
35
Conjunctiva
Anatomy and PhysiologyThe conjunctiva reacts promptly to endogenous and exo-genous irritants and is thus a sensitive indicator of con-tact lens complications. Practically any problem causeddirectly or indirectly by contact lenses is associatedwithconjunctival changes (though not all conjunctivalchanges are due to contact lenses). Lid disease caused bycontact lenses is associated with changes of the tarsalconjunctiva, and corneal disease caused by contactlenses is associated with changes of the bulbar conjunc-tiva.
Changes of the lids and cornea should be soughtwhenever a contact lens wearer presents with con-junctivitis, because, in contact lenswearers, the lids, cor-nea, and conjunctiva constitute a functional unit. Thecomplications that arise are generally due to a distur-bance of the physiological, metabolic, and toxicologicalinterrelationship of these three structures. This inter-relationship is the central theme of contactologicalresearch and accounts for a major part of the ophthal-mologist’s work in caring for the contact lens-wearingpatient.
The conjunctiva is a mucousmembrane that extendsfrom the lid margins to the limbal region of the globe. Itis a well vascularized, translucent membrane with twoportions, tarsal (palpebral) and bulbar. The tarsal con-junctiva is tightly bound to the underlying tissue on theinner surface of the lid, while the bulbar conjunctiva ismore loosely applied to the sclera, except in the limbalarea. The fornix (zone of transition between the tarsaland bulbar conjunctiva) lies at the most remote area ofthe surface of the eyeball and forms the base of the con-junctival sac (cul-de-sac).
The conjunctiva is a mucous membrane containingmany secretory cells; the most important of these forcontact lens wearers are the goblet cells. When theirfunction is impaired, lacrimation becomes deficient, theeye dries out, and a foreign body sensation ensues thatmakes lens-wearing intolerable.
Tarsal Conjunctiva
Follicular Swelling, Papillary Hypertrophy,Giant Papillary Conjunctivitis
Symptoms: Severe itching while wearing lenses; burn-ing; increased secretions; impaired visual acuity (VA).
Clinical findings: Hyperemia, follicular swelling; papil-lary hypertrophy of the tarsal conjunctiva; recurrentdeposition of hydrophobic material on lens surfaces.
Hyperemia, follicular swelling, and papillary hyper-trophy of the tarsal conjunctiva are the classic signs ofGPC in contact lens wearers, a complication that is not atall rare inwearers of hard or soft lenses. This condition isbecoming significantly more common, not least becauseof air pollution.
Both in etiology and in phenotype, GPC resemblesvernal conjunctivitis (vernal catarrh), a condition seen inthe springtime in patients with an allergic predisposi-tion. GPC is caused by proteins from the lacrimal fluidthat are presumably denatured by lens-hygiene solu-tions and thereby become immunologically active.Deposited on the surface of the lens, these proteins act asantigens, towhich antibodies thenbind. The sandwichoflens, antigen, and antibody rubs on the tarsal conjunc-tiva, causing increased conjunctival swelling and secre-tions—the vicious cycle of GPC.
The hallmark of GPC is the coating of the contact lenssurface with a strongly adherent protein layer, whichpierces the film of tear fluid over the lenswithin secondsof insertion, leading to diminished visual acuity and in-creased glare. The case history generally points to thediagnosis: The patient wears lenses without complica-tions forweeks ormonths and then, suddenly, a problemdevelops. A few minutes after lens insertion the patientexperiences burning, chafing, and itching in the eyes.Tears and a film deposited on the surface of the lens im-pair visual acuity within a few seconds after the eyes areopened, and until the next blink. Conjunctival secretionscause the eyelids to stick together and limit the mobilityof the contact lens during blinking and eye movements.
Examination reveals the following: the contact lensis barely mobile or immobile on the surface of the eyeand is coated with a grayish-white film that makes itlook dry and dull. The lids are mildly swollen, and theirmargins are coated with dried yellowish-white secre-tion. The bulbar conjunctiva is mildly injected; evertingthe lids reveals a massive papillary swelling of the tarsalconjunctiva, which is made even more evident withfluorescein staining. GPC can be classified into fourstages (Table 9).
Conjunctiva
36
57
59
58
60
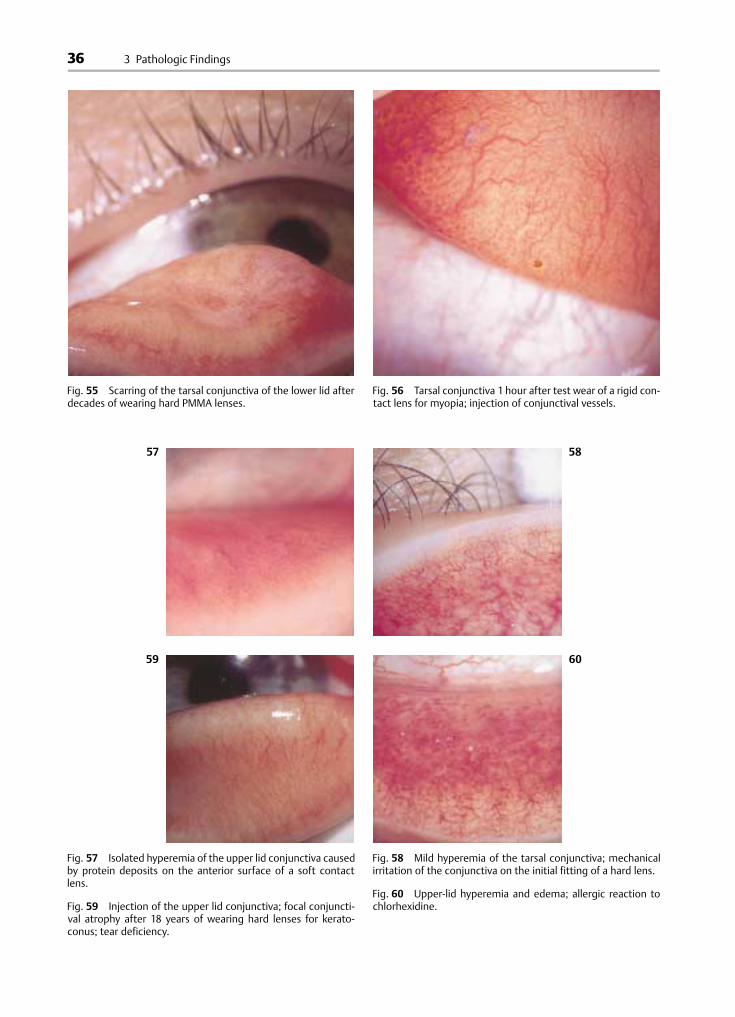
Fig. 55 Scarring of the tarsal conjunctiva of the lower lid afterdecades of wearing hard PMMA lenses.
Fig. 56 Tarsal conjunctiva 1 hour after test wear of a rigid con-tact lens for myopia; injection of conjunctival vessels.
Fig. 57 Isolated hyperemia of the upper lid conjunctiva causedby protein deposits on the anterior surface of a soft contactlens.
Fig. 59 Injection of the upper lid conjunctiva; focal conjuncti-val atrophy after 18 years of wearing hard lenses for kerato-conus; tear deficiency.
Fig. 58 Mild hyperemia of the tarsal conjunctiva; mechanicalirritation of the conjunctiva on the initial fitting of a hard lens.
Fig. 60 Upper-lid hyperemia and edema; allergic reaction tochlorhexidine.
3 Pathologic Findings
37
61
63
62
64
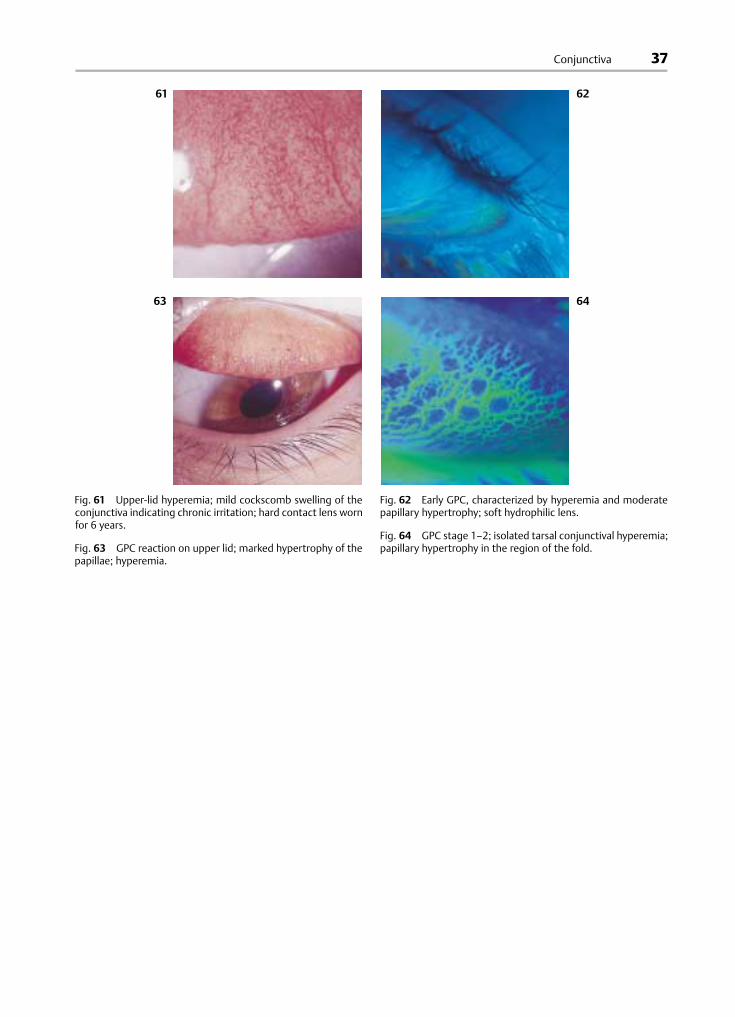
Fig. 61 Upper-lid hyperemia; mild cockscomb swelling of theconjunctiva indicating chronic irritation; hard contact lens wornfor 6 years.
Fig. 63 GPC reaction on upper lid; marked hypertrophy of thepapillae; hyperemia.
Fig. 62 Early GPC, characterized by hyperemia and moderatepapillary hypertrophy; soft hydrophilic lens.
Fig. 64 GPC stage 1–2; isolated tarsal conjunctival hyperemia;papillary hypertrophy in the region of the fold.
Conjunctiva

38
Fig. 65 GPC stage 2–3; papillary hypertrophy; identical pic-ture to vernal conjunctivitis.
Fig. 66 GPC in a CAB lens wearer; stage 2; fluorescein staining.
Fig. 67 GPC follicular swelling in the region of the lower con-junctival fold; soft contact lens worn for 3 months.
3 Pathologic Findings
39
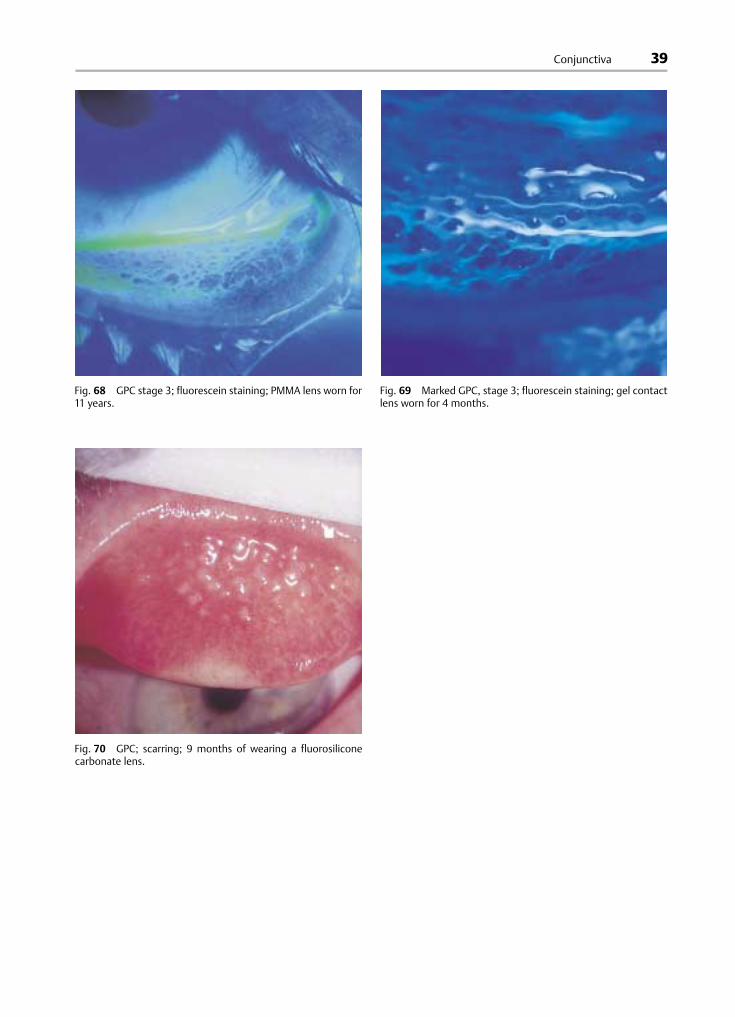
Fig. 68 GPC stage 3; fluorescein staining; PMMA lens worn for11 years.
Fig. 69 Marked GPC, stage 3; fluorescein staining; gel contactlens worn for 4 months.
Fig. 70 GPC; scarring; 9 months of wearing a fluorosiliconecarbonate lens.
Conjunctiva
40
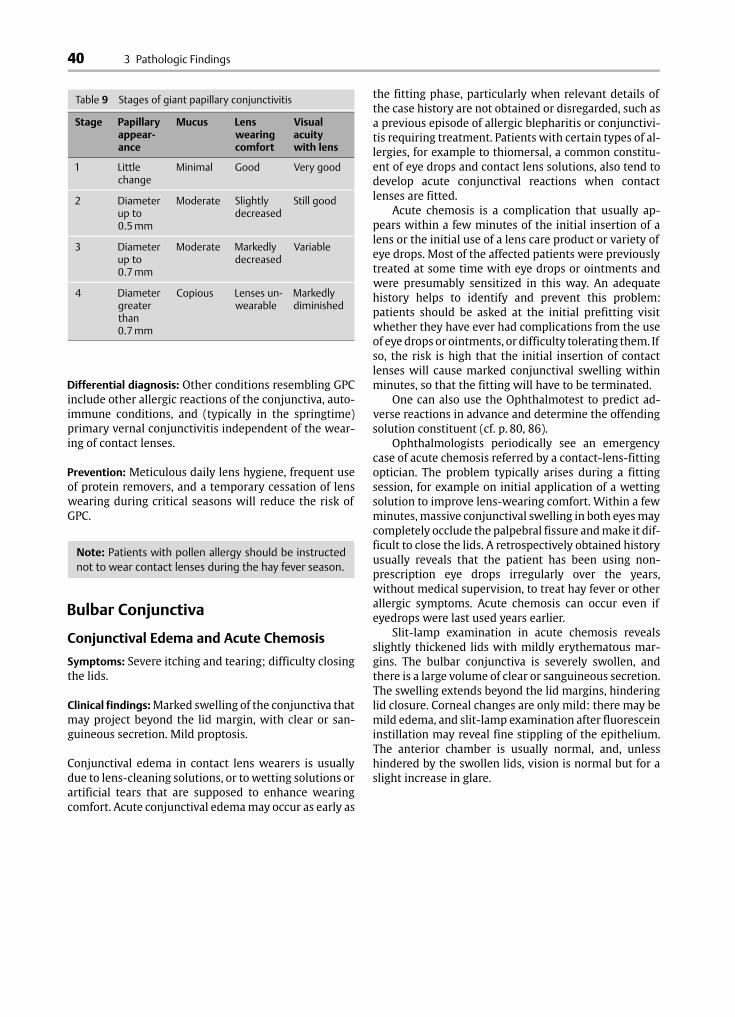
Table 9 Stages of giant papillary conjunctivitis
Stage Papillaryappear-ance
Mucus Lenswearingcomfort
Visualacuitywith lens
1 Littlechange
Minimal Good Very good
2 Diameterup to0.5 mm
Moderate Slightlydecreased
Still good
3 Diameterup to0.7 mm
Moderate Markedlydecreased
Variable
4 Diametergreaterthan0.7 mm
Copious Lenses un-wearable
Markedlydiminished
Differential diagnosis: Other conditions resembling GPCinclude other allergic reactions of the conjunctiva, auto-immune conditions, and (typically in the springtime)primary vernal conjunctivitis independent of the wear-ing of contact lenses.
Prevention: Meticulous daily lens hygiene, frequent useof protein removers, and a temporary cessation of lenswearing during critical seasons will reduce the risk ofGPC.
Note: Patients with pollen allergy should be instructednot to wear contact lenses during the hay fever season.
Bulbar Conjunctiva
Conjunctival Edema and Acute Chemosis
Symptoms: Severe itching and tearing; difficulty closingthe lids.
Clinical findings:Marked swelling of the conjunctiva thatmay project beyond the lid margin, with clear or san-guineous secretion. Mild proptosis.
Conjunctival edema in contact lens wearers is usuallydue to lens-cleaning solutions, or to wetting solutions orartificial tears that are supposed to enhance wearingcomfort. Acute conjunctival edemamay occur as early as
the fitting phase, particularly when relevant details ofthe case history are not obtained or disregarded, such asa previous episode of allergic blepharitis or conjunctivi-tis requiring treatment. Patients with certain types of al-lergies, for example to thiomersal, a common constitu-ent of eye drops and contact lens solutions, also tend todevelop acute conjunctival reactions when contactlenses are fitted.
Acute chemosis is a complication that usually ap-pears within a few minutes of the initial insertion of alens or the initial use of a lens care product or variety ofeye drops. Most of the affected patients were previouslytreated at some time with eye drops or ointments andwere presumably sensitized in this way. An adequatehistory helps to identify and prevent this problem:patients should be asked at the initial prefitting visitwhether they have ever had complications from the useof eyedrops or ointments, or difficulty tolerating them. Ifso, the risk is high that the initial insertion of contactlenses will cause marked conjunctival swelling withinminutes, so that the fitting will have to be terminated.
One can also use the Ophthalmotest to predict ad-verse reactions in advance and determine the offendingsolution constituent (cf. p. 80, 86).
Ophthalmologists periodically see an emergencycase of acute chemosis referred by a contact-lens-fittingoptician. The problem typically arises during a fittingsession, for example on initial application of a wettingsolution to improve lens-wearing comfort. Within a fewminutes, massive conjunctival swelling in both eyesmaycompletely occlude the palpebral fissure andmake it dif-ficult to close the lids. A retrospectively obtained historyusually reveals that the patient has been using non-prescription eye drops irregularly over the years,without medical supervision, to treat hay fever or otherallergic symptoms. Acute chemosis can occur even ifeyedrops were last used years earlier.
Slit-lamp examination in acute chemosis revealsslightly thickened lids with mildly erythematous mar-gins. The bulbar conjunctiva is severely swollen, andthere is a large volume of clear or sanguineous secretion.The swelling extends beyond the lid margins, hinderinglid closure. Corneal changes are only mild: there may bemild edema, and slit-lamp examination after fluoresceininstillation may reveal fine stippling of the epithelium.The anterior chamber is usually normal, and, unlesshindered by the swollen lids, vision is normal but for aslight increase in glare.
3 Pathologic Findings
41
73
75
74
76
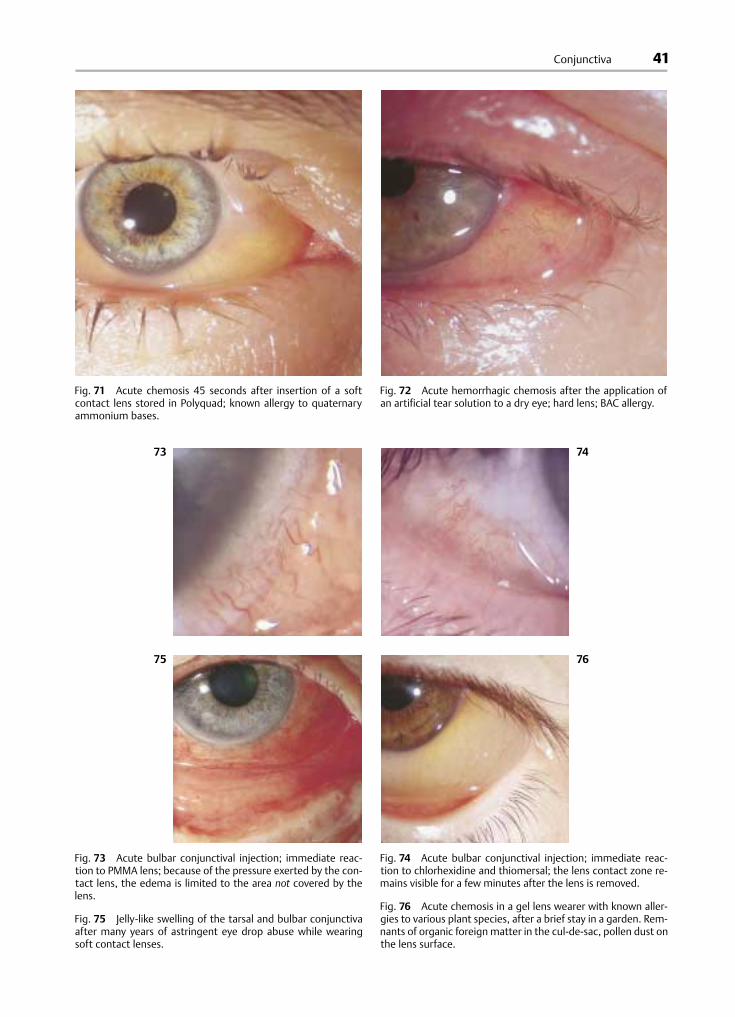
Fig. 71 Acute chemosis 45 seconds after insertion of a softcontact lens stored in Polyquad; known allergy to quaternaryammonium bases.
Fig. 72 Acute hemorrhagic chemosis after the application ofan artificial tear solution to a dry eye; hard lens; BAC allergy.
Fig. 73 Acute bulbar conjunctival injection; immediate reac-tion to PMMA lens; because of the pressure exerted by the con-tact lens, the edema is limited to the area not covered by thelens.
Fig. 75 Jelly-like swelling of the tarsal and bulbar conjunctivaafter many years of astringent eye drop abuse while wearingsoft contact lenses.
Fig. 74 Acute bulbar conjunctival injection; immediate reac-tion to chlorhexidine and thiomersal; the lens contact zone re-mains visible for a few minutes after the lens is removed.
Fig. 76 Acute chemosis in a gel lens wearer with known aller-gies to various plant species, after a brief stay in a garden. Rem-nants of organic foreign matter in the cul-de-sac, pollen dust onthe lens surface.
Conjunctiva

42
Table 10 Causes of conjunctival hemorrhage in contactlens wearers
A Related to contact lensesMaterial defects, inadequate polishing, edge defectsImproper lens insertion or removalSurface deposits
B Not related to contact lensesMechanical irritation, strong eye-rubbingVascular sclerosisCoagulopathy, leukemiaIatrogenic (anticoagulation)Tear deficiency syndrome
Differential diagnosis: Acute chemosis can also occur asan allergic reaction to pollen, environmental pollutants,or other substances. Other causes include retrobulbarmasses, severe intraocular infections, and radiation in-jury to the eyes.
Prophylaxis: Acute chemosis can often be prevented bymeticulous history-taking.
Note: When acute chemosis occurs, its cause must bedetermined before the lenses are worn again or newlenses are fitted; otherwise, a recurrence is likely.
Subconjunctival Hemorrhage
Symptoms: Usually no pain or discomfort, but patientsare highly distressed by the prominently visible abnor-mality.
Clinical findings: Deep-red hematoma under the con-junctiva, which is usually somewhat raised.
Multiple microhemorrhagic spots are often present inthe conjunctiva of contact lens wearers, usually in theperilimbal region where the lens rests, but occasionallyin the tarsal conjunctiva. These easily visible lesions ap-pear spontaneously, often sending the highly distressedpatient to the emergency service of the eye clinic. Thereis usually no pain or impairment of visual acuity.
Blood begins to pool under the bulbar conjunctivashortly after lens insertion, usually arising from a site ofinjury near the limbus and spreading out evenly underthe conjunctiva of the lower half of the eye. When a softlens is still on the eye, the hematoma in the area coveredby the lens is somewhat compressed and thus paler thanelsewhere. There is no pain, discomfort, or cornealedema, unless the eyes are rubbed.
High-power slit-lamp examination reveals thesource of the bleeding as a small tear of the bulbar con-junctiva, rarely more than 1mm long. Such tears oftenresult from improper lens insertion or removal. Othercauses are long fingernails or devices used for lens inser-tion or removal. Another common cause is a defect of therim of the lens, for example, a sharp-edged lens tear,breakage, or deposit. Such lesions are usually caused byhard lenses but can also be caused by inadequately rehy-
drated soft lenses, or by disposable lenses that are wornfar beyond the recommended period, until they physi-cally deteriorate. Excessively long wear of disposablelenses regularly produces breaks and tears in the lens,which can injure the lids, conjunctiva, and cornea; simi-lar defects can be produced by improper handling, in-adequate hygiene, or storage under excessively dry con-ditions. The most common causes of subconjunctivalhemorrhage are listed in Table 10.
Tominimize the risk of subconjunctival hemorrhage,the contact lenses should be inspected under a dissect-ing microscope, or a slit lamp fitted with a contact-lens-holding device, at every follow-up visit.
Differential diagnosis: Subconjunctival hemorrhage hasa unique appearance and is hardly likely to be confusedwith any other disorder. It may, however, appear for rea-sons unrelated to the wearing of contact lenses.
Prophylaxis: Patients should be instructed to discard anylenseswith visible defects, and to take care not to cut theeye when inserting and removing the lens. Persons withhemorrhagic disorders of any kind should not wear con-tact lenses.
Note: Whenever conjunctival hemorrhage occurs, thecontact lenses should be inspected for defects. Patientswith recurrent hemorrhages should undergo medicalevaluation for a bleeding disorder.
3 Pathologic Findings
43
79
81
80
82
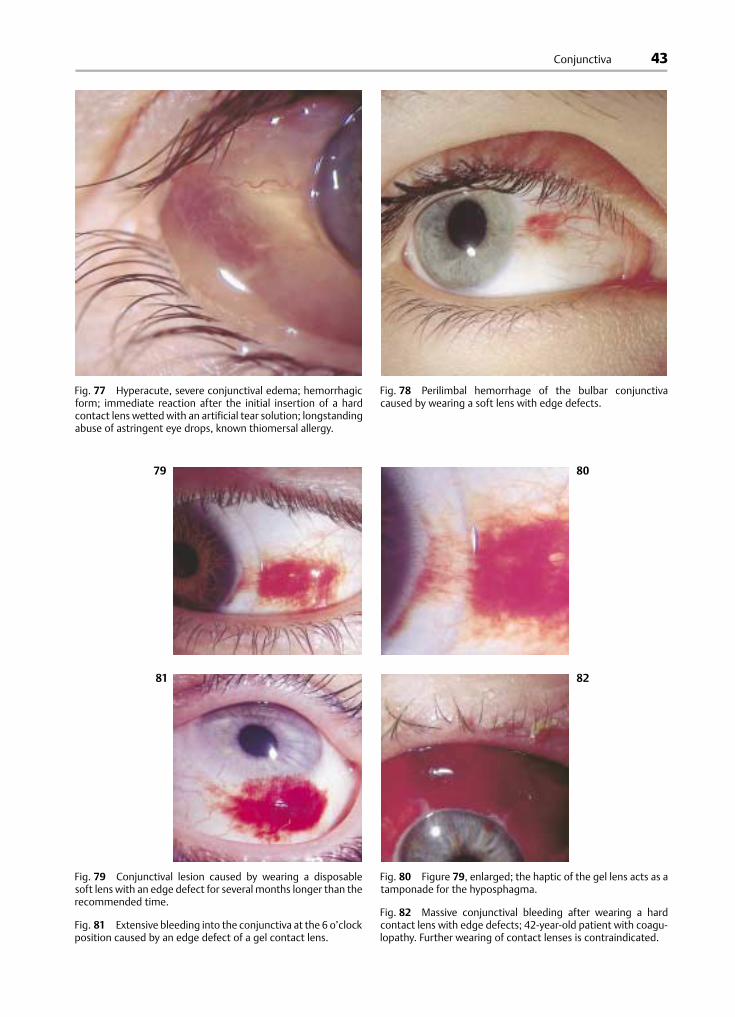
Fig. 77 Hyperacute, severe conjunctival edema; hemorrhagicform; immediate reaction after the initial insertion of a hardcontact lens wetted with an artificial tear solution; longstandingabuse of astringent eye drops, known thiomersal allergy.
Fig. 78 Perilimbal hemorrhage of the bulbar conjunctivacaused by wearing a soft lens with edge defects.
Fig. 79 Conjunctival lesion caused by wearing a disposablesoft lens with an edge defect for several months longer than therecommended time.
Fig. 81 Extensive bleeding into the conjunctiva at the 6 o’clockposition caused by an edge defect of a gel contact lens.
Fig. 80 Figure 79, enlarged; the haptic of the gel lens acts as atamponade for the hyposphagma.
Fig. 82 Massive conjunctival bleeding after wearing a hardcontact lens with edge defects; 42-year-old patient with coagu-lopathy. Further wearing of contact lenses is contraindicated.
Conjunctiva
44
83
85
84
86
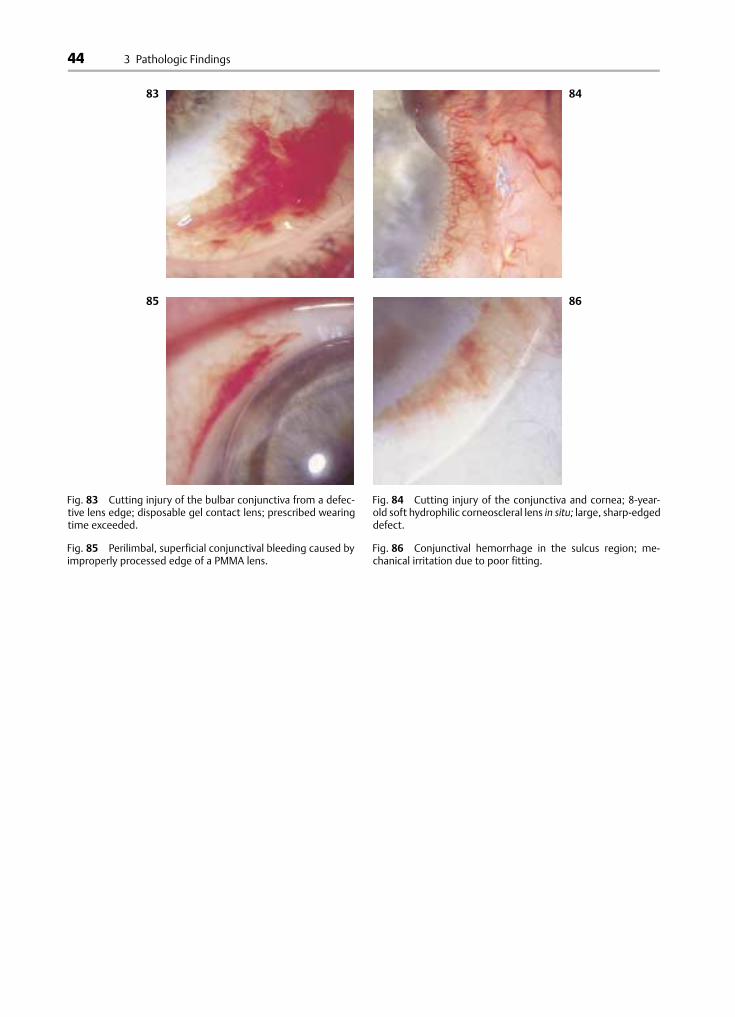
Fig. 83 Cutting injury of the bulbar conjunctiva from a defec-tive lens edge; disposable gel contact lens; prescribed wearingtime exceeded.
Fig. 85 Perilimbal, superficial conjunctival bleeding caused byimproperly processed edge of a PMMA lens.
Fig. 84 Cutting injury of the conjunctiva and cornea; 8-year-old soft hydrophilic corneoscleral lens in situ; large, sharp-edgeddefect.
Fig. 86 Conjunctival hemorrhage in the sulcus region; me-chanical irritation due to poor fitting.
3 Pathologic Findings

45
Table 11 Causes of mechanical irritation in contact lenswearers
Material defects, inadequate polishingFlat fitting, decentrationSurface depositsLesion of the lid marginLesion of the corneaTear deficiency syndrome
Generalized Conjunctival Hyperemia
Conjunctival hyperemia in contact lens wearers has avariety of causes, which can often be distinguished fromone another by the location and appearance of hyper-emia. Focal conjunctival hyperemia is most often due tomechanical irritation of the conjunctiva in a circum-scribed area from a dried-out, ill-fitted, defective, ordeposit-coated lens; annular perilimbal injection is usu-ally of toxic or allergic etiology. Generalized conjunctivalhyperemia (i.e., of the entire conjunctiva, including thearea under the contact lens) is usually caused by me-chanical irritation or infection; other causes include in-adequate lacrimation, allergic or toxic processes, andradiation injury. Whether focal or generalized, thehyperemic area is superficially discolored (brick-red);the reactively dilated vessels of the conjunctiva are al-ways bright red and freely mobile over the scleral sur-face. (This is not so in cases of conjunctival hyperemiasecondary to underlying deep or scleral infection.)
Mechanical Irritation and Injury
Symptoms: Eye-rubbing; foreign body sensation; tear-ing.
Clinical findings: The entire bulbar conjunctiva is in-jected and appears brick-red.
Conjunctival vasodilatation as a rapidly occurring re-sponse to a foreign body is routinely observed when apatient first starts towear contact lenses. Surface vesselsof the bulbar conjunctiva are greatly enlarged duringthis period. This response is normal in the initial phase ofcontact lens wear, but pathological at later times.
The causes of mechanical irritation of the conjunc-tiva in contact lens wearers are listed in Table 11.
If a lens is fitted too flatly, its edge does not lie se-curely on the limbus and can rub against the conjunctiva.Lens cracks, fractures, or polishing defects, as well assurface deposits due to inadequate cleaning are othercauses of mechanical irritation. Injury of the conjunctivafrom an exogenous foreign body looksmuch the same asinjury from a contact lens; the two situationsmay be dif-ficult to distinguish. It may be useful to remove the lensand examine the conjunctiva with fluorescein or rosebengal staining; distinctive traces of the foreign bodymay become evident.
A common cause of generalized conjunctival hyper-emia in contact lens wearers is inadequate lacrimation.Any qualitative or quantitative, primary or secondaryimpairment of lacrimation impairs the ability of the lensto glide without friction over the cornea and conjunc-tiva. The unlubricated lens acts as a foreign body andcauses mechanical conjunctivitis. The symptoms in-clude burning, foreign body sensation, rubbing of theeye, and epiphora. Defects in the conjunctival and cor-neal epithelium can be detected with rose bengal.
Infection
Symptoms: Burning; eye-rubbing; foreign body sensa-tion; epiphora.
Clinical findings: Injection and chemosis of the entireconjunctiva; secretions.
Conjunctivitis with generalized injection is certainly themost common complication of contact lenswearing. Thesymptoms include burning, foreign body sensation, eye-rubbing, and epiphora.
1. Bacterial Conjunctivitis
Symptoms: Burning; eye-rubbing; foreign body sensa-tion; tearing.
Clinical findings: Generalized injection and chemosis;secretions in the cul-de-sac.
Conjunctiva

46
89
91
90
92
Fig. 87 Severe conjunctival hemorrhage after a punch in theeye; the gel lens remained intact.
Fig. 88 Conjunctival hyperemia; mechanical irritation from ahard contact lens characterized by an even, brick-red discolora-tion of the entire bulbar conjunctiva.
Fig. 89 Focal lateral bulbar conjunctival hyperemia from aforeign body reaction; hard contact lens; typical brick-red color.
Fig. 91 Focal limbal conjunctival hyperemia from a foreignbody reaction; gel contact lens.
Fig. 90 Focal lateral conjunctival hyperemia from a foreignbody reaction; rigid contact lens.
Fig. 92 Focal conjunctival hyperemia with accentuation nearthe limbus, due to a foreign body reaction; soft contact lens.
3 Pathologic Findings
47
95
97
96
98
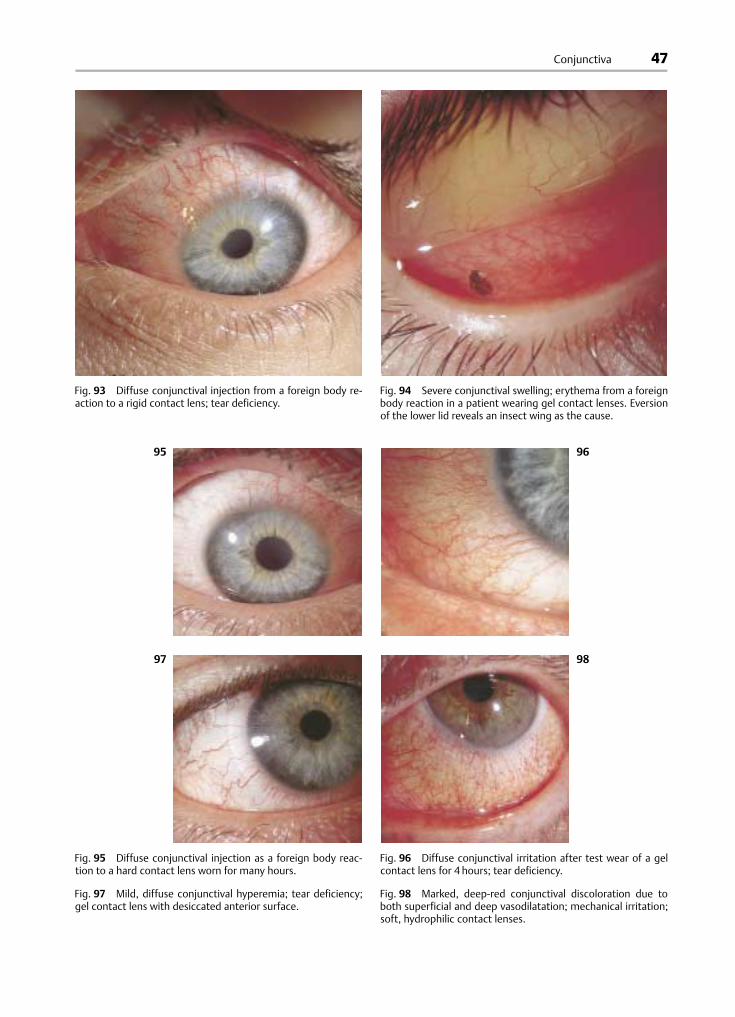
Fig. 93 Diffuse conjunctival injection from a foreign body re-action to a rigid contact lens; tear deficiency.
Fig. 94 Severe conjunctival swelling; erythema from a foreignbody reaction in a patient wearing gel contact lenses. Eversionof the lower lid reveals an insect wing as the cause.
Fig. 95 Diffuse conjunctival injection as a foreign body reac-tion to a hard contact lens worn for many hours.
Fig. 97 Mild, diffuse conjunctival hyperemia; tear deficiency;gel contact lens with desiccated anterior surface.
Fig. 96 Diffuse conjunctival irritation after test wear of a gelcontact lens for 4 hours; tear deficiency.
Fig. 98 Marked, deep-red conjunctival discoloration due toboth superficial and deep vasodilatation; mechanical irritation;soft, hydrophilic contact lenses.
Conjunctiva

48
Fig. 99 Marked, diffuse brick-red coloration of the conjunctivain bacterial conjunctivitis.
Fig. 100 Bacterial conjunctivitis due to Haemophilus in a pa-tient wearing gel contact lenses.
Fig. 101 Massive conjunctival injection, mildly accentuated inthe area contacted by the (soft, hydrophilic) contact lens;bacterial conjunctivitis due to Pseudomonas.
3 Pathologic Findings

49
Table 12 Causes of conjunctivitis in contact lens wearers
Altered ocular floraEpithelial defectsFaulty lens cleaningFaulty lens disinfectionTear deficiencyElevated temperature of the corneal surfaceImpaired immune competenceChronic hypoxiaOverwearingWearing deteriorated lensesSystemic infectionWearing lenses during sleepParasitic infection
Table 13 The organisms that most frequently cause con-junctivitis in contact lens wearers
Adenovirus Herpes simplex virus Pneumococcus
Aspergillus Haemophilus Pseudomonas
Candida Klebsiella Staphylococcus
Chlamydia Moraxella
Infectious conjunctivitis is among the more commonconditions treated by the ophthalmologist, affectingboth contact lens wearers and the general population.Improper lens wear (Table 12) predisposes to its occur-rence; it is caused by a broad spectrum of micro-organisms—bacteria, viruses, and occasionally fungi orAcanthamoeba.
The characteristic signs of bacterial conjunctivitis areswelling of the lids and generalized injection of thebulbar and tarsal conjunctivae. The cul-de-sac containscopious mucous or proteinaceous secretions. As long asthe infection is limited to the conjunctiva, the cornea isclear and visual acuity is unaffected; the anterior cham-ber is normal. Excessive tearing may affect vision. If theinterior of the eye is inflamed, changes in the refractivemedia may impair visual acuity, but this is rare. Cultureof the secretions in the cul-de-sac may reveal the etio-logic organism; Pseudomonas, Staphylococcus, Haemo-philus, and Pneumococcus commonly cause conjunctivi-tis in contact lens wearers (Table 13).
Bacterial conjunctivitis is often the result of inade-quate lens hygiene. The biofilm in the lens case providesan excellent breeding ground for bacteria and fungi; soft,
hydrophilic lenses are more commonly the vector of in-fection than hard lenses because their aqueous portioncan act as a culture medium for microorganisms.
In patients with infectious conjunctivitis, samplesfor culture should be obtained not only from the cul-de-sac, but also from the surfaces of the contact lenses, andfrom the lens case, for identification of the organism anddetermination of its pattern of antibiotic sensitivity andresistance. The latter is particularly important, not onlyfor the choice of the best antibiotic, but also for assess-ment of the efficacy of the various contact lens hygienesystems currently available on the market.
Differential diagnosis: Bacterial conjunctivitis is a clini-cally distinctive entity. It should not be forgotten,however, that conjunctivitis can be caused by foreignbodies of various kinds in the cul-de-sac, including “lost”contact lenses or lens fragments. Recurrent conjunctivi-tis may be due to an immunodeficient state, a metabolicdisorder, or repeated reinfection from the throat, nose,skin, or ear (transfer of organisms by way of the pillow).
Prophylaxis: Two basic steps will minimize the risk ofconjunctival inflammation: first do careful lens hygiene,second stop all lens wearing during an infection.
Note: Bacterial conjunctivitis in contact lens wearers isalmost always due to poor lens hygiene. If lens-wearingis not discontinued, corneal infection may ensue.
Conjunctiva
50
102
104
103
105
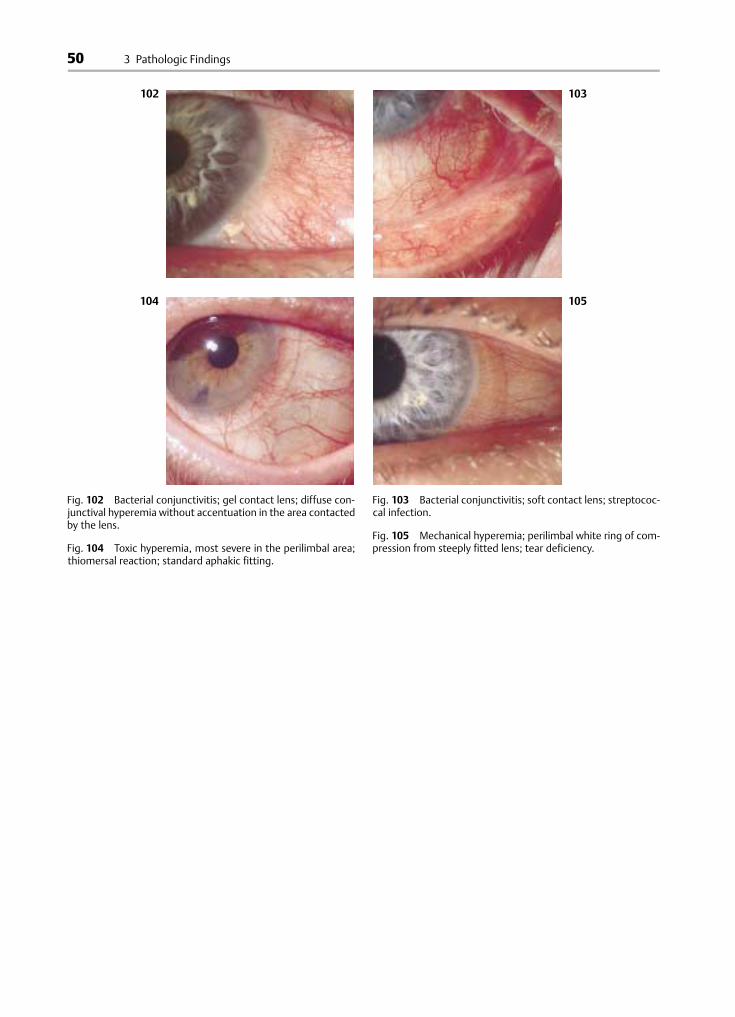
Fig. 102 Bacterial conjunctivitis; gel contact lens; diffuse con-junctival hyperemia without accentuation in the area contactedby the lens.
Fig. 104 Toxic hyperemia, most severe in the perilimbal area;thiomersal reaction; standard aphakic fitting.
Fig. 103 Bacterial conjunctivitis; soft contact lens; streptococ-cal infection.
Fig. 105 Mechanical hyperemia; perilimbal white ring of com-pression from steeply fitted lens; tear deficiency.
3 Pathologic Findings

51
Fig. 106 Bacterial conjunctivitis; pus in the lower cul-de-sac;staphylococcal infection.
Fig. 107 Diffuse conjunctival infection and hemorrhage; viralconjunctivitis; hard contact lens.
Fig. 108 Viral conjunctivitis; diffuse brick-red to deep-red dis-coloration of the conjunctiva, with hemorrhage; soft contactlens wearer.
Fig. 109 Fungal conjunctivitis; diffuse vasodilatation with mildparalimbal accentuation; soft contact lens; candidiasis in adiabetic patient.
Conjunctiva
52
2. Viral Conjunctivitis
Symptoms: Burning; itching; foreign body sensation;tearing.
Clinical findings: Marked injection; microhemorrhages;swelling of the plicae; minimal secretion.
Unlike bacterial conjunctivitis, viral conjunctivitis israrely related to contact lens wearing; it is usually amanifestation of systemic viral infection, for example in-fluenza. Nonetheless, though primary viral conjunctivi-tis is the most common type, fitters of contact lensesmust be aware that poor hygiene on their partmay causean outbreak of iatrogenic epidemic keratoconjunctivitis(EKC).
Differential diagnosis: Viral conjunctivitis is distin-guished from bacterial conjunctivitis by the waterysecretion in the cul-de-sac, and by the swollen plicae(particularly in EKC). Signs of infection often involve thecornea as well. Cases that fail to improve with treatmentshould arouse suspicion of another type of infection,such as fungal or parasitic. Foreign body reactions aswell as toxic and allergic processes must be excluded.
Note: Viral conjunctivitis is highly contagious. Thepatient’s family and acquaintances are at risk, as are thepersonnel and patients of the lens-fitting practice.
3. Fungal Infection
Symptoms: Foreign body sensation; eye-rubbing; sensa-tion of heat and dryness.
Clinical findings:Marked surface injection accompaniedbymarked, generally livid, deep injection;whitish secre-tions in the cul-de-sac.
Fungal infection is rare in healthy contact lens wearersand is usually seen in those suffering from immune com-promise, diabetes, or other metabolic disorders. Candidaalbicans and Aspergillus niger are often the cause. Fungalinfections are difficult to treat. Corneal involvement orinfiltration into the interior of the globe poses a majorthreat to vision.
Fungal infections are much more common in softlens wearers than in hard lens wearers, as the soft lens isan ideal fungal culture medium. The organisms take thewater they need from the aqueous compartment of thelens, and nutrients and electrolytes from the lacrimalfluid.
Fungal infections are best diagnosed by microbialculture of the secretions from the cul-de-sac. Micro-scopic examination of secretions and of the contact lensitself may reveal fungal hyphae. Demonstration of theresponsible fungal organism serves to exclude otherpossible causes of conjunctivitis, for example GPC.
Differential diagnosis: Fungal infections of the anteriorsegment are not always readily distinguishable frombacterial or viral infections, particularly because mixedflora may be present. Microbial culture is required.
Prophylaxis: In general, patients at risk of fungal infec-tion should not wear contact lenses. Those who do wearlensesmust comply rigidlywith the recommended lens-care routine.
Note: The diagnosis of a fungal infection in a contactlens wearer should prompt medical evaluation for latentor active diabetes or an immunocompromised state.
Focal Conjunctival Hyperemia
Focal conjunctival hyperemia is due to a spatially re-stricted process; thus, in contact lens wearers, it is usu-ally found in the limbal area, (i.e., at the periphery of thecontact lens). The etiology of hyperemia in contact lenswearers (as in other persons)may be toxic, allergic, met-abolic, mechanical, or inflammatory.
3-O’Clock and 9-O’Clock Limbal Hyperemia
Symptoms: Increased foreign body sensation; increasedtear flow.
Clinical findings: Marked dilatation of the vessels at the3-o’clock and 9-o’clock positions. These sites are oftencovered with a mildly raised, yellowish deposit.
Conjunctival injection near the limbus at the 3-o’clockand 9-o’clock positions in a hard lens wearer implies aninadequate cushion of tear fluid between the lens andthe eye. The lens mechanically irritates the conjunctivaand cornea during horizontal saccades. The problemmay be caused by inadequate lacrimation or by poor fit-ting. Diagnostic assessment includes quantitative tearanalysis, inspection of the sit of the lens, and slit-lampexamination of the cornea after staining.
Differential diagnosis: Conjunctival injection near thelimbus can also result from local lesions of the conjunc-tiva and cornea.
Note: Check for corneal defects in all cases of localizedconjunctival injection.
3 Pathologic Findings

53
Fig. 110 Marked deep-red discoloration of the conjunctiva dueto candidiasis in a soft contact lens wearer with AIDS.
Fig. 111 Marked conjunctival vasodilatation at the 3-and9-o’clock positions in a hyperopic wearer of hard contact lenseswith tear deficiency.
Fig. 112 Focal conjunctival hyperemia at the 4-to 5-o’clock po-sition; injury of the edge of the cornea through improper fitting.
Fig. 113 Isolated perilimbal conjunctival hyperemia under ahard corneoscleral contact lens. Mechanical irritation by exces-sively tight fitting in the haptic zone.
Conjunctiva

54
Table 14 Differential diagnosis of perilimbal hyperemia incontact lens wearers
Color Location Cause
Brick-red Conjunctivalsurface
Mechanical irritation,fitting error
Bluish-red Superficial anddeep conjunctiva
Toxic, allergic reaction
Livid blue Deep conjunctiva,sclera
Intraocular complication,iritis, iridocyclitis, uveitis
Perilimbal and Limbal Injection
Symptoms: The discomfort is rarely severe and is usuallylimited to itching and a feeling of dryness.
Clinical findings: Markedly dilated vessels in the para-limbal or perilimbal region.
Isolated, superficial perilimbal injection is a pathologicalfinding seen almost exclusively inwearers of soft contactlenses. It is easily mistaken for ciliary injection, whichindicates an intraocular process. The affected vessels inciliary injection are livid in color, more deeply situated,and more finely reticulated.
An arc-shaped, superficial perilimbal area of injec-tion (sometimes accompanied by fine microhemor-rhages) is usually due to faulty lens fitting. If the edge ofthe lens is too steep or too firmly applied to the conjunc-tival surface, it can compress the bulbar conjunctiva inthe region of the corneal sulcus. On the other hand, if thelens is too flat, its edges can scrape the perilimbal con-junctiva. The differential diagnosis is straightforward: Ifthe perilimbal redness disappears within 10 minutes oflens removal, the lens was too flat; if in the same periodof time a reactive hyperemia appears, the lens was toosteep.
Redness from wearing lenses with abrasive edgesor edge defects disappears within 1–2hours after thelenses are removed. Hyperemia of this type is only rarelyassociated with corneal injury.
Deep perilimbal vasodilatation indicates an entirelydifferent situation. Deep-red or livid vessels, locatedbelow the surface and parallel to the limbus, are a defi-nite indication of corneal damage or an intraocularprocess. The usual cause in contact lens wearers is toxickeratopathy in reaction either to the lensmaterial or to alens care product.
A finding of deep and livid (rather than superficialand brick-red) vasodilatation limited to the limbal re-gion is classically termed “ciliary injection.” The dilatedvessels are located in the perilimbal sclera and are an in-dication of deep corneal and intraocular changes, such asiritis or uveitis, which are very rarely related to thewear-ing of contact lenses. It may prove difficult to determineby examination whether the finding is superficial (peri-limbal) or deep (ciliary), particularly in protracted cases.A rule of thumb for the crucial differentiation of primaryintraocular problems from contact lens complications isthat the latter, unlike the former, generally resolve afterthe lenses are removed.
It is not always easy to classify limbal hyperemia orto determine whether it is due to the wearing of contactlenses. A thorough history and a meticulous slit-lampexamination of the limbus under highest power aremandatory. The most important criteria for differentialdiagnosis are listed in Table 14.
The Ophthalmotest is an excellent aid to the exami-nation of conjunctival changes, especially perilimbal re-actions, and enables differentiation of improper lens fit-ting from a toxic or allergic reaction (pp. 80, 86).
Differential diagnosis: In summary, perilimbal and limbalinjection must be distinguished from scleral and in-traocular processes, which cause deep perilimbal (par-ticularly ciliary) vasodilatation and thereby produce alivid (bluish-purple)—rather than brick-red—perilimbalring.
Prophylaxis: Immediate ophthalmological examinationin the early phase of perilimbal injection can preventfurther injury.
Note: Intraocular disease must be ruled out wheneverperilimbal vasodilatation is found.
3 Pathologic Findings
55
116
115114
117
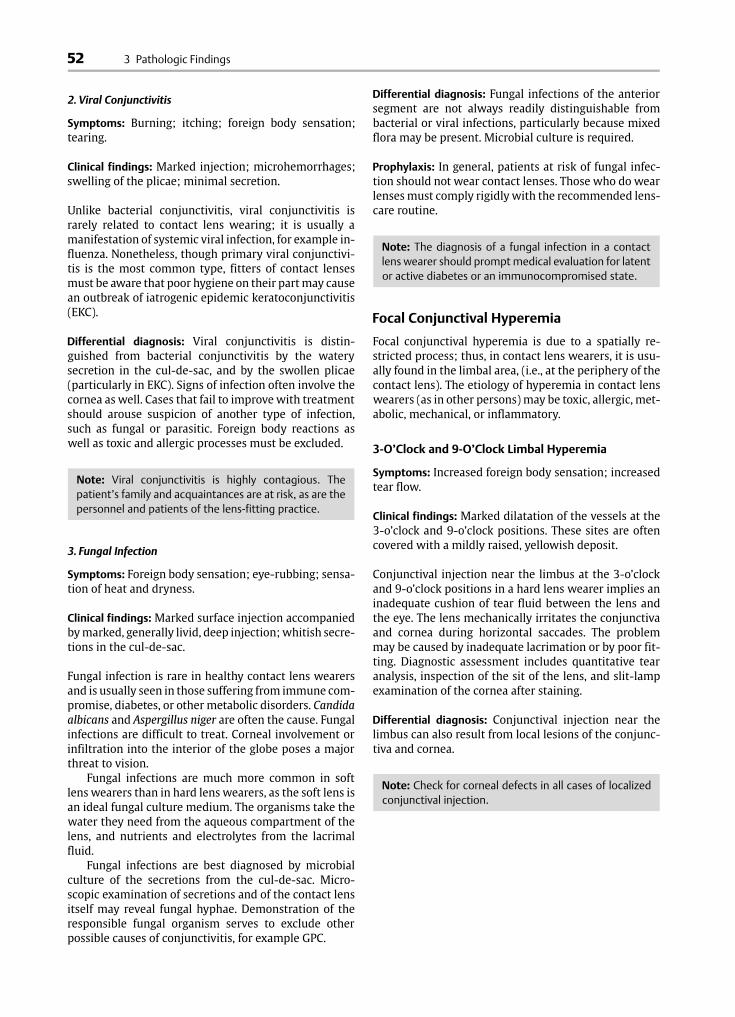
Fig. 114 Focal conjunctival hyperemia at the limbus; hard con-tact lens; tear deficiency.
Fig. 116 Diffuse vasodilatation of the bulbar conjunctiva withaccentuation at the limbus; dry eye; gel contact lens.
Fig. 115 Marked, diffuse conjunctival hyperemia; tear defi-ciency; soft contact lens; marked drying of the anterior surfaceof the lens.
Fig. 117 Diffuse bulbar conjunctival vasodilatation with accen-tuation at the limbus at the area of contact of the soft contactlens; deposits on the lens surface; tear deficiency.
Conjunctiva
56
119
121
120
122
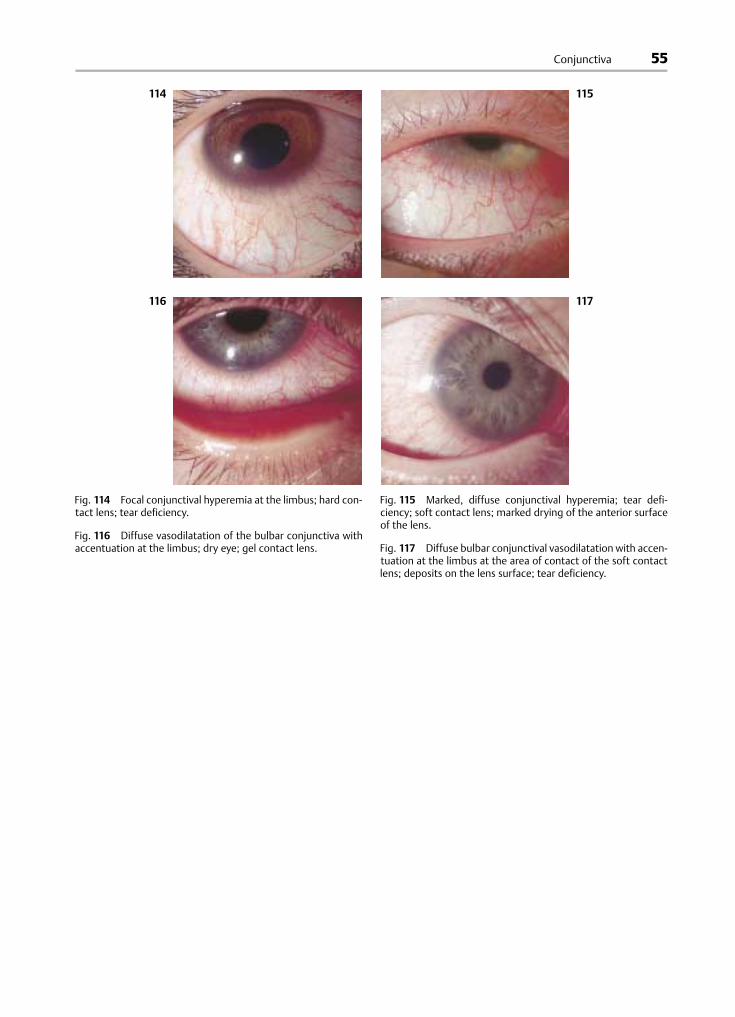
Fig. 118 Brick-red perilimbal injection from poorly seated softcontact lens; hyperopia + 6.5 D.
Fig. 119 Limbal hyperemia; diffuse bulbar conjunctival vaso-dilatation due to a toxic keratopathy; gel lenses; PMMA intoler-ance.
Fig. 121 Fire-red limbal hyperemia in toxic keratopathy; reac-tion to lens cleaning agents; gel contact lens.
Fig. 120 Limbal injection in toxic keratopathy; hyperemia ofthe bulbar and tarsal conjunctiva. Soft hydrophilic contact lens.
Fig. 122 Enlargement of Figure 121.
3 Pathologic Findings
57
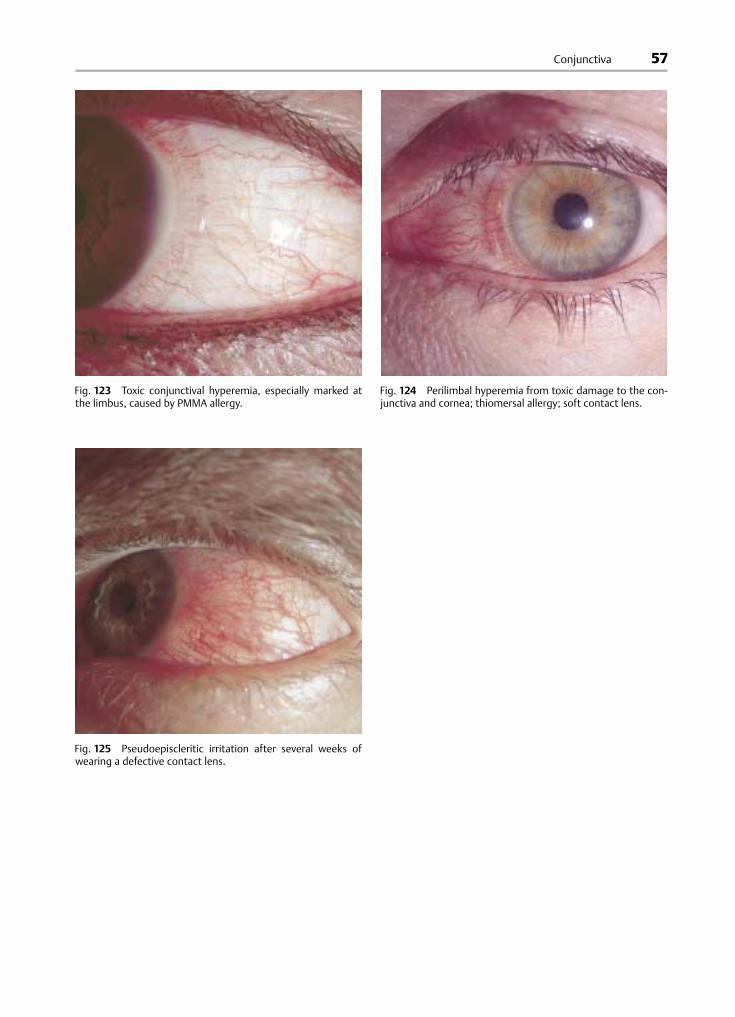
Fig. 123 Toxic conjunctival hyperemia, especially marked atthe limbus, caused by PMMA allergy.
Fig. 124 Perilimbal hyperemia from toxic damage to the con-junctiva and cornea; thiomersal allergy; soft contact lens.
Fig. 125 Pseudoepiscleritic irritation after several weeks ofwearing a defective contact lens.
Conjunctiva
Recommended



![National Library of Serbia...feronasa] bulbar conjunctiva [61 According to some references, pans of conjunctiva higher goblet cell density are Inferonasal bulbar conjunctiva, tarsal](https://img.dokumen.tips/doc/110x75/6084bbb33561423ad20313c4/national-library-of-feronasa-bulbar-conjunctiva-61-according-to-some-references.jpg)













