-
Portorož, 8. in 9. april 2016
ZBORNIK REFERATOV
Univerza v LjubljaniVeterinarska fakulteta
XXIX. SIMPOZIJAo aktualnih boleznih malih `ivali
-
ZBORNIK REFERATOV
XXIX. SIMPOZIJA O AKTUALNIH
BOLEZNIH MALIH ŽIVALI
Portorož, 2016 http://www.zdruzenje-szvmz.si/
-
XXIX. SIMPOZIJ O AKTUALNIH BOLEZNIH MALIH ŽIVALI ZBORNIK
REFERATOV
Portorož, 8. in 9. april 2016
4
Izdalo: Slovensko združenje veterinarjev za male živali
Oblikovanje:AKTA DESIGNwww.aktadesign.si
270 izvodov
Vsebina
Findji L. Principles of oncologic surgery
........................................................................................
8
Findji L. Skin reconstruction in oncologic surgery
........................................................................
11
Nemec A. Tumorji in načela onkološke kirurgije v ustni votlini
.................................................... 15
Findji L. Canine and feline soft tissue sarcomas
..........................................................................
18
Findji L. Tumours of the body walls
............................................................................................
24
Nemec A. Defekti neba
..............................................................................................................
28
Krofič Žel M. Oskrba in klinično spremljanje pacienta s kronično
ledvično boleznijo ..................... 38
Kožuh T. Surova prehrana kot del terapije
..................................................................................
42
Tozon N. Kaj moramo vedeti o odkrivanju, zdravljenju in predvsem
preprečevanju nekaterih
parazitarnih obolenj
..................................................................................................................
44
Pogorevc E. Ultrazvočna diagnostika malih živali
........................................................................
46
Nemec A. Halo, veterina? Moj pes si je ravnokar zlomil zob
........................................................ 52
Plavec T. Pozdravljeni, rad bi govoril s kirurgom… Najpogostejša
vprašanja in (ne)enostavni
odgovori
...................................................................................................................................
55
Sist B. Perioperative pain management in dogs and cats
............................................................ 66
Tozon N, Lampreht Tratar U, Žnidar K, Serša G, Teissie J,
Čemažar M. Elektrokemoterapija –
operativni postopek
...................................................................................................................
67
Butinar J, Rejec A, Benoit J. Resekcije tumorjev v kombinaciji z
radioterapijo – multimodalni
pristop k zdravljenju onkoloških pacientov
.................................................................................
67
Plavec T, Rupp S, Kessler M. Zasuk širokega črevesja pri psih in
primerjava z zasuki želodca
in mezenterialnega korena
........................................................................................................
68
Zadravec M, Račnik J, Nemec A, Bahč I. Prehrana malih
rastlinojedih sesalcev z boleznimi zob .... 68
Kvapil P, Kastelic M, Gorenšek M. Zlom radiusa in ulne pri
zlatoličnem gibonu ............................ 69
Dolenšek T, Gombač M, Švara T. Patohistološka preiskava - kakšne
so koristi za veterinarja
praktika?
..................................................................................................................................
69
Hudobivnik A. Uporaba akupunkture za lajšanje bolečin pri
pacientu z lumbalno stenozo,
artritisom komolca ter boreliozo
................................................................................................
69
Kvapil P, Kastelic M, Zadravec M, Gombač M, Švara T, Golob M,
Račnik J. Kloacitis pri
bradatih agamah v živalskem vrtu Ljubljana
...............................................................................
70
Praprotnik Borko Š. Kirurška sanacija mastocitoma pri zlati
prinašalki ......................................... 70
Trojner G, Kessler M. Torzija pljučnega režnja pri ruskem hrtu
..................................................... 70
Zakošek Pipan M, O’Connor C. Neustrezen spolni razvoj –
trisomija X ........................................ 71
-
ZBORNIK REFERATOV XXIX. SIMPOZIJ O AKTUALNIH BOLEZNIH MALIH
ŽIVALI
Portorož, 8. in 9. april 2016
5
Generalni pokrovitelj
Iris mednarodna trgovina d.o.o. Cesta v Gorice 8, 1000
Ljubljana
in partnerji
Elanco
Natures Menu
Zoetis
Posebni pokrovitelji
Krka d.d., Šmarješka cesta 6, 8501 Novo mesto
Richter Pharma AG, Feldgasse 19, 4600 Wels, Austria
Vetconsult Pharma d.o.o., Grebičeva 50, 1000 Ljubljana
Vetpromet, Cesta na Brdo 100, 1000 Ljubljana
Simpozij so omogočili še
e MEDICA, d.o.o., Linhartova 8a, 8250 Brežice
EVG molekularna diagnostika d.o.o., Taborska ulica 8, 2000
Maribor
Farmina in DJ Plus d.o.o., Tovarniška c. 15, 3312 Prebold
Genera SI d.o.o., Parmova ulica 53, 1000 Ljubljana
IDEXX Laboratories Italia, Via Guglielmo Silva 36, 20149 Milano,
Italija
Kemofarmacija d.d., Cesta na Brdo 100, 1000 Ljubljana
Merck MSD AH, Intervet international B.V. Boxmeer, Podružnica
Ljubljana, Šmartinska cesta 140, 1000 Ljubljana
Metalka Media d.o.o., Dalmatinova 2, 1000 Ljubljana
MM Surgical d.o.o., Galjevica 81, 1000 Ljubljana
Royal Canin Ljubljana d.o.o., Letališka c. 29/A, 1000
Ljubljana
Vetpet d.o.o., Letališka cesta 29, 1000 Ljubljana
-
XXIX. SIMPOZIJ O AKTUALNIH BOLEZNIH MALIH ŽIVALI ZBORNIK
REFERATOV
Portorož, 8. in 9. april 2016
6
ORGANIZACIJSKI IN UREDNIŠKI ODBOR SZVMŽ (UO SZVMŽ)
Doc. dr. Alenka Seliškar, dr. vet. med. (predsednica)
Prof. dr. Nataša Tozon, dr. vet. med. (podpredsednica – bodoča
predsednica)
Igor Firm, dr. vet. med. (podpredsednik – prejšnji
predsednik)
Barbara Celinšek, dr. vet. med. (tajnik)
Tjaša Pukl, dr. vet. med. (blagajnik)
Milan Matko, dr. vet. med. (član)
Doc. dr. Joško Račnik, dr. vet. med. (član)
ČASTNI ČLANI ZDRUŽENJA:
Prof. dr. Vjekoslav Simčič, dr. vet. med.
Prof. dr. Boyd R Jones, BVSc, FACVSc, DECVIM-Ca, MRCVS
Emil Mlinarič, dr. vet. med.
WORLD SMALL ANIMAL VETERINARY ASSOCIATION - WSAVA
OFFICERS
Prof. Colin Burrows, Executive Board Member, President
Prof. Jolle Kirpensteijn, Past President
Dr. Walt Ingwersen, President Elect
Dr. Shane Ryan, Executive Board Member, Vice-President
Dr. Siraya Chunekamrai, Honorary Secretary
Dr. Ellen van Nierop, Honorary Treasurer
Dr. Renée Chalmers Hoynck van Papendrecht, Executive Board
Member
Dr. Nicola Neumann, Executive Board Member
FEDERATION OF EUROPEAN COMPANION ANIMAL VETERINARY ASSOCIATIONS
- FECAVA
OFFICERS
Dr. Jerzy Gawor, President
Dr. Wolfgang Dohne, Vice President
Dr. Ann Criel, Secretary
Dr. Denis Novak, Treasurer
Dr. Monique Megens, Senior Vice-President
-
ZBORNIK REFERATOV XXIX. SIMPOZIJ O AKTUALNIH BOLEZNIH MALIH
ŽIVALI
Portorož, 8. in 9. april 2016
7
ČETRTEK, 7. april 2016 PREDKONGRESNI DAN – Ortopedija, (dvorana
Adria) VOG-Veterinary Orthopaedics and Neurology Group(pokrovitelj
Vetpromet)08.30 – 09.00 PRIJAVA UDELEŽENCEVModerator: Matko M 09.00
– 09.30 Lončar Z. Orthopaedics exam of the hip and elbow09.30 –
10.00 Zorko B. Slikovna diagnostika patologije kolka10.00 – 10.30
Petazzoni M: Hip dysplasia: Early diagnosis and treatment
10.30 – 11.00 ODMORModerator: Zorko B11.00 – 11.45 Petazzoni M.
Hip dysplasia in growing dogs: Treatment decision making 11.45 –
12.30 Matko M. Artroskopska in slikovna diagnostika patologije
komolca 12.30 – 13.15 Petazzoni M. Elbow dysplasia: Early diagnosis
and treatment.
13.15 – 14.30 KOSILOModerator: Matko M14.30 – 15.15 Petazzoni M.
TTTT-Tibial Tuberosity Transposition Tool and Technique 15.15 –
17.00 Matko M, Zorko B. Case presentation section and hip and elbow
cross fire section
17.15 VOG meeting
ČETRTEK, 7. april 2016
PREDKONGRESNI DAN – Prostoživeče ptice v Sloveniji – od
biologije do veterinarske oskrbe, (dvorana Pharos)14.00 – 14.30
PRIJAVA UDELEŽENCEVModerator: Račnik J14.30 – 15.15 Vrezec A.
Vzroki pogina pri prostoživečih pticah in njihova biologija: vidik
muzejskih evidenc 15.15 – 16.00 Račnik J. Prva veterinarska pomoč
pri bolnih, oslabelih in poškodovanih prostoživečih pticah 16.00 –
16.45 Maričič P. Hranjenje in nega bolnih, oslabelih in
poškodovanih prostoživečih ptic
16.45 – 17.15 ODMOR Moderator: Zadravec M17.15 – 18.00 Zadravec
M. Trihomonoza pri prostoživečih pticah – klinične izkušnje18.00 –
18.45 Račnik J. Zadravec M. Nekateri klinični primeri bolezni in
poškodb pri prostoživečih pticah 18.45 – 19.30 Trilar T. Zakaj
ptice pojejo?
PETEK, 8. april 2016, Smaragdna dvorana08.30 – 09.00 PRIJAVA
UDELEŽENCEV09.00 – 09.15 OTVORITEV SIMPOZIJAModerator: Tozon N09.15
– 10.00 Findji L. Principles of oncologic surgery10.00 – 10.45
Findji L. Skin reconstruction in oncologic surgery
10.45 – 11.15 ODMOR (pokrovitelj VetConsult Pharma)Moderator:
Firm I11.15 – 12.45 Nemec A. Tumorji in načela onkološke kirurgije
v ustni votlini
12.45 – 14.15 KOSILOModerator: Matko M14.15 – 15.00 Findji L.
Canine and feline soft tissue sarcomas15.00 – 15.45 Findji L.
Tumours of the body walls
15.45 – 16.15 ODMOR (pokrovitelj Krka)Moderator: Seliškar A16.15
– 17.00 Nemec A. Defekti neba
17.00 – 18.30 SKUPŠČINA SZVMŽ20.00 SVEČANA VEČERJA (Smaragdna
dvorana, ansambel Victory)
SOBOTA, 9. april 2016
Program za VETERINARJE, Smaragdna dvoranaModerator: Firm I09.30
– 10.30 Sist B. Peri-operative pain management in dogs and cats
(VetConsult Pharma/Richter Pharma)10.30 – 11.00 Tozon N, Lampreht
Tratar U, Žnidar K, Serša G, Teissie J, Čemažar M.
Elektrokemoterapija – operativni postopek
11.00 – 11.30 ODMOR (pokrovitelji IRIS, ELANCO, Natures
Menu)Moderator: Matko M11.30 – 12.00 Butinar J, Rejec A, Benoit J.
Resekcije tumorjev v kombinaciji z radioterapijo – multimodalni
pristop k zdravljenju onkoloških pacientov12.00 – 12.30 Plavec T,
Rupp S, Kessler M. Zasuk širokega črevesja pri psih in primerjava z
zasuki želodca in mezenterialnega korena
12.30 – 14.00 KOSILOModerator: Račnik J14.00 – 14.30 Zadravec M,
Račnik J, Nemec A, Bahč I. Prehrana malih rastlinojedih sesalcev z
boleznimi zob14.30 – 15.00 Kvapil P, Kastelic M, Gorenšek M. Zlom
radiusa in ulne pri zlatoličnem gibonu (Nomascus Gabrillae)15.00 –
15.30 Dolenšek T, Gombač M, Švara T. Patohistološka preiskava -
kakšne so koristi za veterinarja praktika?15.30 ZAKLJUČEK
SIMPOZIJA
SOBOTA, 9. april 2016
Program za VETERINARSKE TEHNIKE, (dvorana Adria)Moderator: Matko
M09.30 – 10.15 Krofič Žel M. Oskrba in klinično spremljanje
pacienta s kronično ledvično boleznijo10.15 – 11.00 Kožuh T. Surova
prehrana kot del terapije (Natures Menu/IRIS)11.00 – 11.30 ODMOR
(pokrovitelji IRIS, ELANCO, Natures Menu)Moderator: Račnik J11.30 –
12.15 Tozon N. Kaj moramo vedeti o odkrivanju, zdravljenju in
predvsem preprečevanju nekaterih parazitarnih obolenj
(ELANCO/IRIS)12.15 – 13.00 Pogorevc E. Ultrazvočna diagnostika
malih živali
13.00 – 14.00 KOSILOModerator: Firm I14.00 – 14.45 Nemec A.
Halo, veterina? Moj pes si je ravnokar zlomil zob ...14.45 – 15.30
Plavec T. Pozdravljeni, rad bi govoril s kirurgom… Najpogostejša
vprašanja in (ne)enostavni odgovori
15.30 ZAKLJUČEK SIMPOZIJA
POSTERJI
1. Hudobivnik A. Uporaba akupunkture za lajšanje bolečin pri
pacientu z lumbalno stenozo, artritisom komolca ter boreliozo
2. Kvapil P, Kastelic M, Zadravec M, Gombač M, Švara T, Golob M,
Račnik J. Kloacitis pri bradatih agamah v živalskem vrtu
Ljubljana
3. Praprotnik Borko Š. Kirurška sanacija mastocitoma pri zlati
prinašalki
4. Trojner G, Kessler M. Torzija pljučnega režnja pri ruskem
hrtu
5. Zakošek Pipan M, O’Connor C. Neustrezen spolni razvoj –
trisomija X
PROGRAM XXIX. SIMPOZIJA O AKTUALNIH BOLEZNIH MALIH ŽIVALI,
Portorož, 7. – 9. april 2016
-
XXIX. SIMPOZIJ O AKTUALNIH BOLEZNIH MALIH ŽIVALI ZBORNIK
REFERATOV
Portorož, 8. in 9. april 2016
8
PRINCIPLES OF ONCOLOGIC SURGERY
Laurent Findji
Surgery has been and remains the mainstay of tumour treatment,
except for cancers which are exclusively sys-temic (e.g.
leukaemia), and most cancer cures in humans today still result from
surgery alone.
Historically, surgeons were first limited in the extension of
surgical excisions by their own technical insufficiencies and
shortcomings of supporting disciplines such as anaes-thesia and
intensive care medicine. As these progressed came the era of large
resections. Initially, it appeared that wider resections improved
the prognosis. However, this was only true to a certain point and,
although local dis-ease control was more often achieved, metastatic
disease remained an obstacle to cure. Surgery as sole treatment of
cancer was obviously not the panacea.
The most efficient treatment of cancer is today multi-modal. It
is now clear that surgeons should be members of a team including
radiographers, anaesthetists, criticalists, pathologists, and
medical and radiation oncologists. Sur-geons need to have a good
knowledge of tumour biology to determine the role and contribution
of surgery, for each case, to the whole treatment. They also need
to under-stand how other therapies work, in order to adapt their
surgical technique to previous or later treatments.
These are exciting perspectives for oncologic surgeons. Their
role is constantly evolving as they increasingly work in close
collaboration with other therapies such as chemo-therapy,
radiotherapy and immunotherapy. Whilst the times of extensive,
technically challenging resections are not over, the oncologic
surgeon has evolved from a techni-cian to a more complete
clinician, whose deep knowledge in cancer biology allows more
concerted and tailored pro-cedures.
TYPES OF ONCOLOGIC SURGERY
Surgery for diagnosisBiopsies
Biopsies are crucial in the diagnosis process of tumours. They
can be incisional or excisional. They are performed
transcutaneously (core-needle biopsies), or by minimally-invasive
or conventional surgery.
Staging surgerySurgery can be involved in tumour staging.
Lymph
node biopsies (incisional or excisional) provide helpful
information on locoregional spreading of a tumour. Ex-ploration of
body cavities for signs of metastatic disease can also be
performed, either when operating the main tumour (e.g. inspection
of the abdomen when resecting an abdominal tumour) or separately.
Minimally-invasive surgery (laparoscopy, thoracoscopy) is
increasingly used in such indications.
Surgery for cureSurgery is most often performed with an
intention to
cure, whether it be by surgery alone or combined with other
therapies. Depending on the surgical “dosing”, sev-eral types of
tumour resections are possible: cytoreductive or intracapsular,
marginal, wide and radical.
Cytoreductive surgery consists of removing as much of the tumour
as possible but leaving macroscopic disease behind. It is only
considerable if some kind of adjuvant therapy is planned, in a view
of potentiating this adjuvant treatment.
Marginal resections consist of excision of the tumour with
minimal amounts of surrounding tissues. The likeli-hood of leaving
microscopic residual disease is high and this type of resection
should be avoided as much as pos-sible. However, in certain cases,
it is preferable to more ex-tensive resections, either because of
difficulties in wound reconstruction (e.g. tumours of extremities)
or vicinity of non-expandable structures (e.g. brain tumours). In
such cases, surgery should be followed by adjuvant therapy,
ra-diotherapy especially.
Wide resections consist of excision of the tumour with enough
surrounding tissues to expect complete excision including
microscopic disease. This is the type of resection to seek as often
as possible. Its main limitation comes from the fact that precise
guidelines as to necessary margins are lacking. Therefore, in some
cases, microscopic disease
Laurent Findji DMV MS MRCVS DiplECVS Fitzpatrick Referrals
Guildford GU7 2AJ, United Kingdom
-
ZBORNIK REFERATOV XXIX. SIMPOZIJ O AKTUALNIH BOLEZNIH MALIH
ŽIVALI
Portorož, 8. in 9. april 2016
9
remains, leading to recurrence. Good communication with the
pathologist is essential to have as precise an assess-ment of the
excision margins as possible.
Radical resections consist in even wider resections. Of-ten, it
consists of the excision of body parts (amputations). A good
definition is that after radical excision, there is no need to
await the pathology results to know that the mar-gins are
clear.
Surgery for palliationPalliative surgery is performed to improve
the patient’s
quality of life, without extending its life expectancy.
Am-putation for an appendicular osteosarcoma and splenec-tomy on a
haemangiosarcoma are two examples of pallia-tive surgeries, as they
do not improve survival times per se.
Surgery for cancer preventionSome cancers, such as
hormone-dependant cancers,
can be prevented by surgical procedures: prepubertal
ova-riectomy in dogs dramatically reduces the risk of mam-mary
tumour; castration of dogs prevents the occurrence of testicular
tumours and perianal adenomas; etc.
Surgery for medical supportPlacement of feeding tubes can be
necessary to sup-
port nutrition of cancer patients. Cachexia is a major con-cern
in some cancer patients. Nutritional support is known to decrease
associated morbidity in humans.
Surgery for treatment device implantationSurgeons can play a
part in non-surgical treatments by
placing several types of implants such as vascular access ports,
intracavitary catheters, brachytherapy catheters, etc.
ONCOLOGIC SURGERY TECHNIQUES
BiopsiesBiopsies can be incisional or excisional. Incisional
biop-
sies consist of sampling a portion of the tumour to allow
histopathological determination of its nature. Excisional biopsies
consist of the complete excision of the tumour prior to any
histopathological diagnosis.
Excisional biopsies should only be chosen when knowl-edge of the
tumour type would not alter the surgical dose required for
resection. Excessive and inappropriate use of marginal excisional
biopsies is a major cause for cancer treatment failure. If in
doubt, perform fine-needle aspi-rates or an incisional biopsy to
ascertain that the subse-quent resection plan is appropriate.
In general, it is best to biopsy at the junction between healthy
and tumoral tissues, so that the pathologist can study the
characteristics of the tumour invasion in sur-rounding tissues.
Also, many tumours are necrotic, in-flammatory or infected in their
centre, which may lead to misdiagnosis. However, some tumours, such
as osteosar-coma, should be biopsied in their centre as they induce
a strong reaction within surrounding tissues, which may lead to
misdiagnosis if biopsied in periphery1. In addition, if the
surrounding tissues are essential for later reconstruc-
tion, they should not be included in the biopsy. Overall, it is
crucial not to jeopardise later treatments by performing biopsies
in a way that the biopsy tract can be later excised en-bloc with
the tumour.
Fine-needle aspiration and cytological examination of the
regional lymph nodes should be performed, regardless of their
palpation and size, as they are not reliable indica-tors of lymph
node metastasis. However, tumours do not necessarily drain to the
closest lymph node and may even drain controlaterally. Therefore,
ideally, individual map-ping of the tumour drainage should be
obtained to deter-mine the position of the sentinel lymph nodes,
which are the first to which the tumour drains and whose aspiration
therefore is the most sensitive for detection of metasta-sis2. This
is increasingly performed in oncology specialist centres and should
become more common in the future. In the absence of sentinel lymph
node mapping, it can only be recommended to sample as many regional
lymph nodes as possible, as long as their biopsy does not increase
surgical time and risk excessively.
Tumour resectionThe most important point, when planning
surgery
for tumour resection, is to balance the consequences of surgery
and potential complications against the expect-ed benefits. In
other words, the treatment should never be worse than the disease!
It is easy for surgeons to be tempted to perform technically
challenging procedures, which turn out to be of no significant
benefit for the patient. Inversely, surgeons should not deter
owners to proceed with some apparently extensive, but well
toler-ated, surgeries (amputations, extensive mandibulectomies /
maxillectomies, etc.) because they personally feel uncom-fortable
with them. Referral should then be offered.
It is crucial that surgeons place the patient’s welfare first,
before owners’ wishes. In-depth discussion with the owners will
allow understanding what their expectations are and whether they
can be met by possible treatments. This will avoid
misunderstandings and later issues.
Knowledge of the tumour type and biology is para-mount in
appropriate surgical planning. The surgical “dose” depends on it.
The first surgery is the best chance to cure, it should not be
wasted.
As often as possible, tumours should be resected widely. Fear of
not being able to close the resulting de-fect should not limit the
resection extension. Depending on the tumour type and size, 1 to
3-cm lateral margins are generally recommended. Some surgeons
advocate for even wider (5-cm) lateral margins for excision of soft
tissue sarcomas in cats3. In depth, depending on tumour type and
size, one or two fascial planes should be excised en-bloc with the
tumour.
Alternatively, if an adjuvant treatment is planned
(ra-diotherapy especially), the surgical excision can be more
conservative. Taking intraoperative pictures and leaving metallic
vascular clips at the margins of excision can then help the
radiation oncologist plan subsequent treatments.
-
XXIX. SIMPOZIJ O AKTUALNIH BOLEZNIH MALIH ŽIVALI ZBORNIK
REFERATOV
Portorož, 8. in 9. april 2016
10
Tumours should be manipulated as little and as gently as
possible to prevent seeding of tumour cells. Ideally, the tumour
should not be approached or visualised and only healthy surrounding
tissues be manipulated. Previous bi-opsy and drain tracts are
excised en-bloc with the tumour. Whenever possible, major
arteriovenous pedicles should be ligated as early as possible in
the procedure and veins be ligated before arteries to limit the
risk of macroscopic embolisation of tumour cells when the tumour is
manipu-lated.
Tumour should be treated as an infection: any tissues,
instruments, gloves and drapes which may have been contaminated by
tumour cells should be changed. The same instruments should not be
used to excise, or biopsy, two separate masses. Similarly, when
closing the surgical wound, it is important to remember that any
distant tis-sues used (skin flaps for instance) will be considered
con-taminated if any subsequent treatment is required. Using large
skin flaps after tumour excision should be avoided if the tumour
margins are not known to be clear. It could lead to tumour seeding
and recurrence away from the initial site and prevent adjuvant
radiotherapy as the irra-diation field would become too large. An
option allowing skin flaps to be used in the face of uncertain
margins is to harvest the flap before starting the tumour
resection. I regularly use this approach, which requires careful
surgical planning.
Postoperative care should be anticipated. Enteral feeding tubes
should be placed as appropriate. Similarly, wound catheters can be
left in surgical wounds, allowing regular instillation of local
anaesthetics in the wound.
Even if the tumour has previously been biopsied, the entire
piece of excision is fixed in 10% formalin and sub-mitted for
pathology.
POSTOPERATIVE CARE
Non-specifically, postoperative care of cancer patients include
wound care, analgesia, nutritional support, and medical care as
appropriate. Depending on the tumour type, specific treatments of
paraneoplastic treatments can be required (e.g. blood levels
monitoring and manage-ment of calcium in patients with
hyperparathyroidism or of glucose in patients with insulinomas,
etc.). Depending on the procedure performed, specific management
may be required (chest drain for thoracic tumours, nursing on
animals with spinal tumours, rehabilitation for amputees,
etc.).
When adjuvant therapies are planned, they are initi-ated as soon
as possible. Usually, chemotherapy can be started early, most often
7 to 10 days after surgery. Al-though most chemotherapeutic agents
experimentally im-pair wound healing, it is of little, if any,
clinical relevance. On the other hand, radiotherapy has a clear
detrimental effect on wound healing and it is most often only
initiated after wound healing is complete, i.e. 2 to 3 weeks after
surgery.
References
1. Ehrhart NP, Culp WTN. Principles of oncologic surgery. In:
Kudnig ST, Séguin B (eds): Veterinary surgical oncology. Oxford:
Wiley-Blackwell, 2012;3-13.
2. Tuohy JL, Milgram J, Worley DR, Dernell WS. A review of
sentinel lymph node evaluation and the need for its incorporation
into veterinary oncology. Veterinary and Comparative Oncology.
2009;7: 81-91.
3. Phelps HA, Kuntz CA, Milner RJ, Powers BE, Bacon NJ. Radical
excision with five-centimeter margins for treatment of feline
injection-site sarcomas: 91 cases (1998-2002). Journal of the
American Veterinary Medical Association. 2011;239: 97-106.
-
ZBORNIK REFERATOV XXIX. SIMPOZIJ O AKTUALNIH BOLEZNIH MALIH
ŽIVALI
Portorož, 8. in 9. april 2016
11
SKIN RECONSTRUCTION IN ONCOLOGIC SURGERY
Laurent Findji
It is essential for oncologic surgeons to have a deep knowledge
of reconstruction techniques. Indeed, limita-tions in the ability
to reconstruct a wound should not lead to insufficiently wide
resections. The greater the recon-struction abilities of the
surgeon, the more comfortable they will be administering the
appropriate dose of surgery in the face of a large or awkwardly
located tumour.
Reconstructive surgery is an extensive subset of sur-gical
science. It is presented exhaustively in a number of textbooks1-3.
Only basic notions and particular points per-taining to oncologic
surgery can be discussed here.
Vascular anatomy of the skin
In dogs and cats, the skin is vascularised by 3 plexi: the
subpapillary, cutaneous and subdermal plexi. The two most
superficial plexuses depend on the subdermal plexus, which is
therefore the most important to preserve. This subdermal plexus
lies in depth of the hypodermis. In re-gions of the body where a
panniculus muscle is present (trunk, neck), the subdermal plexus
runs immediately deeply and superficially to it. As a practical
consequence, when the skin is undermined for primary closure or
perfor-mance of a skin flap, it must be elevated in depth of the
panniculus muscle. In areas where no such muscle is pre-sent, the
skin must be elevated as close as possible from the underlying
fascial or muscular plane.
Wound closure options
Simple closureWound closure may be primary (immediate),
delayed
primary (before formation of granulation tissue) or sec-ondary
(after formation of granulation tissue). Delayed pri-mary and
secondary closures are recommended by some surgeons when margin
status is uncertain after tumour removal4: the wound is managed as
an open wound for a few days while pathology results and margin
assessment are pending. When the margins are known to be free of
tumour, the wound is closed surgically using any available
technique (simple closure, skin flap, skin graft). Several
techniques (tension-relieving sutures and incisions, plas-ties) are
available to achieve wound closure when simple closure is not
possible. Alternatively, the wound may be left to heal by second
intention.
Laurent Findji DMV MS MRCVS DiplECVS Fitzpatrick Referrals
Guildford GU7 2AJ, United Kingdom
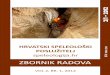
Figure : Vascular anatomy of the skin
(a: epidermis; b: dermis; c: panniculus muscle; d: squelettal
muscle; 1: subpapillary plexus; 2: cutaneous plexus; 3: subdermal
plexus; 4: hypodermis; arrow: direct cutaneous artery)
-
XXIX. SIMPOZIJ O AKTUALNIH BOLEZNIH MALIH ŽIVALI ZBORNIK
REFERATOV
Portorož, 8. in 9. april 2016
12
Skin flaps
Skin flaps are either subdermal (relying on the subder-mal
vascular plexus) or axial (relying on a direct cutaneous
artery).
Subdermal flaps are sometimes referred to as “ran-dom” flaps, as
they rely on the random subdermal plexus to vascularise the
elevated skin. This means that these flaps can be harvested in any
location and direction. How-ever, the perfusion pressure of the
elevated skin has to be estimated as an empirical statistical
notion, as the po-tential presence and direction of direct
cutaneous arteries supplying the elevated skin are unknown (Figure
2). As a consequence, these flaps can only be elevated on a limited
length, and their base need to be at least as wide as their free
end. As an empirical rule, subdermal flaps should only be 1.5 to 2
times longer than they are wide.
Figure 2: Vascularisation subdermal flaps
Subdermal flaps can either be local or distant.
Local flaps include advancement (Figure 3), rotation (Figure 4),
transposition (Figure 5) and interpolation flaps (Figure 6). These
flaps are elevated from skin adjacent to the wound.
Figure 3: Advancement flap
Figure 4: Rotation flap
Figure 5: Transposition flap
Figure 6: Interpolation flap
-
ZBORNIK REFERATOV XXIX. SIMPOZIJ O AKTUALNIH BOLEZNIH MALIH
ŽIVALI
Portorož, 8. in 9. april 2016
13
Distant flaps include hinge and pouch flaps, in which a
monopedicular or bipedicular subdermal flap is elevated on the
lateral aspect of the abdomen or thorax and used to cover a wound
on the distal portion of a limb brought to the flap (Figure 7).
Figure 7: Principle of distant flaps
Axial pattern flaps are determined by the area of skin
vascularised by a major direct cutaneous artery (angio-some), after
which it is named (Figure 8a). Many direct cutaneous arteries which
can be used to perform axial flaps have been described (Figure 9).
Provided this artery is preserved, such flaps are more robust and
survive on greater lengths compared to equivalent subdermal flaps.
They can even be islanded, i.e. entirely cut out from the donor
site apart from their vascular pedicle (Figure 8b). However, axial
flaps cannot be elevated in any direction: their design has to
follow the description of the cutaneous area vascularised by the
chosen direct cutaneous artery. The most commonly used axial flaps
include the caudal superficial epigastric, thoracodorsal,
omocervical, deep cir-cumflex iliac and caudal auricular flaps.
Figure 8: Vascularisation of axial flaps (a). Island flap
(b)
Figure 9: Main direct cutaneous arteries of the dog
Skin flaps, either subdermal or axial, are transposed with their
own vascularisation and can survive on poorly vascular beds or over
cavities.
Skin grafts
Skin grafts consist of transposing free portions of
par-tial-thickness or full-thickness skin to a wound. The
trans-posed skin is therefore no longer perfused and relies on the
development of a neovascularisation from the receiv-ing bed for
survival. The receiving bed must therefore be healthy and
well-vascularised, so that sufficient neovascu-larisation can
develop from it.
In veterinary surgery full-thickness grafts, harvested from the
ventrolateral portions of the trunk, are most commonly used.
Different forms of grafts exist: meshed, unmeshed, pinch, punch and
strip grafts.
Meshed and unmeshed grafts use a single skin por-tion to cover
the recipient bed. Numerous slit incisions are made in meshed
grafts. These incisions allow postopera-tive drainage which favours
graft adhesion and survival. In addition, meshed grafts can be
expanded more easily than unmeshed grafts.
Pinch and punch grafts consist of a number of
few-millimetre-wide portions of skin placed evenly apart in the
recipient bed. Pinch grafts are harvested with a scalpel, whereas
punch grafts are harvested with a biopsy punch. Matching-size holes
or pockets are created in the granula-tion tissue of the recipient
bed to accommodate the grafts. The main advantages of these grafts
are that they are easy to perform, allow very good drainage of the
wound and withstand infection better than other types of graft.
How-ever, the resulting cosmetic aspect is rather poor.
Strip grafts consist of several strips of skin placed par-allel
in the recipient bed. Matching-size strips of granula-tion tissue
are excised to accommodate the grafts. Like pinch and punch grafts,
these grafts allow good drainage but often lead to poor cosmetic
results.
Wound closure decision making
Wound closure options depend on the location, age, type,
severity and contamination of the wound. In small
a
b
-
XXIX. SIMPOZIJ O AKTUALNIH BOLEZNIH MALIH ŽIVALI ZBORNIK
REFERATOV
Portorož, 8. in 9. april 2016
14
animals, the great skin elasticity allows primary or second-ary
closure of many wounds. If not, the wound can either be left to
heal by second intention or more advanced re-constructive
techniques be used to achieve wound closure. Second intention
healing may seem financially attractive at first, but it is often
long to complete, requires numer-ous dressing/bandages and regular
follow-up, which may eventually cost more than a reconstructive
surgery. In ad-dition, it often leaves an epithelium of poor
quality and cosmetics, and occasionally results in skin
contractures.
Skin flaps and grafts can be used to avoid these draw-backs.
In all cases, the surgeon must opt for the technique which, in
his hands, is the safest, simplest and cheapest. The technique with
the greatest chances of success must be chosen in priority. If
several techniques have equal chances of success, the simplest must
be preferred. Lastly, the financial aspect may also be accounted
for and the cheapest method among the most likely to be successful
may also be chosen.
References
1. Pavletic MM. Atlas of small animal wound management and
reconstructive surgery. Oxford: Wiley-Blackwell, 2010.
2. Williams J, Moores A. BSAVA manual of canine and feline wound
management and reconstruction. Quedgeley: British Small Animal
Veterinary Association, 2009.
3. Slatter DH. Textbook of small animal surgery. Philadelphia,
PA ; [Great Britain]: Saunders, 2003.
4. Liptak J. The Principles of Surgical Oncology: Surgery and
Multimodality Therapy. Compendium Continuing Education for
Veterinarians. 2009;31: 14 p.
-
ZBORNIK REFERATOV XXIX. SIMPOZIJ O AKTUALNIH BOLEZNIH MALIH
ŽIVALI
Portorož, 8. in 9. april 2016
15
NOVOTVORBE V USTNI VOTLINI IN NAČELA ONKOLOŠKE KIRURGIJE V USTNI
VOTLINI
Ana Nemec
Klasifikacija novotvorb v ustni votlini
Ustna votlina je peto najpogostejše mesto za pojav novotvorb pri
psih in tretje najpogostejše pri mačkah, pri čemer maligne
novotvorbe ustne votline predstavljajo 6% vseh novotvorb. Glede na
biološko vedenje novotvorbe ustne votline opišemo kot maligne ali
benigne novotvorbe. Histološko pa novotvorbe ustne votline lahko
razvrstimo med neodontogene ali odontogene novotvorbe ter
ne-neoplastične proliferativne spremembe.
Neodontogene novotvorbeNajpogostejše neodontogene novotvorbe
ustne votline
psov in mačk so ploščatocelični karcinom (SCC), maligni melanom
(MM), fibrosarkom (FSA) in osteosarkom (OSA). Prav tako pa v ustni
votlini lahko diagnosticiramo multilob-ularni osteohondrosarkom,
ekstramedularni plazmocitom, limfom, mastocitom, hemangiosarkom,
fibrom, osteom in druge redke neodontogene novotvorbe.
Ploščatocelični karcinom je najpogostejša novo-tvorba ustne
votline pri mačkah in druga najpogostejša pri psih. Je invazivna
epitelijska novotvorba, ki pogosto vrašča v kost. Večinoma izvira
iz zobnega dela čeljusti in zaseva pozno in sorazmerno redko.
Tonzilarni SCC in SCC pri mačkah zasevata prej (regionalne bezgavke
in pljuča) in pogosteje. Prognoza je odlična pri psih ob zgodnji
diag-nozi in radikalnem zdravljenju. Prognoza za SCC jezika in
tonzil ter za SCC pri mačkah je slaba.
Maligni melanom je najpogostejša novotvorba ustne votline pri
psih in redka pri mačkah. Histološka diagnos-tika je lahko
zapletena zaradi različnih tipov MM. Maligni melanom pogosto vrašča
v kost in pogosto ter zgodaj za-seva (regionalne bezgavke, pljuča).
Prognoza je najslabša za MM ustne votline, nekoliko boljša je za
ustnični MM (in najboljša za MM kože).
Fibrosarkom je druga najpogostejša novotvorba ustne votline pri
mačkah in tretja pri psih. Pri psih (zlasti zlati prinašalci) je
opisan tudi t.i. »high-low« podtip FSA, ka-terega histološke
značilnosti so tiste benignih novotvorb, vendar je biološko izjemno
agresiven. Fibrosarkom najpo-gosteje najdemo na dlesni zgornje
čeljusti in trdem nebu in je lokalno zelo invaziven, čeprav
sorazmerno redko zaseva. Prognoza je zaradi pogosto neuspešne
lokalne kontrole bolezni sorazmerno slaba, vendar je odvisna od
lokacije novotvorbe (prognoza je najslabša za novotvorbe neba),
velikosti, načina zdravljenja in histološkega gradusa.
Osteosarkom je lokalno izjemno invazivna novotvor-ba, ki
sorazmerno redko zaseva. Prognoza je sorazmerno slaba zaradi
pogoste lokalne ponovitve in napredovanja bolezni. Multilobularni
osteohondrosarkom je novotvorba ploščatih kosti glave.
Odontogene novotvorbeOdontogene novotvorbe so pogoste pri psih
in redke
pri mačkah. Glede na tkivni izvor jih delimo na epitelijske,
mezenhimske in mešane. Odontogene novotvorbe so po-navadi lokalno
agresivne, vendar ne zasevajo. Maligne od-ontogene novotvorbe so
izjemno redke, zato je prognoza za odontogene novotvorbe
najpogostejše odlična.
Pasji akantomatozni ameloblastom (CAA; »akan-tomatozni epulis« -
v opuščanju) je lokalno invazivna epitelijska novotvorba z odlično
prognozo ob popolni re-sekciji.
Periferni odontogeni fibrom (POF; »fibromatozni, osificirajoči
epulis« - v opuščanju) je lokalno invazivna mezenhimska novotvorba
z odlično prognozo ob popolni resekciji.
Odontom je induktivna mešana novotvorba, ki bi lahko bila tudi
hamartom. Diagnosticiramo jo večinoma pri mladih živalih. Prognoza
je ob popolni neinvazivni odstran-itvi odlična.
Ne-neoplastične proliferativne spremembeV ustni votlini lahko
diagnosticiramo številne ne-
neoplastične proliferativne spremembe, kot so fokalna ali
generalizirana hiperplazija dlesni, preraščanje dlesni, pio-geni
granulom, periferni granulom velikih celic, reaktivna eksostoza,
travmatska hiperplazija sluznice, papilomatoza in eozinofilni
granulom, plak ali ulkus.
Doc. dr. Ana Nemec, dr. vet. med., spec. med. psov in mačk,
Dipl. AVDC, Dipl. EVDC Klinika za male živali, Veterinarska
fakulteta, Univerza v Ljubljani, Slovenija; Department of Surgical
and Radiological Sciences, School of Veterinary Medicine,
University of California-Davis, USA; e-pošta:
[email protected]; www.kkmz.si
-
XXIX. SIMPOZIJ O AKTUALNIH BOLEZNIH MALIH ŽIVALI ZBORNIK
REFERATOV
Portorož, 8. in 9. april 2016
16
Diagnostični postopki
Najpomembnejša napovedna dejavnika pri živalih z no-votvorbo v
ustni votlini sta vrsta novotvorbe in zamejitev bolezni. Pri
določanju zamejitve bolezni se poslužujemo TNM sistema, pri čemer s
»T« opišemo primarni tumor, z »N« vpletenost regionalnih bezgavk in
z »M« morebitne oddaljene zasevke. Da lahko določimo TNM, moramo
opraviti popoln klinični pregled ter ustrezno laboratorijsko in
slikovno diagnostiko.
Primarna novotvorbaDa določimo vrsto novotvorbe, moramo opraviti
biop-
sijo. Biopsijo v idealnih razmerah opravimo po opravljeni
slikovni diagnostiki, saj tako najbolje načrtujemo odvzem dobrega
vzorca tkiva in se obenem izognemo morebitnim pomembnim strukutram
v okolici. Večinoma opravljamo incizijsko biopsijo po odprti
metodi, pri čemer (če velikost novotvorbe dopušča) odvzamemo vsaj 2
vzorca iz globine več kot 2 mm, pri tem pa se izogibamo mestom
nekroze in ulceracije. Mesto biopsije in pot inštrumenta morata
biti kasneje vključena v polje resekcije (ali obsevanja). Zelo
pomembno je, da primer opišemo patohistologu in se z njim tudi
temeljito pogovorimo ob kakršnemkoli dvomu ter upoštevamo načela
klinično-patološke korelacije.
Velikost novotvorbe je izjemnega pomena pri načrtovanju
zdravljenja in predvidevanju poteka bolezni. Obseg novotvorbe,
zlasti pri velikih novotvorbah in novo-tvorbah kavdalno v ustni
votlini in/ali na zgornji čeljusti, določimo najbolje z
računalniško tomografijo (CT) glave, pri čemer naredimo 1-mm rezine
pred in po aplikaciji kon-trastne snovi, v polje pa vključimo tudi
vse regionalne bez-gavke.
Regionalne bezgavkePalpacija bezgavk je nezanesljiva, saj tudi
na otip nor-
malne bezgavke lahko vsebujejo zasevke, obenem pa večine
regionalnih bezgavk glave ne tipamo. Tankoigel-na biopsija bezgavk
je trenutno najbolj uveljavljena me-toda pregleda. Rutinsko
opravljamo tankoigelno biopsijo enostavno dostopnih čeljustnih
bezgavk. Vedno odvzam-emo vzorce iz bezgavk na obeh straneh, ne
glede na lokacijo novotvorbe v ustni votlini, saj je potek
dreniranja limfe iz ustne votline nepredvidljiv. Še bolje je, če CT
izvid bezgavk po potrebi kombiniramo z ultrazvočno vodeno
tankoigelno biopsijo retrofaringealnih bezgavk, ki so glav-ni
zbirni center limfe glave. Negativen izvid tankoigelne biopsije
bezgavk pa tudi ne pomeni zanesljivo odsotnosti zasevkov.
Ekscizijska biopsija vseh bezgavk glave in vratu je kontroverzen
poseg, saj sam po sebi predstavlja obsežen kirurški poseg. Vedno
bolj se stremi k ekscizijski biopsiji bezgavk, ki prve drenirajo
območje novotvorbe (ang. sen-tinel node), pri čemer pa obstajajo v
veterini še vedno precejšnji diagnostični izzivi.
Oddaljeni zasevkiZamejitev bolezni po TNM klasifikaciji
zaokrožimo z
ultrazvočno preiskavo trebuha ter rentgenskim slikanjem ali, še
bolje, CT prsnega koša. Z rentgenskim slikanjem (v treh
projekcijah) zaznamo zgolj 9% pljučnih nodulov, ki jih sicer
diagnosticiramo s CT pri psih z zasevki v pljučih.
Zdravljenje in prognoza
Metode zdravljenja novotvorb ustne votline so številne (npr.
kirurško zdravljenje, obsevanje, elektrokemo-/ele-ktrogenska
terapija, kemoterapija, imunoterapija), zato je najbolje, da ekipa
specialistov (ki jo v idealnih razme-rah sestavljajo veterinarski
stomatolog, kirurg, onkolog, radiacijski onkolog, internist,
anesteziolog in specialist slikovne diagnostike) pripravi načrt
zdravljenja za vsakega posameznega pacienta glede na vrsto
novotvorbe, zame-jitev bolezni, morebitne ostale bolezni in starost
pacienta ter želje in finančne zmogljivosti lastnika. Veterinar
mora lastnika živali obvestiti o poteku zdravljenja, prognozi,
morebitnih neželenih učinkih zdravljenja, pooperacijskem okrevanju
in izgledu živali ter stroških zdravljenja, pred pričetkom
zdravljenja.
Kirurško zdravljenje je trenutno najpogostejša me-toda
zdravljenja, ki pa ima glede na vrsto in velikost tu-morja ter
morebitno prisotnost zasevkov lahko različen cilj – ozdravitev
pacienta (npr. večina majhnih/zgodaj od-kritih neodontogenih in
zlasti odontogenih novotvorb), zmanjšanje tumorske mase (npr.
neoperabilne novotvorbe pred obsevanjem), lokalno kontrolo bolezni
(npr. opera-bilni melanom), paliativno zdravljenje (npr. velike
novo-tvorbe, ki motijo normalno hranjenje živali). Cilj si lahko
pravilno zastavimo le po opravljeni natančni diagnostiki in na
podlagi tega načrtujemo kirurško ekscizijo, ki je lahko
intrakapsularna (ostanejo ostanki tumorskega tkiva - npr. pri cilju
paliativnega zdravljenja ali zmanjšanja tumorske mase), marginalna
(vključuje psevdokapsulo tumorja, lahko ostanejo tumorske celice –
npr. zdravljenje dobro diferenciranih benignih tumorjev), široka
(vključuje tumor, psevdokapsulo, reaktivno cono in ponavadi 1 – 2
cm vid-no zdravega tkiva, odvisno od vrste tumorja – npr. delna
maksilektomija z namenom ozdravitve SCC) ali radikalna (odstranitev
celotne anatomske strukture ali kompart-menta s tumorjem). Kirurške
tehnike in z njimi povezane spremembe videza in funkcije živali so
različne in bodo predstavljene na podlagi kliničnih primerov
Literatura
Amory JT, Reetz JA, Sánchez MD, et al. Computed tomographic
characteristics of odontogenic neoplasms in dogs. Vet Radiol
Ultrasound 2014; 55(2): 147-158.
Armbrust LJ, Biller DS, Bamford A, et al. Comparison of
three-view thoracic radiography and computed tomography for
detection of pulmonary nodules in dogs with neoplasia. J Am Vet Med
Assoc 2012; 240: 1088-1094.
Arzi B, Verstraete FJM. Clinical staging and biopsy of
maxillofacial tumors. In: Verstraete FJM, Lommer M, eds. Oral and
maxillofacial surgery in dogs and cats. Edinburgh: Saunders
Elsevier, 2012: 373-380.
Barnes L, Eveson JW, Reichart P, et al. World Health
Organization Classification of Tumours. Pathology and Genetics of
Head and Neck Tumours. Lyon: IARC Press, 2005.
Bonello D, Roy CG, Verstraete FJM. Non-neoplastic proliferative
oral lesions. In: Verstraete FJM, Lommer M, eds. Oral and
maxillofacial surgery in dogs and cats. Edinburgh: Saunders
Elsevier, 2012: 411-421.
-
ZBORNIK REFERATOV XXIX. SIMPOZIJ O AKTUALNIH BOLEZNIH MALIH
ŽIVALI
Portorož, 8. in 9. april 2016
17
Boston SE, Lu X, Culp WT, et al. Efficacy of systemic adjuvant
therapies administered to dogs after excision of oral malignant
melanomas: 151 cases (2001-2012). J Am Vet Med Assoc 2014; 245(4):
401-407.
Chamberlain TP, Lommer MJ (2012). Clinical behavior of
odontogenic tumors. In: Verstraete FJM, Lommer M, eds. Oral and
maxillofacial surgery in dogs and cats. Edinburgh: Saunders
Elsevier, 2012: 403-410.
Coyle VJ, Rassnick KM, Borst LB, et al. Biological behaviour of
canine mandibular osteosarcoma. A retrospective study of 50 cases
(1999-2007). Vet Comp Oncol 2015; 13(2): 89-97.
Culp WT, Ehrhart N, Withrow SJ, et al. DC. Results of surgical
excision and evaluation of factors associated with survival time in
dogs with lingual neoplasia: 97 cases (1995-2008). J Am Vet Med
Assoc 2013; 242(10): 1392-1397.
Evans SM, Shofer F. Canine oral non-tonsillar squamous cell
carcinoma. Prognostic factors for recurrence and survival following
orthovoltage radiation therapy. Vet Radiol 1988; 29: 133-137.
Farcas N, Arzi B, Verstraete FJ. Oral and maxillofacial
osteosarcoma in dogs: a review. Vet Comp Oncol 2014; 12(3):
169-180.
Fiani N, Arzi B, Johnson EG, et al. Osteoma of the oral and
maxillofacial regions in cats: 7 cases (1999-2009). J Am Vet Med
Assoc 2011; 238(11): 1470-1475.
Fiani N, Verstraete FJ, Kass PH, et al. Clinicopathologic
characterization of odontogenic tumors and focal fibrous
hyperplasia in dogs: 152 cases (1995-2005). J Am Vet Med Assoc
2011; 238: 495-500.
Gardner H, Fidel J, Haldorson G, Dernell W, Wheeler B. Canine
oral fibrosarcomas: a retrospective analysis of 65 cases
(1998-2010). Vet Comp Onco 2015; 13(1): 40-47.
Head KW, Cullen JM, Dubielzig RR, et al. Histological
Classification of Tumors of the Alimentary System of Domestic
Animals (WHO). Washington DC: Armed Forces Institute of Pathology,
2003.
Herring ES, Smith MM, Robertson JL. Lymph node staging of oral
and maxillofacial neoplasms in 31 dogs and cats. J Vet Dent 2002;
19(3): 122-126.
Hillman LA, Garrett LD, de Lorimier LP, et al. Biological
behavior of oral and perioral mast cell tumors in dogs: 44 cases
(1996-2006). J Am Vet Med Assoc 2010; 237(8): 936-942.
Liptak JM, Withrow SJ. Cancer of the gastrointestinal tract.
Section A: oral tumors. In: Withrow SJ, Vail DM, eds. Withrow &
MacEwen’s Small Animal Clinical Oncology. St Louis: Saunders
Elsevier, 2007.
Lommer MJ, Verstraete FJM. Principles of oral oncologic surgery.
In: Verstraete FJM, Lommer M, eds. Oral and maxillofacial surgery
in dogs and cats. Edinburgh: Saunders Elsevier, 2012: 423-430.
McEntee MC. Clinical behavior of nonodontogenic tumors. In:
Verstraete FJM, Lommer M, eds. Oral and maxillofacial surgery in
dogs and cats. Edinburgh: Saunders Elsevier, 2012: 387-402.
Nemanic S, London CA, Wisner ER. Comparison of thoracic
radiographs and single breath-hold helical CT for detection of
pulmonary nodules in dogs with metastatic neoplasia. J Vet Intern
Med 2006; 20(3): 508-515.
Nemec A, Murphy B, Kass PH, et al. Histological subtypes of oral
non-tonsillar squamous cell carcinoma in dogs. J Comp Pathol 2012;
147: 111-120.
Ottnod JM, Smedley RC, Walshaw R et al. A retrospective analysis
of the efficacy of Oncept vaccine for the adjunct treatment of
canine oral malignant melanoma. Vet Comp Oncol 2013; 11(3):
219-229.
Regezi JA, Verstraete FJM. Clinical-pathologic correlations. In:
Verstraete FJM, Lommer M, eds. Oral and maxillofacial surgery in
dogs and cats. Edinburgh: Saunders Elsevier, 2012; 381-385.
Soltero-Rivera MM, Krick EL, Reiter AM, Brown DC, Lewis JR.
Prevalence of regional and distant metastasis in cats with advanced
oral squamous cell carcinoma: 49 cases (2005-2011). J Feline Med
Surg 2014; 16(2): 164-169.
Todoroff RJ, Brodey RS. Oral and pharyngeal neoplasia in the
dog: a retrospective survey of 361 cases. J Am Vet Med Assoc 1979;
175: 567-571.
-
XXIX. SIMPOZIJ O AKTUALNIH BOLEZNIH MALIH ŽIVALI ZBORNIK
REFERATOV
Portorož, 8. in 9. april 2016
18
CANINE AND FELINE SOFT TISSUE SARCOMAS
Laurent Findji
The term soft tissue sarcoma (STS) refers to a group of
mesenchymal tumours originating in soft tissues (connec-tive,
adipose, muscular, nervous and fibrous tissues) and sharing
somewhat similar pathological appearances and biological
behaviours. These tumours are classically re-ported to be
potentially locally aggressive (pseudo-encap-sulated, easily spread
along and through fascial planes), with a marked tendency to recur
when incompletely re-sected but a limited metastatic potential. For
most STS, the preferred route for metastasis is haematogeneous. In
general, their histopathological grade is predictive for local
recurrence and metastasis, and surgical margins after exci-sion are
predictive for local recurrence. The most common tumour types of
the STS of the skin and subcutis include fi-brosarcoma, peripheral
nerve sheath tumour, perivascular wall tumour
(haemangiopericytoma), myxosarcoma and liposarcoma. Although
histiocytic sarcomas, lymphangio-sarcomas and haemangiosarcomas are
by definition soft tissue sarcomas, they are often not considered
as such because their different, more aggressive biological
behav-iour, which warrants to consider and treat them differently
from other, more classic STSs.
Although STS can occur anywhere in the body (e.g. splenic
haemangiosarcoma, intestinal leiomyosarcoma, urinary bladder
rhabdomyosarcoma), this text will focus on cutaneous and
subcutaneous STS.
In cats, a particular type of STS is feline injection-site
sarcomas, whose aetiology, clinical presentation and bio-logical
behaviour differs from other canine and feline STS to some degree.
They will be discussed separately at the end of this text.
Epidemiology, clinical signs and diagnosis
The median age of animals affected with STS is 10 years (5-17
years) in dogs and 8 to 11 years in cats (1-17 years). The reported
proportions of STS among all cutane-ous and subcutaneous tumours
are 8% to 15% in dogs, and 7% to 18% of in cats2.
Cutaneous and subcutaneous STS tend to be firm, ad-herent,
slow-growing masses. The clinical signs associated with them
largely depend on their location and relation-ships with
surrounding anatomical structures. Typically, STS are not
associated with significant systemic effects, although some
paraneoplastic syndromes can be encoun-tered, such as hypoglycaemia
with muscle tumours (leio-myomas, leiomyosarcomas,
rhabdomyosarcomas), and anaemia and thrombocytopenia with HSAs and
dissemi-nated histiocytic sarcomas.
Fine-needle aspirations (FNAs) are recommended to rule out
non-neoplastic lesions and to differentiate mes-enchymal tumours
from round cell tumours. However, STS tend to not exfoliate well
and give poorly cellular sam-ples. In one study, FNAs lead to a
correct diagnosis in only 62.5% of STS, whereas 96% of mast cell
tumours were correctly diagnosed3. Fine-needle aspirations are also
rec-ommended for evaluation of regional lymph nodes for high-grade
tumours or the untypical STS which have a propensity to metastasise
to lymph nodes (e.g. synovial cell sarcomas, histiocytic sarcomas,
lymphangiosarcomas, haemangiosarcomas).
Biopsies of the primary mass are therefore recom-mended.
Core-needle or incisional biopsies are preferred, as excisional
biopsies are fraught with the risk of achieving insufficient
margins, which complicates further treatments and jeopardises the
clinical response and overall survival.
Advanced imaging (CT scan, MRI) is most helpful in the local
staging (T staging) of the tumour. It allows de-termination of the
tumours extension in 3 dimensions and identification of the
surrounding anatomical structures, which greatly facilitates the
treatment planning of the lo-cal disease, whether it be surgery,
radiotherapy or both.
STS tend to spread haematogeneously, preferentially to the
lungs, and metastasis to regional lymph nodes is uncommon, except
for synovial cell sarcomas. Distant staging (M staging) should
therefore always include imag-ing of the chest either through 3
radiographic views or CT scan of the chest, knowing that CT is more
sensitive than conventional radiographs for detection of thoracic
meta-static disease4.
The gathered information (tumour diagnosis and grade, and TNM
staging) is used to define the tumour stage (Table 1).
Laurent Findji DMV MS MRCVS DiplECVS Fitzpatrick Referrals
Guildford GU7 2AJ, United Kingdom
-
ZBORNIK REFERATOV XXIX. SIMPOZIJ O AKTUALNIH BOLEZNIH MALIH
ŽIVALI
Portorož, 8. in 9. april 2016
19
T Primary tumour
TX Primary tumour cannot be assessed
T0 No evidence of primary tumour
T1 Tumour 5 cm in greatest dimension
T2a Superficial tumour*
T2b Deep tumour*
N Regional lymph nodes
NX Regional lymph nodes cannot be assessed
N0 No regional lymph node metastasis
N1 Regional lymph node metastasis
M Distant metastasis
MX Distant metastasis cannot be assessed
M0 No distant metastasis
M1 Distant metastasis
G Histologic grade
GX Grade cannot be assessed
G1 Low (grade I)
G2 Intermediate (grade II)
G3 High (Grade III)
Stage
I G1–2 Any T N0 M0II G3 T1a-b,T2a N0 M0III G3 T2b N0 M0IV Any G
Any T N1 Any M
Any G Any T Any N M1
* A superficial tumour is a tumour located above the superficial
fascia and not invading it.
A deep tumour is located deep to the superficial fascia, invades
it, or both.
Adapted from Ryan et al.2
Table 1: TNM staging and grading of soft tissue sarcomas
Treatment
Since typical STS metastasise infrequently but have a marked
propensity for local recurrence, the main con-cern in their
treatment most often is local tumour control. Therefore, complete
surgical excision is the treatment of choice, whenever possible.
When surgery is unlikely or fails to provide sufficient margins, it
can be combined with radiotherapy, either in an adjuvant or
neoadjuvant setting. When surgery is not possible, radiotherapy can
be consid-ered as the main treatment, although it is most likely to
only be palliative in the face of macroscopic disease. Lastly, the
role of chemotherapy in the treatment of typical STS is unclear,
although new protocols (local or metronomic chemotherapy) may prove
of value.
SurgeryThe surgical treatment of STS should abide by the
rules
of oncologic surgery. The surgical treatment of STS should abide
by the rules of oncologic surgery. In all cases, com-plete excision
should be thought. The width of surgical margins to be sought
should be determined on a case-ba-sis. When possible, 1-3 cm
lateral margins and 1-2 fascial plane in depth should be sought,
depending on each par-
ticular tumour, taking into consideration its location,
clini-cal features (inflammation, invasion, adhesion to underly-ing
structures, size, rate of growth, biopsy grading, etc.). Absolute
recommendations applicable to all canine soft tissue sarcoma can
however not be made, and increasing evidence exists that tumour
biology, and not the size of surgical margins, is the main
determinant of the outcome in dogs5, 6. It is essential to keep in
mind that STS may seem encapsulated but that they are only
surrounded by a pseudocapsule actually constituted of compacted
tumour cells. Therefore, a marginal or narrow excision should not
be considered a satisfactory primary surgical objective.
One potential exception concerns low-grade STS of the
extremities, for which marginal resection may provide satisfactory
local tumour control and survival times. Recur-rence rates of
marginally resected low-grade STS of the extremities (distal to the
elbow or stifle) have been report-ed to be 11% overall7. In another
study, recurrence rates were dependant on the grade of the
marginally resected canine STS: 7% for grade 1, 24% for grade 2 and
75% for grade 3, although the number of grade 3 STS included in
this study (n=4) was too low for this figure to be reliable8. No
recurrences were observed when wide resection was performed,
indicating that clean tumour margins were predictive for
non-recurrence (n=30)8. Another study of
-
XXIX. SIMPOZIJ O AKTUALNIH BOLEZNIH MALIH ŽIVALI ZBORNIK
REFERATOV
Portorož, 8. in 9. april 2016
20
revision excision of incompletely excised STS on 41 dogs found
recurrence and metastatic rates of 15% and 10%, respectively9. The
presence of residual tumour was identi-fied in 22% of resected scar
tissues and it did not appear to predict recurrence9. When marginal
resection of STS of the limbs was intentional and followed by
adjuvant radio-therapy (hypofractionated protocol, 4 x 8-9Gy),
recurrence rates of 18% have been observed and the only factor
pre-dicting recurrence appeared to be the delay between sur-gery
and radiotherapy10.
In view of these studies, marginal resection of canine low-grade
STS of the extremities may be considerable, ei-ther alone or
combined with radiotherapy, when a wider excision is not easily
possible. In this setting, the propor-tion of dogs dying of causes
related to their STS varies between 10% and 33%2.
As stated above, advanced imaging is most valuable in planning
surgery, as the main obstacles to achieving suffi-cient margins are
the vicinity of non-expendable anatomi-cal structures (resection
phase) and the ability to recon-struct the operated area
(reconstruction phase).
When considering the resection phase, the targeted margins are
planned from the 3-dimensional advanced images and any important
anatomical structure located within them is considered. The benefit
of achieving the sought margins should be balanced against the
potential functional and cosmetic consequences of sacrificing these
structures, and a decision can be made. When all tissues within the
planned margins are considered expendable, the surgical excision is
considered likely to be satisfactory. When not, the surgery will be
unlikely to provide sufficient margins and adjuvant therapies
should be considered.
The reconstruction phase is however often the most challenging
part of the surgery of STS. In general, onco-logic surgery requires
a solid knowledge of reconstruc-tive surgery, as limitations in the
ability to reconstruct a wound should never lead to insufficiently
wide resections. The greater the reconstruction abilities of the
surgeon, the more comfortable they will be administering the
appropri-ate dose of surgery in the face of a large or awkwardly
located tumour.
RadiotherapyRadiotherapy can be used either alone or
combined
with surgery for local disease control.
Used as the sole treatment, it is mainly palliative.
Ra-diotherapy cannot cure macroscopically detectable sarco-mas, as
these tumours are radioresistant. In this setting, “control” is
therefore defined as regression or stabilisation of the tumour
size. With radiotherapy as the sole treat-ment, control rates of
STS have been reported to be 50% at 1 year and 33% at 2 years11,
12. A hypofractionated pro-tocol (4x8Gy) was associated with a 50%
response rate, a median time to progression of the disease of 155
days (72-460 days) and a mean survival time of 309 days in a study
of 16 dogs with STS11. Combination of radiation with hyperthermia
increases the median duration of local
control (350 days for radiotherapy alone versus 750 days
combined with hyperthermia)1.
Radiotherapy is best used as a combination with sur-gery, either
in a neoadjuvant or adjuvant setting. It is also indicated when
insufficient margins are achieved by sur-gery, and revision surgery
is not possible or unlikely to be more successful13, 14. Control
rates for adjuvant radiothera-py after incomplete excision of STS
in dogs are reported to be 80-95% at 1 year and 72-91% at 2 years,
with 3-year and 5-year survival rates of 76% and 68%1. Reported
recurrence rates after revision surgery or adjuvant radio-therapy
have been reported to be 15%9 and 17-31%13-15, respectively. Median
survival times after revision surgery (1416 days16) are comparable
to those after adjuvant radiotherapy (1851 days14). Adjuvant
radiotherapy for in-completely excised STS has been reported to be
associated with lower median survival times for oral tumours (540
days) than tumours of other sites (2270 days)14.
ChemotherapyMost STS are resistant to chemotherapy with
response
rates typically being below 30%. Chemotherapy is there-fore not
a good option as the primary treatment for STS.
On the other hand, the benefit of adjuvant chemo-therapy after
complete excision of STS is unclear, except for non-typical STS
having a moderate-to-high metastatic rate, such as
haemangiosarcomas (grade II, III or viscer-al), histiocytic
sarcomas, etc. Chemotherapy can also be considered for
metastasised, high-grade or incompletely-excised STS. Protocols
used for treatment of STS are based on a single agent (e.g.
doxorubicin or mitoxantrone) or combinations of chemotherapeutic
drugs including doxo-rubicin, vincristine and cyclophosphamide.
Metronomic chemotherapy using piroxicam and low-dose doxorubicin
seems to prolong the disease-free interval in dogs with
incompletely excised STS17.
The role of neoadjuvant (primary) chemotherapy be-fore surgery
for STS remains to be investigated in veteri-nary medicine.
ImmunotherapySeveral studies have investigated the effect of
immu-
notherapy on recurrence rates of soft tissue sarcomas.
Ad-ministration of interleukin 2 (IL-2) via viral vectors has been
shown to decrease recurrence rates of spontaneous feline soft
tissue sarcomas. Increases in the disease-free intervals and
survival times have also been observed after intratu-moral
administration of histocompatible cells expressing human IL-2.
Prognosis
The prognosis for STS is very variable and depends on the
precise nature of the tumour. For typical STS, it is fair and the
main obstacle to cure is local disease control. Re-currence rates
after surgery, with or without radiotherapy, have been reported to
be 7% to 32%. Prognostic factors for tumour recurrence include
tumour grade, tumour size and incomplete surgical excision.
-
ZBORNIK REFERATOV XXIX. SIMPOZIJ O AKTUALNIH BOLEZNIH MALIH
ŽIVALI
Portorož, 8. in 9. april 2016
21
The metastasic rate of STS is reported to be around 20%, and it
is dependent on the tumour grade, ranging from 15% for grades 1 and
2, to 41% for grade 3 STS1. The metastases tend to be delayed and
occur late in the course of the disease with a median time to
development of metastatic disease of 365 days1.
Since the time to local recurrence and distant metas-tasis
development can be long, it is important to follow the affected
patients on the long-term. An example of recommended schedule would
be to recheck the patient at 1,2,3,6,9 and 12 months after
treatment, and twice a year thereafter.
Feline injection-site sarcomas
Feline injection-site sarcomas (FISS) include different types of
tumours of similar clinical presentation and be-haviour, occurring
in the location of a previous inflamma-tion (injection, insect bite
wound, etc.). The pathogene-sis of these tumours is still poorly
understood, but local growth factors and cellular mutations seem
involved in the malignant transformation of fibroblast within the
in-flammation. They are extremely locally invasive tumours which
tend to metastasise infrequently (up to 26%18) and late in their
course. However, as veterinarians’ ability to achieve local control
of these tumours improve (better planned surgeries, adjuvant
radiotherapy, chemotherapy), cats survive longer and it seems that
metastases are more frequent a problem than originally reported. In
any event, when metastatic disease is not detected at the time of
diagnosis, these tumours are mainly a local problem for which an
aggressive (wide) resection, whenever possible, is the treatment of
choice. In cats, sarcomas developing in the location of an
inflammation (“FISS”) tend to be more aggressive than other soft
tissue sarcomas19. Practically, sarcomas occurring in areas of
injections (vaccine or oth-ers) or in the location of an earlier
trauma (bite, wound, etc.) must be treated aggressively (wide
surgical excision and radiotherapy as possible).
SurgeryWhen to operate?
Any mass located in the location of an injection or
inflammation, with clinical and cytological presentations
compatible with a sarcoma must be excised widely. How to manage an
inflammatory or post-injection reaction is more controversial. When
does an inflammatory reaction become suspicious enough to be
treated as a malignancy? Most authors base their approach on the
guidelines of the Vaccine-Associated Feline Sarcoma Task Force
(VAFSTF) which recommends to treat as FISS any inflammatory
re-action persisting more than 3 months after an injection,
measuring more than 2 cm or still increasing in size more than 1
month after the injection20.
How to plan surgery?Advanced imaging techniques
(contrast-enhanced CT
and MRI) are essential to precisely determine the tumour
invasion in 3 dimensions, which will dictate the extent of the
required surgical excision. The external physical pres-entation of
the tumour can be deceiving and the tumoral
volume as determined from a CT study was found to be twice as
large as the volume estimated from direct physical measurement of
the tumour21.
How to operate?Initially, it has been recommended to excise FISS
with
a minimum of 2-cm lateral margins and one deep fascial plane.
These recommendations are not sufficient and lead to complete
excision of such tumours in less than 50% of cases22, 23, which
results in high recurrence rates. A more aggressive surgery is
associated with better results: in a study of 61 cases, the time to
first recurrence was sig-nificantly shorter after marginal
resection than after wide resection (66 versus 419 days)22.
Similarly, cats operated by non-specialist veterinarians appeared
to have earlier recurrences than those operated in a referral
centre (66 versus 274 days)22. Whereas surgery as sole treatment is
not currently the gold standard of FISS treatment (combin-ing
surgery with radiotherapy and chemotherapy improve the
prognosis24), it clearly appears that a more aggressive surgery is
associated with a better outcome in terms of disease-free interval
and survival times, whether the sur-gery be used alone or combined
with other treatments. Some surgeons recommend excising FISS with
5-cm lateral margins and two deep fascial planes25. This more
aggres-sive approach resulted in complete excision of the tumour in
97% of cases, leading to a recurrence rate of 11% and disease-free
rates of 91%, 86% and 74% at 1, 2 and 3 years, respectively26. A
larger retrospective study of this approach (91 cases) reported a
recurrence and metastatic rates of 14% and 20% respectively27.
Median survival times were 499 days for cats with tumour recurrence
ver-sus 1461 days for cats without27. Median survival times were
388 days for cats which developed metastatic dis-ease and 1528 days
for cats who did not27. The drawbacks of such an approach are the
more challenging reconstruc-tions and the increased rate of wound
dehiscence. In this latter study, 7 out of 91 cats (8%) had
dehiscence of their surgical wound27.
The wide excision of FISS often involves extensive re-sections,
frequently including bony resections (spinous processes, scapulae,
etc.). Similarly, wound reconstruction can be technically
challenging and necessitate placement of prostheses, such as
meshes, and skin or myocutaneous flaps28.
These aggressive resections are very traumatic and in-duce
severe pain. In addition to usual analgesia routes, the use of
wound catheters is very efficacious. These cath-eters are
commercially available, but can alternatively be designed from
polyethylene tubing18. They are placed in the wound during surgery
and are used postoperatively to instil local anaesthetics in the
wound for several days after surgery. I routinely use these
catheters after FISS resection. They subjectively are very helpful
to control postoperative pain and make it possible to lower the
doses and limit the side-effects of other analgesic drugs.
Radiotherapy
Ideally, as FISS have a high local recurrence rate in spite
-
XXIX. SIMPOZIJ O AKTUALNIH BOLEZNIH MALIH ŽIVALI ZBORNIK
REFERATOV
Portorož, 8. in 9. april 2016
22
of surgery, radiotherapy should always be associated to surgery
in their treatment. Radiotherapy can be neoad-juvant or adjuvant.
With FISS, neoadjuvant radiotherapy may be of particular interest,
although studies have failed to show a significant improvement in
local tumour control in this setting29, 30. When radiotherapy is
combined with surgery, mean survival times of 600 to 1300 days have
been reported, with 1-, 2- and 3-year survival rates of 86%, 44-71%
and 28-68%, respectively.
Radiotherapy alone is only palliative but can be consid-ered for
inoperable tumours.
Chemotherapy
For the moment, chemotherapy seems to be of lim-ited benefit in
the treatment of FISS. In a study of 76 cats with FISS treated with
surgery and radiotherapy, with or without chemotherapy, the latter
made no difference in recurrence rates, metastatic rates and
survival times (Co-hen JAVMA 2001). Responses have been reported
with doxorubicin, either alone or combined, but these lasted only a
few months31, 32. However, in cats responding to chemotherapy it
appeared to prolong survival, including for incompletely excised
tumours also treated with radio-therapy33.
References
1. Liptak JM, Forrest LJ. Soft tissue sarcomas. In: Withrow SJ,
Vail DM, Page RL (eds): Withrow & MacEwen’s small animal
clinical oncology, 2013;356-380.
2. Ryan S, Wouters EGH, Van Nimwegen S, Kirpensteijn J. Skin and
subcutaneous tumors. In: Kudnig ST, Séguin B (eds): Veterinary
surgical oncology. Oxford: Wiley-Blackwell, 2012;55-85.
3. Baker-Gabb M, Hunt GB, France MP. Soft tissue sarcomas and
mast cell tumours in dogs; clinical behaviour and response to
surgery. Aust Vet J. 2003;81: 732-738.
4. Yoon J, Feeney DA, Cronk DE, Anderson KL, Ziegler LE.
Computed tomographic evaluation of canine and feline mediastinal
masses in 14 patients. Veterinary Radiology & Ultrasound.
2004;45: 542-546.
5. Bray JP, Polton GA, McSporran KD, Bridges J, Whitbread TM.
Canine soft tissue sarcoma managed in first opinion practice:
outcome in 350 cases. Veterinary Surgery. 2014;43: 774-782.
6. Chase D, Bray J, Ide A, Polton G. Outcome following removal
of canine spindle cell tumours in first opinion practice: 104
cases. Journal of Small Animal Practice. 2009;50: 568-574.
7. Stefanello D, Morello E, Roccabianca P, Iussich S, Nassuato
C, Martano M, et al. Marginal excision of low-grade spindle cell
sarcoma of canine extremities: 35 dogs (1996-2006). Veterinary
Surgery. 2008;37: 461-465.
8. McSporran KD. Histologic Grade Predicts Recurrence for
Marginally Excised Canine Subcutaneous Soft Tissue Sarcomas.
Veterinary Pathology Online. 2009;46: 928-933.
9. Bacon NJ, Dernell WS, Ehrhart N, Powers BE, Withrow SJ.
Evaluation of primary re-excision after recent inadequate resection
of soft tissue sarcomas in dogs: 41 cases (1999–2004). Journal of
the American Veterinary Medical Association. 2007;230: 548-554.
10. Demetriou JL, Brearley MJ, Constantino-Casas F, Addington C,
Dobson J. Intentional marginal excision of canine limb soft tissue
sarcomas followed by radiotherapy. Journal of Small Animal
Practice. 2012;53: 174-181.
11. Lawrence J, Forrest L, Adams W, Vail D, Thamm D.
Four-fraction radiation therapy for macroscopic soft tissue
sarcomas in 16 dogs. Journal of the American Animal Hospital
Association. 2008;44: 100-108.
12. McChesney SL, Withrow SJ, Gillette EL, Powers BE, Dewhirst
MW. Radiotherapy of soft tissue sarcomas in dogs. Journal of the
American Veterinary Medical Association. 1989;194: 60-63.
13. McKnight JA, Mauldin GN, McEntee MC, Meleo KA, Patnaik AK.
Radiation treatment for incompletely resected soft-tissue sarcomas
in dogs. Journal of the American Veterinary Medical Association.
2000;217: 205-210.
14. Forrest LJ, Chun R, Adams WM, Cooley AJ, Vail DM.
Postoperative radiotherapy for canine soft tissue sarcoma. Journal
of Veterinary Internal Medicine. 2000;14: 578-582.
15. Simon D, Ruslander DM, Rassnick KM, Wood CA, Frimberger AE,
Cotter SM, et al. Orthovoltage radiation and weekly low dose of
doxorubicin for the treatment of incompletely excised soft-tissue
sarcomas in 39 dogs. Veterinary Record. 2007;160: 321-326.
16. Kuntz CA, Dernell WS, Powers BE, Devitt C, Straw RC, Withrow
SJ. Prognostic factors for surgical treatment of soft-tissue
sarcomas in dogs: 75 cases (1986-1996). Journal of the American
Veterinary Medical Association. 1997;211: 1147-1151.
17. Elmslie RE, Glawe P, Dow SW. Metronomic therapy with
cyclophosphamide and piroxicam effectively delays tumor recurrence
in dogs with incompletely resected soft tissue sarcomas. Journal of
Veterinary Internal Medicine. 2008;22: 1373-1379.
18. Davis KM, Hardie EM, Lascelles BDX, Hansen B. Feline
fibrosarcoma: perioperative management. Compendium Continuing
Education for Veterinarian. 2007;29: 712-729.
19. Hauck M. Feline injection site sarcomas. Veterinary Clinics
of North America, Small Animal Practice. 2003;33: 553-571.
20. Morrison WB, Starr RM. Vaccine-associated feline sarcomas.
Journal of the American Veterinary Medical Association. 2001;218:
697-702.
21. McEntee MC, Page RL. Feline vaccine-associated sarcomas.
Journal of Veterinary Internal Medicine. 2001;15: 176-182.
22. Hershey AE, Sorenmo KU, Hendrick MJ, Shofer FS, Vail DM.
Prognosis for presumed feline vaccine-associated sarcoma after
excision: 61 cases (1986-1996). Journal of the American Veterinary
Medical Association. 2000;216: 58-61.
23. Davidson EB, Gregory CR, Kass PH. Surgical excision of soft
tissue fibrosarcomas in cats. Veterinary Surgery. 1997;26:
265-269.
24. Séguin B. Feline injection site sarcomas. Veterinary Clinics
of North America, Small Animal Practice. 2002;32: 983-995.
25. Kuntz CA. Modified wide local excision for vaccine
associated soft tissue sarcomas in cats (abstract). Veterinary
Surgery. 2000;29.
26. Liptak JM, Forrest LJ. Soft tissue sarcomas. In: Withrow SJ,
Vail DM (eds): Withrow & MacEwen’s small animal clinical
oncology. St. Louis, Mo.: Saunders Elsevier, 2007;425-454.
27. Phelps HA, Kuntz CA, Milner RJ, Powers BE, Bacon NJ. Radical
excision with five-centimeter margins for treatment of feline
injection-site sarcomas: 91 cases (1998-2002). Journal of the
American Veterinary Medical Association. 2011;239: 97-106.
-
ZBORNIK REFERATOV XXIX. SIMPOZIJ O AKTUALNIH BOLEZNIH MALIH
ŽIVALI
Portorož, 8. in 9. april 2016
23
28. Lidbetter DA, Williams FA, Jr., Krahwinkel DJ, Adams WH.
Radical lateral body-wall resection for fibrosarcoma with
reconstruction using polypropylene mesh and a caudal superficial
epigastric axial pattern flap: a prospective clinical study of the
technique and results in 6 cats. Veterinary Surgery. 2002;31:
57-64.
29. Kobayashi T, Hauck ML, Dodge R, Page RL, Price GS, Williams
LE, et al. Preoperative radiotherapy for vaccine associated sarcoma
in 92 cats. Veterinary Radiology & Ultrasound. 2002;43:
473-479.
30. Cronin K, Page RL, Spodnick G, Dodge R, Hardie EN, Price GS,
et al. Radiation therapy and surgery for fibrosarcoma in 33 cats.
Veterinary Radiology & Ultrasound. 1998;39: 51-56.
31. Poirier VJ, Thamm DH, Kurzman ID, Jeglum KA, Chun R,
Obradovich JE, et al. Liposome-encapsulated doxorubicin (Doxil) and
doxorubicin in the treatment of vaccine-associated sarcoma in cats.
Journal of Veterinary Internal Medicine. 2002;16: 726-731.
32. Barber LG, Sørenmo KU, Cronin KL, Shofer FS. Combined
doxorubicin and cyclophosphamide chemotherapy for nonresectable
feline fibrosarcoma. Journal of the American Animal Hospital
Association. 2000;36: 416-421.
33. Eckstein C, Guscetti F, Roos M, Martín de las Mulas J,
Kaser-Hotz B, Bley CR. A retrospective analysis of radiation
therapy for the treatment of feline vaccine-associated sarcoma.
Veterinary and Comparative Oncology. 2009;7: 54-68.
-
XXIX. SIMPOZIJ O AKTUALNIH BOLEZNIH MALIH ŽIVALI ZBORNIK
REFERATOV
Portorož, 8. in 9. april 2016
24
TUMOURS OF THE BODY WALL
Laurent Findji
In oncologic surgery, full-thickness resections of por-tions of
the abdominal and thoracic walls are not un-common. They may be
required for treatment of primary tumours of the body wall (e.g.
rib tumours) or to obtain sufficient margins when resecting tumours
of nearby tis-sues (e.g. soft tissue sarcomas, pulmonary or
mediastinal tumours).
Tumour types
Tumours most frequently requiring thoracic wall resec-tions are
rib osteosarcomas (OSA) and chondrosarcomas (CSA), as well as
tumours of soft tissues of the thoracic wall itself or of tissues
in its vicinity, such as soft tissue sarcomas.
Diagnosis
The diagnosis of body wall tumours often starts by the detection
of a subcutaneous mass over the trunk. The ex-ternal aspect of
these tumours can be deceiving and ad-vanced imaging (CT scanning
or MRI) is essential to plan their potential surgical resection.
The origin of the tumour, from which the tissue planes to resect
can be decided, and its intracavitary extension can be determined
from ad-vanced imaging. Conventional radiography can also show
invasion of body cavities by the tumour, especially for the
thoracic cavity, but with lesser sensitivity and reliability.
Preoperative biopies are essential. Fine-needle aspi-rates are
often insufficient to obtain a reliable diagnosis of the tumoral
type and, in any case, cannot provide grading of the tumour.
Incisional biopsies can be performed with a core-needle or
surgically (e.g. wedge biopsies). Surgical biopsies are more
reliable because of their larger size1. As per general rules of
oncologic surgery, it is crucial not to jeopardise the potential
subsequent surgical resection and the fact that the biopsy tract
will require to be excised en-bloc with the tumour needs to be
carefully anticipated.
Treatment
SurgeryIdeally, surgery must be planned from advanced imag-
ing studies. When resecting rib tumours, the excision must
include at least one rib cranially and one rib caudally to the
affected rib and, in the dorsoventral direction, margins of at
least 3 cm are generally recommended. This recom-mendation is
obviously not rigid and the required margins depend on the tumour
type and size. In addition, a com-partmental resection of the
affected rib (i.e. resecting the entire rib) can be preferable for
locally aggressive tumours (e.g. OSA).
For tumours infiltrating or in the vicinity of the thoracic
wall, the number of ribs to resect is determined from the findings
of advanced imaging and the determined tumour type and grade. It is
widely accepted that up to 6 ribs can safely be resected without
any rigid reconstruction of the chest wall. Resecting 7 ribs has
however been reported2 and is considered feasible by surgical
oncologists. Con-versely, it seems that resecting 8 ribs or more is
more likely to result in significant functional impairment of the
tho-racic wall and is not recommended.
When resecting tumours originating from the tho-racic (ribs,
intercostal muscles) and abdominal (transverse, oblique or rectus
abdominis muscles) walls, the number of tissue layers external
(superficial) to the tumour is suf-ficient to make wide resection
of the skin unnecessary. Therefore, except for any biopsy tracts, a
linear or curvi-linear incision of the skin and cutaneous trunci
muscle is appropriate. When a biopsy tract is present, it must
ex-cised en-bloc with the tumour with at least 2 to 3 cm of lateral
margins. This general rule is obviously not absolute and the
necessity to resect portions of skin is best judged on the
extension of the tumour as evaluated on advanced imaging, as well
as from the subjective assessment of the adherence of the skin and
subcutaneous tissues to the un-derlying tumour.
Conversely, when resecting more superficial tumours, wide
resection of the skin, en-bloc with the rest of the excision, is
most often indicated.
For thoracic wall resections, depending on tumour ex-tension,
the latissimus dorsi muscle is either partially re-sected along the
lines of the underlying costal resection or reclined dorsally if it
can be spared2. Again, determining
Laurent Findji DMV MS MRCVS DiplECVS Fitzpatrick Referrals
Guildford GU7 2AJ, United Kingdom
-
ZBORNIK REFERATOV XXIX. SIMPOZIJ O AKTUALNIH BOLEZNIH MALIH
ŽIVALI
Portorož, 8. in 9. april 2016
25
whether the latissimus dorsi muscle can be spared or must be
resected is best done by assessing the number of tissue planes
between it and the tumour from advanced imaging studies.
Thoracic wall resections generally starts with an in-tercostal
thoracotomy at the cranial or caudal boundary of the planned
resection. The safest thoracotomy site, in terms of margins, must
be chosen on the base of ad-vanced imaging. This thoracotomy allows
verification of the macroscopic intrathoracic extension of the
tumour, to ascertain that it is not greater than assessed on
advanced imaging. Ribs are then sectioned with an oscillating saw
or rib shears, along the line of the ventral or dorsal bound-ary of
the planned resection. Between each rib section, the intercostal
muscles are cut and the intercostal artery and vein are cauterised
with uni- or bipolar electrocautery. Once this ventral or dorsal
section has been carried out, the costal flap can be slightly
elevated to assess once more the macroscopic extension of the
tumour and verify that the next planned section line is
appropriate. The next sec-tion line is then performed
(ventral/dorsal or caudal/cra-nial) and, once more, the tumour
position and extension is checked by elevating the costal flap
further. The remaining section line is then performed and the
costal flap is freed. It is lifted gently and the presence of any
adhesions of the flap/tumour with intrathoracic structures
(diaphragm, lungs) is evaluated. When the tumour is adherent to the
diaphragm, the latter is partially resected with a minimum a 2 to 3
cm margins, en-bloc with the tumour and chest wall. When the tumour
is adherent to a lung lobe, a partial or complete lung lobectomy.
If a complete lung lobectomy is chosen, it is most easily performed
with a stapler (e.g. TA stapler) as the pulmonary hilus may be
quite remote from a rather caudal costal flap and therefore be
difficult to reach. Occasionally, adhesions of the tumour with the
pericardium necessitate to perform a partial pericardec-tomy. In
all such cases, adhesions between the tumour and intrathoracic
structures are not detached to avoid dis-semination of tumour cells
in the surgical field and chest. The adhered organ is partially
resected en-bloc with the tumour whenever possible.
A chest drain is then placed under direct visual control and
intercostal nerve blocks are performed on resected rib spaces and 2
to 3 spaces cranially and caudally to them.
The chest wall is then reconstructed. Several tech-niques are
available to restore the functional capacity of the rib cage. When
the wall resection involved caudal ribs and the diaphragm needed to
be disinserted, it can be attached to the remaining dorsal portion
of the sectioned ribs and along the rib immediately cranial to the
thoracic wall defect. This technique is referred to as
diaphragmatic advancement. Once the diaphragm is advanced, the
tho-racic cavity is reconstituted and closed, but of a smaller
volume than previously. The body wall defects then be-comes an
abdominal well defect. When the diaphragm is markedly advanced, the
diminution in the volume of the thoracic cavity can be
physiologically significant and cause ventilation-perfusion
mismatches in the lung on the oper-ated side, which cannot fully
expand. Therefore, when the
diaphragmatic advancement results in a great reduction of the
thoracic volume, raising concerns about the expansion of the
ipsilateral lung, it can be preferable to perform a caudal lung
lobectomy to prevent any postoperative res-piratory
complications.
The reconstruction of body wall defects must use au-tologous
tissues as often and as much as possible to re-duce the risk of
postoperative complications3. The utilisa-tion of synthetic meshes
only to reconstruct defects in the thoracic wall was associated
with 12.8 times more compli-cations and the combined use of meshes
and autologous tissues with 3 times more complications, both
compared with the exclusive use of autologous tissues3. In many
cas-es, a muscle flap using the latissimus dorsi can be used to
cover thoracic wall defects. To perform such a flap, the
cranioventral insertion of the muscle on the humerus is left intact
and its caudodorsal insertion is on the lumbar fascia is sectioned
as caudally and as dorsally as possible to elevate the muscle,
which is then transposed and sutured to the edges of the thoracic
wall defect, thereby covering it. Other muscle flaps, using nearby
muscles such as pecto-rals, or lumbar fascia grafts can also be
used to cover the parietal defect. Lastly, when all sources of
autologous tis-sues are insufficient to entirely cover the body
wall defect, synthetic implants such as meshes, either
non-absorbable (e.g. polypropylene) or absorbable (e.g.
polydioxanone), can be used. Ideally, intracavitary organs should
be pre-vented to come into contact with the mesh by interposing
autologous tissues. The greater omentum is most com-monly used for
this purpose. It is easily transposed and brought to the parietal
defect, directly for abdominal wall defects and either through a
retrocostal or transdiaphrag-matic approach for thoracic wall
defects.
The addition of rigid implants such a












![Zbornik referatov - GZS · Udovič]. - Ljubljana : Gospodarska zbornica Slovenije, Zbornica za poslovanje z nepremičninami, 2016 Zbornik povzetkov izšel v kompletu z zbornikom referatov](https://img.dokumen.tips/doc/110x75/5f034bf87e708231d408840e/zbornik-referatov-gzs-udovi-ljubljana-gospodarska-zbornica-slovenije.jpg)
![SLOVENSKO DRUŠTVO ZA ZNANOST V PROMETUsladkowski.com/uploads/publications/138/180a.pdf · Prometna politika [Elektronski vir] : zbornik referatov = Transport policy : conference](https://img.dokumen.tips/doc/110x75/5fca5387e314be0cda55ca14/slovensko-drutvo-za-znanost-v-prometna-politika-elektronski-vir-zbornik-referatov.jpg)