Embed Size (px)
Citation preview
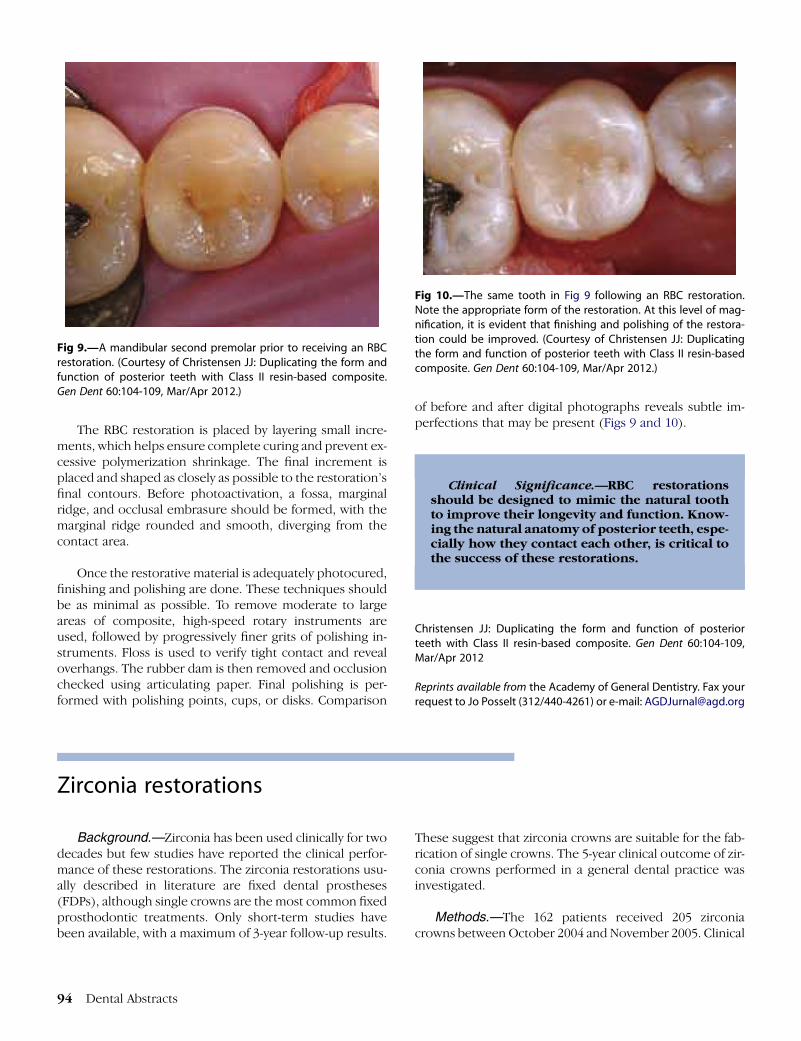
Fig 9.—A mandibular second premolar prior to receiving an RBCrestoration. (Courtesy of Christensen JJ: Duplicating the form andfunction of posterior teeth with Class II resin-based composite.Gen Dent 60:104-109, Mar/Apr 2012.)
Fig 10.—The same tooth in Fig 9 following an RBC restoration.Note the appropriate form of the restoration. At this level of mag-nification, it is evident that finishing and polishing of the restora-tion could be improved. (Courtesy of Christensen JJ: Duplicatingthe form and function of posterior teeth with Class II resin-basedcomposite. Gen Dent 60:104-109, Mar/Apr 2012.)
The RBC restoration is placed by layering small incre-ments, which helps ensure complete curing and prevent ex-cessive polymerization shrinkage. The final increment isplaced and shaped as closely as possible to the restoration’sfinal contours. Before photoactivation, a fossa, marginalridge, and occlusal embrasure should be formed, with themarginal ridge rounded and smooth, diverging from thecontact area.
Once the restorative material is adequately photocured,finishing and polishing are done. These techniques shouldbe as minimal as possible. To remove moderate to largeareas of composite, high-speed rotary instruments areused, followed by progressively finer grits of polishing in-struments. Floss is used to verify tight contact and revealoverhangs. The rubber dam is then removed and occlusionchecked using articulating paper. Final polishing is per-formed with polishing points, cups, or disks. Comparison
94 Dental Abstracts
of before and after digital photographs reveals subtle im-perfections that may be present (Figs 9 and 10).
Clinical Significance.—RBC restorationsshould be designed to mimic the natural toothto improve their longevity and function. Know-ing the natural anatomy of posterior teeth, espe-cially how they contact each other, is critical tothe success of these restorations.
Christensen JJ: Duplicating the form and function of posteriorteeth with Class II resin-based composite. Gen Dent 60:104-109,Mar/Apr 2012
Reprints available from the Academy of General Dentistry. Fax yourrequest to Jo Posselt (312/440-4261) or e-mail: [email protected]
Zirconia restorations
Background.—Zirconia has been used clinically for twodecades but few studies have reported the clinical perfor-mance of these restorations. The zirconia restorations usu-ally described in literature are fixed dental prostheses(FDPs), although single crowns are the most common fixedprosthodontic treatments. Only short-term studies havebeen available, with a maximum of 3-year follow-up results.
These suggest that zirconia crowns are suitable for the fab-rication of single crowns. The 5-year clinical outcome of zir-conia crowns performed in a general dental practice wasinvestigated.
Methods.—The 162 patients received 205 zirconiacrowns between October 2004 and November 2005. Clinical

Table 4.—Life Table Analysis of Placed ZirconiaCrowns. 5-Year Cumulative Survival Rate (CSR) IsPresented
Period Examined crowns Lost Failed* CSR (%)
Crown cementation 216 0 0 1001 year 205 10 1 99.52 year 189 15 1 99.03 year 171 8 10 93.04 year 145 20 6 89.95 year 143 1 1 88.3Total 143 54 19 88.3
* A crown was considered a failure when it was remade due to irrepa-
rable complications: loose crown; veneer fracture, pain, abutment tooth
extraction.
(Courtesy of €Ortorp A, Kihl ML, Carlsson GE: A 5-year retrospective study
of survival of zirconia single crowns fitted in a private clinical setting. J
Dent 40:527-530, 2012.)
data were collected and used to determine the perfor-mance of the zirconia restorations and cumulative survivalrate (CSR).
Results.—Eighty-eight percent of the crowns had nocomplications over the 5-year follow-up. Forty crowns/abut-ment teeth (19%) experienced some type of complication,with the most common being extraction of abutment tooth(3%), root fracture (0.5%), endodontic and/or periodontalproblems (3%), porcelain veneer fracture (3%), loss ofretention (7%), and need for endodontic treatment (4%).Nine of the 15 crowns that lost retention could bere-cemented. Two of the loosened crowns were cemented
with zinc phosphate cement and 13 with Rely X Unicem;the rate of loosening was 12.5% and 6.6%, respectively, forthe two types of cement. Eliminating easily managed com-plications yielded a 9% failure rate, with 19 crowns consid-ered failures. Five-year CSR was 88.3% (Table 4).
Discussion.—These 5-year results show that zirconiacrowns offer promise as a prosthodontic alternative foruse in the premolar and molar regions. Nine percent ofthe restorations failed, however. Further studies are neededto assess long-term success.
Clinical Significance.—Porcelain veneeredzirconia single crowns demonstrated favorableclinical outcomes even when they were placedin posterior areas. However, interventionswere needed for 19% of the crowns/abutmentteeth, and the failure rate was somewhat high.
€Ortorp A, Kihl ML, Carlsson GE: A 5-year retrospective study of sur-vival of zirconia single crowns fitted in a private clinical setting. JDent 40:527-530, 2012
Reprints available from A €Ortorp, Dept of Prosthetic Dentistry/Dental Materials Science, Inst of Odontology, Box 450, SE-40530 G€oteborg, Sweden; fax: þ46 31 786 3193; e-mail:[email protected]
RadiologyPatient fears
Background.—Concerns about radiation and lack ofeducation about the benefits of radiographs may cause pa-tients to hesitate to agree to have the dental office do imag-ing studies. The dentist is the one who decides the patientneeds radiographs, but often the dental hygienist is the onewho broaches the topic of radiographs andmust handle thepatient’s concerns. The purposes of radiographs, the guide-lines used to determine when to take radiographs, and is-sues regarding the safety of radiographs were discussedto reinforce dental hygienists’ knowledge and allow themto provide reassurance.
Purposes of Radiographs.—It is important that the pa-tient understand that the dentist has recommended theradiographs and the dental hygienist and/or other dental
professional is carrying out the dentist’s prescription. Ra-diographs provide valuable information that cannot be ob-tained through visual examinations alone. Examples aredecay between the teeth and under restorations, cracks,periodontal disease, abscesses, cysts, infections, or devel-opmental anomalies. Radiographs also help in planningtreatment involving implants, orthodontic procedures,and dentures. Disease can be detected radiographically atearly stages, when the problem can bemanagedmore easilyand effectively. Radiographs contribute significantly toamore complete understanding of the patient’s oral health.
Guidelines.—The frequency of having dental radio-graphs depends on the patient’s present oral health, riskof caries, age and/or stage of growth and development,
Volume 58 � Issue 2 � 2013 95





























