Embed Size (px)
Citation preview

The Foot (1994) 4, 88-91
0 1994 Longman Group Ltd
Wound healing after toenail avulsion
A comparison of Kaltostat and Melolin as postoperative dressings
G. B. Foley, J. Allen
Nail Surgery Unit, New Street Health Centre, Barnsley, UK
S UMMA R Y. Factors which may influence the rate of healing after toenail avulsion and phenolization were investigated by comparison of an alginate wound dressing (Kaltostat), with a non-adherent dry dressing (Melolin).
70 patients requiring partial or total nail avulsion were assessed for age, sex, smoking habits, ischaemic index of the limb requiring surgery, concurrent disease and medication. Surgery was performed according to a stan- dardized protocol, and the patients were assigned randomly to one of the two postoperative dressing treatment groups.
Time to complete healing varied from 7 to 70 days, and none of the patient factors recorded correlated with healing time. Mean healing time was reduced by 8.6 days in the alginate dressed group when compared to those who received the dry dressing. The number of postoperative dressing changes was correspondingly reduced by 1. Both differences were statistically significant (P ~0.05).
It was concluded that the concept of moist wound healing has a place in the postoperative management of toenail surgery.
Ingrowing toenail and onychogryphosis are common complaints. A recent survey of workers required to wear safety footwear found that 30% had ingrown toenails.’ Another survey’ indicated that 5% of all NHS chiropody patients required treatment for ingrowing toenails and a further 4% for ony- chogryphosis.
Recurrence rates of 45% have been reported in the conservative management of ingrown toenails.3 Partial or total nail avulsion can produce rapid relief of symptoms, but again recurrence rates are high unless additional measures are taken to prevent regrowth of the nail.4 This may be achieved by surgical excision, cauterization, cryotherapy or a variety of chemical agents, but the most reliable is ablation of the nail matrix with pheno1.3,4
In a comparative study of phenolization versus wedge excision’ recurrence of symptoms, postopera- tive pain and bleeding were all significantly more common with wedge resection, although the phe- nolized wounds took longer to heal. Healing is delayed as the phenol induces a chemical burn and the resultant necrotic tissue must separate from the wound bed before complete healing can be achieved.
Despite the increased use of the phenolization technique, little attention has been paid to the influence of wound dressings upon subsequent heal- ing. Frequent redressings are necessary until the operation site is completely healed, usually 4-6 weeks post-surgery, but up to 8 weeks where total nail avulsion has been performed.
88
In other areas of wound care the concept of moist wound healing has been widely accepted.‘j Autolysis of necrotic tissue and growth of epithelium are enhanced in a moist environment and a wide variety of wound dressings have been developed which aim to achieve these conditions. A small scale study7 found that healing time following toenail avulsion was 16 days less with a modern hydrocolloid dressing than with chlorhexidine gauze.
The object of this study was to investigate factors which influence the rate of healing after toenail avulsion and phenolization, including a comparison of an alginate wound dressing with a non-adherent dry dressing. The alginate was chosen as it holds a product licence for topical haemostasis, and was therefore likely to be effective in controlling any postoperative blood loss. Other factors studied included the patient’s ischaemic index, age, medical condition and concurrent medication. It was antici- pated that these measurements might have some correlation with the healing time and could be used to give patients a more reliable estimate of the time taken for the operation site to heal.
Ethical approval for this study was obtained from the Barnsley Health Authority Ethical Committee.
MATERIALS AND METHODS
Patients referred by their general practitioner for toenail surgery were assessed for inclusion in the

Comparison of Kaltostat and Melolin as postoperative dressings 89
study and informed consent was obtained. Patients with mycotic nail infections, and those undergoing treatment with antibiotics, steroids or immuno- suppressants were excluded. Also excluded were diabetics and patients with absent foot pulses or peripheral neuropathy.
Table 1. Criteria for healing
Assessment
1. 2. 3. 4. 5. 6. 7. 8.
No signs of infection No pain or tenderness around the operation site No exudate Operation site dry Re-epithelialization complete No swelling around the area No inflammation in the area The sensation in the operation area should be returned to normal
9. No irritation at the operation site
A presurgical assessment of each patient included their relevant medical history and smoking habits. The ischaemic index (ratio of brachial artery systolic pressure to posterior tibia1 systolic pressure) of the limb requiring surgery was also recorded.
Surgical technique
Kaltostat group the dressing was always replaced with moistened Kaltostat at the first outpatient review. At subsequent follow-up visits the chiropodist was permitted to use dry sterile gauze in place of Kaltostat if the wound was no longer sufficiently moist for the alginate to be an appropriate choice.
All surgery was carried out using a standardized protocol and full aseptic technique. The foot was swabbed preoperatively with 0.5% chlorhexidine gluconate in alcohol. Local anaesthesia was induced with lignocaine hydrochloride 2.13% w/v, maximum dose 80 mg, using a ring block technique. The toe was exsanguinated and a tourniquet applied. Following partial or total nail avulsion, liquefied phenol was applied to the exposed nail matrix for 90 s with a Black’s file. It was then dried with sterile gauze and irrigated with 100 ml of the chlorhexidine solution per side for partial or 200 ml for total nail avulsions.
The use of topical antiseptics was discouraged, and if these were used on two consecutive visits the patient was excluded. Postoperative infections and other complications were recorded. At each post- operative appointment the patients were asked to rate the dressings for comfort, acceptability and pain on dressing removal.
RESULTS
The wound dressing, either Kaltostat (BritCair, calcium sodium alginate 5 x 5 cm flat dressing) or Melolin (Smith & Nephew, cotton and acrylic fibre pad bonded to perforated low adherent polyester film 5 x 5 cm) was allocated by means of a predeter- mined random sequence.
If bleeding occurred after removal of the Esmarch toumequet the study dressing was applied, with pressure in the Melolin dressed group, until haemo- stasis was achieved. In the Melolin-treated group, all wounds were then dressed with fresh Melolin covered with sterile gauze and tubegauze. In the Kaltostat group, haemostasis was achieved by application of a dry Kaltostat dressing, which was then replaced with Kaltostat moistened with sterile normal saline and covered with a trimmed gauze swab and tubegauze.
A total of 70 patients was recruited to the study. Their ages ranged from 10 to 70 years, with a mean of 27 years, and approximately twice as many were male as female. Only 6 subjects (8.6%) were smokers. 5 subjects were taking medication for concurrent conditions and 2 females were taking oral contracep- tives and HRT respectively. 1 subject suffered from bronchitis but was not taking medication at the time of entry to the study.
An ischaemic index above 0.8 is generally regarded as indicating an adequate blood supply to the foot. 1 subject had an index of 0.79, but all others were above 0.8. 8 subjects (11.4%) required total nail avulsions.
Healing time was extremely variable, ranging from 7 to 70 days, and showed no correlation with age or ischaemic index. Concurrent disease and smoking occurred too infrequently to permit any effect upon
Review and redressing Table 2. Comparison of dressing treatment groups
Patients were reviewed on the day following surgery and then dressed weekly when the wound was assessed against defined criteria for healing (Table 1).
Kaltostat Melolin
A standardized redressing procedure was adopted to minimize variation between chiropodists. Dressings in both groups were soaked with sterile normal saline prior to removal, and the site swabbed with saline and blotted dry. Patients in the Melolin group had Melolin reapplied throughout the trial. In the
Number of patients 35 35 Mean age (years) 23.7 (SD 14) 29.8 (SD 17) Males : females 23: 11 20: 10 Sex not recorded 1 5 Non-smokers : smokers 3212 31:4 Smoking not recorded 1 0 Ischaemic index 1.08 (SD 0.12) 1.08 (SD 0.14) Partial nail avulsion 32 30 Total nail avulsion 3 5

90 The Foot
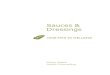
Number of patients 121
1 2 3 4 5 6 7 8 9 10
Dressing changes
@ MELOLIN - KALTOSTAT
Figure. Number of dressing changes to full healing.
healing rate to be determined. There were however, significant differences between dressing treatment groups (Figure).
The two groups of patients were similar for all the characteristics recorded (Table 2). Healing was 8.6 days less in the alginate-treated group (Table 3): this difference is statistically significant, P < 0.05. The number of dressing changes required was correspond- ingly approximately 1 fewer in this group: this was also significant (P-cO.05). When the groups were divided according to whether a total or partial avulsion was carried out, it was found that the difference between dressings was 22.7 days for total avulsions (P < 0.05) and 6.6 days for partial avulsions (P = 0.069). Differences between groups for patient comfort, pain on dressing removal and acceptability of the dressing were not significant.
At the initial postoperative dressing change, 4 patients treated with Kaltostat and 9 with Melolin had suffered postoperative bleeding (not statistically significant). Strike through of blood or exudate occurred in 4 of the Kaltostat-treated group and 15 of those treated with Melolin, a significant difference,
Table 3. Outcome of treatment
P < 0.05. In addition, 1 patient dressed with Kaltostat developed a wound infection which was treated with antibiotics, and the nail of 1 patient in the Melolin group appeared to be regrowing. All other patients healed without complications.
CONCLUSION
Healing after toenail avulsion was variable and none of the patient factors recorded was significantly correlated with healing time. Advanced age and a poor local blood supply (indicated by a low ischaemic index) are likely to retard healing, but this study did not produce extreme values of either variable to demonstrate a correlation.
The use of an alginate dressing which promotes moist wound healing, was shown to reduce signifi- cantly both time to healing and the number of dressing changes required. In patients requiring total nail avulsion, a reduction in healing time of 22.7 days was recorded in the alginate-treated group when compared to those treated with a dry dressing. For
All patients Kaltostat Melolin
Number of patients Days to healing Dressing changes
35 ::.8 (SD 12.9) 34.4 (SD 15.2) PiO.05
3.6 (SD 1.8) 4.5 (SD 2.2) P<O.O5
Total nail avulsions Number of patients Days to healing 2i.3 (SD 6.7)
5 43.0 (SD 16.9) P<O.O5
Partial nail avulsions Number of patients Mean days to healing
32 30 26.3 (SD 13.2) 32.9 (SD 14.8) P=O.O69

Comparison of Kaltostat and Melolin as postoperative dressings 91
partial avulsions, healing time was reduced by 6.6 days. Wounds remained moist longer when the alginate was used and this appeared to aid epithelializ- ation. These results demonstrate that moist Kaltostat and other modern wound dressings are more expens- ive than traditional dry dressings: the additional dressing cost was between &I .60 and E2.20 per patient in this study (3 or 4 alginate dressings per patient). The reduction in healing time however represents a saving of one or two clinic appointments.
Nail avulsion and phenolization are now widely accepted as the best treatment for recurring onychoc- ryptosis and onychogryphosis. Kaltostat offers con- siderable advantages both in terms of faster healing time and in reducing the number of dressings needed.
Acknowledgements
The authors are grateful to the staff of the Barnsley Community and Priority Services NHS Trust Department of Foot Health, to C. D. Blakemore PhD, for undertaking the statistical analysis and to BritCair Division of C V Laboratories Ltd for their support of this study.
References
1. Marr S J, Quine S. Prevalence and type of foot problems amongst workers wearing safety footwear. J Br Podiatr Med 1992; 47: 2399240.
2.
3.
4.
5.
6.
7.
Widdicombe M J. A comparative study of the public and private sectors in chiropodial care. Chiropodist 1990; 45: 97-194. Tanner A. Fail-safe approach to ingrowing toenails. Irish Doctor 1989: 15 Jan, 344-348. Sykes P A. Ingrowing toenails. Surgery 1988; 1: 1342-l 344. Beaton D F et al. Ingrowing toenails: a patient evaluation of phenolisation versus wedge excision. Chiropodist 1990; 45: 62-64. Thomas S. Functions of a wound dressing. In: Wound management and dressings. London: Pharmaceutical Press, 1990: 9911. Bruce G. Toenail avulsion study. J Tissue Viability 1991; I: 34435.
The authors
Gary B. Foley MBA, DPodM, MChS Locality Manager and Chiropody Adviser Barnsley Community and Priority Services NHS Trust Community Headquarters Mount Vernon Hospital Mount Vernon Road Bamsley S70 4DP UK Jean Allen BSc, PhD Clinical Research Associate C V Laboratories Limited Gordon House Gordon Road Aldershot GUI 1 1LD UK
Correspondence to G. B. Foley.