ENDOCRINE

JOHN MINARCIK, MD
• [email protected]• http://snurl.com/pathology
• OPTIONAL– youtube.com “histopathology”– youtube.com “shotgun histology”

CLASSICAL ALGORHYTHM• PITUITARY
– ANTERIOR– POSTERIOR
• THYROID• PARATHYROID• PANCREAS (endo.)• ADRENAL
– CORTEX– MEDULLA
• DEGENERATION (aka, “involution”)
• INFLAMMATION
• NEOPLASM– BENIGN
– MALIGNANT

BETTER ALGORHYTHM• NON-NEOPLASTIC
– HYPER-function– HYPO-function
• NEOPLASTIC– FUNCTIONAL– NON-FUNCTIONAL– Functional endocrine
malignancies are RARE. Why?
• PITUITARY– ANTERIOR– POSTERIOR
• THYROID
• PARATHYROID
• PANCREAS (endo.)
• ADRENAL– CORTEX– MEDULLA

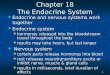
FEEDBACK SYSTEMS• HYPOTHALAMUS • ANTERIOR PITUITARY • ENDOCRINE GLAND • END ORGAN • HYPOTHALAMUS



HORMONES•POLYPEPTIDE (2nd MESSENGER)
•STEROID (DIRECT on NUCLEUS)

ACIDOPHILS
BASOPHILS
CHROMOPHOBES
AXONS
AXONS and “PITUI-”cytes
A
I P


ANTERIOR PITUITARY• ACIDOPHILS
–GROWTH HORMONE
–PROLACTIN
• BASOPHILS–TSH
–ACTH
–LH, FSH


POSTERIOR PITUITARY
• OXYTOCIN (contracts uterine smooth muscle)
• VASOPRESSIN (ADH) (vasoconstriction, gluconeogenesis, platelet aggregation, release of Factor-VIII and vWb factor, concentrates urine, main effects on kidney and brain)

PITUITARY PATHOLOGY
• CLINICAL FEATURES, mimic the endocrine effects or mass effects)
• FUNCTIONING ADENOMAS
• HYPO-PITUITARISM
• POSTERIOR PITUITARY SYNDROMES
• HYPOTHALAMIC (SUPRASELLAR) TUMORS

CLINICAL FEATURES• HYPER: growth, lactation, thyroid,
adrenal cortex
• HYPO: growth, thyroid, adrenal cortex
• MASS EFFECT: visual fields, brain


G
A
L
A
C
T
O
R
R
H
E
A

GIGANTISM
(excess somatotropin [GH]
BEFORE
epiphyseal
closure)

ACROMEGALY:
(excess somatotropin
[GH] AFTER epiphyseal closure)

MOON FACIES
BUFFALO HUMP
STRIAE



BITEMPORAL
HEMIANOPSIA


HYPO-pituitarism• Pituitary tumors, functional or not.• NON-pituitary tumors, primary or metastatic• Pituitary surgery, of course• Radiation, of course• “Apoplexy”, i.e., sudden hemorrhage• Sheehan’s syndrome (Post-partum ischemic
necrosis)• Cysts (Rathke’s cleft)• Empty sella syndrome, (is NOT a disease)• Genetic defects (pit-1 gene mutations)

POSTERIOR pituitary•DIABETES INSIPIDUS
•SIADH (Syndrome of Inappropriate Andi- Diuretic Hormone)

DIABETES INSIPIDUS
• ADH deficiency• Head trauma, tumors,
inflam. hypothal/pit• Hyperdiureses with
LOW sp.gr.

Inappropriate ADH• ADH EXCESS
–Hyponatremia, cerebral edema, neurologic symptoms
–Neoplasms, esp. Small Cell CA.
–NON-neoplastic lung diseases
–Posterior pituitary injury


15-25 grams


HYPER-THYROIDISM• aka, thyrotoxicosis
• Diffuse
• Nodular
• Adenoma
• Carcinoma
• Neonatal
• Secondary to TSH pituitary adenoma

HYPER-THYROIDISM• HYPERMETABOLISM
• Tachycardia, palpitations
• Increased T3, T4
• Goiter
• Exophthalmos
• Tremor
• GI hypermotility
• Thyroid “storm”, life threatening


HYPO-THYROIDISM• 1° Developmental
• 1° Surgery, I-131, external radiation
• 1° Auto-immune (i.e., Hashimoto’s)
• 1° Iodine deficiency
• 1° Li+, iodides, p-aminosalicylates
• 2° (pituitary)
• 3° (hypothalamic, rare)

HYPO-THYROIDISM
• Cretinism– Severe retardation– CNS/Musc-skel– Short stature– Protruding tongue– Umbilical hernia
• Myxedema (coma)– Sluggishness– Cool skin

THYROIDITIS• Hashimoto (Auto-Immune) (Lymphoid
follicles with germinal centers), MOST COMMON cause of acquired hypothyroidism in USA
• Subacute Granulomatous (DeQuervain)
• Subacute Lymphocytic (just like Hashimoto’s but NO fibrosis and no germinal centers), often post-partum




GRAVES DISEASE(aka, diffuse toxic goiter)
• HYPERTHYROIDISM
• EXOPHTHALMOS
• PRE-TIBIAL MYXEDEMA
• Autoimmune, auto-antibodies to TSH


SCALLOPING


GRAVES DISEASE(aka, diffuse toxic goiter)
PLUMMER DISEASE(aka, nodular toxic goiter)
HARDER TO TREAT
Surg
PTU (Propyl Thio Uracil)
I-131

GOITERS(aka, thyromegaly, diffuse or nodular)
• IODINE deficiency
• Increased TSH
• Goitrogens, e.g., cabbage, Brussels sprouts, cauliflower, turnips, cassava)
• Associated with HYPO thyroidism eventually, NOT hyperthyroidism


GOITER

Thyroid Neoplasms• “Nodules” vs. true neoplasms
• Adenomas vs. Carcinomas

“NODULES”• Solitary vs. Multiple
• Younger vs. Older
• Male vs. Female
• Hx. neck radiation vs. NO Rx.
• “Cold” vs. HOT (really NOT-cold)


NEOPLASMS• ADENOMAS
–FOLLICULAR–HÜRTHLE
(oxyphilic)
• CARCINOMAS
–FOLLICULAR–PAPILLARY– MEDULLARY
(AMYLOID)– ANAPLASTIC
(worst)



HÜRTHLE CELL ADENOMA, note “atypia”





ORPHAN ANNIE CELLS in PAPILLARY CARCINOMA

MEDULLARY CARCINOMA of the thyroid with “HYALINIZATION”, i.e.,
AMYLOID!!!

HYALINIZATION showing APPLE GREEN birefringence in CONGO RED stain, i.e., AMYLOID

BIOLOGIC BEHAVIOR• Papillary CA lymph nodes
• Follicular CA blood vessels, bone

35-40 mg

PTH• HYPOCALCEMIA is MAIN
STIMULUS (9-10.5 mg/dl)
• ANTAGONIZES CALCITONIN

PARATHYROID DISORDERS
• HYPER-–PRIMARY (usually adenomas)
–SECONDARY (LOW CA++ of Renal Failure)
• HYPO-: Surgical, congenital, familial, idiopathic
• PSEUDO-HYPO-–(end organ resistance)

HYPER-PARATHYROIDISM
• Bone pain, fractures
• Nephrolithiasis
• Constipation, ulcers, gallstones
• Depression, lethargy
• Weakness, fatigue
• Valve calcifications

HYPO-PARATHYROIDISM
• Neuromuscular irritability
• Mental status change
• Parkinsonism like effects
• Lens calcification* (paradox)
• Widened QT interval
• Defective, carious, teeth

ADRENAL CORTEX• Glomerulosa (Salt), mineralocorticoids
– ALDOSTERONE
• Fasciculata (Sugar), glucocorticoids– CORTISOL
• Reticularis (Sex), gonadocorticoids– ANDROGENS, ESTROGENS


4 g.

SALT
SUGAR
SEX
STRESSSTRESS

HYPERADRENALISM• HYPERALDOSTERONISM
• CUSHING SYNDROME (CORTISOL)
• ADRENOGENITAL (VIRILIZING) SYNDROME

CUSHING SYNDROME
• CENTRAL OBESITY• MOON FACIES• WEAKNESS• HIRSUTISM• HYPERTENSION• DIABETES• OSTEOPOROSIS• STRIAE

MOON FACIES
BUFFALO HUMP
STRIAE

CUSHING SYNDROME
• PITUITARY ACTH INCREASE• TUMOR ACTH INCREASE• HYPERPLASIA OF CORTEX• ADENOMA OF CORTEX• CARCINOMA OF CORTEX
•EXOGENOUS STEROIDS (90%)

PRIMARY HYPERALDOSTERONISM
(Conn’s Syndrome)
• Na+ RETENTION• K+ EXCRETION• HYPERTENSION

PRIMARY HYPERALDOSTERONISM
• CORTICAL NEOPLASM• CORTICAL HYPERPLASIA• FAMILIAL (rare)

SECONDARY HYPERALDOSTERONISM
• DECREASED RENAL PERFUSION
• EDEMA (HEART, LIVER, KIDNEY)
• PREGNANCY

ADRENOGENITAL SYNDROME
• VIRILIZATION/feminization• CORTICAL NEOPLASM• CORTICAL HYPERPLASIA• 21-Hydroxylase Deficiency


ADRENAL INSUFFICIENCY
• PRIMARY ACUTE (ADRENAL CRISIS)
• PRIMARY CHRONIC (ADDISON DISEASE)
• SECONDARY (PITUITARY)

PRIMARY ACUTE• RAPID WITHDRAWAL OF STEROIDS
• MASSIVE ADRENAL HOMORRHAGE (WATERHOUSE-FRIDERICHSEN, if it follows infection and shock)– Newborns with DIFFICULT DELIVERY
– ANTICOAGULANT RX
– POSTSURGICAL DIC PATIENTS

PRIMARY CHRONIC• Most of Addison disease is auto-
immune adrenalitis• INFECTIONS
• METASTASES
• GENETIC DISORDERS

NEOPLASMS• ADENOMAS of ADRENAL
CORTEX
• CARCINOMAS of ADRENAL CORTEX





ADRENAL MEDULLA• PHEOCHROMOCYTOMAS, aka,
primary tumors of the adrenal medulla– 10% arise in an MEN setting
– 10% are EXTRA-adrenal
– 10% are bilateral
– 10% are malignant
– 10% are in childhood
– You can only call them malignant if they metastasize

PHEO

TWO crucially important points specific for endocrine tumors:
• 1. FUNCTIONING carcinomas are very RARE in ANY endocrine gland. Why? (KEY principle of oncology)
• 2. Benign adenomas may have extremely bizarre nuclei, but are most usually BENIGN!!!

MEN-1, aka, Wermer Syndrome (3 P’s)
• HYPERPARATHYROIDISM, chiefly hyperplasia
•Pancreatic endocrine tumors
•Pituitary adenoma, usually prolactinoma

MEN-2• MEN-2A (SIPPLE): Pheo,
Medullary CA., Parathyroid hyperplasia
• MEN-2B: NO hyperparathyroidism, but neuromas present
• Familial Medullary Thyroid CA

PINEAL “GLAND”• PINEALOMAS
–PINEOBLASTOMAS
–PINEOCYTOMAS



ENDOCRINE
PANCREAS

Exocrine
Endocrine
Islets
Alpha Cells
Beta Cells
Delta Cells (suppress insulin and glucagon)
Pancreatic Polypeptide (PP) cells
Epsilon Cells make
gherlin

DIABETES MELLITUS
• 16 Million in the USA
• 1 Million/yr
• 50K people die of it per year in the USA

How to Diagnose Dm:
• Glucose >200
• Or…………….
• Fasting glucose >126 trice
• Or…………….
• Post-prandial glucose > 200, 2 hrs AFTER standard OGTT (Oral Glucose Tolerance Test)

TWO* Types of DM•1• Genetic• Autoimmune• Childhood (juvenile)
onset• Antibodies to beta
cells• Beta cell depletion• NON-OBESE
patients
•2• Genetic, but diff. from
Type 1• NOT autoimmune• Adult, or maturity
onset, e.g., 40’s, 50’s• Insulin may be low,
BUT, peripheral resistance to insulin is the main factor
• OBESE patients
* MODY might be regarded as the third type

Dm•POLY-
•POLY-
•POLY-

INSULIN• FAT
– IN-creased glucose uptake– IN-creased lipogenesis– DE-creased lipolysis
• MUSCLE– IN-creased glucose uptake– IN-creased glycogen synthesis– IN-creased protein synthesis
• LIVER– DE-creased gluconeogenesis– IN-creased glycogen synthesis– IN-creased lipogenesis

PATHOGENESIS• 1• T-Lymphocytes
reacting against poorly defined beta cell antigens
• Inflammatory inflitrate, chronic, i.e., “INSULITIS”
• 2• Diet• Life Style• Obesity• INSULIN
RESISTANCE• Beta cells UN-able
to adapt to the “long term demands of insulin resistance”

MODY (Maturity Onset Diabetes of the Young)
• Multiple types
• 2-5% of diabetics
• Primary beta cell defects
• Multiple genetic mechanisms, especially GLUCOKINASE mutations

PANCREAS in Dm

PANCREAS in Dm

COMPLICATIONS• MACRO-VASCULAR disease, i.e.,
ASCVD
• MICRO-VASCULAR disease, kidneys, retina, nerves
• IMMUNE related problems, INFECTIONS, e.g., TB, pneumonia, pyelonephritis, candida, etc.

COMPLICATIONS• ADVANCED GLYCATION
– collagen, laminin, polypeptides, GBM (glomerular basement membrane)
• ACTIVATION of PROTEIN KINASE C, VEGF, endothelin-1, increased ECM, decreased fibrinolysis, inflam. cytokines
• INTRACELLULAR HYPERGLYCEMIA

COMPLICATIONSMORPHOLOGY
• (MACRO-vascular) Atherosclerosis• MICRO-vascular
– Retinopathy– Nephropathy- glomerular, vascular, KW– Neuropathy
• Infections

ATHEROSCLEROSIS

ATHEROSCLEROSIS

RETINOPATHY in DmShows microaneurysms,
areas of hemorrhage,
cotton wool spots, hard exudates, venous beading, neovascularization, retinal detachment, vitreous detachment, pre retinal hemorrhage


NEPHROPATHYKimmelstiel-Wilson (KW) Kidneys
Is…………
“Nodular” glomerulosclerosis

NEPHROPATHYNEPHROSCLEROSIS

NEPHROPATHYGBM thickening

NEPHROPATHYDiffuse
Mesangial
Sclerosis

INFECTIONS in Dm• SKIN
• TUBERCULOSIS
• PNEUMONIA
• PYELONEPHRITIS
• CANDIDA

NEOPLASMS of the Endocrine Pancreas
• Islet cell tumors– Beta cells INSULINOMAS (NOT rare)
– Alpha cells GLUCAGONOMAS (rare)
– Delta cells SOMATOSTATINOMAS (rare)
– GASTRINOMAS, producing ZOLLINGER-ELLISON SYNDROME, consisting of increased acid and ulcers
Recommended