Diabetic Nephropathy
Diabetic Nephropathy A clinical syndrome
DM +DM +
Persistent albuminuria, Worsening Persistent albuminuria, Worsening proteinuria, Hypertension & proteinuria, Hypertension &
progressive renal failureprogressive renal failure
Diabetic nephropathy (DN) is a Diabetic nephropathy (DN) is a majormajor
cause of ESRD, and the incidence of cause of ESRD, and the incidence of diabetesdiabetes
mellitus is rising rapidly.mellitus is rising rapidly.

Objectives
Prevalence of diabetic kidney diseasePrevalence of diabetic kidney disease Pathogenesis of diabetic nephropathyPathogenesis of diabetic nephropathy Clinical course of diabetic nephropathyClinical course of diabetic nephropathy Slowing the progression of nephropathySlowing the progression of nephropathy Screening for early nephropathyScreening for early nephropathy
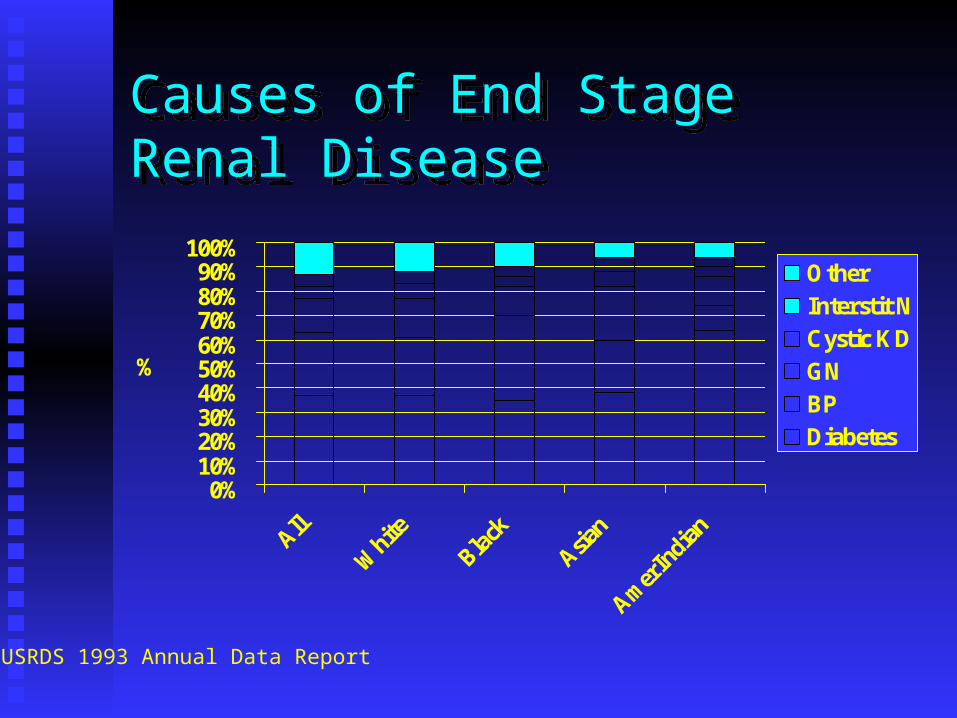
Causes of End Stage Renal DiseaseCauses of End Stage Renal Disease
0%10%20%30%40%50%60%70%80%90%
100%
%
OtherInterstit NCystic KDGNBPDiabetes
USRDS 1993 Annual Data Report
Diabetic Nephropathy The most common cause of ESRD in USA.The most common cause of ESRD in USA.
However one needs to keep in mind all diabetic However one needs to keep in mind all diabetic patients with ESRD do not have DN as underlying patients with ESRD do not have DN as underlying cause of ESRD. cause of ESRD.
Diabetic Nephropathy Mortality of ESRD patients with Diabetes Mellitus Mortality of ESRD patients with Diabetes Mellitus
is higher than in ESRD patients without Diabetes.is higher than in ESRD patients without Diabetes.
This higher mortality is due to increase in This higher mortality is due to increase in Cardiovascular, cerebro-vascular, peripheral Cardiovascular, cerebro-vascular, peripheral vascular and infection related morbidity.vascular and infection related morbidity.
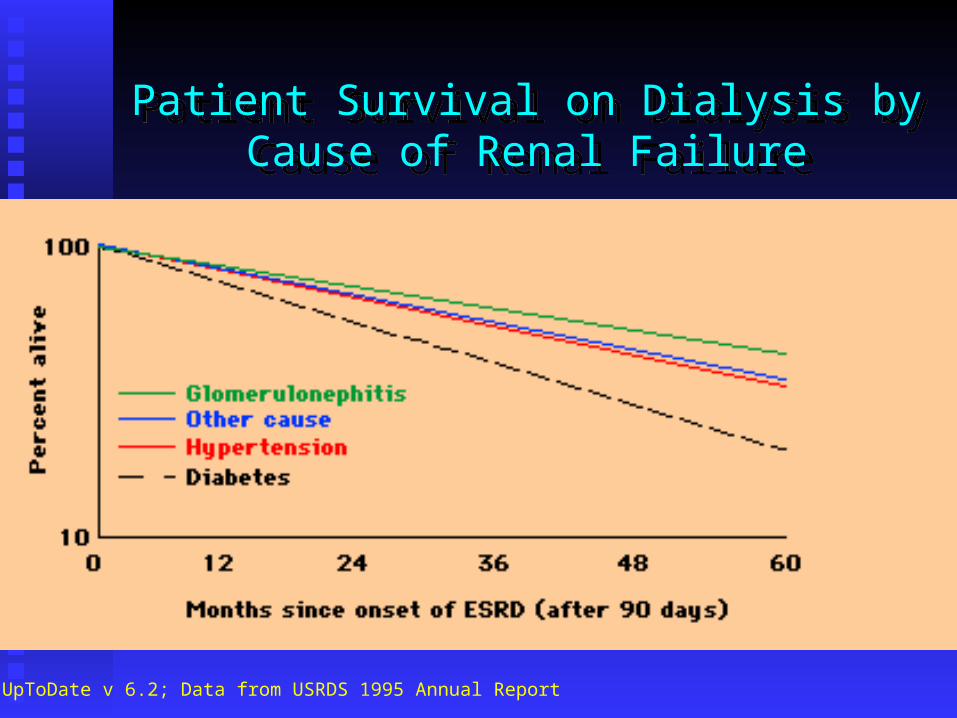
Patient Survival on Dialysis by Cause of Renal Failure
Patient Survival on Dialysis by Cause of Renal Failure
From UpToDate v 6.2; Data from USRDS 1995 Annual Report
Diabetic Nephropathy DN occurs in 35-40% of patients with type I DN occurs in 35-40% of patients with type I
diabetes (IDDM) whereas it occurs only in 15-diabetes (IDDM) whereas it occurs only in 15-20% of patients with type II diabetes (NIDDM).20% of patients with type II diabetes (NIDDM).
Definition or Criteria for diagnosis of DNDefinition or Criteria for diagnosis of DN Presence of persistent proteinuria in sterile urine of Presence of persistent proteinuria in sterile urine of
diabetic patients with concomitant diabetic retinopathy diabetic patients with concomitant diabetic retinopathy and hypertension.and hypertension.
D.N.- Pathogenesis Familial - Genetic Familial - Genetic
Only 35-40% patients with IDDM develop DN.Only 35-40% patients with IDDM develop DN.
There is an increased risk of DN in a patient with There is an increased risk of DN in a patient with family member having DN.family member having DN.
D.N.- Pathogenesis Glycemic Control-in both expt & humanGlycemic Control-in both expt & human
DN does not occur in euglycemic patients.DN does not occur in euglycemic patients.
Confirmed role of hyperglycemia in pathogenesis Confirmed role of hyperglycemia in pathogenesis of DN.of DN.
Renal transplant with early DN showed structural Renal transplant with early DN showed structural recovery in euglycemic receipient. (Abouna)recovery in euglycemic receipient. (Abouna)
Strict Glycemic Control Prevents
Microalbuminuria in Type 1 Diabetes mellitus
Strict Glycemic Control Prevents
Microalbuminuria in Type 1 Diabetes mellitus
From UpToDate v 6.2; Data from the DCCT Research Group, NEJM(1993) 329:977.
D.N.- Pathogenesis Glomerular Glomerular HyperfiltrationHyperfiltration Glomerular Glomerular HypertensionHypertension Glomerular Glomerular HypertrophyHypertrophy GBM thickeningGBM thickening Mesangial ExpansionMesangial Expansion
D.N.- Pathogenesis
Renal lesions mainly related to Renal lesions mainly related to extracellular matrix accumulationextracellular matrix accumulation
- Occurs in glomerular & tubular basement - Occurs in glomerular & tubular basement
membranemembrane
- - Principal cause of mesangial expansionPrincipal cause of mesangial expansion
D.N.- Pathogenesis
Extracellular matrix accumulationExtracellular matrix accumulation
- Imbalance between synthesis & degradation of - Imbalance between synthesis & degradation of
ECM componentsECM components
- Linkage between glucose concentration & ECM - Linkage between glucose concentration & ECM
accumulationaccumulation
- - Transforming growth factor-Beta associated withTransforming growth factor-Beta associated with
increased production of ECM molecules increased production of ECM molecules
D.N.- Pathogenesis
Extracellular matrix accumulationExtracellular matrix accumulation
- TGF-B can down regulate synthesis of ECM- TGF-B can down regulate synthesis of ECM
degrading enzymes & upregulate inhibitors ofdegrading enzymes & upregulate inhibitors of
these enzymesthese enzymes
- - Angiotensin II can stimulate ECM synthesis Angiotensin II can stimulate ECM synthesis
through TGF-B activity through TGF-B activity
- Hyperglycemia activates protein kinase C,- Hyperglycemia activates protein kinase C,
stimulating ECM production through cyclic AMPstimulating ECM production through cyclic AMP
PathwayPathway
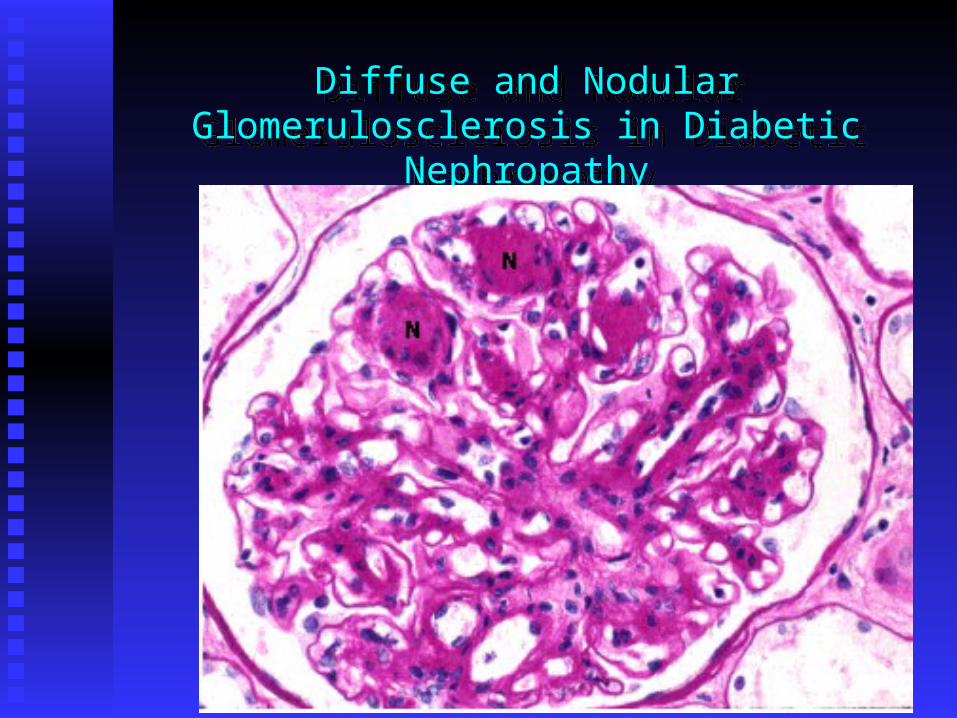
Diffuse and Nodular Glomerulosclerosis in Diabetic Nephropathy
Diffuse and Nodular Glomerulosclerosis in Diabetic Nephropathy
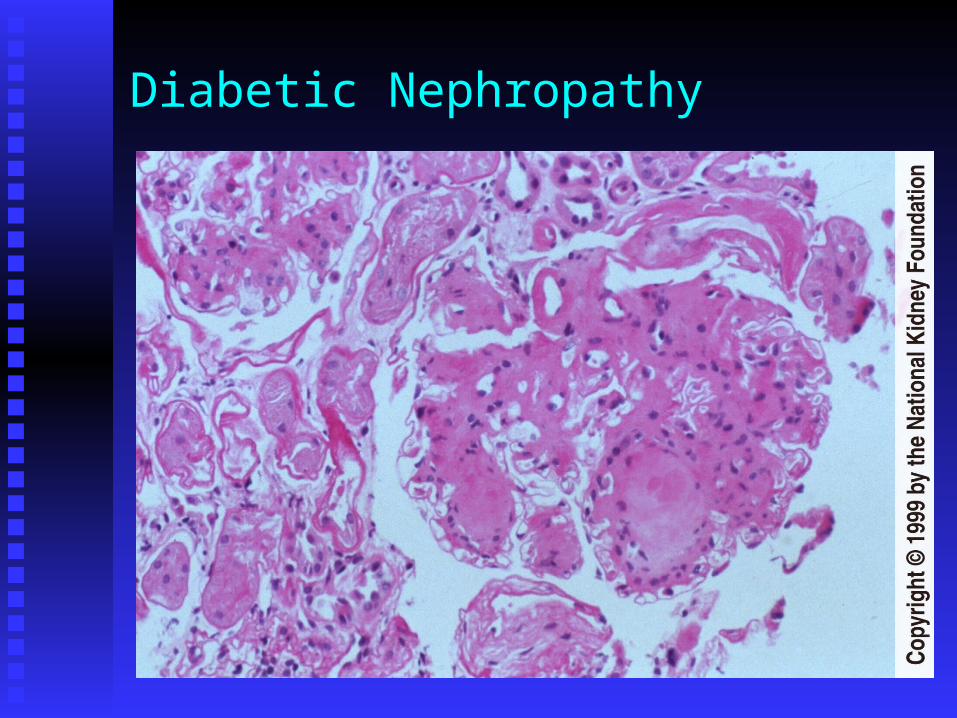
Diabetic Nephropathy
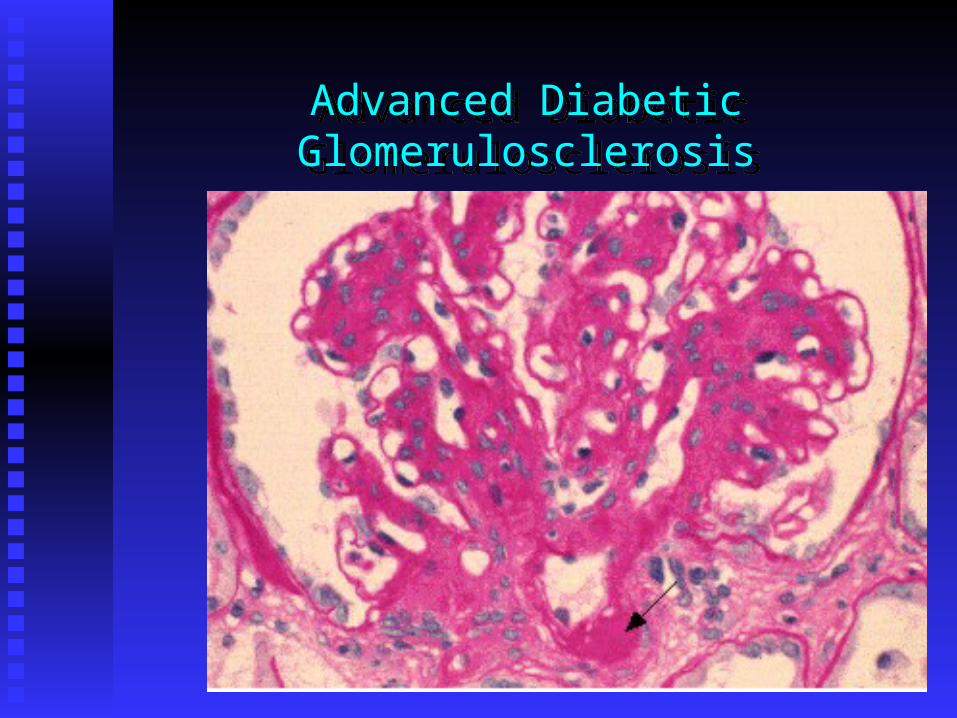
Advanced Diabetic GlomerulosclerosisAdvanced Diabetic Glomerulosclerosis
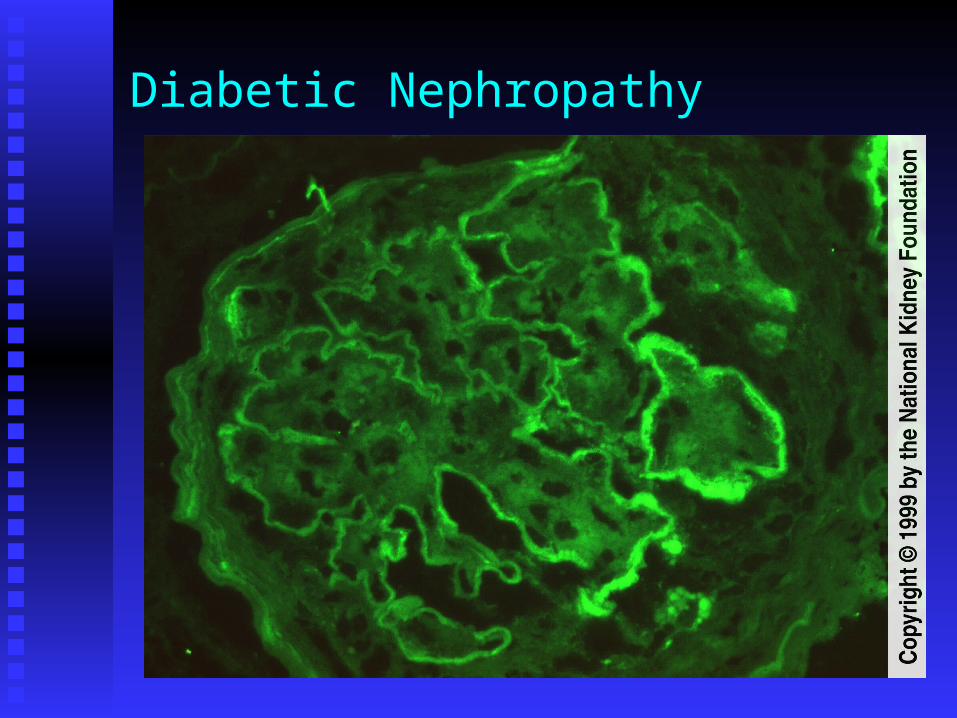
Diabetic Nephropathy
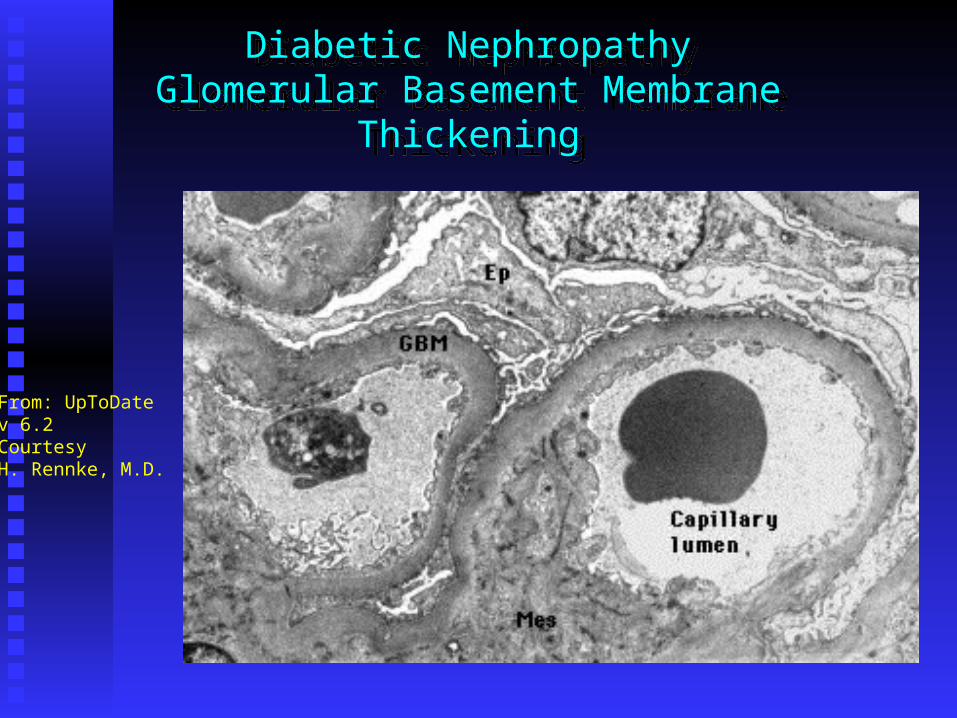
Diabetic NephropathyGlomerular Basement Membrane Thickening
Diabetic NephropathyGlomerular Basement Membrane Thickening
From: UpToDatev 6.2CourtesyH. Rennke, M.D.
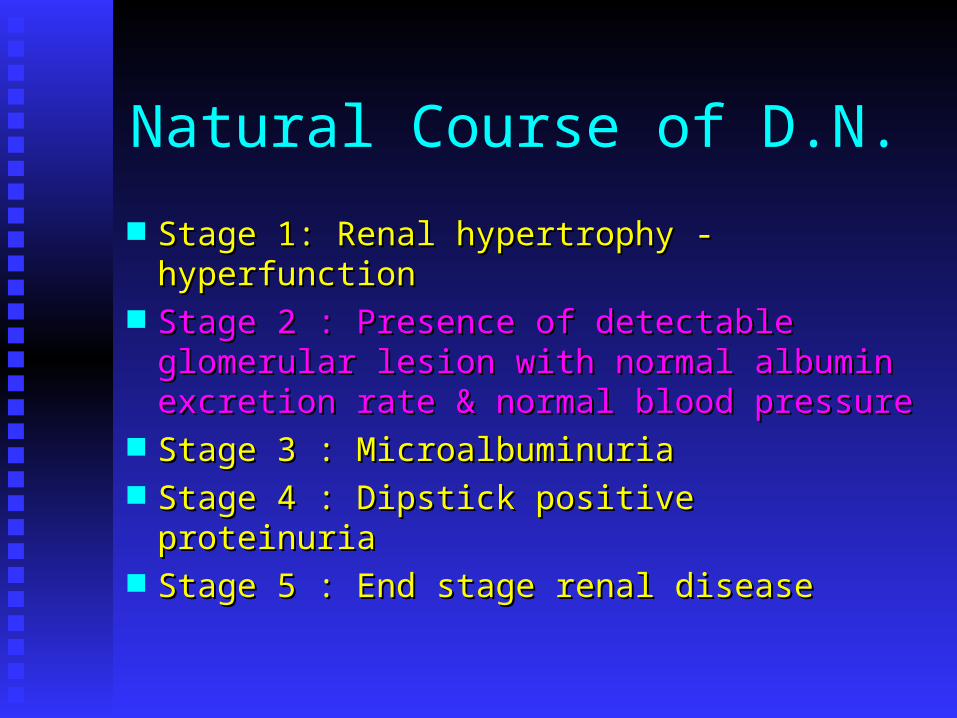
Natural Course of D.N.
Stage 1: Renal hypertrophy - hyperfunctionStage 1: Renal hypertrophy - hyperfunction Stage 2 : Presence of detectable glomerular Stage 2 : Presence of detectable glomerular
lesion with normal albumin excretion rate lesion with normal albumin excretion rate & normal blood pressure& normal blood pressure
Stage 3 : MicroalbuminuriaStage 3 : Microalbuminuria Stage 4 : Dipstick positive proteinuriaStage 4 : Dipstick positive proteinuria Stage 5 : End stage renal disease Stage 5 : End stage renal disease
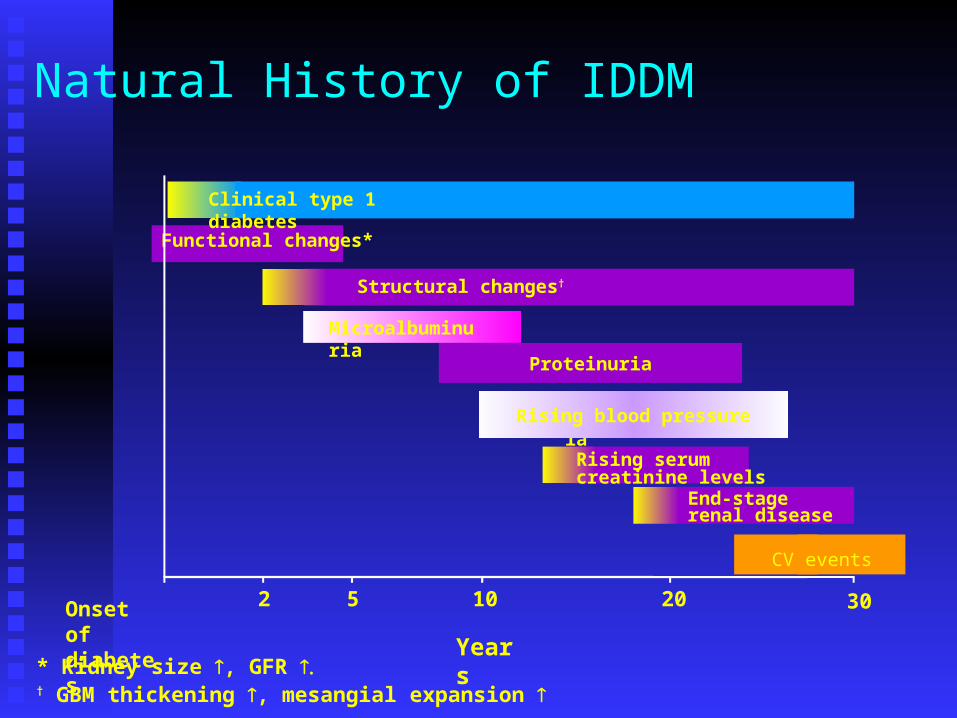
Functional changes*
Natural History of IDDM
Proteinuria
End-stage renal disease
Clinical type 1 diabetes
Structural changes†
Proteinuria
Rising serum creatinine levels
Rising blood pressure
Onset of diabetes
2 5 10 20
Years* Kidney size , GFR † GBM thickening , mesangial expansion
Microalbuminuria
30
CV events
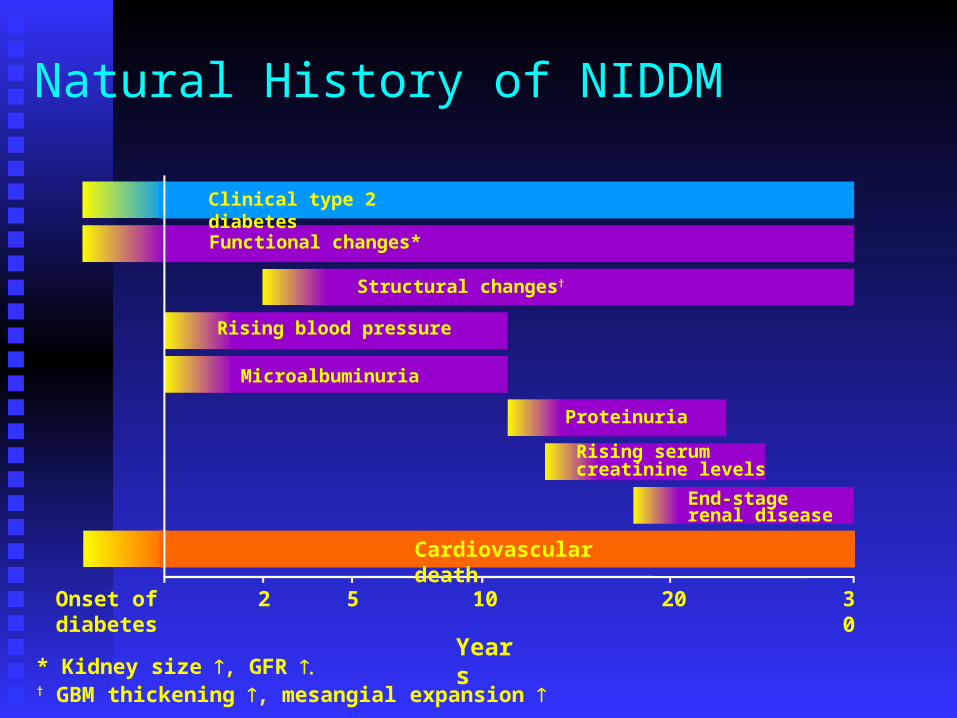
Functional changes*
Natural History of NIDDM
Proteinuria
End-stage renal disease
Clinical type 2 diabetes
Structural changes†
Rising blood pressure
Rising serum creatinine levels
Cardiovascular death
Microalbuminuria
Onset of diabetes
2 5 10 20 30
Years* Kidney size , GFR † GBM thickening , mesangial expansion
D.N.- Pathogenesis Hypertension - in both expt & humanHypertension - in both expt & human
Hypertension follows 8-10 years of hyperglycemia Hypertension follows 8-10 years of hyperglycemia in IDDM patients but it is frequently present at the in IDDM patients but it is frequently present at the diagnosis of NIDDM.diagnosis of NIDDM.
Many experimental & human studies have shown Many experimental & human studies have shown HTN accelerating progressive renal injury in DN.HTN accelerating progressive renal injury in DN.

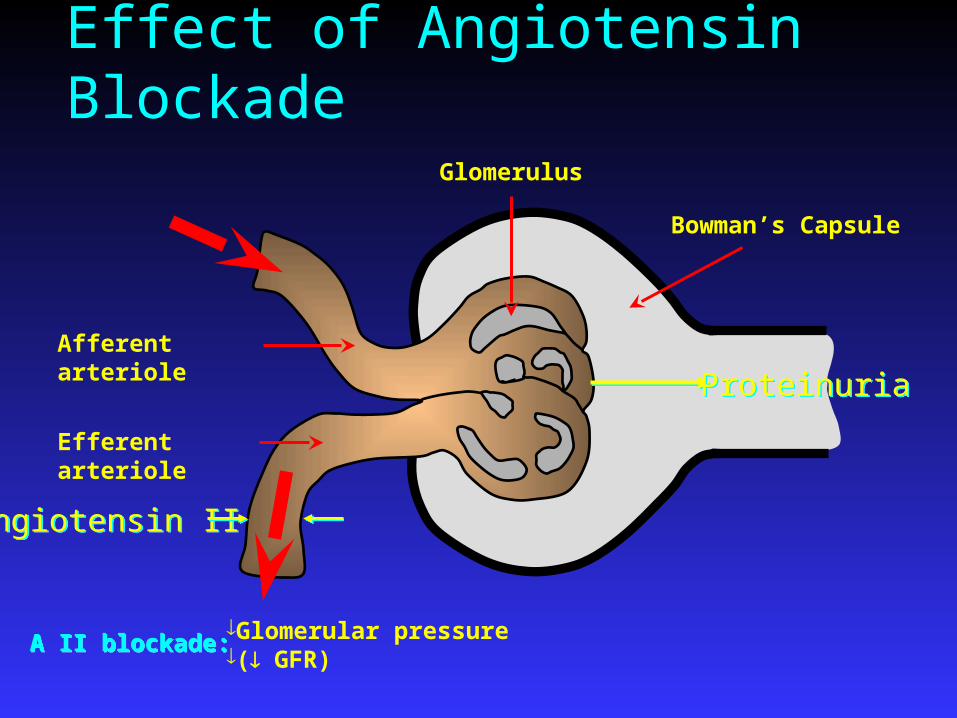
Effect of Angiotensin Blockade
Afferent arteriole
Efferent arteriole
Glomerular pressure( GFR)
Glomerulus
Bowman’s Capsule
Angiotensin IIAngiotensin II
ProteinuriaProteinuria
A II blockade:A II blockade:
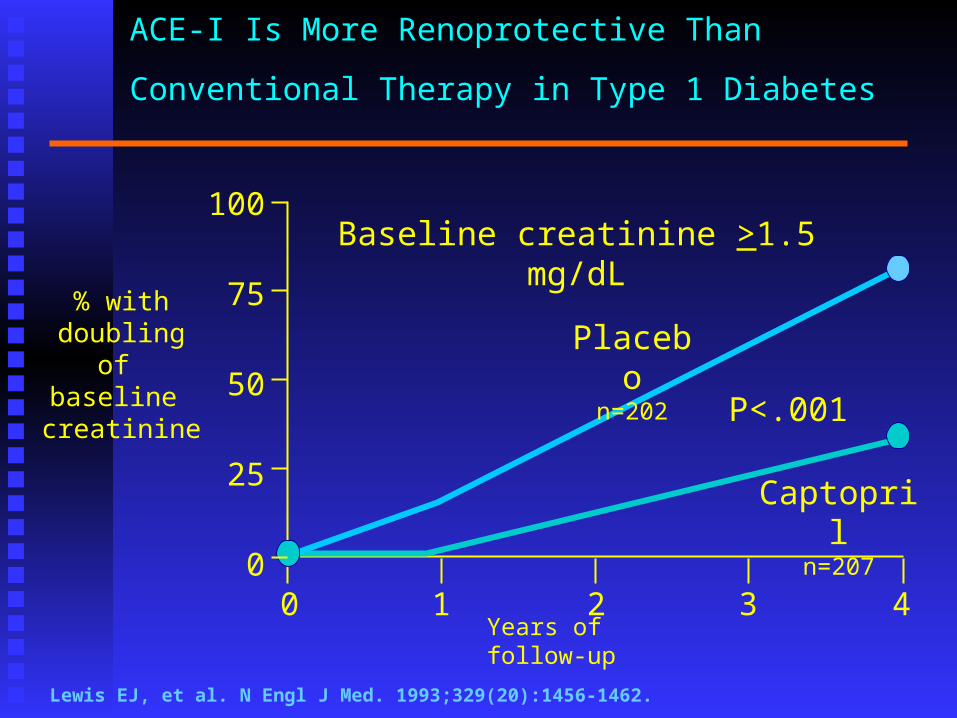
ACE-I Is More Renoprotective Than Conventional Therapy
in Type 1 Diabetes
% with doubling of
baseline creatinine
100
75
50
25
00 1 2 3 4
Baseline creatinine >1.5 mg/dL
Captopriln=207
Placebon=202
P<.001
Lewis EJ, et al. N Engl J Med. 1993;329(20):1456-1462.
Years of follow-up
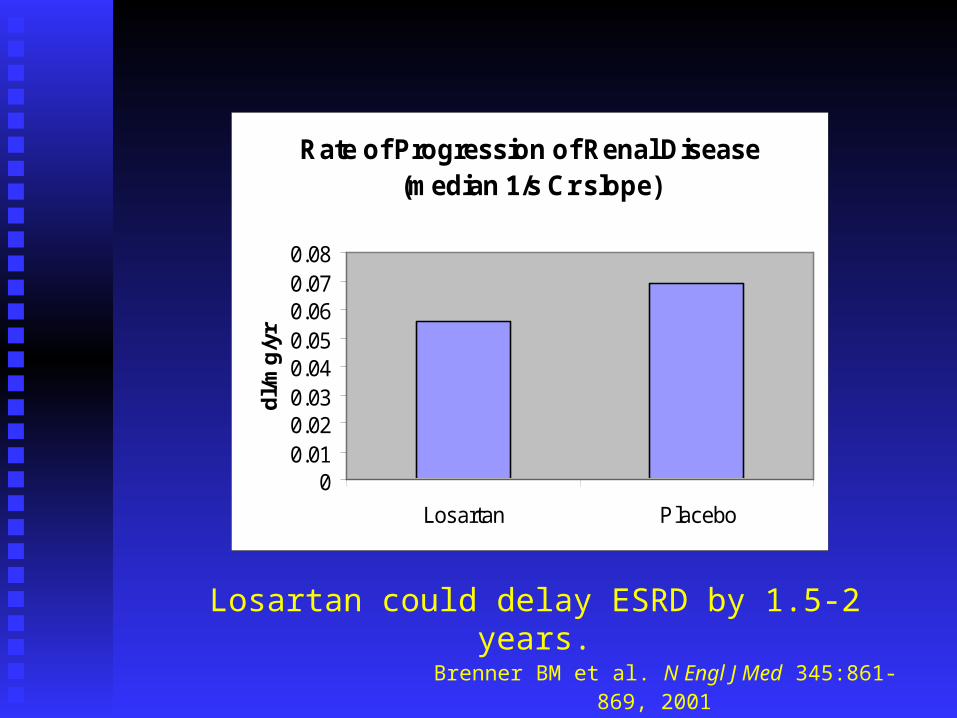
Brenner BM et al. N Engl J Med 345:861-869, 2001
Rate of Progression of Renal Disease (median 1/s Cr slope)
00.010.020.030.040.050.060.070.08
Losartan Placebo
dl/
mg
/yr
Losartan could delay ESRD by 1.5-2 years.
Irbesartan in patients with type 2 diabetes & microalbuminuria study
590 NIDDM patients with HTN and microalbuminuria 590 NIDDM patients with HTN and microalbuminuria with nearly normal GFR.with nearly normal GFR.
Randomly assigned to placebo, 150 mg or 300 mg of Randomly assigned to placebo, 150 mg or 300 mg of irbesartan for 2 years.irbesartan for 2 years.
Primary outcome was time to the onset of diabetic Primary outcome was time to the onset of diabetic nephropathy (urinary albumin excretion rate >200 nephropathy (urinary albumin excretion rate >200 mcg/min and at least 30% greater albuminuria)mcg/min and at least 30% greater albuminuria)
14.9% patients on placebo group, 9.7% of irbesartan 14.9% patients on placebo group, 9.7% of irbesartan 150mg group and 5.2% of irbesartan 300 mg group 150mg group and 5.2% of irbesartan 300 mg group reached the primary point.reached the primary point.
– (Parving et al, NEJM, 2001)(Parving et al, NEJM, 2001)
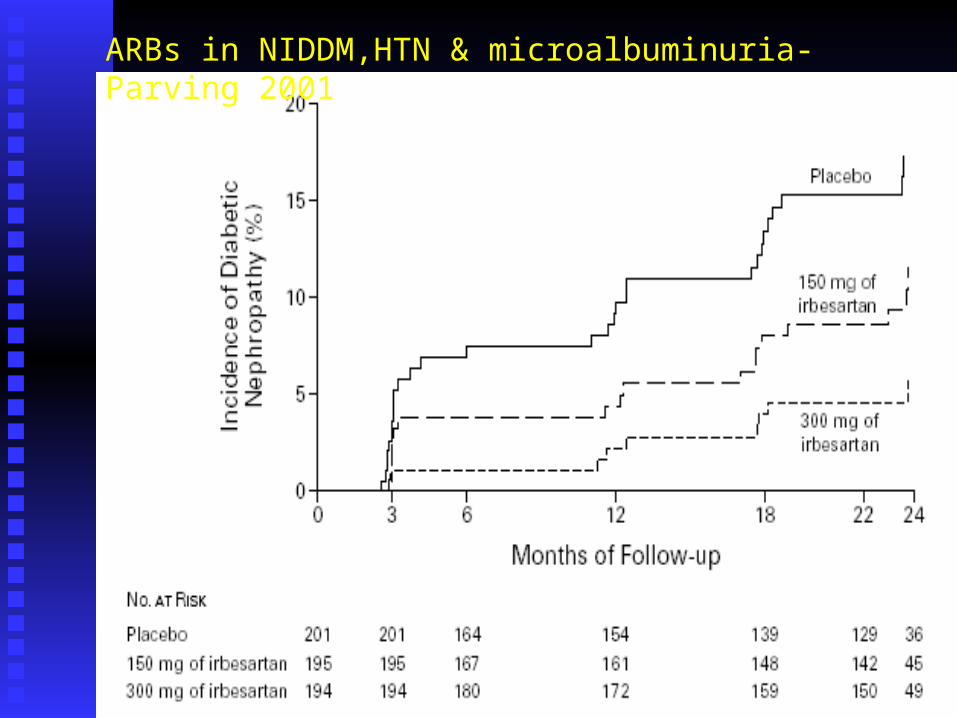
ARBs in NIDDM,HTN & microalbuminuria-Parving 2001
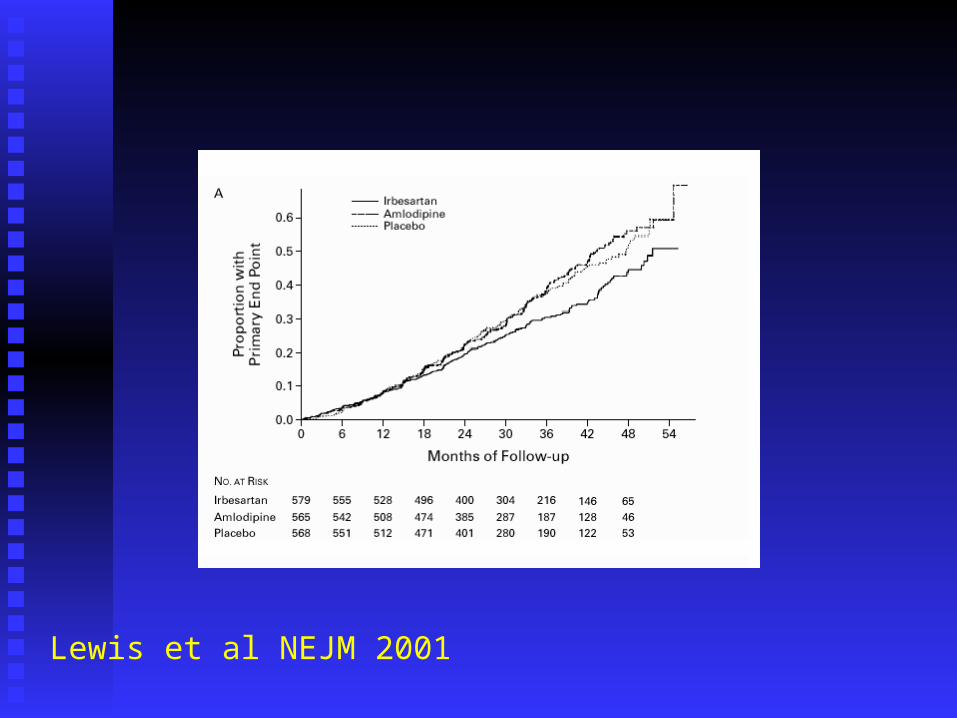
Lewis et al NEJM 2001
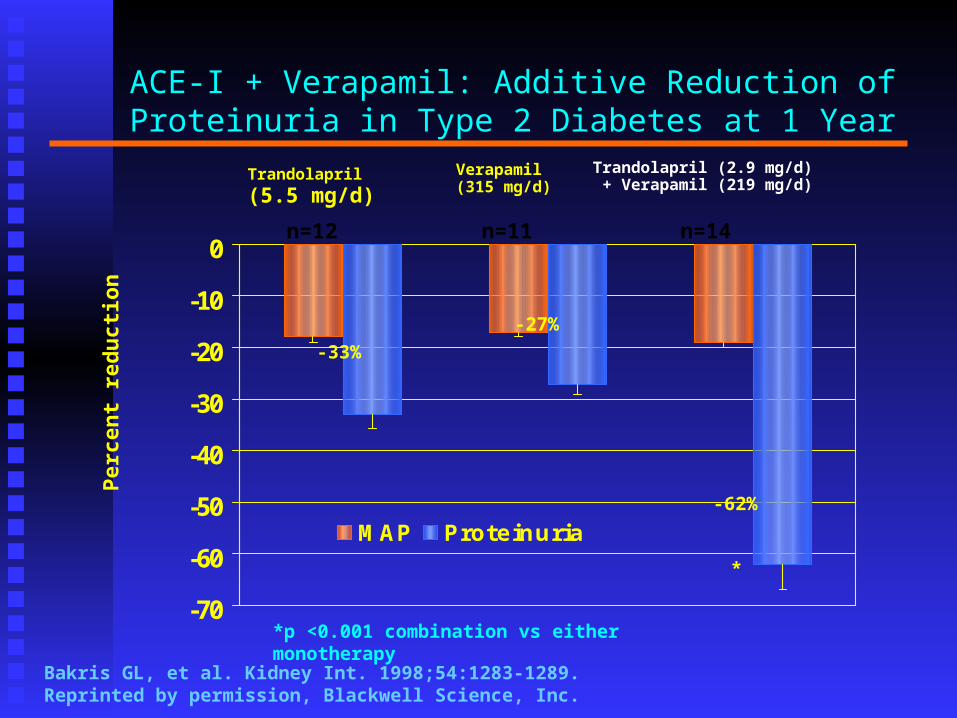
ACE-I + Verapamil: Additive Reduction of Proteinuria in Type 2 Diabetes at 1 Year
Trandolapril (5.5 mg/d)
Verapamil (315 mg/d)
Trandolapril (2.9 mg/d) + Verapamil (219 mg/d)
-70
-60
-50
-40
-30
-20
-10
0
MAP Proteinuria
*
Bakris GL, et al. Kidney Int. 1998;54:1283-1289. Reprinted by permission, Blackwell Science, Inc.
-33%
-27%
-62%
*p <0.001 combination vs either monotherapy
Perc
en
t re
du
cti
on
n=12 n=11 n=14
D.N.-Management ACEI or AII RB- in both expt & humanACEI or AII RB- in both expt & human
Reduce glomerular hypertensionReduce glomerular hypertension Reduce proteinuria independent of Reduce proteinuria independent of
hemodynamic effectshemodynamic effects Reduce glomerular hypertrophyReduce glomerular hypertrophy well tolerated apart from hyperkalemia & well tolerated apart from hyperkalemia &
worsening of anemia in severe CRFworsening of anemia in severe CRF Cautious use in presence of severe renovascular Cautious use in presence of severe renovascular
diseasedisease
DN: ADA Position Statement
Screening:
Perform an annual test for the presence of microalbuminuria in1) type 1 diabetic patients who have had diabetes > 5 years and2) all type 2 diabetics patients starting at diagnosis.
Treatment:
• In the treatment of albuminuria/nephropathy both ACE inhibitors and ARBs can be used:
• In hypertensive and nonhypertensive type 1 diabetic patients with microalbuminuria or clinical albuminuria, ACE inhibitors are the initial agents of choice
• In hypertensive type 2 diabetic patients with microalbuminuria or clinical albuminuria, ARBs are the initial agents of choice.
• If one class is not tolerated, the other should be substituted
American Diabetes Association: Position Statement Diabetes Care 25:S85-S89, 2002American Diabetes Association: Position Statement Diabetes Care 25:S85-S89, 2002
UK Prospective Diabetes Study (UKPDS) Major Results: Powerful Risk Reductions
Better blood pressure control reduces…Better blood pressure control reduces… Strokes by Strokes by > > one thirdone third Serious deterioration of vision by Serious deterioration of vision by > > one thirdone third Death related to diabetes by Death related to diabetes by one thirdone third
Better glucose control reduces…Better glucose control reduces… Early kidney damage by Early kidney damage by one thirdone third Major diabetic eye disease by Major diabetic eye disease by one fourthone fourth
Turner RC, et al. BMJ. 1998;317:703-
713.
National Kidney Foundation Recommendations on Treatment of HTN and Diabetes
Blood pressure goal: 130/80 mmHgBlood pressure goal: 130/80 mmHg Target blood pressure: 125/75 for patients Target blood pressure: 125/75 for patients
with >1 gram/day proteinuriawith >1 gram/day proteinuria Blood pressure lowering medications should Blood pressure lowering medications should
reduce both blood pressure + proteinuriareduce both blood pressure + proteinuria Therapies that reduce both blood pressure Therapies that reduce both blood pressure
and proteinuria have been known to reduce and proteinuria have been known to reduce renal disease progression and incidence of renal disease progression and incidence of ischemic heart diseaseischemic heart disease
Bakris GL, et al. Am J Kidney Dis. 2000;36(3):646-661.
Cholesterol Lowering Therapy and Diabetic Nephropathy
Cholesterol Lowering Therapy and Diabetic Nephropathy
Management of ESRD due to DN
Early planning of Vascular AccessEarly planning of Vascular Access Both HD & PD could be appropriate modalities. Both HD & PD could be appropriate modalities. Early initiation of Dialysis at GFR 18-20 mls/min.Early initiation of Dialysis at GFR 18-20 mls/min. Renal TransplantationRenal Transplantation Combined Renal & Pancreatic Transplantation for Combined Renal & Pancreatic Transplantation for
IDDM.IDDM.
Treatment Objectives to Prevent Macrovascular Disease in Diabetic Patients
HypertensionHypertension BP < 130/80 mmHgBP < 130/80 mmHg
HypercholesterolemiaHypercholesterolemia LDL < 100 mg/dLLDL < 100 mg/dL
HyperglycemiaHyperglycemia Hgb AHgb A1C1C < 7.0 % < 7.0 %
American Diabetes Association Clinical Practice Recommendations. Diabetes Care. 2001;24(suppl1):S1-S133.
Management of HTN and Chronic Renal Disease (CRD) in Diabetics
Reduce BP to <130/80 mmHgReduce BP to <130/80 mmHg Use multiple antihypertensive drugs (ACEI, ARB, Use multiple antihypertensive drugs (ACEI, ARB,
diuretic, CCB, beta-blocker)diuretic, CCB, beta-blocker) Maximal reduction of proteinuriaMaximal reduction of proteinuria Treat hyperlipidemia (LDL <100 mg/dL)Treat hyperlipidemia (LDL <100 mg/dL) Control Hgb AControl Hgb A1C1C to <7% to <7%
Low salt diet (<2 gm NaCl/day)Low salt diet (<2 gm NaCl/day) Stop cigarette smokingStop cigarette smoking

Metformin Metformin
Hyperuricemia ??Hyperuricemia ??
Allopurinol ??Allopurinol ??
Recommended

















