Embed Size (px)
Citation preview

(IVF) programs. While blastocyst culture was created for the selection oftwo competent embryos for ET, extended culture has not replaced tradi-tional protocols in a large number of laboratories. Elective transfer of twoembryos on Day-3 ET may offer superior results. For this study we corre-lated pregnancy rates with embryo quality and examined pregnancy rateswith two vs. three embryos transferred on Day-3 ET.
Design: A retrospective analysis of pregnancy rates related to embryoquality and the number of embryos selected for ET.
Materials and Methods: IVF outcome vs. embryo quality was assessed incycles in 1999 where ET occurred on Day-3 (Group 1, N5 178). Pregnancyrates with two vs. three embryo ET were also compared (Group 2). Embryoquality was based on morphological “grade” relating to fragmentation andblastomere size, and cleavage rates (quality5 cleavage rate3 grade). Allstatistics were based on the quality of the lead (best) embryo transferred.Clinical pregnancy was defined as the presence of a gestational sac onultrasound examination.
Results: Analysis of Group 1 data revealed that lead embryo quality wasdirectly related to clinical pregnancy outcome (P,0.01, Spearman RankCorrelation) and it appeared that pregnancy rates were maximal with leadembryo scores of$10.7 ($7-cell embryo with good morphology). Thus,only patients with a lead embryo score of$10.7 were included in Group 2(results summarized in Table 1). Pregnancy rates with two or three embryoET were not different (P5 0.48, Chi Square). There was a definite trendtowards reduction in multiple pregnancy with two vs. three embryo ET (notstatistically significant, P5 0.24). The incidence of higher-order multiplepregnancy ($triplets) was further reduced with the two embryo ET group(P 5 0.08).
Table 1. Clinical pregnancy (pg) rates with 2 vs. 3 embryo ET on Day-3with lead embryo quality$10.7. Percentages are given as # pregnancies/ET.
# Embryos/ET NAvg.age
# Pg(%)
# Multiple(%)
# $Triplet(%)
2 15 33 7 (47) 2 (13) 0 (0)3 49 33 28 (57) 15 (31) 9 (18)
Discussion: These data provide compelling evidence that, with carefulembryo quality assessment, two embryo ET on Day-3 can provide equalpregnancy rates to three embryo ET and reduce the incidence of multiplepregnancies. Our sample size is modest, but these results illustrate analternative to extended embryo culture for patients at risk for multiplepregnancy.
P-224
Blastocyst Culture and Transfer Maintain Pregnancy Rate but Reducethe Risk of a High Order Multiple Gestation. C. McCaffrey, A. S.Berkeley, D. Grimes, A. Adler, L. Chi, L. C. Krey. Program for In VitroFertilization, Reproductive Surgery and Infertility. New York UniversitySchool of Medicine, New York, NY.
Objectives: Transfer of 3 or more embryos in assisted reproduction isassociated with a significant risk for a high order multiple gestation. Strat-egies proposed to reduce such multiple pregnancies include limiting trans-fers to 2 embryos either on day 3 (D3) or, following extended embryoculture, on day 5 (D5), at which time blastocyst stage embryos can be se-lected. This study’s objective is to determine if, in a select group of patients,embryo culture to D5 using sequential media would reduce the incidence ofhigh order multiple gestations while maintaining a high pregnancy rate.
Design: A group of patients (n516) scheduled for IVF were prospec-tively selected based on the following criteria:#36 years old; no PCOS; andno male factor infertility necessitating ICSI. Clinical pregnancy and im-plantation rates in 1999 for similar patients in our practice with D3 embryotransfer were 57% and 34%, respectively.
Materials and Methods: Patients were treated with several stimulationprotocols but all were down-regulated with a low dose Lupront protocolbegun in the luteal phase. Oocytes were retrieved 36 h after hCG injectionand inseminated in HTF1 6% Plasmanatet. At fertilization check zygotes(2 pn) were rinsed 43 and placed in 50ml droplets of G1 media (ZanderIVF) under oil and cultured until D3. If there was#3 embryos on D3,embryo transfer was performed that day. Otherwise, embryos of similarcleavage stage and quality were grouped, rinsed 43 in G2 and cultured until
D5 in 50ml droplets of G2 under oil. Morula/blastocyst development wasevaluated using compaction or expansion, as well as cell number and qualityof the trophectoderm and inner cell mass. The most advanced and/or bestquality blastocysts were selected for transfer. When excellent quality blas-tocysts were available, 2 embryos were replaced; if only moderate to poorquality blastocysts or morulae, 3 embryos were replaced. A clinical preg-nancy was defined by fetal heartbeat.
Results: One patient was converted to a 2 embryo transfer on D3 and ispregnant with a singleton. The remaining 15 patients had a D5 embryotransfer; 9 have ongoing clinical pregnancies (60% rate); one additionalpatient had an ectopic pregnancy. Six patients had 2 embryos replaced; allare pregnant and two have a twin pregnancy. Nine patients had 3 embryosreplaced resulting in one twin pregnancy and two triplet pregnancies.Overall, the blastocyst implantation rate was 44%; the rates were 67% and33%, respectively, for the 2 and 3 blastocyst transfer groups.
Conclusion: Embryo transfer on D5 resulted in a comparable pregnancyrate but a higher implantation rate than transfer on D3. Since culture to D5allows better selection of embryos for transfer, a 2 embryo transfer shouldbe sufficient to maintain a high pregnancy rate while reducing the rate ofhigh order multiple gestations. In this study, the transfer of only 2 blasto-cysts would have had no effect on the absolute pregnancy rate but wouldhave prevented two sets of triplets.
P-225
The Relation of the Maturity of Retrieved Oocytes and DevelopmentalVelocity of Embryos with Pregnancy Rates in IVF-ET Program.1S. Han,1M. K. Kim, 1D. H. Kim, 1H. G. Kang,2W. I. Park,2H. C. Kwon.1Eulji Medical Science Institute, Eulji Medical Center, Seoul,2Departmentof Obstetrics/Gynecology, and3Department of Physiology, School of Med-icine, Eulji University, Taejon, Korea.
Objectives: The aim of this study was to evaluate the relation betweenoocyte maturity and developmental velocity of embryos during 3 daysculture and pregnancy rates in IVF-ET program.
Design: A retrospective chart review of 119 cases of IVF-ET cases exceptICSI.
Materials and Methods: According to the oocyte maturity at ovum pick-up, all patients were divided into group A (MII, MI# 50%) and B (MII,MI . 50%). Thereafter, the groups were subdivided according to thedevelopmental velocity (the number of 6–8 cell embryo# 50% or.50%)and embryo quality (fragmentation or.50%). According to the develop-mental velocity (the number of 6–8 cell embryo) of the embryos on 3 day,same patients were also divided into group C (#50%) and D (.50%)respectively. Thereafter, the groups were subdivided according to the oocytematurity and embryo quality on the same basis of above criteria. The clin-ical outcomes were compared and analyzed by Student’s t-test and Fisher’sexact test.
Results: Between group A (n530) and B (n589), the respective fer-tilization rate (51.5 vs. 63.3%) and clinical pregnancy rate (23.3 vs. 41.6%)were significantly different (P,0.05). Other clinical outcomes were notsignificantly different. The developmental velocity was closely related withincreased clinical pregnancy rate only in group B (6/23 vs. 31/66), not ingroup A (2/12 vs. 5/18). However, the embryo quality was not related withthe clinical pregnancy in both groups (22/51 vs. 15/38 and 3/16 vs. 4/14).Between group C (n535) and D (n584), there was significant difference inthe clinical pregnancy rate (23.3 vs. 41.6%; P,0.05), while other clinicaloutcomes were not significantly different. The oocyte maturity was relatedwith the increased clinical pregnancy rate only in group D (5/18 vs. 31/66),not in group C (2/12 vs. 6/23). Embryo quality was related with theincreased the clinical pregnancy rate in group C (3/21 vs. 5/14), not in groupD (26/57 vs. 10/27).
Conclusions: Our data showed that consecutive developmental velocityof embryo were more positively related to clinical pregnancy rate thanquality of embryo. Therefore, developmental velocity of embryo should beconsidered prior to quality of embryo in IVF-ET program.
P-226
Zygote Morphology Does Not Correlate with Embryo Quality in Hu-mans. N. Prados, R. Herrer, A. Cobo, A. Ruiz, J. Remohı´, A. PellicerInstituto Valenciano de Infertilidad and Department of Obstetrics/Gynecol-ogy, School of Medicine, Valencia, Spain.
S166 Abstracts Vol. 74, No. 3, Suppl. 1, September 2000
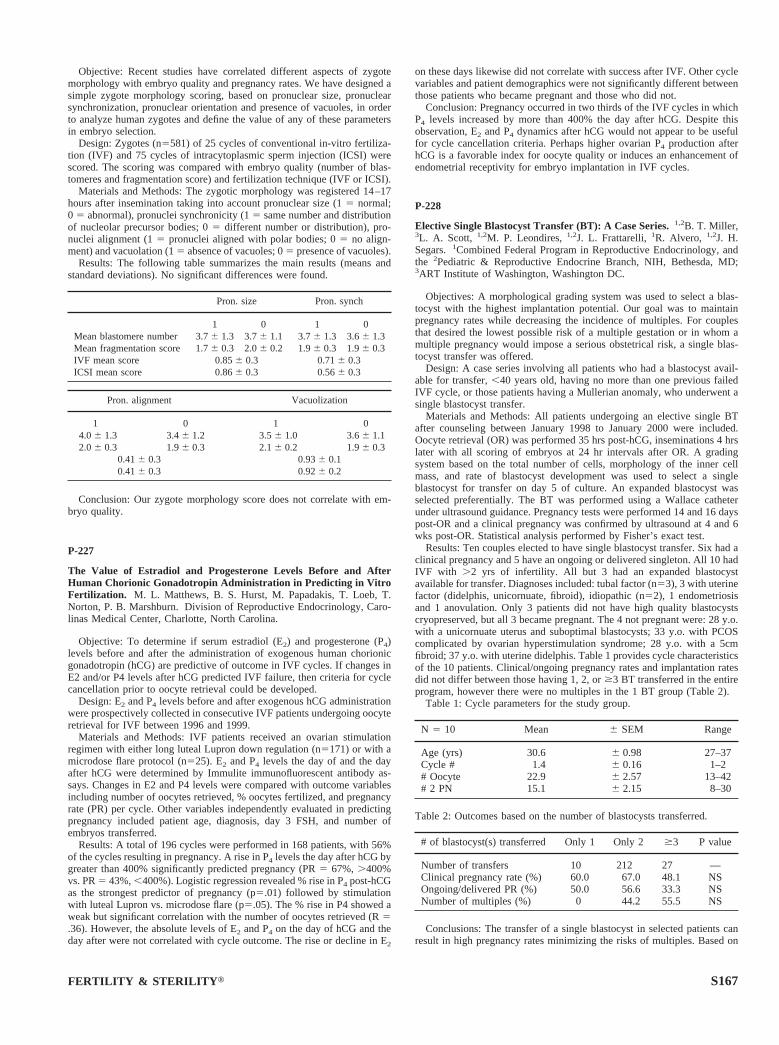
Objective: Recent studies have correlated different aspects of zygotemorphology with embryo quality and pregnancy rates. We have designed asimple zygote morphology scoring, based on pronuclear size, pronuclearsynchronization, pronuclear orientation and presence of vacuoles, in orderto analyze human zygotes and define the value of any of these parametersin embryo selection.
Design: Zygotes (n5581) of 25 cycles of conventional in-vitro fertiliza-tion (IVF) and 75 cycles of intracytoplasmic sperm injection (ICSI) werescored. The scoring was compared with embryo quality (number of blas-tomeres and fragmentation score) and fertilization technique (IVF or ICSI).
Materials and Methods: The zygotic morphology was registered 14–17hours after insemination taking into account pronuclear size (15 normal;0 5 abnormal), pronuclei synchronicity (15 same number and distributionof nucleolar precursor bodies; 05 different number or distribution), pro-nuclei alignment (15 pronuclei aligned with polar bodies; 05 no align-ment) and vacuolation (15 absence of vacuoles; 05 presence of vacuoles).
Results: The following table summarizes the main results (means andstandard deviations). No significant differences were found.
Pron. size Pron. synch
1 0 1 0Mean blastomere number 3.76 1.3 3.76 1.1 3.76 1.3 3.66 1.3Mean fragmentation score 1.76 0.3 2.06 0.2 1.96 0.3 1.96 0.3IVF mean score 0.856 0.3 0.716 0.3ICSI mean score 0.866 0.3 0.566 0.3
Pron. alignment Vacuolization
1 0 1 04.06 1.3 3.46 1.2 3.56 1.0 3.66 1.12.06 0.3 1.96 0.3 2.16 0.2 1.96 0.3
0.416 0.3 0.936 0.10.416 0.3 0.926 0.2
Conclusion: Our zygote morphology score does not correlate with em-bryo quality.
P-227
The Value of Estradiol and Progesterone Levels Before and AfterHuman Chorionic Gonadotropin Administration in Predicting in VitroFertilization. M. L. Matthews, B. S. Hurst, M. Papadakis, T. Loeb, T.Norton, P. B. Marshburn. Division of Reproductive Endocrinology, Caro-linas Medical Center, Charlotte, North Carolina.
Objective: To determine if serum estradiol (E2) and progesterone (P4)levels before and after the administration of exogenous human chorionicgonadotropin (hCG) are predictive of outcome in IVF cycles. If changes inE2 and/or P4 levels after hCG predicted IVF failure, then criteria for cyclecancellation prior to oocyte retrieval could be developed.
Design: E2 and P4 levels before and after exogenous hCG administrationwere prospectively collected in consecutive IVF patients undergoing oocyteretrieval for IVF between 1996 and 1999.
Materials and Methods: IVF patients received an ovarian stimulationregimen with either long luteal Lupron down regulation (n5171) or with amicrodose flare protocol (n525). E2 and P4 levels the day of and the dayafter hCG were determined by Immulite immunofluorescent antibody as-says. Changes in E2 and P4 levels were compared with outcome variablesincluding number of oocytes retrieved, % oocytes fertilized, and pregnancyrate (PR) per cycle. Other variables independently evaluated in predictingpregnancy included patient age, diagnosis, day 3 FSH, and number ofembryos transferred.
Results: A total of 196 cycles were performed in 168 patients, with 56%of the cycles resulting in pregnancy. A rise in P4 levels the day after hCG bygreater than 400% significantly predicted pregnancy (PR5 67%, .400%vs. PR5 43%,,400%). Logistic regression revealed % rise in P4 post-hCGas the strongest predictor of pregnancy (p5.01) followed by stimulationwith luteal Lupron vs. microdose flare (p5.05). The % rise in P4 showed aweak but significant correlation with the number of oocytes retrieved (R5.36). However, the absolute levels of E2 and P4 on the day of hCG and theday after were not correlated with cycle outcome. The rise or decline in E2
on these days likewise did not correlate with success after IVF. Other cyclevariables and patient demographics were not significantly different betweenthose patients who became pregnant and those who did not.
Conclusion: Pregnancy occurred in two thirds of the IVF cycles in whichP4 levels increased by more than 400% the day after hCG. Despite thisobservation, E2 and P4 dynamics after hCG would not appear to be usefulfor cycle cancellation criteria. Perhaps higher ovarian P4 production afterhCG is a favorable index for oocyte quality or induces an enhancement ofendometrial receptivity for embryo implantation in IVF cycles.
P-228
Elective Single Blastocyst Transfer (BT): A Case Series.1,2B. T. Miller,3L. A. Scott, 1,2M. P. Leondires,1,2J. L. Frattarelli,1R. Alvero, 1,2J. H.Segars.1Combined Federal Program in Reproductive Endocrinology, andthe 2Pediatric & Reproductive Endocrine Branch, NIH, Bethesda, MD;3ART Institute of Washington, Washington DC.
Objectives: A morphological grading system was used to select a blas-tocyst with the highest implantation potential. Our goal was to maintainpregnancy rates while decreasing the incidence of multiples. For couplesthat desired the lowest possible risk of a multiple gestation or in whom amultiple pregnancy would impose a serious obstetrical risk, a single blas-tocyst transfer was offered.
Design: A case series involving all patients who had a blastocyst avail-able for transfer,,40 years old, having no more than one previous failedIVF cycle, or those patients having a Mullerian anomaly, who underwent asingle blastocyst transfer.
Materials and Methods: All patients undergoing an elective single BTafter counseling between January 1998 to January 2000 were included.Oocyte retrieval (OR) was performed 35 hrs post-hCG, inseminations 4 hrslater with all scoring of embryos at 24 hr intervals after OR. A gradingsystem based on the total number of cells, morphology of the inner cellmass, and rate of blastocyst development was used to select a singleblastocyst for transfer on day 5 of culture. An expanded blastocyst wasselected preferentially. The BT was performed using a Wallace catheterunder ultrasound guidance. Pregnancy tests were performed 14 and 16 dayspost-OR and a clinical pregnancy was confirmed by ultrasound at 4 and 6wks post-OR. Statistical analysis performed by Fisher’s exact test.
Results: Ten couples elected to have single blastocyst transfer. Six had aclinical pregnancy and 5 have an ongoing or delivered singleton. All 10 hadIVF with .2 yrs of infertility. All but 3 had an expanded blastocystavailable for transfer. Diagnoses included: tubal factor (n53), 3 with uterinefactor (didelphis, unicornuate, fibroid), idiopathic (n52), 1 endometriosisand 1 anovulation. Only 3 patients did not have high quality blastocystscryopreserved, but all 3 became pregnant. The 4 not pregnant were: 28 y.o.with a unicornuate uterus and suboptimal blastocysts; 33 y.o. with PCOScomplicated by ovarian hyperstimulation syndrome; 28 y.o. with a 5cmfibroid; 37 y.o. with uterine didelphis. Table 1 provides cycle characteristicsof the 10 patients. Clinical/ongoing pregnancy rates and implantation ratesdid not differ between those having 1, 2, or$3 BT transferred in the entireprogram, however there were no multiples in the 1 BT group (Table 2).
Table 1: Cycle parameters for the study group.
N 5 10 Mean 6 SEM Range
Age (yrs) 30.6 6 0.98 27–37Cycle # 1.4 6 0.16 1–2# Oocyte 22.9 6 2.57 13–42# 2 PN 15.1 6 2.15 8–30
Table 2: Outcomes based on the number of blastocysts transferred.
# of blastocyst(s) transferred Only 1 Only 2 $3 P value
Number of transfers 10 212 27 —Clinical pregnancy rate (%) 60.0 67.0 48.1 NSOngoing/delivered PR (%) 50.0 56.6 33.3 NSNumber of multiples (%) 0 44.2 55.5 NS
Conclusions: The transfer of a single blastocyst in selected patients canresult in high pregnancy rates minimizing the risks of multiples. Based on
FERTILITY & STERILITY t S167



















![EPRODUCTION IN NIMALS D · 2019-04-11 · 104 SCIENCE Development of Embryo Fertilisation results in the formation of zygote which begins to develop into an embryo [Fig. 9.8(a)]](https://img.dokumen.tips/doc/110x75/5ea4a83f0ada486f871666aa/eproduction-in-nimals-d-2019-04-11-104-science-development-of-embryo-fertilisation.jpg)









