Case Report
A Simultaneous Liver-Kidney Transplant Recipient With IgANephropathy Limited to Native Kidneys and BK Virus
Nephropathy Limited to the Transplant Kidney
Manasa P. Ujire, MD,1 Michael P. Curry, MD,1 Isaac E. Stillman, MD,2
Douglas W. Hanto, MD, PhD,1 and Didier A. Mandelbrot, MD1
Immunoglobulin A (IgA) deposition in the native kidneys of patients with liver disease is well described.Secondary IgA nephropathy usually is thought to be benign, but hematuria, proteinuria, and loss of kidneyfunction have been reported in this context. BK virus nephropathy is an important cause of kidney transplantloss; however, BK virus nephropathy is rare in the native kidneys of patients who underwent transplantation ofother organs. We report the case of a patient with alcohol-related end-stage liver disease and chronic kidneydisease with hematuria who underwent simultaneous liver-kidney transplantation. His kidney function de-creased over the course of several weeks posttransplantation. Biopsy of the transplant kidney showed BK virusnephropathy, but no IgA deposits. In contrast, biopsy of the native kidneys showed IgA deposits, but no BKvirus nephropathy. To our knowledge, this is the first reported case of a simultaneous liver-kidney transplanta-tion wherein both the native and transplant kidneys were biopsied posttransplantation and showed exclusivelydifferent pathologies. These findings confirm the predilection of BK virus nephropathy for transplant rather thannative kidneys.Am J Kidney Dis. 62(2):331-334. © 2013 by the National Kidney Foundation, Inc.
INDEX WORDS: Simultaneous liver-kidney transplant; immunoglobulin A (IgA) nephropathy; BK virusnephropathy.
Secondary immunoglobulin A (IgA) nephropathy(IgAN) is a well-known complication of liver
disease. Since it was first reported in the 1970s,1,2
kidney IgA deposition has been described in 33%-90% of patients with cirrhosis.3,4 Portosystemic anti-gen overload, intrinsic abnormalities of the IgA im-mune system, IgA complexes being shunted directlyto the systemic circulation due to portal hypertension,and defective liver IgA clearance all may contribute tothe development of IgAN in patients with liver dis-ease.5 Pooled biopsy and autopsy data suggest that50%-100% of patients with alcoholic cirrhosis havesome glomerular abnormalities on light microscopy.6
The light microscopic features of hepatic IgAN aresimilar to those of primary IgAN. Precise data arelimited due to the paucity of kidney biopsies inpatients with cirrhosis.
Patients with hepatic IgAN often are asymptom-atic. Secondary IgAN usually is thought to be benign,but hematuria and proteinuria in this setting are welldescribed. As with primary IgAN, the most commonurine abnormality in secondary IgAN is microscopichematuria. Nakamoto et al3 reported hematuria orproteinuria in 9.6% and nephrotic syndrome in 1.6%of a series of 752 patients with cirrhosis. The risk ofprogressive chronic kidney disease in hepatic IgANhas been reported to be low,6 but clearly some of thesepatients progress to chronic kidney failure.5
During the last decade, BK virus nephropathy in-creasingly has been recognized as an important cause
of decreased kidney function and transplant loss afterAm J Kidney Dis. 2013;62(2):331-334
kidney transplantation. The prevalence of BK virusnephropathy in kidney transplantation ranges from1%-10%.7 Reported rates of transplant loss rangefrom 10%-80%.7,8 Although most cases of BK virusnephropathy occur in transplant kidneys, a few casesof BK virus nephropathy in native kidneys has beendescribed in patients who underwent lung, pancreas,bone marrow, or heart transplantation.9 The preva-lence of BK viremia is lower in liver transplantrecipients compared with other solid-organ transplantrecipients, possibly due to the lower level of immuno-suppression used for livers.9
We report the case of a 60-year-old man whoreceived a simultaneous liver-kidney transplant andexperienced decreasing kidney function. Biopsy speci-mens of the native kidneys showed IgAN, but no BKvirus nephropathy. The transplant kidney biopsy speci-men showed BK virus nephropathy, but no IgAN. Toour knowledge, this is the first reported case of simul-taneous liver-kidney transplantation wherein both func-
From 1The Transplant Institute and 2Department of Pathology,Beth Israel Deaconess Medical Center, Boston, MA.
Received June 26, 2012. Accepted in revised form December 17,2012. Originally published online March 13, 2013.
Address correspondence to Didier A. Mandelbrot, MD, TheTransplant Institute, 110 Francis St, Boston, MA 02215. E-mail:[email protected]
© 2013 by the National Kidney Foundation, Inc.0272-6386/$36.00
http://dx.doi.org/10.1053/j.ajkd.2012.12.031331

ermin
Ujire et al
tioning native and transplant kidneys were biopsiedposttransplantation and showed different pathologies.This case also illustrates that BK virus nephropathy islimited to the transplant kidney and spares the nativekidneys.
CASE REPORTA 60-year-old man with end-stage liver disease from alcoholism
who had a serum creatinine (SCr) level of 1.1 mg/dL (correspond-ing to estimated glomerular filtration rate [eGFR] of 68 mL/min/1.73 m2 using the 4-variable Modification of Diet in Renal Disease[MDRD] Study equation) 2 weeks prior to evaluation was found tohave an SCr level of 2.9 mg/dL (eGFR, 22 mL/min/1.73 m2).Urinalysis showed 20-50 red blood cells, many of which weredysmorphic, and a urine protein-creatinine ratio of 0.4. Totalbilirubin level was 2.9 mg/dL, international normalized ratio was1.7, and platelets were 113 �103/�L. Ultrasound showed a 10.8-cmright kidney, 11.0-cm left kidney, and no other abnormalities.Kidney biopsy was not performed because of the risk of bleeding,but a presumptive diagnosis of IgAN was made. Medical historyincluded hypertension, hypercholesterolemia, aortic stenosis, anda chronic stable abdominal aortic aneurysm.
During the next 4 months, the patient’s bilirubin level increasedto 6.9 mg/dL, international normalized ratio increased to 2.6, andSCr level increased to 4.1 mg/dL (eGFR, 15 mL/min/1.73 m2), andhe underwent simultaneous liver-kidney transplantation. The imme-diate posttransplantation course was uncomplicated, with rapidnormalization of liver function test results and a SCr level nadir of0.9 mg/dL (eGFR, 86 mL/min/1.73 m2; Table 1). The initialimmunosuppressive regimen was tacrolimus (target level 10-15
Table 1. Laboratory Va
Pre-tx2 wk
Post-tx 4-6 wk Po
SCr (mg/dL) 4.1 0.9 2.2
eGFR (mL/min/1.73 m2) 15 86 31
Serum BK viral load(copies/mL)
— �500 15,000
Urine RBC count/hpf �20 �20 �20
Other findings Presumptivediagnosis:IgAN
— Tx Kidney bBKN, nokidney fu52% (Tx)(native)a
Abbreviations: BKN, BK virus nephropathy; eGFR, estimated glin A nephropathy; RBC, red blood cells; SCr, serum creatinine; T
aThe relative function of transplant and native kidneys was det
332
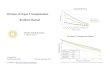
ng/mL), mycophenolate mofetil (1,000 mg twice a day), andprednisone (tapered to 10 mg/day). One month posttransplanta-tion, screening serum BK viral load was 1,200 copies/mL. Amodified renal MAG3 (mercaptuacetyltriglycine) scan10 showed52% function from the transplant kidney, 24% function from theright native kidney, and 24% function from the left native kidney,which suggested substantial recovery of native kidney function. Inthe following weeks, the patient’s SCr level increased to 2.2mg/dL (eGFR, 31 mL/min/1.73 m2) and BK viral load increased to15,000 copies/mL. Transplant kidney biopsy performed 6 weeksposttransplantation showed mild tubulitis, atypical tubular cells(Fig 1A), and a positive signal upon immunostaining for simianvirus 40 (SV40) T antigen (the anti-SV40 antibody cross-reactswith the T antigen of the BK polyomavirus; Fig 1B). Results ofimmunofluorescence studies were all negative.
The tacrolimus target level was decreased to 5-7 ng/mL, andmycophenolate therapy was discontinued 6 weeks posttranplanta-tion. However, the BK viral load continued to increase, reaching�50,000 copies/mL, so the patient was started on cidofovir, 0.5mg/kg, weekly. Two months posttransplantation, he developedtransaminitis and liver biopsy showed mild cellular rejection. Hereceived high-dose steroids and the tacrolimus target level wasincreased to 10 ng/mL. Repeat liver biopsy was performed due topersistent transaminitis and showed bile duct proliferation andneutrophilic infiltration. This biopsy was consistent with drugtoxicity and possible biliary obstruction, so cidofovir therapy wasdiscontinued. Endoscopic retrograde cholangiopancreatographywas performed and a stent was placed in the common bile duct,which led to subsequent normalization of liver function testresults. Gradually, the BK viral load increased to 134,000 and SCrlevel increased to 4.0 mg/dL (eGFR, 15 mL/min/1.73 m2). Repeat
nd Findings Over Time
10 wk Post-tx 3 mo Post-tx 7 mo Post-tx
4.0 4.0 2.5
15 15 26
134,000 22,000 �500
�2 �2 �2
y:;n:
Tx kidney biopsy:BKN, no IgAN
Native kidneybiopsy:IgAN, noBKN
Native kidney biopsy:IgAN, no BKN;Kidney function:42% (Tx), 58%(native)a
rular filtration rate; hpf, high-powered field; IgAN, immunoglobu-nsplantation.ed by renal MAG3 (mercaptuacetyltriglycine) scan.
Figure 1. Biopsy specimenfrom transplant kidney. (A) Lightmicroscopy (original magnifica-tion, �40) shows focal tubulitis andepithelial cells with viral cytopathicchanges (arrow). (B) Positive sim-ian virus 40 staining. (Immunoper-oxidase; original magnification,
lues a
st-tx
iopsIgANnctio, 48%
lomex, tra
�40.)
Am J Kidney Dis. 2013;62(2):331-334

Posttransplantation IgA and BK Virus Nephropathy
transplant kidney biopsy performed 10 weeks posttransplantationshowed increased tubulitis, nuclear atypia, and positive SV40staining. By this time, hematuria had resolved and did not recur.
The cause of such an increase in SCr level was unclear becausean early renal scan showed good native kidney function. There-fore, 3 months posttransplantation, a native kidney biopsy wasperformed. Light microscopy showed mesangial prominence andischemic changes (Fig 2A). Staining for SV40 in extensive amountsof cortical and medullary tissue gave negative results, and immuno-fluorescence results were positive for IgA only (Fig 2B). BK viralload was �22,000 copies/mL. For ongoing management of BKvirus nephropathy, tacrolimus was switched to sirolimus andprednisone was tapered to 5 mg daily.
Seven months posttransplantation, the patient’s BK viral loadbecame undetectable and SCr level stabilized around 2.5 mg/dL(eGFR, 26 mL/min/1.73 m2). Repeat native kidney biopsy againgave negative results for SV40 immunostaining, but positivesignal for IgA immunofluorescence. BK viral load remained unde-tectable at the time of writing this report.
DISCUSSION
We believe that our case is unique for severalreasons. To our knowledge, this is the only case in theliterature in which both the functioning native and thetransplant kidneys were biopsied after simultaneousliver-kidney transplantation and showed mutually ex-clusive pathologies. In addition, this appears to be thefirst case in which sequential native kidney biopsieswere performed after liver transplantation in a patientwith hepatic IgAN. This case also confirms by biopsythat BK virus nephropathy is a disease more likely toaffect transplant kidneys than native kidneys. Thisfinding likely is due to the “2-hit hypothesis,” whichstates that both immunosuppression and kidney dam-age related to transplantation surgery are required forBK virus nephropathy to develop.11,12 Immunosup-pression alone, whether used to treat autoimmunediseases or nonkidney solid-organ transplantation,rarely causes BK virus nephropathy.12 In addition,transplantation between identical twins involves isch-emic damage and denervation of the kidney, but doesnot require immunosuppression, and BK virus ne-phropathy has not been reported in this context.
There is no specific treatment for hepatic IgAN.Liver transplantation has been reported to improve
Figure 2. Biopsy specimenfrom native kidney. (A) Light mi-croscopy (hematoxylin and eosin;original magnification, �40) showsglomeruli with mildly expandedmesangium together with capillarycollapse, basement membranewrinkling, and occasional doublecontours. (B) Positive immuno-globulin A immunofluorescence.(Original magnification, �40.)
urinary abnormalities.13,14 After liver transplantation,
Am J Kidney Dis. 2013;62(2):331-334
portosystemic shunting disappears and IgA clearanceshould improve, which possibly leads to the resolu-tion of kidney IgA deposits, but to our knowledge,there are no reported cases with sequential biopsies toconfirm this.
We did not perform a pretransplantation kidneybiopsy, but we believe that our patient developedhepatic IgAN before transplant surgery and that thiscondition remained apparent in the posttransplanta-tion biopsy specimens of the native kidney. The lackof IgA deposits in the transplant kidney suggests thatthe transplanted liver cured the primary cause ofIgAN, thereby preventing further IgA deposition inthe transplant kidney. Of note, recurrent IgA depositsin the transplant kidney are extremely common intransplant recipents who receive a kidney alone totreat end-stage renal disease caused by primaryIgAN.15 The absence of IgA deposits on multipletransplant biopsy specimens after simultaneous liver-kidney transplantation in our patient is consistent withhis having secondary IgAN rather than primary IgAN.Similar to prior reports, our patient’s hematuria re-solved 2 months after simultaneous liver-kidney trans-plantation, which is consistent with the successfulliver transplant having removed the primary stimulusfor IgAN. The persistence of IgA deposits in ourpatient’s repeat native kidney biopsy specimen at 7months posttransplantation suggests that these depos-its will either take longer to resolve or will remainindefinitely. In addition, despite the relatively rapidresolution of hematuria, significant scarring of thenative kidneys remained.
Liver transplants are unique among organ trans-plants in that some recipients of simultaneous liver-kidney transplantation show substantial recovery ofnative kidney function after combined organ transplan-tation.16 Our patient provided an unusual opportunitybecause we were able to demonstrate recovery of thenative kidneys, and then biopsies of both the nativeand transplant kidneys were clinically indicated. Inperforming these biopsies, we provide a unique ex-ample in which BK virus nephropathy was present in
only the transplant kidney, but not in the native333

Ujire et al
kidneys, despite prolonged viremia. These findingsconfirm the previously postulated predilection of BKvirus nephropathy for transplant over native kidneys.
ACKNOWLEDGEMENTSSupport: This work was supported by the Julie Henry Research
Fund in the Transplant Institute at Beth Israel Deaconess MedicalCenter.
Financial Disclosure: The authors declare that they have norelevant financial interests.
REFERENCES1. Callard P, Feldman G, Prandi P, et al. Immune complex type
glomerulonephritis in cirrhosis of the liver. Am J Pathol. 1975;80:329-340.
2. Berger J, Yaneva H, Nabarra B. Glomerular changes inpatients with cirrhosis of the liver. Adv Nephrol. 1977;7:3-14.
3. Nakamoto Y, lida H, Kobayashi K, et al. Hepatic glomerulo-nephritis. Characteristics of hepatic IgA glomerulonephritis as themajor part. Virchows Arch (A). 1981;392:45-54.
4. Sinniah R. Heterogeneous IgA glomerulonephropathy inliver cirrhosis. Histopathology. 1984;8:947-962.
5. Pouria S, Barratt J. Secondary IgA nephropathy. SeminNephrol. 2008;28:27-37.
6. Newell GC. Cirrhotic glomerulonephritis: incidence, morphol-ogy, clinical features, and pathogenesis. Am J Kidney Dis. 1987;9:183-190.
7. Hirsch HH, Brennan DC, Drachenberg CB, et al. Polyomavi-
rus associated nephropathy in renal transplantation: interdisciplin-334
ary analyses and recommendations. Transplantation. 2005;79:1277-1286.
8. Ramos E, Drachenberg CB, Papadimitriou JC, et al. Clinicalcourse of polyoma virus nephropathy in 67 renal transplant pa-tients. J Am Soc Nephrol. 2002;13:2145-2151.
9. Munoz P, Fogeda M, Bouza E, et al. Prevalance of BK virusreplication in recipients of solid organ transplants. Clin Infect Dis.2005;41(12):1720-1725.
10. Palmer MR, Donohoe KJ, Francis JM, Mandelbrot D.Evaluation of relative renal function for patients who had under-gone simultaneous liver-kidney transplants using Tc-99m-MAG3scintigraphy with attenuation correction from anatomical imagesand SPECT/CT. Nucl Med Commun. 2011;32(8):738-744.
11. Fishman JA. BK virus nephropathy—polyomavirus addinginsult to injury. N Engl J Med. 2002;347:527-530.
12. Pendse SS, Vadivel N, Ramos E, et al. BK viral reactivationin cardiac transplant patients: evidence for a double-hit hypothesis.J Heart Lung Transplant. 2006;25:814-819.
13. Noble-Jmieson G, Thiru S, Johnston P, Friend P, Barnes N.Glomerulonephritis with end stage liver disease in childhood.Lancet. 1992;339:706-707.
14. Ghabra N, Piraino B, Greenberg A, Banner B. Resolution ofcirrhotic glomerulonephritis following successful liver transplanta-tion. Clin Nephrol. 1991;35(1):6-9.
15. Ortiz F, Gelpi R, Koskinen P, et al. IgA nephropathy recursearly in the graft when assessed by protocol biopsy. Nephrol DialTransplant. 2012;27(6):2553-2558.
16. Francis J, Palmer R, Donohoe K, et al. Evaluation of nativekidney recovery after simultaneous liver- kidney transplantation.
Transplantation. 2012;93:530-535.Am J Kidney Dis. 2013;62(2):331-334
Recommended