D262Division of Orthodontic & Paediatric Dentistry
University of Western OntarioDr. Sahza Hatibovic-Kofman
PRIMARY DENTITION ANATOMY AND CAVITY
PREPARATION
2004-2005

GENERAL OBJECTIVES:
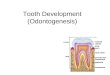
To present the anatomy of primary
teeth and key anatomical differences
between primary and permanent teeth
that influence cavity preparation.

SPECIFIC OBJECTIVES:
(1) Describe the general morphological differences between primary andpermanent teeth and their clinicalimplications.
(2) Identify special features and location of theroots of primary teeth. Comment onclinical applications.
(3) Describe the general morphology of thedental pulp, location of the pulp horns andorifices of canals in the primary teeth.Comment on clinical considerations.

Specific Objectives (continued):
(4) Identify histological differences between the pulp of primary and permanent teethand the clinical relevance.
(5) Identify the reason for most restorative problems in paediatric dentistry.
(6) Describe the principles of operativedentistry.
(7) Describe the steps for preparation andrestoration of Class I and Class II amalgamrestorations.

Specific Objectives (continued):
(8) Describe common errors in Class I and IIrestorations.
(9) Describe the differences in cavitypreparation when composite is used asa restorative material for primary teeth.

Most problems in paediatric dentistry occur because of
• failure to prepare and restore the teeth in a way that takes into account their:
ANATOMIC or MORPHOLOGIC structural characteristics and limitations.

ANATOMIC CONSIDERATIONS OF PRIMARY TEETH
1. Crowns of primary teeth are smaller, and more bulbous than permanent teeth.
2. Both lingual and buccal walls of theprimary teeth taper occlusally, thereforethe occlusal surface is quite narrow.
3. Primary teeth demonstrate greater cervicalconstriction and have more prominentcervical enamel contour than permanent teeth.


Anatomic considerations (continued)
4. Primary teeth have thinner enamel and dentin than permanent teeth.
5. The pulp of primary teeth are larger in relation to the crown than permanent teeth.
The pulp horns of primary teeth are closerto the outer surface of the tooth than for
permanent teeth.
The MESIOBUCCAL pulp horn is the most prominent.



Anatomic considerations (continued)6. Fine canals.7. Thin pulpal floor.8. The roots of primary teeth are long, slender
and curved. Interradicular space canaccommodate the developing permanenttooth.
9. In primary teeth the enamel rods of the gingival third of the crown extend in anocclusal direction. The rods of the permanent teeth extend in a cervical direction.




Anatomic considerations (continued)
10. Primary teeth have broad, flat proximal contact areas.
11. Primary teeth are whiter in colour than their permanent successors.




PRINCIPLES OF OPERATIVE DENTISTRY
Gain access.
Establish outline form
Eliminate caries.
Establish resistance and retention form.
Refinement and debridement of the cavity.



RESTORATIVE TRAY - SPEC
1. Mirror
2. Explorer
3. Cotton pliers
4. Small spoon
5. Large spoon
6. Hatchet
7. Small condensor
8. Large condensor

Restorative Tray (continued)
9. T-3 (Beaver tail)
10. Discoid-cleoid
11. Burnisher
12. G-38 (gold knife)
13. PFI (black felt)
14. Syringe









INFORMATION
In order to provide the best care for the child patient and teach excellence, we, at the children’s clinic, have decided to use tooth-coloured materials and stainless steel crowns as a first choice of treatments.
Occasionally other materials will be used according to the medical indications and/or child/guardian demand.

Montreal, November 27, 2000
It was very refreshing for us, as clinicians, to hear from a
university professor that the University of Western
Ontario actually teaches dental materials and techniques
that are up-to-date, in order to prepare the students to
the challenges of everyday clinical dental pediatric
practice.… J. Victor Legault
Quebec Assoc. of Pediatric Dentists

Information (continued)
Currently, there are four conventional and two hybrid restorative materials available for the restorations in primary teeth.
Conventional materials:
1. Stainless steel crowns (SSC).
2. Amalgam.
3. Composite resin.
4. Glass ionomer cement (GIC).

Information (continued)
Hybrids:
1. Resin-modified glass ionomer cement
(RMGIC).
2. Polyacid-modified resin composite
materials (PMRC), compomer.

Information (continued)
The restorative material for primary teeth should possess the following properties:• be biocompatible• join a strong adhesive bond to reminded
tooth• strengthen residual tooth structure• easy handling characteristic• be economical

Information (continued)
Amalgam is good material and has been used successfully for about 200 years, but tooth coloured materials accompanied with the bonding systems offer advantages over dental amalgam in:• Preservation of healthy tooth structure.
Today literally we can restore a tooth by removing only decayed structure. To accommodate amalgam a lot of healthy tooth structure has to be removed to provide mechanical retention of the restoration.

Information (continued)
• Repairability.• Esthetics.• Release of fluoride.
Our students are performing high quality care for the child patient and will be using the most current tooth-coloured materials.

GUIDELINES for Usage of the Restorative Materials in Mixed Dentition
First step in restorative dentistry is to perform good caries diagnosis and elimination of the lesion.
Under diagnosis = misdiagnoses.
In the SPEC clinic after visual diagnosis, we will use regularly light caries detector “DIAGNOdent” and/or dye caries detector “Seek and Sable”.






STATE OF THE TOOTH
• Caries free primary and permanent teeth
• Small decalcification
• Small lesion in dentin occlusally
TREATMENT
• Pit and fissure sealants
• Bur preparation or air abrasion - pit and fissure sealants
• Cavity preparation, and use caries seek and restore it with composite

STATE OF THE TOOTH
• MO or DO
• DO or MO next to permanent tooth if exfoliation will occur within two years.
TREATMENT
• Conservative preparation without extensions for prevention and use combination of flowable and filled composite.
• Conservative cavity preparation and glass ionomer cement.

Guidelines (continued)
• Multi surface lesions and teeth after pulp therapy will be restored with stainless steel crown (SSC).

STEPS FOR PREPARATION AND RESTORATION OF CLASS I AMALGAM RESTORATIONS
• Administer appropriate anaesthesia and place the rubber dam.
• Using a No. 330 bur gain access and penetrate into the tooth to a depth of 0.5 mm into dentin.
• Removal all carious dentin by using large, round bur.
• Provide retention and resistance by making cavity surface parallel with its external surface.

Steps Class I (continued)
• Smooth the enamel walls and refine the final outline form with No. 330 bur.
• Place pulp protection as needed.• Place and condense amalgam.• Carve amalgam.• Burnish the carved amalgam when it has
begun its initial set and resists deformation.• Remove the rubber dam and check the
occlusion.




COMMON ERRORS WITH CLASS I AMALGAM RESTORATIONS
• Not including all susceptible fissures.• Preparing the cavity too deep.• Undercutting the marginal ridges.• Carving the anatomy of the amalgam too deep.• Not removing the amalgam flash from the
cavosurface margins.• Undercarving, which leads to fracture of the
amalgam from hyperocclusion.

STEPS FOR PREPARATION AND RESTORATION OF CLASS II AMALGAM RESTORATIONS
• Administer appropriate anaesthesia and place the rubber dam.
• Place a wooden wedge in the in interproximal area.
• With No. 330 bur in the high speed turbine handpiece, prepare the occlusal outline form at the ideal depth.

Steps Class II (continued)• To prepare the proximal box, use the same bur
moving it buccolingually in a pendulum motion and in a gingival direction. The contact should be broken between the adjacent tooth gingivally, buccally and lingually.
• Remove any remaining caries.• Round axiopulpal line angle.• Remove any unsupported enamel off the
buccal, lingual and gingival walls.

Steps Class II (continued)• Place pulp protection if necessary.• Remove the wedge, place a matrix band, and
reinsert the wedge.• Condense amalgam.• Carving of the occlusal portion is performed
with a small carver. The marginal ridge can be carved with the tip of the explorer.
• Remove the wedge and the matrix.• Gently floss the interproximal contact.• Burnish the restoration.• Remove the rubber dam and check occlusion.




















PROCEDURE OF CLASS II CAVITY PREPARATION FOR COMPOSITE
RESTORATION1. A local anaesthetic will be administered in
the usual fashion and in the appropriate amount to ensure adequate anaesthesia during the procedures.
2. A rubber dam will be used routinely.3. Wooden wedges will be inserted in the
proximal areas to maximize the protection of gingiva and the adjacent tooth, and protection from tearing the rubber dam by bur.

Procedure Class II(continued)
4. The outline form of the cavity preparationswill be conservative as presented in thepicture.
5. No flaring buccal and lingual walls of theproximal box.
6. Caries has to be completely removed,please use seek and sable.
7. The line angles will be rounded slightly,but the cavity will not be extended forprevention.
8. Do not remove healthy and unsupportedenamel.

Procedure Class II(continued)
9. Rinse the cavity.10. A “cure-thru” celluloid matrix band or
onmi-paedo matrix will be inserted firmlyinto place.
11. Acid etch the cavity for 25 seconds.12. Rinse it for 20 seconds.13. Rub in one bottle bonding system, air dry
and cure for 10 seconds.14. Apply flavable composite on the edges
cure it.

Procedure Class II(continued)
15. Restore with filled composite (do goodmodeling to be able to avoid finishing).
16. Cure for 40 seconds.17. The matrix band will be removed and the
restoration will be finished and polished.Finishing and polishing will be done byusing finishing and polishing discs andstrips.
18. The rubber dam will be removed and theocclusal contacts evaluated and adjustedas necessary.

Procedure Class II(continued)
19. Any tooth with carious or iatrogenic pulpinvolvement will obtain pulp treatment,
andstainless steel crown.











PREVENTIVE RESIN RESTORATION (PRR)
OBJECTIVES:
1.List the indications and contra-indications for PRR for primary and permanent teeth.
2.Describe the PRR materials.
3.Describe the clinical procedures for PRR.
4. Identify the advantages of using PRR and their cost effectiveness.

PRR (continued)
Non-surgical management of initial carious lesions by remineralizaiton offers an opportunity to extend preventive dentistry into early therapy.
It is now recommended, for smooth surface, that cavity preparation and restoration placement is appropriate only after the lesion has progressed into the dentin.







































D262Division of Orthodontic & Paediatric Dentistry
University of Western OntarioDr. Sahza Hatibovic-Kofman
RUBBER DAM AND MATRIX APPLICATION
2004-2005

GENERAL OBJECTIVES:
• Discuss the armamentarium and
application of the rubber
dam
in paediatric patients.

SPECIFIC OBJECTIVES:
(1) Identify the need, indications and relativecontraindications for the paediatric patient.
(2) State the advantages of rubber dam anddescribe its preparation for a paediatricpatient.
(3) Describe clamps and their applications.(4) Describe the explanation of the rubber dam
to the child.(5) Select and apply the matrices for Class II
preparations in primary molars.

INDICATIONS:
All paediatric restorative procedures should be completed with the rubber dam in place.
RELATIVE CONTRINDICATIONS:
(1) Fixed orthodontic applicance.
(2) Partially erupted teeth.
(3) A child with upper respiratory infection.

ADVANTAGES:
1. Saves time.
2. Improvement of access.
3. Controls saliva.
4. Retraction and protection of soft tissues.
5. Prevention of the ingestion and inhalation
of foreign bodies.
6. Provision of aseptic environment.
7. Aid management.
8. Helps the dentist to educate parents.


























Retrospective Clinical Study
of Vitalescence in Primary
Molars

Table 1: Clinical Performance of Vitalescence in Primary Molars
A Three-Year Study
FAILURE SUCCESSTooth
Number ofTeeth
Restored # % # %
Upper 1st 106 12 11.32 94 88.68
Lower 1st 122 9 7.38 113 92.62
Upper 2nd 191 16 8.38 175 91.62
Lower 2nd 171 9 5.26 162 94.74
TOTAL 590 46 7.80 544 92.20

AMALGAM COMPOSITE
Location SPEC PRIVATEPRACTICE
SPEC PRIVATEPRACTICE
%Success
%Failure
%Success
%Failure
%Success
%Failure
%Success
%Failure
96 4 95 5 93.7 6.3 96.3 3.7
Table 2 - Success/Failure of Amalgam and Composite Restoration in SPEC Clinic and
Private Practice - A Two-Year Study

0
10
20
30
40
50
60
70
80
90
100
Amalgam inSPEC
Composite inSPEC
Amalgam inPaediatricPractice
Composite inPaediatricPractice
Perc
ent (%
)
1 Year 2 Year

Recommended