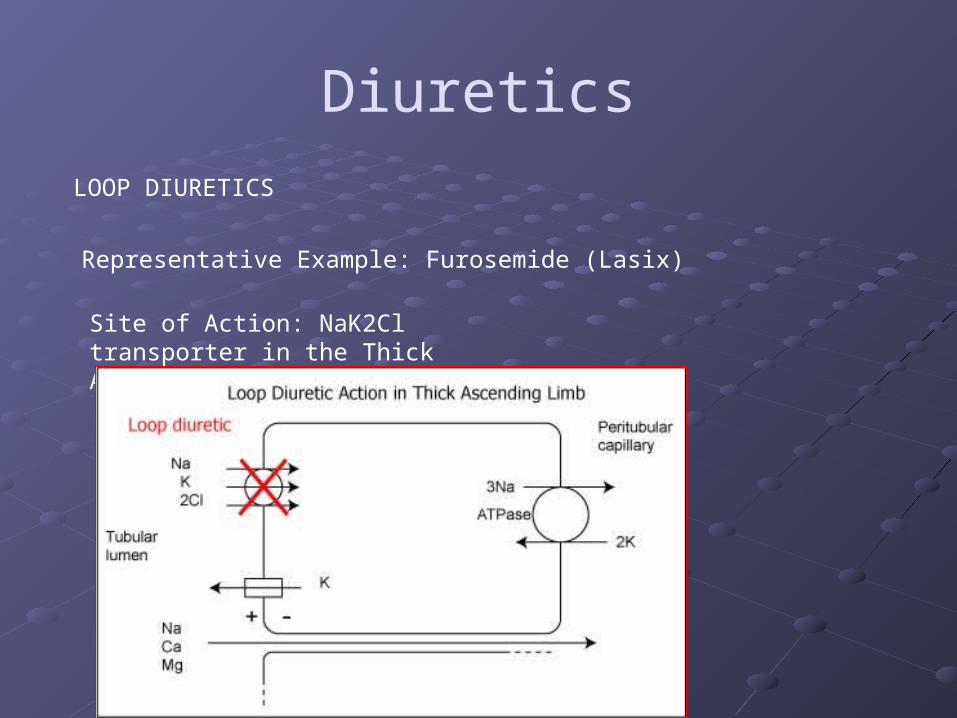
LOOP DIURETICS
Representative Example: Furosemide (Lasix)
Onset of action: roughly 30 minutes with PO, 5 minutes with IV
Duration: 6 hours
LASIX = “Lasts Six [Hours]”
Diuretics
LOOP DIURETICS
Representative Example: Furosemide (Lasix)
Site of Action: NaK2Cl transporter in the Thick Ascending Limb

Loop Diuretics
Decrease sodium reabsorption
Impairs the generation of a medullary gradient
Thus… Impairs urine dilution Impairs urine concentration
Regulation of Urine Content
ADH
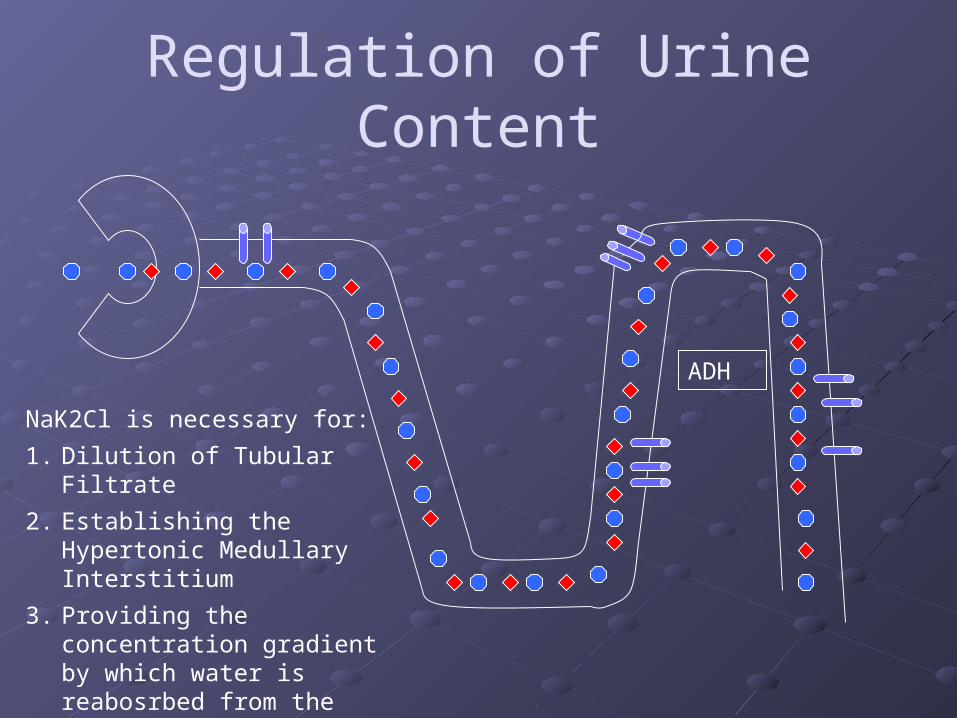
NaK2Cl is necessary for:
1. Dilution of Tubular Filtrate
2. Establishing the Hypertonic Medullary Interstitium
3. Providing the concentration gradient by which water is reabosrbed from the collecting duct (urinary concentration)
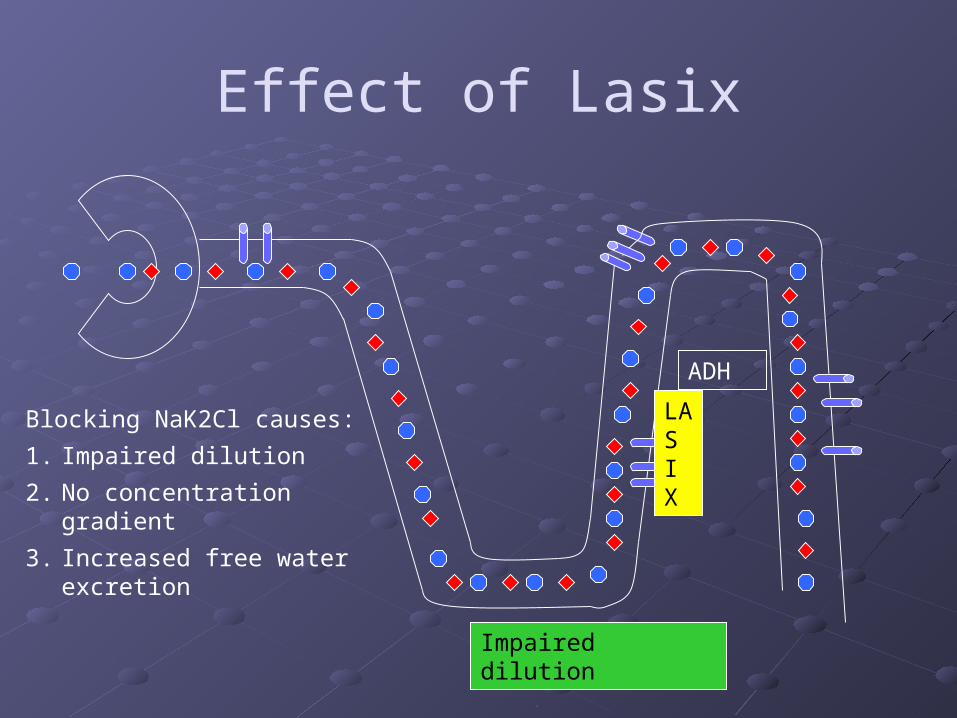
Effect of Lasix
ADH
Blocking NaK2Cl causes:
1. Impaired dilution
2. No concentration gradient
3. Increased free water excretion
LAS I X
Impaired dilution
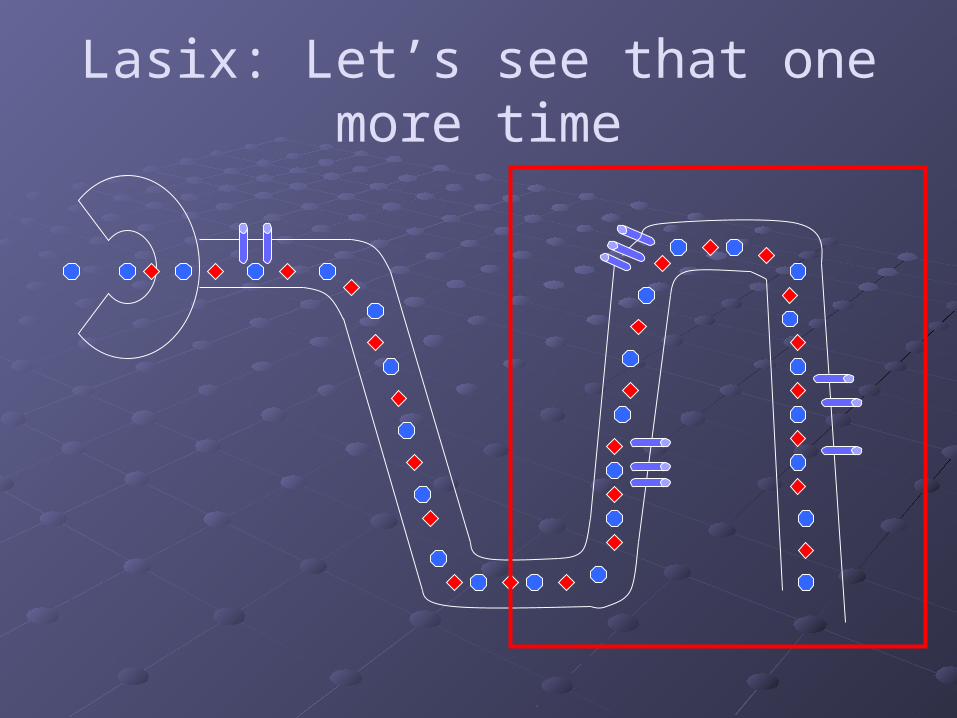
Lasix: Let’s see that one more time
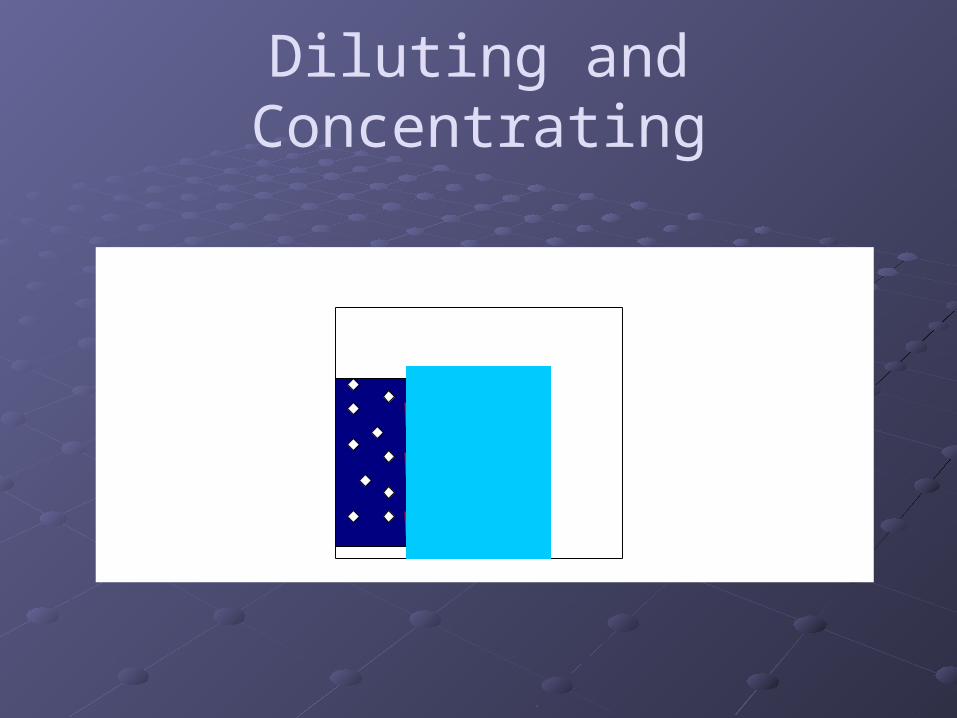
Diluting and Concentrating
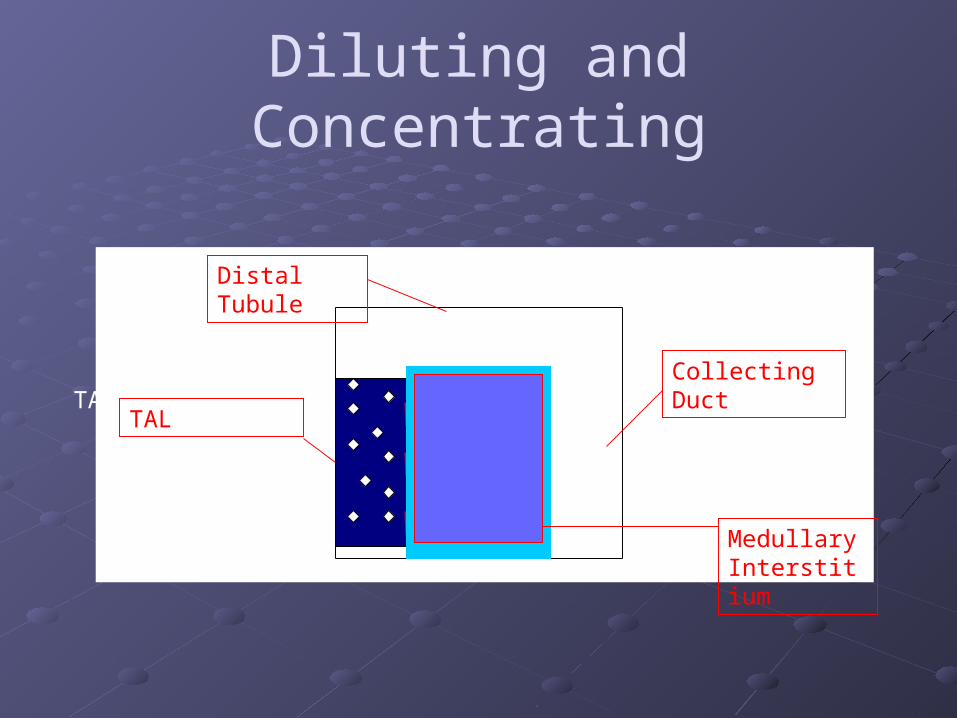
Diluting and Concentrating
TAL
TAL
Distal Tubule
Collecting Duct
Medullary Interstitium
Loop Diuretics
Decrease sodium reabsorption
Impairs the generation of a medullary gradient
Thus… Impairs urine dilution Impairs urine concentration
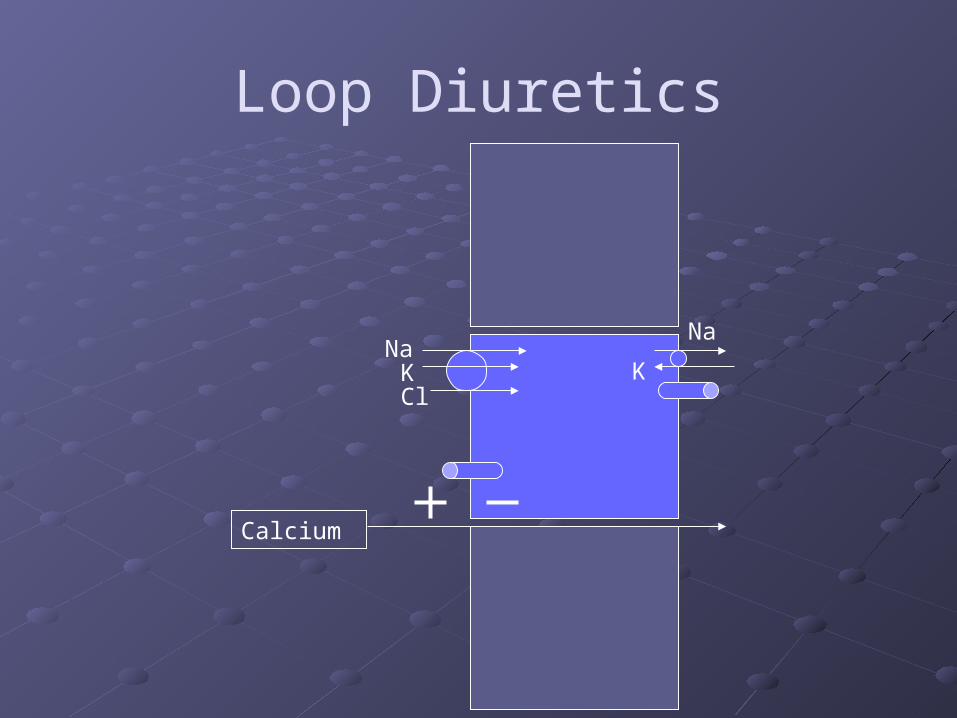
Loop Diuretics
NaKCl
Na
K
Calcium
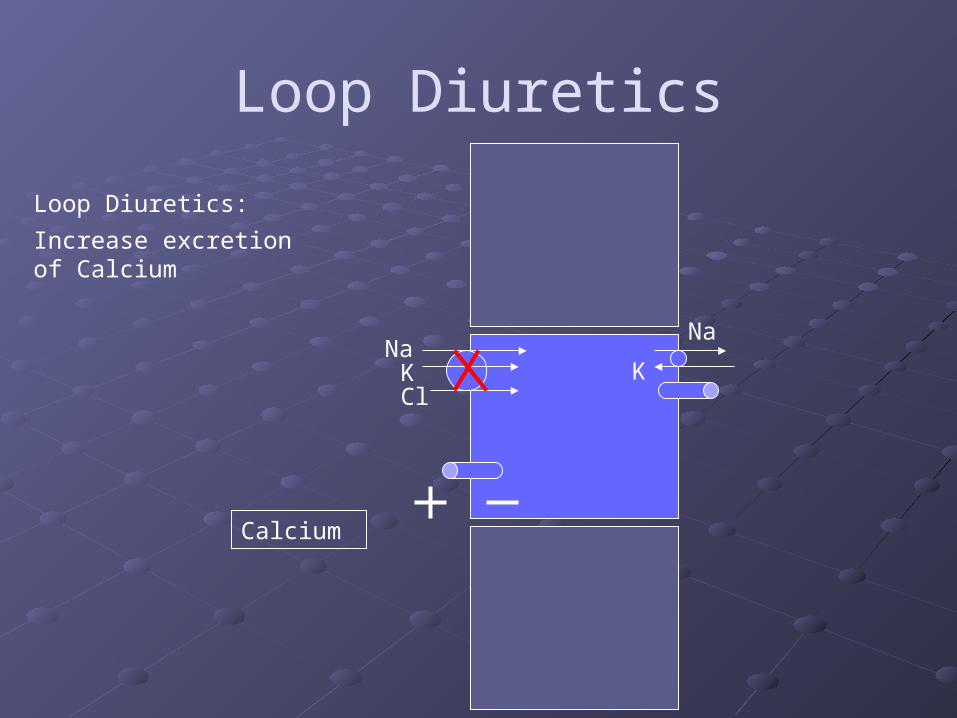
Loop Diuretics
NaKCl
Na
K
Calcium
Loop Diuretics:
Increase excretion of Calcium

Loop Diuretics
Collecting Duct
Na Na
NaNa
K
The increase in Na delivery to the Collecting Duct causes an increase in the exchange of Na for secretion of K/H+
H

Diuretics
LASIX Quick onset of diuresis
Good for acute volume overload Increases urinary calcium excretion
Used to treat hypercalcemia (Malignancy, Hyperparathyroidism)
Increases urinary excretion of potassium and hydrogen ions
Used to treat acute hyperkalemia
3 Reasons to love your loop diuretic
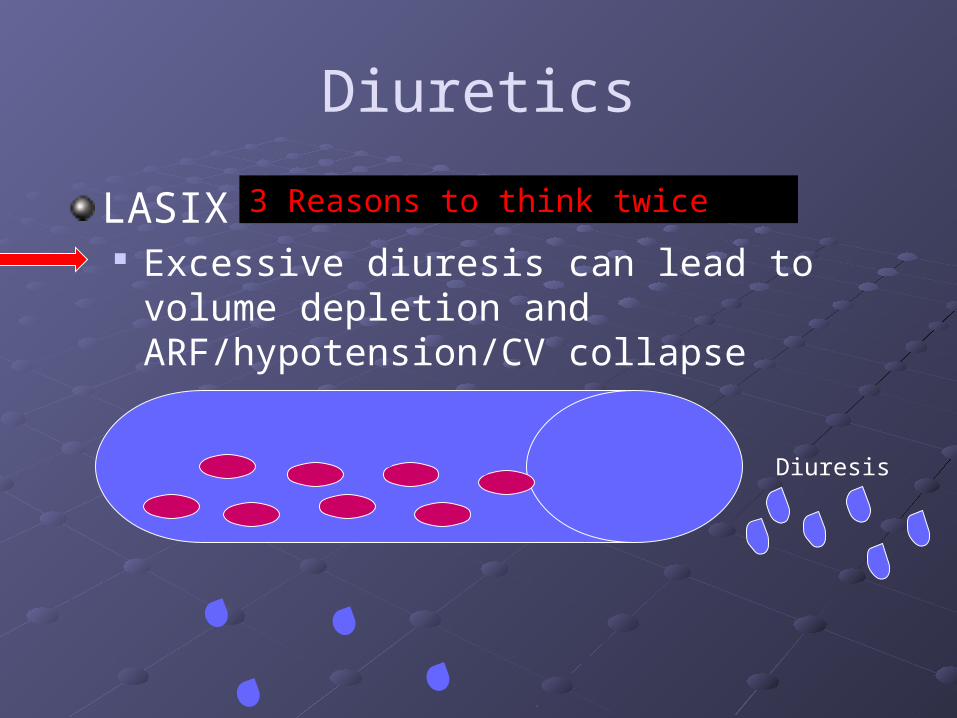
Diuretics
LASIX Excessive diuresis can lead to volume
depletion and ARF/hypotension/CV collapse
3 Reasons to think twice
Diuresis
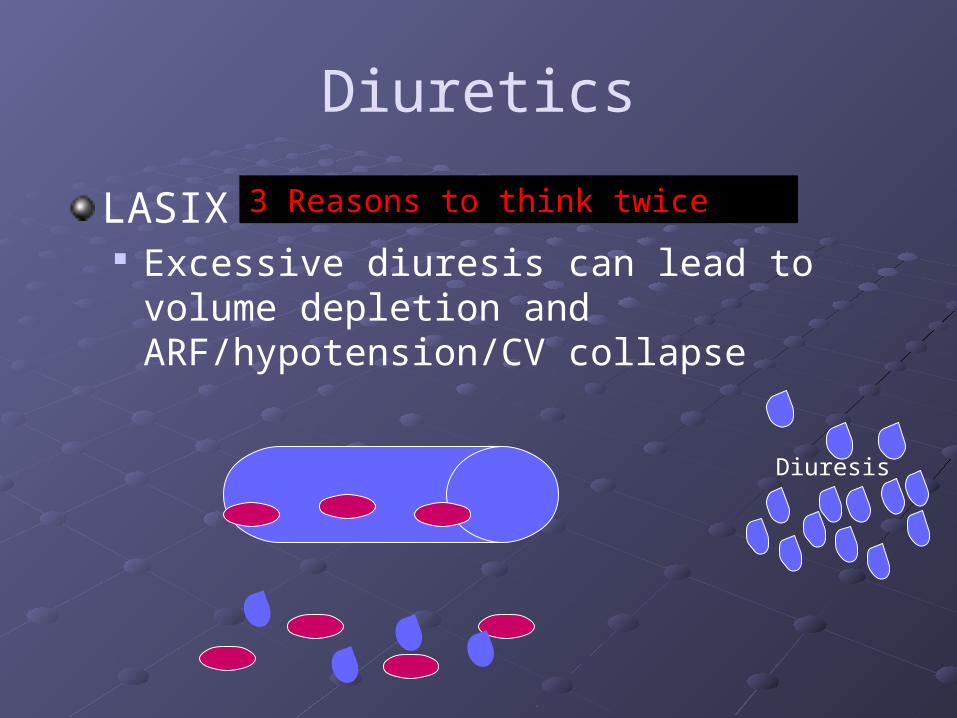
Diuretics
LASIX Excessive diuresis can lead to volume
depletion and ARF/hypotension/CV collapse
3 Reasons to think twice
Diuresis
Diuretics
LASIX Excessive diuresis can lead to volume
depletion and ARF/hypotension/CV collapse Can exacerbate calcium based kidney stones Can cause hypokalemia, metabolic alkalosis
3 Reasons to think twice
Diuretics
Class Site Effect Use Side Fx
Thiazides
Loop
K Sparing
Other
TAL
NaK2Cl
Impairs dilution and concentration
Acute overload, edema, ↑Ca/K
↓serum K, Met Alkalosis, Volume Depletion, ↑U Ca

Diuretics
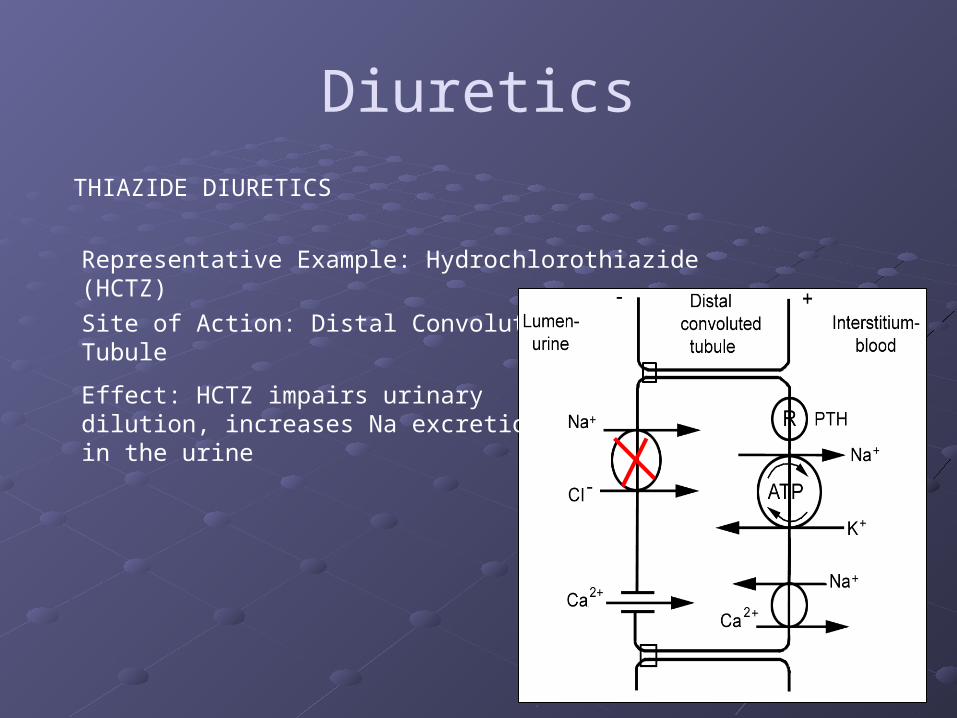
THIAZIDE DIURETICS
Representative Example: Hydrochlorothiazide (HCTZ)
Onset of action: roughly 2 hours
Duration: 6-12 hours
Factoid: In April of 2005, Hydrochlorothiazide was nominated as one of the “most intimidating medication names.”Less effective at GFR < 40
Diuretics
THIAZIDE DIURETICS
Representative Example: Hydrochlorothiazide (HCTZ)
Site of Action: Distal Convoluted Tubule Factoid: In April of 2005, Hydrochlorothiazide was nominated as one of the “most intimidating medication names.”Effect: HCTZ impairs urinary dilution,
increases Na excretion in the urine
Regulation of Urine Content
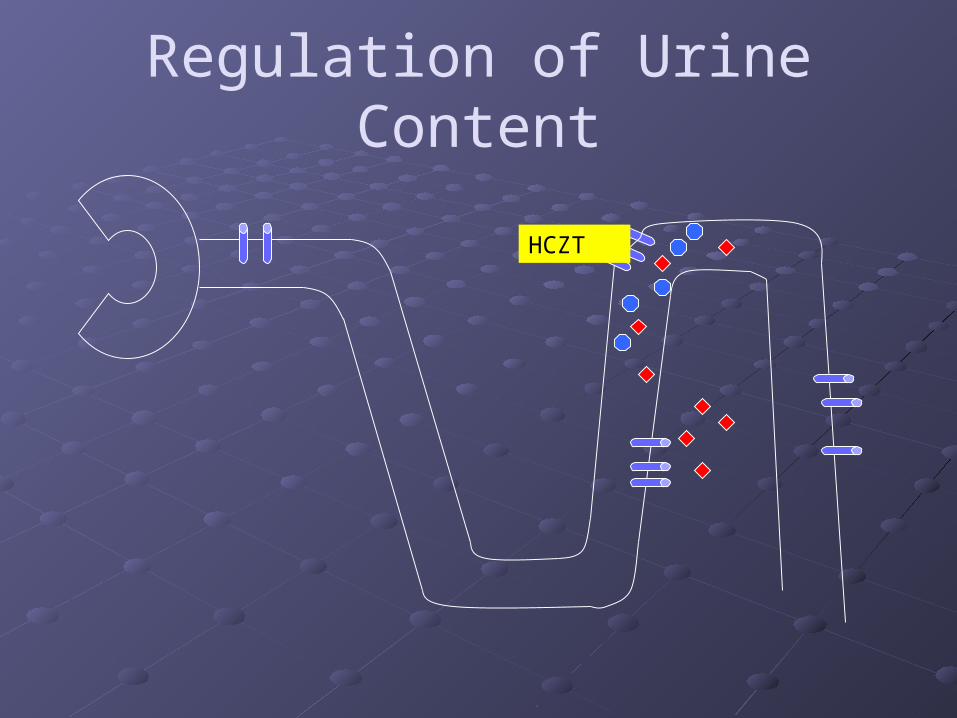
Regulation of Urine Content
HCZT

Regulation of Urine Content
ADH
HCZT
Thiazide Diuretics:
1. Impair Dilution, leading to excretion of salt and water
2. Do not disrupt the concentrating mechanism

Question 3
Why are patients on thiazides more prone to hyponatremia than those on loop diuretics?
A. Thiazides provide greater natriuretic effect than loop diuretics
B. Trick question: They both equally predispose patients to hyponatremia
C. Loop diuretics impair renal urine concentration and dilution, whereas thiazides impair only urine dilution
D. By increasing delivery of salt to the collecting duct, thiazide diuretics increase the drive for free water absorption, leading to hyponatremia
DiureticsHow do I choose between a loop diuretic and a thiazide diuretic?
Similarities:
Both will make you pee
Both can result in hypokalemia and metabolic alkalosis
Both can be used for edema and HTN
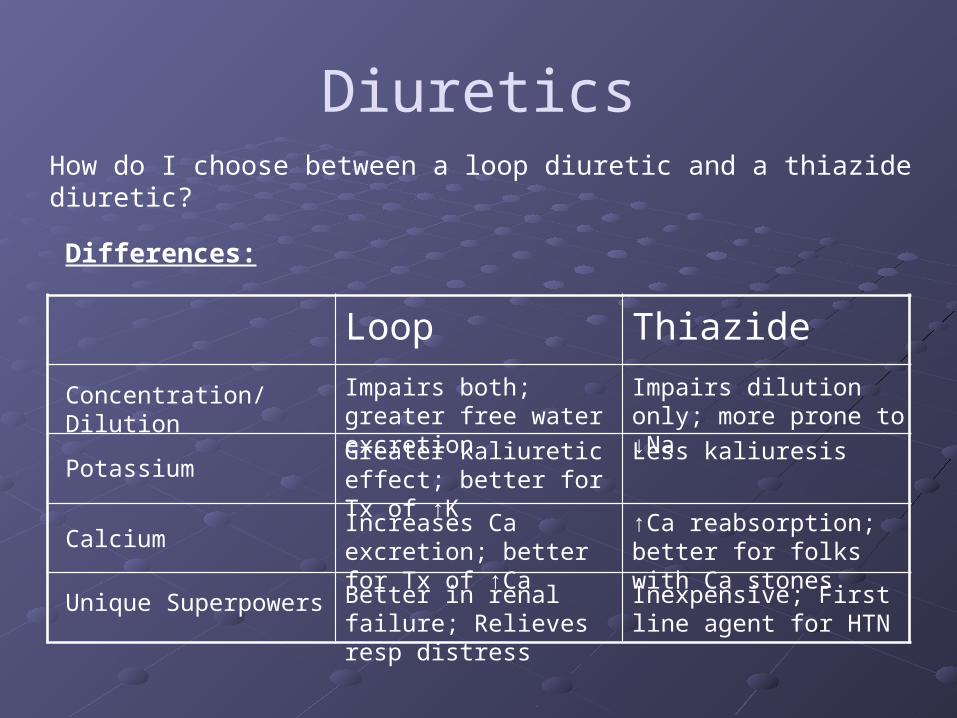
DiureticsHow do I choose between a loop diuretic and a thiazide diuretic?
Differences:
Loop Thiazide
Concentration/Dilution Impairs both; greater free water excretion
Impairs dilution only; more prone to ↓Na
PotassiumGreater kaliuretic effect; better for Tx of ↑K
Less kaliuresis
CalciumIncreases Ca excretion; better for Tx of ↑Ca
↑Ca reabsorption; better for folks with Ca stones
Unique Superpowers Better in renal failure; Relieves resp distress
Inexpensive; First line agent for HTN
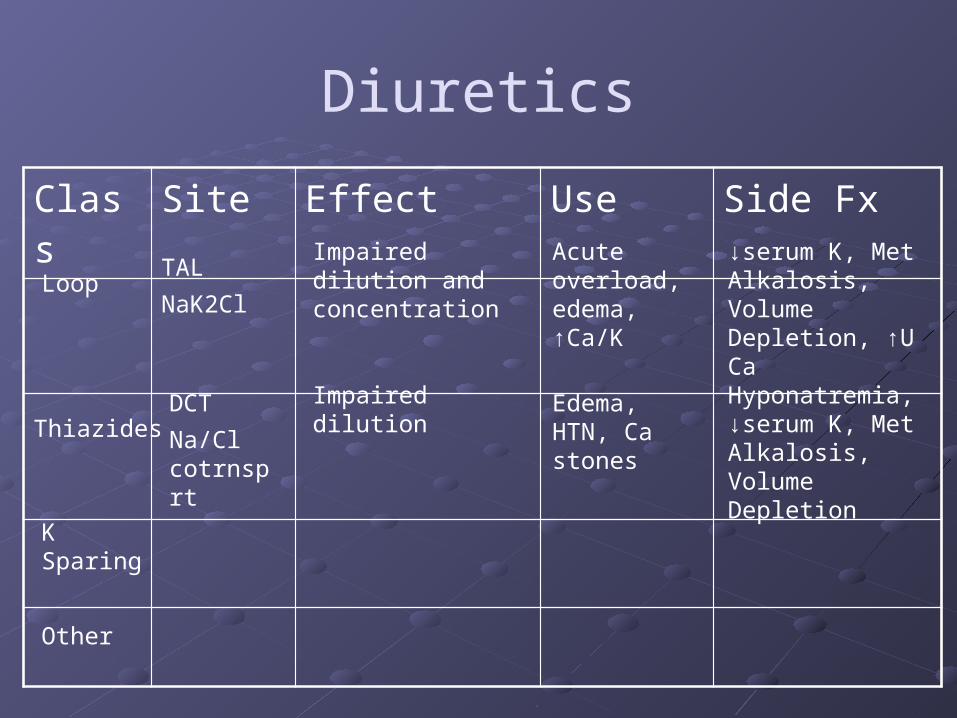
Diuretics
Class Site Effect Use Side Fx
Thiazides
Loop
K Sparing
Other
TAL
NaK2Cl
Impaired dilution and concentration
Acute overload, edema, ↑Ca/K
↓serum K, Met Alkalosis, Volume Depletion, ↑U Ca
DCT
Na/Cl cotrnsprt
Impaired dilution Edema, HTN, Ca stones
Hyponatremia, ↓serum K, Met Alkalosis, Volume Depletion
K-Sparing Diuretics
1. Aldosterone Antagonists
Representative Example: Spironolactone
Site of Action: Cortical Collecting Duct
Mechanism: Competes with aldosterone receptor
Pharmacokinetics: Can take between 10-48 hours to reach maximal efficacy
Factoid:
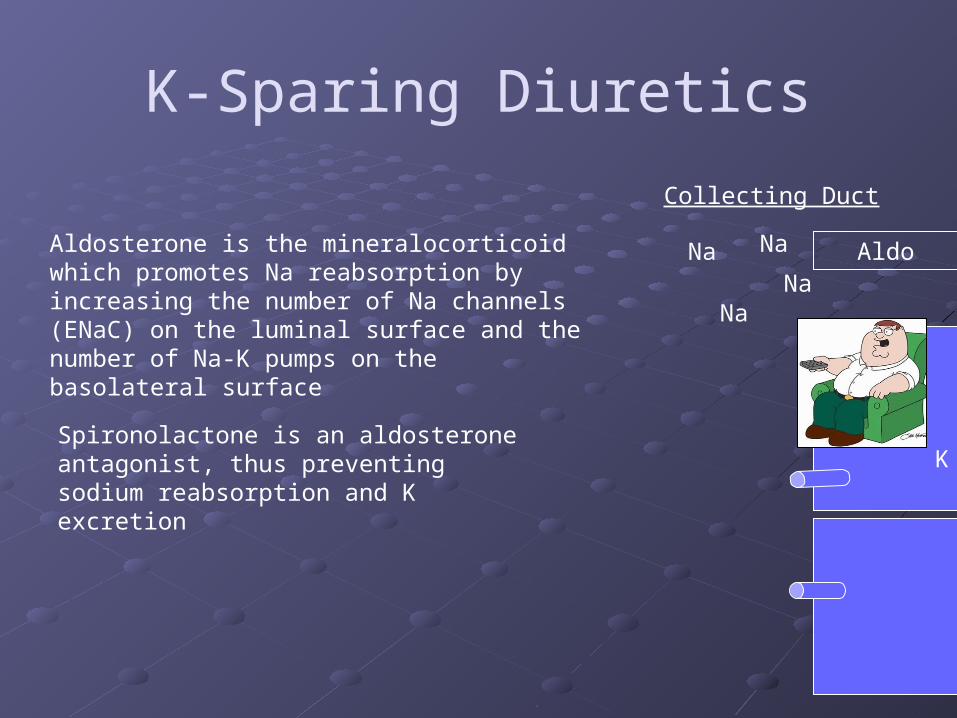
If Peter Griffin (Family Guy) was on a diuretic it would probably be spironolactone, which would account for his gynecomastia
K-Sparing Diuretics
Collecting Duct
Na Na
NaNa
K
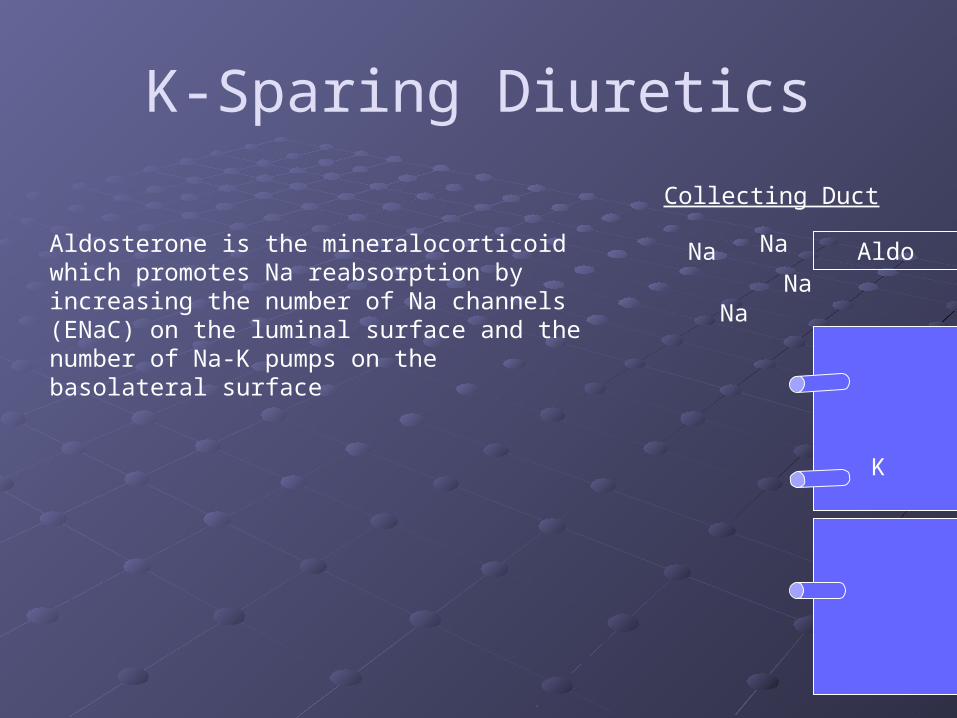
Aldosterone is the mineralocorticoid which promotes Na reabsorption by increasing the number of Na channels (ENaC) on the luminal surface and the number of Na-K pumps on the basolateral surface
Aldo
K-Sparing Diuretics
Collecting Duct
Na Na
NaNa
Aldosterone is the mineralocorticoid which promotes Na reabsorption by increasing the number of Na channels (ENaC) on the luminal surface and the number of Na-K pumps on the basolateral surface
Aldo
Spironolactone is an aldosterone antagonist, thus preventing sodium reabsorption and K excretion
K
K Sparing DiureticsThere’s more to aldosterone than meets the eye…
There are mineralocorticoid receptors in the heart as well
Local production of aldosterone in the heart is proportional to degree of heart failure
Aldosterone may stimulate cardiac fibrosis and hypertrophy (Bad)
Aldosterone Antagonists may be particularly beneficial in the long term management of certain patients with heart failure

K Sparing Diuretics Despite being a weaker diuretic, aldosterone
antagonists have a greater effect in cirrhotics than lasix!
Cirrhotic patients have a poor response to lasix due to their low albumin state and reduced tubular secretion.
Aldosterone antagonists do not require secretion into the tubular lumen, and thus may remain effective despite marginal renal perfusion in the context of cirrhosis
K-sparing Diuretics
2. ENaC Blockers
Representative Example: Amiloride, triamterene
Site of action: Corical collecting duct
Mechanism: Blocks ENaC channels
Pharmacokinetics: Half-life = 3-5 hours
Factoid:
Amiloride was first approved for use in 1967, the same year that Thurgood Marshall was sworn in as the first African American justice of the Supreme Court
Spares potassium by decreasing the lumen-negative gradient that drives the exulsion of K/H into the lumen
K-Sparing Diuretics
Collecting Duct
Na Na
NaNa
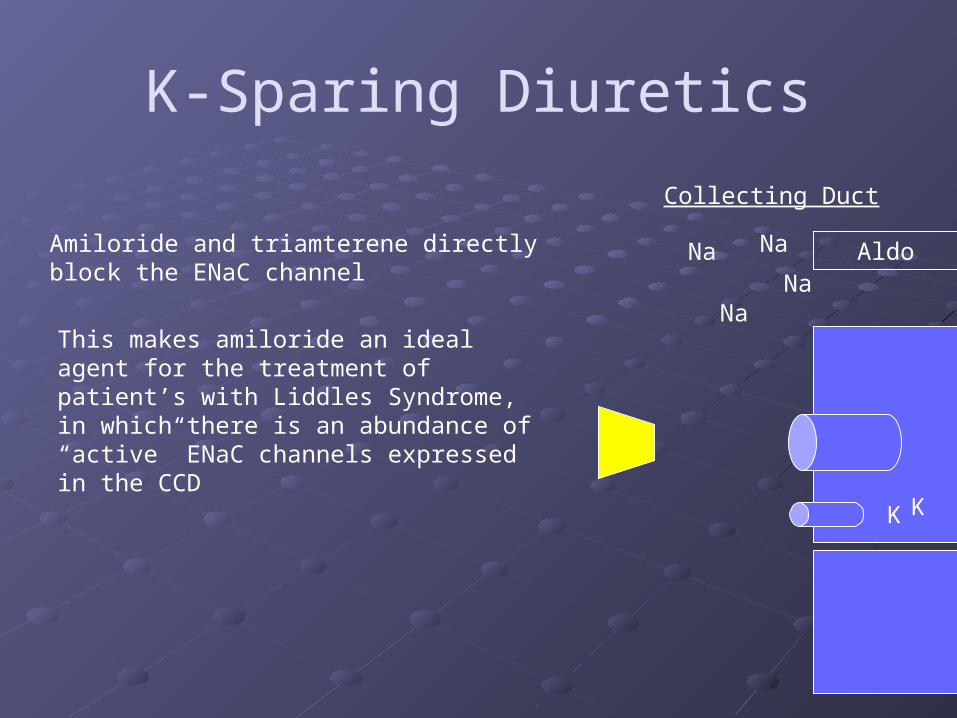
Amiloride and triamterene directly block the ENaC channel
Aldo
This makes amiloride an ideal agent for the treatment of patient’s with Liddles Syndrome, in which there is an abundance of “active” ENaC channels expressed in the CCD
K K
K-Sparing Diuretics
Collecting Duct
Li
Li
Li
Li
Li
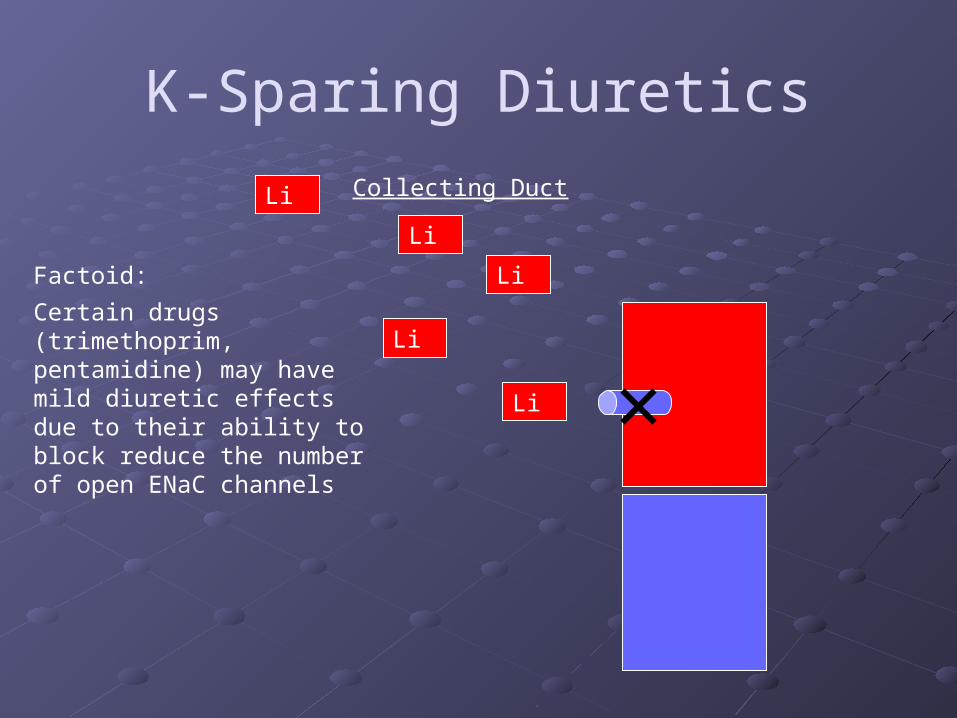
Factoid:
Certain drugs (trimethoprim, pentamidine) may have mild diuretic effects due to their ability to block reduce the number of open ENaC channels
Question 4
A young bipolar patient with AIDS is seen in clinic. He was recently hospitalized and treated for PCP pneumonia with high doses of Bactrim (trimethoprim sulfamethoxazole). He also takes lithium and a cocktail of antiretroviral drugs. Since the completion of his antibiotic, the patient states that his breathing has improved dramatically, but he notes that he is always thirsty and has urine output of Gaussian proportions.
Question 4 (cont)
The intern blows this off, but since you’ve read this syllabus you hypothesize that…
A. Accumulation of TMX has led to nephrogenic DI B. The patient may have lithium-induced nephrogenic
DI because Bactrim increases the open Na channels available for Li entry into cells
C. The patient may have psychogenic polydipsia and worsening mania due to decreased absorption of lithium during treatment with Bactrim
D. Amiloride my alleviate his symptoms.
Diuretics
Class Site Effect Use Side Fx
Thiazides
Loop
K Sparing
Other
TAL
NaK2Cl
Impaired dilution and concentration
Acute overload, edema, ↑Ca/K
↓serum K, Met Alkalosis, Volume Depletion, ↑U Ca
DCT
Na/Cl cotrnsprt
Impaired dilution Edema, HTN, Ca stones
Hyponatremia, ↓serum K, Met Alkalosis, Volume Depletion
CCD Decreased distal Na reabsorption
↓K, CHF, ESLD; Li tox, Liddles
↑ serum K, gynecomastia
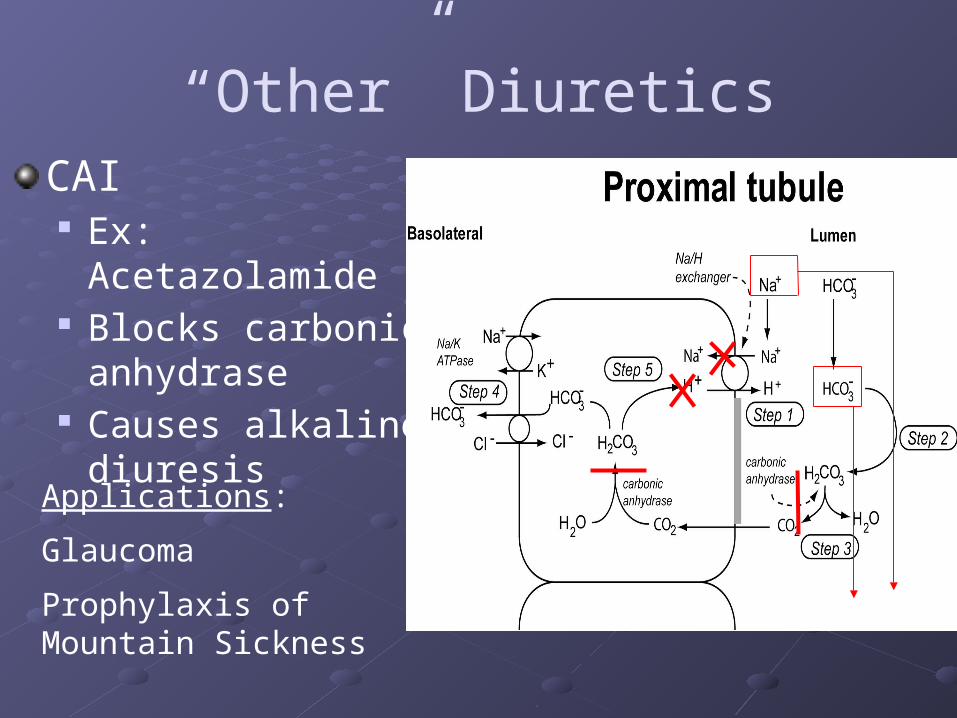
“Other” DiureticsCAI Ex: Acetazolamide Blocks carbonic
anhydrase Causes alkaline
diuresis
Applications:
Glaucoma
Prophylaxis of Mountain Sickness

“Other” Diuretics
Osmotic Diuretics Ex: Mannitol Non-reabsorbable polysaccharide Preferential water diuresis
The net effect is akin to putting SpongeBob Squarepants in the lumen of the renal tubule.
Final thoughts
Rebound The kidney is a master at compensation In the absence of salt restriction, the kidney
will adapt to the effect of the diuretic After an initial diuresis, further natriuresis will
be blunted by post-diuretic salt retention Salt restriction is, thus, crucial to continued
diuresis

Downstream Compensation
ADH
LAS I X
As the kidney is an awfully smart fellow, it may try to restore steady-state Na status by increasing reabsorption distal to the site of diuretic action
The addition of a “downstream” diuretic (in this case, something that blocks the distal tubule) will prevent the kidney from reclaiming Na and water
Fortune Cookie:“To fool the kidney, you must think like the kidney”

Clinical Scenarios
For each of the following clinical scenarios, pick the appropriate diuretic: A. Loop B. Thiazide C. Aldosterone Antagonist D. ENaC Inhibitor E. The square root of Misler/(1.73x Kukla)
Clinical Scenarios 60 year old with history of myocardial infarction presents to ER with sudden onset shortness of breath after participating in regional pickle eating contest
Too winded to speak in full sentences
Crackles/Rales on exam, 2+ LE edema, Oxygen Saturation 74% on 5L O2
LASIX
Why? Rapid onset of diuresis, +Pulmonary edema
Result? Symptomatic relief, avoidance of intubation and mechanical ventilation
Clinical Scenarios 48 year old man seen in clinic after experiencing exquisite pain in groin last week. Passed the following Ca-based stone with urination.
Noted to have BP 153/80
Thiazide
Why? HTN, Ca-based stone
Result? Decrease risk for future stone formation, reduce BP, decrease risk of cardiovascular complications/death due to HTN
Clinical Scenarios 12 year old with a strong family history of HTN, noted to have a BP of 188/60. Has been treated with thiazides, beta-blockers, ACE-inhibitors without BP control. Labs show a serum K of 3.1, bicarb of 32.
ENaC Inhibitor
Why? Suspicion of Liddle’s (family history, HTN, low K, metabolic alkalosis)
Result? Reduced blood pressure, decrease in cardiovascular risk from HTN

Clinical Scenarios 63 year old with a history of CHF. Edema is managed with dietary restriction of Na and a loop diuretic, but patient still occasionally short of breath with minimal exertion. Is in clinic for follow up and management of his heart failure.
Aldosterone Antagonist
Why? Class III-IV HF
Result? Decreased mortality at 16-24 months
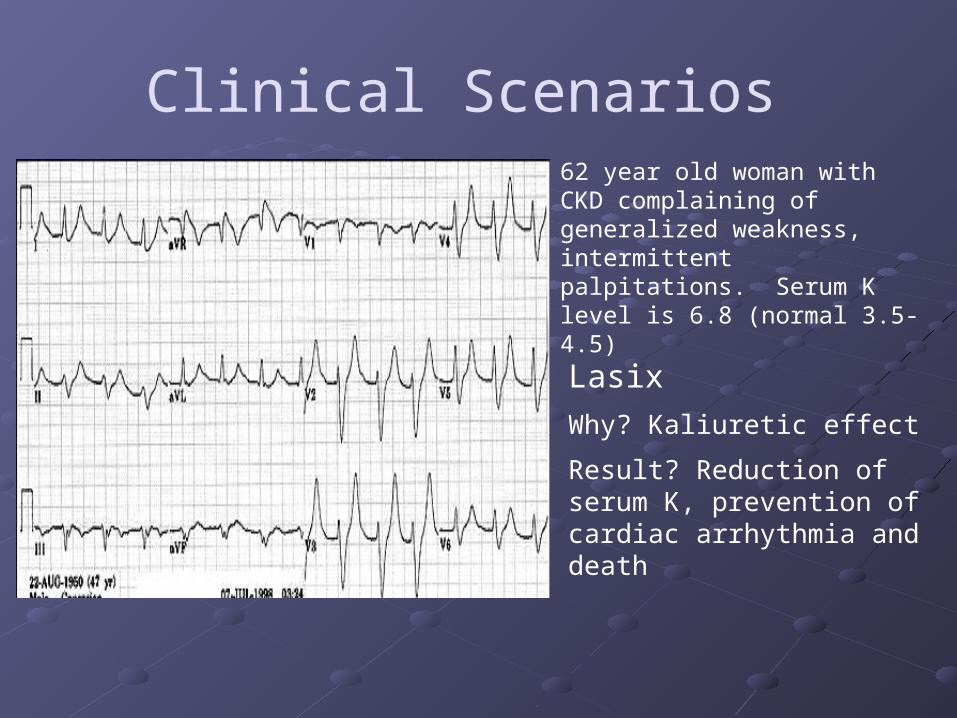
Clinical Scenarios 62 year old woman with CKD complaining of generalized weakness, intermittent palpitations. Serum K level is 6.8 (normal 3.5-4.5)
Lasix
Why? Kaliuretic effect
Result? Reduction of serum K, prevention of cardiac arrhythmia and death
Clinical Scenarios 69 year old man presents with back pain and anemia. Is found to have Ca 11.6 mg/dL. In addition to hydration with NS and the diagnosis of Multiple Myeloma, what diuretic should be given?
Lasix
Why? Increase Ca excretion
Result? Reduce serum Ca, prevent cardiac, renal, neurologic, musculoskeletal complications of hypercalcemia.

Clinical Scenarios Iron Chef Morimoto shows up in your clinic for a routine check up. He has no significant past medical history. His renal function in intact. Electrolytes are stable. BP is 153/87
Thiazide
Why? Essential HTN
Result? Reduction of future cardiovascular risk, many more years of dominance on “The Iron Chef.”
Clinical Scenarios 47 year old with chronic hepatitis and cirrhosis. Has noted increasing abdominal girth over the last several days despite treatment with Lasix. Serum K is 3.2 (normal 3.5-4.5)
Aldosterone Antagonist
Why? Hypokalemia, improved volume removal in a cirrhotic patient
Result? Mild alleviation of volume retention, improvement in serum K.
Clinical Scenarios The previous patient has a slight improvement in edema and ascites. However, after three days she develops worsening renal function. What could have happened?
Recommended