Embed Size (px)
Citation preview

Personal Relationships, (2011). Printed in the United States of America.Copyright © 2011 IARR; DOI: 10.1111/j.1475-6811.2010.01335.x
Worries in expectant parents: Its relation withperinatal well-being and relationship satisfaction
SUSANNE N. BIEHLE AND KRISTIN D. MICKELSON
Kent State University
AbstractAlthough much has been written about the impact of pregnancy on expectant parents, less is known about theworries couples experience during pregnancy. Sex differences in worries and the link between self and coparentworries on perinatal well-being and relationship satisfaction in 104 primiparous couples were examined. It was foundnot only do expectant mothers and fathers worry about different things, but also type of worry is related to differentoutcomes. Moreover, using structural equation modeling, childbirth worries and worry frequency indirectly predictlower relationship satisfaction through worse well-being. However, coparent’s worries did not significantly relate totheir partner’s perinatal well-being or relationship satisfaction. This study suggests the importance of examiningperinatal worries in parents, as well as the dyadic interaction between coparents.
Couples expecting their first child are typi-cally filled with excitement and anticipationabout the impending arrival of their baby(e.g., Feldman & Nash, 1984). Yet, becauseof the all the unknowns surrounding preg-nancy (especially with a first child), it can alsobe a stress-provoking time for both expec-tant mothers and fathers (e.g., Harville, Savitz,Dole, Herring, & Thorp, 2009; Hobbs &Cole, 1976). Expectant parents often worryabout various aspects of the transition andpregnancy from baby’s health, the child-birth process, money, and/or their copar-ent relationship (e.g., Ohman, Grunewald,& Waldenstrom, 2003; Petersen, Paulitsch,Guethlin, Gensichen, & Jahn, 2009). Althoughresearch has examined what expectant moth-ers (and to a lesser degree expectant fathers)worry about, it is less clear how worry dur-ing pregnancy impacts them individually and
Susanne N. Biehle and Kristin D. Mickelson, Departmentof Psychology, Kent State University.
This study was supported by a grant to K.D.M. fromthe Ohio Board of Regents.
Correspondence should be addressed to Susanne N.Biehle, Department of Psychology, Kent State Univer-sity, P.O. Box 5190, Kent, OH 44242-0001, e-mail:[email protected].
how their worries are related to their coparentand coparent relationship. Moreover, despitethe wealth of knowledge that has been gath-ered about the transition to parenthood in thelast few decades, relatively few studies havesystematically examined the combined per-spectives of the expectant mother, father, andcouple. In addition, no prior research existson the impact of a coparent’s worries on theirpartner’s well-being. This study proposes toexamine sex differences in the worries ofexpectant parent, as well as the differentialimpact of these worries on their well-beingand relationship satisfaction. In addition, thisstudy examines whether what one parent wor-ries about, as well as how much they worry,will be related to well-being and relationshipsatisfaction in their coparent.
Sex differences in worries
Worry is considered a normal aspect of dailylife associated with real-life triggers occurringpresently or expected to occur in the nearfuture (Tallis, Davey, & Capuzzo, 1994).Worry has alternately been defined in the liter-ature as the emotional distress or arousal con-nected with an actual or perceived situation
1

2 S. N. Biehle and K. D. Mickelson
or the recurrent thoughts associated with theevent (cf. Borkovec, Robinson, Pruzinsky, &DePree, 1983). Although some of the priorliterature has combined the concept of wor-ries with anxiety, we, and others, argue thatworry is different from anxiety. Specifically,worry is the cognitive aspect, whereas anxietyis the emotional signal of impending danger(Bruhn, 1990; Morris, Davis, & Hutchings,1981). In other words, worry consists of thethoughts about what may or may not occur,whereas anxiety is the feelings of nervous-ness, distress, or fear about those actual orpossible events. Although many may viewthe process of worrying as negative, it canbe an important step in dealing with per-ceived stressors as a form of inner prepa-ration used prior to coping with a situation(Affonso, Liu-Chiang, & Mayberry, 1999;Janis & Leventhal, 1965). For instance, if anexpectant mother is worried about the child-birth process she may be motivated to pre-pare a birth plan to help her cope with thedelivery experience when it occurs. Despitethese potential benefits of worry, excessiveworry has been shown to be detrimental toan individual’s well-being, including increas-ing anxiety and depression (e.g., Andrews &Borkovec, 1988; Nolen-Hoeksema, 1996).
With respect to sex differences in worry,research has consistently found women toworry more than men (e.g., McCann, Stewin,& Short, 1991; Robichaud, Dugas, & Conway,2003). Potential reasons for this sex differ-ence range from worry being considered afeminine trait (Stavosky & Borkovesc, 1988)to women holding lower status positions thatmay create more stress and worries (Gove,1980) to women internalizing their problems,which leads to more worrying (Rosenfield,2000). Despite all these potential explanationsfor sex differences, it is unclear if there arecertain situations where men worry as muchas or more than women. Wood, Conway,Pushkar, and Dugas (2005) found that indi-viduals perceive men as having more finan-cial and achievement worries and women ashaving more interpersonal worries. These per-ceptions of worries being differentiated by sexmirror stereotypes that men are more con-cerned with work and money, whereas women
are more concerned with their relationships.However, when Robichaud and colleagues(2003) studied actual reported worries in maleand female college students, they found no sexdifferences in the worry categories of money,workplace, relationships, or the future. Per-haps these results are dependent on the samplestudied; during college not only are sex dif-ferences fewer, but also college students arelikely more liberal and nontraditional in theirfuture expectations than the general popula-tion, potentially altering the pattern of worriesthat may be seen for these individuals (e.g.,Tavris & Wade, 1984). Thus, these contradic-tory findings make it unclear if sex differencesin worry type actually exist. During an eventwhere expectations are different for men andwomen, such as pregnancy, it may be rea-sonable to assume that men and women willworry about different aspects of the tran-sition to parenthood. For example, one ofthe most consistent findings during the tran-sition to parenthood is a decrease in rela-tionship satisfaction following the birth ofa couple’s first child (e.g., Belsky & Kelly,1994). Researchers have found that comparedto matched nonparent couples, parent couplesexperience more of a decline in relationshipsatisfaction from pregnancy through the firstyears after the birth of their baby (Lawrence,Rothman, Cobb, & Bradbury, 2008). More-over, women have been found to experiencegreater declines in relationship satisfactionthan men during the transition to parenthood(Belsky, Spanier, & Rovine, 1983). Thus,because of women’s greater attention to rela-tionships in general, women may have moreworries than men during pregnancy aboutpotential changes in the relationship once thebaby is born due to the new responsibilitiesand increased focus on the baby.
Worries during pregnancy
Although pregnancy has been found to bean anxiety-provoking time period for bothexpectant mothers and fathers (e.g., Entwisle& Doering, 1981), research on worries dur-ing pregnancy is scarce. The limited litera-ture examining worries during pregnancy hasfound the most frequent worry for expecting

Worries in expectant parents 3
women is their baby’s health and the deliv-ery (Ohman et al., 2003). However, as withthe majority of the parenting literature, menhave been understudied despite research sug-gesting that fathers play a critical parentingrole in a child’s life (e.g., Bogels & Phares,2008). Researchers have found that, for men,anxiety is highest during pregnancy and thendeclines after the birth of the baby, suggest-ing that increased anxiety for men may bea result of concerns about the transition toparenthood (Glazer, 1980). One study thatexamined expectant fathers found their mostcommon worry was being able to providefinancially for their family (Heinowitz, 1982).Two limitations of these prior studies are thatthey only sampled one sex in each study andare descriptive in nature. In other words, nosex differences were tested and they providean understanding of what expectant parentsworry about but not how the worries arerelated to one’s well-being. The first aim ofthis study was to examine if expectant moth-ers and fathers differ in the types of worriesthey report during pregnancy. Specifically,based on the literature reviewed above, wehypothesized that expectant fathers will reportmore security worries (e.g., financial and job),whereas expectant mothers will report morebaby-related (e.g., baby’s health, labor anddelivery, and preparing for the baby) and rela-tionship (e.g., with a coparent or family andfriends) worries. In addition, we hypothesizedthat the relation of worries to well-being andrelationship satisfaction will differ betweenexpectant mothers and fathers. Specifically,security worries will be more important forfathers, whereas baby and relationship worrieswill be most important for mothers.
Another limitation in prior research onpregnancy worries is the absence of the copar-ent—in other words, it is unclear how thecoparent’s worries might be associated withtheir partner’s well-being and relationship sat-isfaction. There are two ways in which acoparent’s worries may be linked with thepartner’s well-being. First, what a coparentworries about and how much the copar-ent worries may be negatively related to thepartner’s well-being and relationship satisfac-tion. For instance, if a coparent is worried
about the marital relationship (regardless ofwhether the partner is), the partner may reportless relationship satisfaction as the coparentmay be making his or her worries known.Moreover, the more a coparent is worried ingeneral about the pregnancy may be related tohigher distress in the partner through a conta-gion effect (e.g., Westman, 2001; Westman &Etzion, 1995). A second way in which copar-ent worries may be related to their partner’swell-being is whether the coparent’s worrymatches the partner’s worry or not. It may bebeneficial for both partners to have the sameconcerns so they can commiserate about theirfears, or it may be better if they have uniqueworries from their partner so they can eachfocus on different aspects of the transition toparenthood and comfort each other. However,as stated above, the literature is silent on therole of coparent worries. Therefore, the sec-ond aim of this study was to examine the roleof coparent worries on partner’s well-beingand relationship satisfaction. Specifically, wepropose that what a coparent worries about aswell as how much they worry will be neg-atively related to their partner’s well-beingand relationship satisfaction. However, due tothe lack of prior research on the topic, ouranalyses on coparent worries and matching ofworries will be exploratory.
Worries about the childbirth process
In addition to having general worries, one spe-cific worry for first-time parents is about theupcoming childbirth process. For new parents,this situation can be especially worrisomebecause it is an unknown, unpredictable eventwith potential complications during deliverythat could affect the health of the baby ormother. Additionally, some expectant parentsworry about the pain they (or their copar-ent) will encounter and the type of care theywill receive while in the hospital. The child-birth process also involves giving up control,which may be difficult for some individuals.Although a few researchers have examinedchildbirth worries, to our knowledge, theyhave only been assessed in expectant mothers.Lowe (2000) found that expectant motherswere worried most about (a) losing control

4 S. N. Biehle and K. D. Mickelson
during the delivery, (b) the birth experience,and (c) something being wrong with the baby.It seems reasonable to assume that expectantfathers will have similar worries related to thechildbirth process, albeit to a lesser degreethan the expectant mother who will actuallybe experiencing childbirth directly. Moreover,it is unclear if childbirth worry is related towell-being and relationship satisfaction overand above one’s general level of worry. Thethird aim of this study examines self andcoparent worries about childbirth, as well asthe frequency of worry. As seen in Figure 1,we hypothesize that both self and coparent’sreported childbirth worries and frequency ofworry will be linked to anxiety which will,in turn, be negatively related to well-being(defined in this study as positive affect anddepression). Finally, reduced well-being willbe associated with lower levels of relationshipsatisfaction. We will examine the proposedmodel separately for expectant mothers andfathers to determine whether it differs by sex.
Present study
To test the three aims proposed above, first-time expectant couples were interviewed dur-ing the third trimester of the pregnancy. Theprior literature focusing on the postpartumperiod is incomplete without an understandingof how perinatal well-being is related to issuesexperienced during the pregnancy. Study-ing the relationship of worries on perinatal
well-being is an important precursor to under-standing how to prevent postpartum dis-tress and relationship deterioration. In thisstudy, we specifically hypothesize that wor-ries will be related to perinatal anxiety,depression, positive affect, and relationshipsatisfaction. Although the literature on thetransition to parenthood has examined anxietyand depression in expecting and new parents,the literature on positive affect in parents isrelatively scarce. Researchers have found thatparents report less happiness than nonparents(Alesina, Tella, & MacCulloch, 2004); how-ever, little is known about how pregnancyis related to an expectant parent’s level ofreported happiness. Despite the lack of lit-erature on positive affect during pregnancy,the importance of positive affect is well estab-lished (e.g., Salovey, Rothman, Detweiler, &Steward, 2000). And, as with other emotions,women experience more positive affect thanmen (e.g., Larsen, Diener, & Emmons, 1986).Thus, we felt it was important to include thisaspect of well-being in this study.
Method
Participants
The sample was composed of 104 hetero-sexual married or cohabitating couples (208individuals) expecting their first child (i.e.,primiparous) and in their third trimesterof pregnancy. Other eligibility requirementsincluded that both the expectant mother and
++
_ +
+
_++
+
Self Childbirth
Worries
Self Worry
Frequency
Coparent Childbirth
Worries
Coparent Worry
Frequency
Anxiety
Positive Affect
Depression
Relationship Satisfaction
Figure 1. Proposed model for childbirth worries and worry frequency.
Worries in expectant parents 5
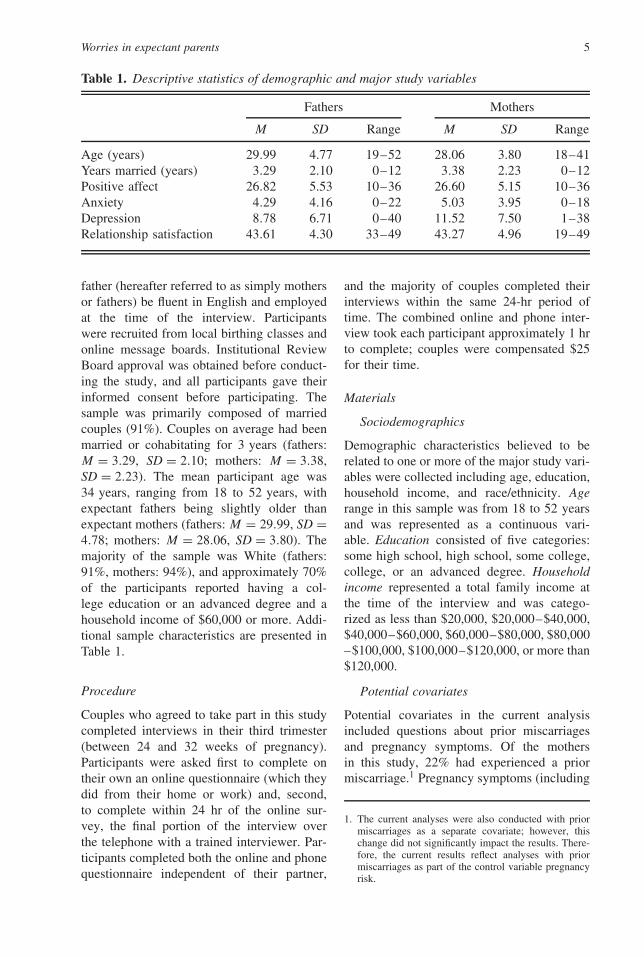
Table 1. Descriptive statistics of demographic and major study variables
Fathers Mothers
M SD Range M SD Range
Age (years) 29.99 4.77 19–52 28.06 3.80 18–41Years married (years) 3.29 2.10 0–12 3.38 2.23 0–12Positive affect 26.82 5.53 10–36 26.60 5.15 10–36Anxiety 4.29 4.16 0–22 5.03 3.95 0–18Depression 8.78 6.71 0–40 11.52 7.50 1–38Relationship satisfaction 43.61 4.30 33–49 43.27 4.96 19–49
father (hereafter referred to as simply mothersor fathers) be fluent in English and employedat the time of the interview. Participantswere recruited from local birthing classes andonline message boards. Institutional ReviewBoard approval was obtained before conduct-ing the study, and all participants gave theirinformed consent before participating. Thesample was primarily composed of marriedcouples (91%). Couples on average had beenmarried or cohabitating for 3 years (fathers:M = 3.29, SD = 2.10; mothers: M = 3.38,SD = 2.23). The mean participant age was34 years, ranging from 18 to 52 years, withexpectant fathers being slightly older thanexpectant mothers (fathers: M = 29.99, SD =4.78; mothers: M = 28.06, SD = 3.80). Themajority of the sample was White (fathers:91%, mothers: 94%), and approximately 70%of the participants reported having a col-lege education or an advanced degree and ahousehold income of $60,000 or more. Addi-tional sample characteristics are presented inTable 1.
Procedure
Couples who agreed to take part in this studycompleted interviews in their third trimester(between 24 and 32 weeks of pregnancy).Participants were asked first to complete ontheir own an online questionnaire (which theydid from their home or work) and, second,to complete within 24 hr of the online sur-vey, the final portion of the interview overthe telephone with a trained interviewer. Par-ticipants completed both the online and phonequestionnaire independent of their partner,
and the majority of couples completed theirinterviews within the same 24-hr period oftime. The combined online and phone inter-view took each participant approximately 1 hrto complete; couples were compensated $25for their time.
Materials
Sociodemographics
Demographic characteristics believed to berelated to one or more of the major study vari-ables were collected including age, education,household income, and race/ethnicity. Agerange in this sample was from 18 to 52 yearsand was represented as a continuous vari-able. Education consisted of five categories:some high school, high school, some college,college, or an advanced degree. Householdincome represented a total family income atthe time of the interview and was catego-rized as less than $20,000, $20,000–$40,000,$40,000–$60,000, $60,000–$80,000, $80,000–$100,000, $100,000–$120,000, or more than$120,000.
Potential covariates
Potential covariates in the current analysisincluded questions about prior miscarriagesand pregnancy symptoms. Of the mothersin this study, 22% had experienced a priormiscarriage.1 Pregnancy symptoms (including
1. The current analyses were also conducted with priormiscarriages as a separate covariate; however, thischange did not significantly impact the results. There-fore, the current results reflect analyses with priormiscarriages as part of the control variable pregnancyrisk.

6 S. N. Biehle and K. D. Mickelson
preeclampsia, bleeding, bed rest, and contrac-tions in the second trimester) were rated ona 4-point Likert scale from 1 (not at all ) to4 (a lot). For the current analyses, a con-trol variable of pregnancy risk was created bytaking the mean score of the four pregnancysymptoms and prior miscarriages, with highernumbers indicating more pregnancy risk.
Worries
Participants were asked to list their wor-ries (“What did you worry about [in thepast 6 months]? Please be as specific aspossible and list them in order of inten-sity”; adapted from the National ComorbiditySurvey; Kessler et al., 1994). The open-ended responses to this question were codedinto nine categories: transition to parenthood,money, baby’s health, mother’s health, rela-tionship with partner, family and friends, job,preparing for baby, and miscellaneous (thebreakdown of each of these categories canbe seen in Table 2). Because not all partic-ipants reported the same number of worries(with reported worries ranging from one tofour), for this study, we only examined the topworry for each expectant parent. Two raterscoded each of the open-ended responses, andinterrater reliability among the two raterswas high, α = .90. In other words, the twocoders agreed on 90% of the worry cod-ing. The remaining 10% disagreement wasthen resolved by a third rater. All the dis-agreements were satisfactorily resolved bythe coders. For analytic purposes, the orig-inal eight categories (minus the miscella-neous category) were further reduced to cre-ate three major categories of worry: (a) babyissues (baby’s health, mother’s health, tran-sition to parenting, and preparing for baby),(b) relationship issues (marriage and familyand friends), and (c) security issues (moneyand job).
Worry frequency
To assess the degree to which participantsworried in general during pregnancy, theywere asked the following question: “Peoplediffer a lot in how much they worry. Con-sidering how things have been going in your
Table 2. Breakdown of worry coding
Baby’s health Baby’s health, problemsduring delivery, pregnancyconcerns
Family andfriends
Relationship with family,relationship with friends
Job Balancing work and baby,job or school stress
Transition toparenthood
Uncertainty about future,coping with baby’s needs,being a good mom or dad,transition to having a baby,meeting demands ofparenthood, bonding withbaby
Relationship Relationship with spouse orpartner
Money Money and childcare issues
Mother’shealth
Mother’s health, labor andchildbirth anxiety, beingpresent during delivery
life over the PAST 6 MONTHS, how muchdid you worry as compared to other peo-ple expecting their first child?” with potentialresponses of 1 (a lot less than other expec-tant parents) to 4 (about the same) to 7 (alot more than other expectant parents). Therewas no significant correlation between worryfrequency and the number of actual worriesthe participant’s reported for the total sam-ple; however, when examined separately bysex we found that number of worries was sig-nificantly correlated with worry frequency forwomen, r(102) = .23, p < .05, but not men,r(102) = .14, p = .16.
Worries about childbirth
To examine worries about the childbirth pro-cess, participants responded to the follow-ing seven items adapted from the ChildbirthAttitudes Questionnaire (Areskog, Kjessler, &Uddenberg, 1982): (a) “I fear losing control ofmyself (or feeling helpless) at the delivery,”(b) “I fear something being wrong with thebaby,” (c) “I fear needing to have a Cesareansection,” (d) “I fear being torn during the birth

Worries in expectant parents 7
of the baby,” (e) “I fear painful labor contrac-tions,” (f) “I fear not getting the kind of carethat I want,” and (g) “I have overall anxietyabout childbirth.” Potential responses rangedfrom 0 (never had that fear) to 3 (it wor-ries you a lot). For the last three items, “mywife” was inserted after “I fear” for expectantfathers (e.g., “I fear my wife having painfullabor contractions”). A mean score was cre-ated from the responses (fathers: α = .72,mothers: α = .68), with higher scores indicat-ing greater levels of childbirth worries.
Anxiety
Participants’ anxiety was assessed throughself-report questions from the SymptomChecklist–90R (Derogatis, 1994). Participantswere asked to report how they felt in thelast week in regards to 10 different items(e.g., “felt nervous,” “felt so restless youcould not sit still”). Possible responses rangedfrom most (5–7 days) = 3, moderate (3–4days) = 2, a little (1–2 days) = 1, or none/rarely (< 1 day) = 0 that week. A sum scorewas created from the responses (fathers: α =.83, mothers: α = .77), with higher scoresindicating higher levels of anxiety.
Depression
To assess depressive symptomatology, theCenter for Epidemiologic Studies DepressionScale (CES–D; Radloff, 1977) was used. Par-ticipants were asked to report how they hadfelt in the past week in regards to 20 dif-ferent items (e.g., “felt sad,” “felt lonely”).Possible responses ranged from none/rarely( < 1 day) = 0, a little (1–2 days) = 1, mod-erate (3–4 days) = 2, or most (5–7 days) =3. A sum score was created from the responses(fathers: α = .87, mothers: α = .88), withhigher scores indicating higher levels ofdepression.
Positive affect
Participants were asked to report how theyhad felt in the last week in regards to feelingsix different positive emotions (e.g., “happy,”“cheerful”), which was adapted from the Pro-file of Mood States (McNair, Lorr, & Drop-pleman, 1981). Potential responses ranged
from 0 (not at all ) to 6 (daily). A sum scorewas created from the responses (fathers: α =.83, mothers: α = .85), with higher scoresindicating higher levels of positive affect.
Relationship satisfaction
The Relationship Assessment Scale (Hendrick,1988) was used to determine relationship sat-isfaction (e.g., “How well does your part-ner meet your needs?” “How good is yourrelationship to most other couples?”). Themeasure consisted of seven questions withpotential responses ranging from 1 (never) to7 (very often). Two questions were reversecoded, and a sum score of the seven items wascreated (fathers: α = .77, mothers: α = .81),with higher scores indicating greater relation-ship satisfaction.
Results
With respect to the major study variables, thesample was not highly distressed as partici-pants reported only moderate levels of anxi-ety (M = 4.66) and depression (M = 10.15).Traditionally, a score of 16 or higher on theCES–D has been used as a marker for indi-viduals who may suffer from a clinical levelof depression (see McDowell, 2006, for areview). Based on the analysis of variance(ANOVA), analyses, mothers were found tohave significantly higher levels of depres-sion than fathers, F (1, 206) = 7.71, p < .01,but similar levels of anxiety, positive affect,and relationship satisfaction (see Table 3 forstudy variables, means, standard deviations,and ranges).
Sex differences in worry type and relationshipon well-being
We first examined the prevalence of varioustypes of worries during pregnancy to deter-mine if they differed by sex. As shown inTable 3, when examining the three major cat-egories of worries, expectant mothers weremore likely to report baby and relationshipworries, whereas expectant fathers were morelikely to report security worries. When furtherexamining the worries that constitute each of

8 S. N. Biehle and K. D. Mickelson
Table 3. Breakdown of worries by type
Fathers Mothers χ2
Baby worries 51.9%b 67.3%a 5.54∗Baby’s health 26.9%b 43.3%a 6.37∗Preparation for baby 10.6%a 9.6%a 0.04Mother’s health 9.6%a 7.7%a 0.22Transition 4.8%a 6.7%a 0.38
Security worries 45.2%a 26.0%b 8.12∗Money 30.8%a 23.1%a 1.46Job and work and home balance 14.4%a 2.9%b 8.64∗∗
Relationship worries 1%a 4.8%a 2.79†
Marriage 1.0%a 2.9%a 1.04Family and friends 0%a 1.9%a 2.04
Miscellaneous (e.g., transportation) 1.9%a 1.0%a 1.33
Note. Different subscripts indicate that fathers and mothers significantly differed in worry type at p < .05. Numbersin bold add to 100% in each column, and numbers that are not in bold also add to 100% and represent the breakdownwithin each category of worries.†p < .10. ∗p ≤ .05. ∗∗p ≤ .01.
the three major categories, mothers’ top worryunder the category of baby concerned thebaby’s health and their top worry under thecategory of relationship concerned the mar-riage and relationship, while fathers worriedmost about issues involving money under thecategory of security.
We next examined the relation of worrytype (i.e., baby, security, relationship) on anindividual’s anxiety, depression, and posi-tive affect. Multivariate analysis of covari-ance (MANCOVA) analyses were conductedseparately for mothers and fathers. Note thatfor fathers, we deleted the category of rela-tionship worry as only one father reportedit as a top worry. For each model, preg-nancy risk was entered as a control variable.For fathers, the multivariate test was signif-icant for worry type, F (3, 96) = 3.29, p <
.05, η2 = .09. Specifically, fathers who wor-ried about security issues reported higherlevels of anxiety than fathers who worriedabout baby issues (security worries: M =5.60, SD = 4.97; baby worries: M = 3.22,SD = 3.04; p < .01, η2 = .08). No differ-ences were found for worry type on depres-sion or positive affect for fathers. For mothers,the multivariate test was also significant forworry type, F (6, 190) = 2.41, p < .05, η2 =
.07. Specifically, mothers who worried abouttheir relationships had significantly higherlevels of depression than mothers who wor-ried about baby issues (relationship worries:M = 20.17, SD = 16.80; baby worries: M =11.05, SD = 7.02; p < .05, η2 = .07). Nodifferences were found for worry type on anx-iety or positive affect for mothers.
Influence of coparent worries on partner’swell-being and relationship satisfaction
For the second aim, we examined the roleof coparent’s worries on partner’s well-beingand relationship satisfaction using theMANCOVA analyses described above butwith coparent worry type as the main factorof interest. None of the results w found to bestatistically significant; in other words, whatone’s coparent worried about was not relatedto their partner’s anxiety, depression, positiveaffect, or relationship satisfaction. Next, weexamined whether matching of partners ontheir primary worry was related to one’s well-being and relationship satisfaction. To explorethis idea, we first created a dichotomous vari-able of matching versus mismatching for thetop worry. Specifically, if expectant mothersand fathers both reported baby or relationship
Worries in expectant parents 9
or security as their top worry, they were codedas matching (0), but if coparents reported dif-ferent top worries (e.g., the mother reportedrelationship worries and the father reportedsecurity worries) they were coded as mis-matching (1). MANCOVA analyses were con-ducted separately for expectant mothers andfathers for the four possible outcomes (anxi-ety, depression, positive affect, and relation-ship satisfaction). None of the multivariatetests were significant. However, for fathers,there was one marginally significant find-ing for positive affect, such that fathers whomismatched with their coparent on the typeof worry reported marginally higher levelsof positive affect than fathers who matchedwith their coparent on the top worry (mis-match: M = 27.88, SD = 5.70; match: M =25.83, SD = 5.25; p = .058, η2 = .04). Asimilar but not significant trend was foundfor father’s depression and relationship sat-isfaction. Expectant mothers showed no dif-ferences on the outcome variables basedon matching with their coparent on worrytype.
Childbirth worry and worry frequency
The third aim of this study was to exam-ine childbirth worries and worry frequency.Results indicated that expectant mothers re-ported both more childbirth worry (moth-ers: M = 1.35, SD = .47; fathers: M = 1.13,SD = .50) and more worry frequency thanfathers (mothers: M = 4.12, SD = 1.65;fathers: M = 3.74, SD = 1.51). Next, we
examined the roles of anxiety, positiveaffect, and depression in the link betweenchildbirth worry and worry frequency on rela-tionship satisfaction. Specifically, we pro-posed that both self and coparent childbirthworry and worry frequency would be relatedto greater perinatal anxiety, which, in turn,would be related to higher depression andlower positive affect, both of which wouldbe negatively related to relationship satisfac-tion during pregnancy. On a more exploratorylevel, we investigated whether this proposedmodel worked similarly for mothers andfathers.
To test the model proposed in Figure 1,structural equation modeling (SEM) was uti-lized (EQS 6.1; Bentler, 2006). SEM allowsfor the testing of all components of themediational model simultaneously while alsomodeling measurement error. Preliminary ex-amination of the data revealed that all theassumptions of linear regression and SEM(e.g., linearity, random residuals, multivari-ate normality) were met with the currentdata set. Examination of the bivariate corre-lation matrix also did not reveal any prob-lems with multicollinearity (Table 4). Prior toconducting SEM, preliminary analyses wereconducted to identify potential variables thatshould be included as covariates. Based onthe results of these analyses, age, education,and pregnancy risk were initially entered intothe models as free-to-float variables. Separatemodels were tested for expectant mothers andfathers given that coparent scores were a partof each model.
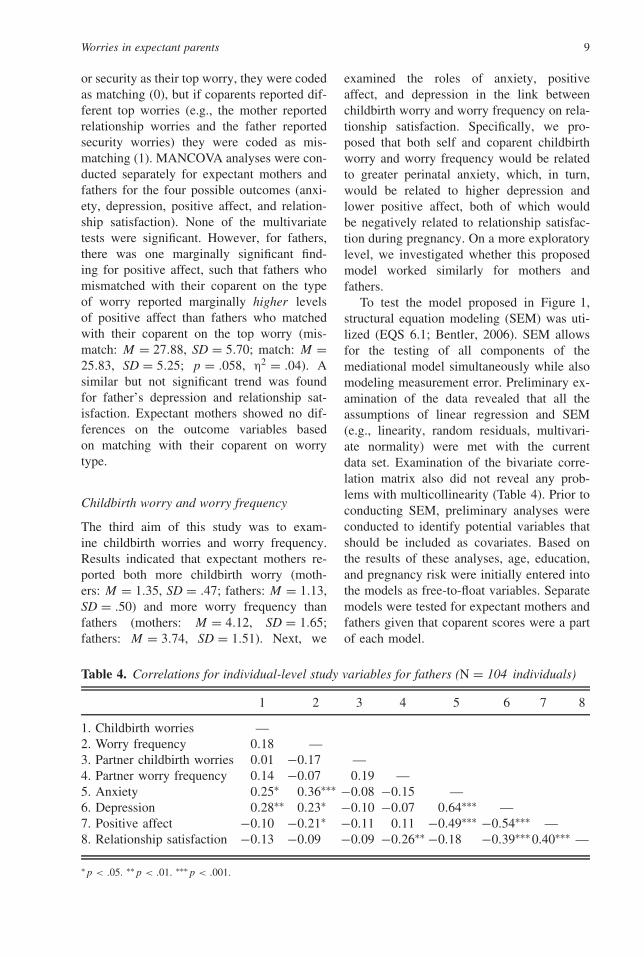
Table 4. Correlations for individual-level study variables for fathers (N = 104 individuals)
1 2 3 4 5 6 7 8
1. Childbirth worries —2. Worry frequency 0.18 —3. Partner childbirth worries 0.01 −0.17 —4. Partner worry frequency 0.14 −0.07 0.19 —5. Anxiety 0.25∗ 0.36∗∗∗ −0.08 −0.15 —6. Depression 0.28∗∗ 0.23∗ −0.10 −0.07 0.64∗∗∗ —7. Positive affect −0.10 −0.21∗ −0.11 0.11 −0.49∗∗∗ −0.54∗∗∗ —8. Relationship satisfaction −0.13 −0.09 −0.09 −0.26∗∗ −0.18 −0.39∗∗∗ 0.40∗∗∗ —
∗p < .05. ∗∗p < .01. ∗∗∗p < .001.

10 S. N. Biehle and K. D. Mickelson
Table 5. Correlations for individual-level study variables for mothers (N = 104 individuals)
1 2 3 4 5 6 7 8
1. Childbirth worries —2. Worry frequency 0.19 —3. Partner childbirth worries 0.01 0.14 —4. Partner worry frequency −0.17 −0.07 0.18 —5. Anxiety 0.32∗∗ 0.42∗∗∗ 0.07 −0.23∗ —6. Depression 0.23∗ 0.44∗∗∗ 0.05 −0.23∗ 0.61∗∗∗ —7. Positive affect −0.19 −0.39∗∗∗ −0.04 0.09 −0.37∗∗∗ −0.62∗∗∗ —8. Relationship satisfaction −0.08 −0.31∗∗ −0.07 0.12 −0.07 −0.36∗∗∗ 0.29∗∗
∗p < .05. ∗∗p < .01. ∗∗∗p < .001.
Expectant mothers’ model
To test the model on expectant mothers, thedata were analyzed using a structural pathmodel. The maximum likelihood (ML) esti-mation method was used for the current modelas there was no violation of the multivari-ate normality assumption. Bentler (2006) sug-gests that an N :q ratio between 5:1 and 10:1(where N equals the sample size and q equalsthe number of free parameters to be esti-mated) provides sufficient power. The N :qis a good measure of power because it fac-tors the complexity of the model, instead ofsimply considering the number of variablesin the model (Jackson, 2003). The presentsample represents an N :q of 6:1, suggestingadequate power to test the proposed structuralpath model.
The participant’s age, education level, andpregnancy risk were initially put in as exoge-nous free-to-float variables. In the mothers’model, paths were retained for (a) age withrelationship satisfaction, (b) age with edu-cation, (c) education with childbirth worry,and (d) pregnancy risk with worry frequency.Including these variables in the current modelensured that any initial inequalities with par-ticipants would be accounted for by themodel, which allowed for the assessment ofthe unique associations of the main variablesin this study. Although the above paths wereretained in the final model, for ease of presen-tation, they are not shown in Figure 2. In addi-tion, we correlated the error terms betweenpositive affect and depression, as we assumedthat the error in self-report of both wouldbe related. Additionally, the model with the
covariate paths was properly overidentified,with 66 known parameters to 24 unknownparameters.
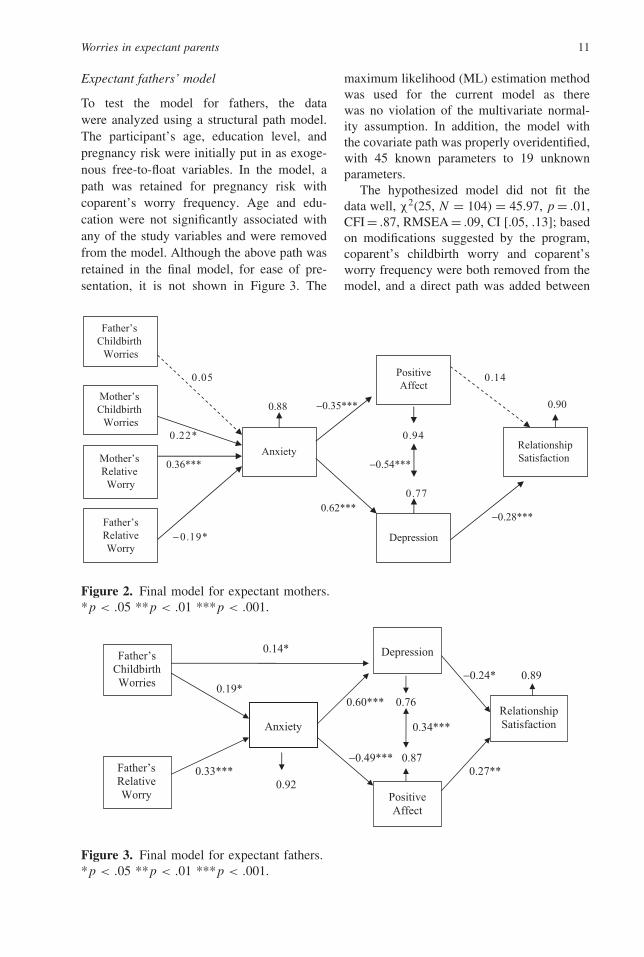
The hypothesized model fit the data well,χ2(41, N = 104) = 57.96, p = .04, compar-ative fit index (CFI) = .91, root mean squareerror of approximation (RMSEA) = .06, CI[.01, .10]. The fit indices demonstrate thismodel to be a good fit of the data because thepvalue for the chi square is marginally sig-nificant, the CFI is above .90, the RMSEA isbelow .08, and the confidence interval lowestnumber is close to 0 and the highest numberis close to 0.10. However, two modificationswere suggested by the program: (a) removalof the path between positive affect and rela-tionship satisfaction and (b) removal of thepath between coparent’s childbirth worry andanxiety. Making these modifications did notsignificantly improve the fit of the model,�χ2 (2, N = 104) = 1.57, p > .05; thus, theywere retained even though the individualpaths were not significant. The model suggeststhat mothers who reported more childbirthworry and greater worry frequency had higheranxiety level, which was, in turn, relatedto less positive affect and more depression,and higher reported depression was relatedto lower relationship satisfaction. A test ofthe indirect associations on relationship sat-isfaction was significant for both childbirthworry (b = −.75, SE = .33, t = −2.25, p <
.05) and worry frequency (b = .26, SE = .10,t = −2.76, p < .05). Finally, one surprisingresult was that husband’s worry frequencywas related to lower levels of anxiety formothers (Table 5).
Worries in expectant parents 11
Expectant fathers’ model
To test the model for fathers, the datawere analyzed using a structural path model.The participant’s age, education level, andpregnancy risk were initially put in as exoge-nous free-to-float variables. In the model, apath was retained for pregnancy risk withcoparent’s worry frequency. Age and edu-cation were not significantly associated withany of the study variables and were removedfrom the model. Although the above path wasretained in the final model, for ease of pre-sentation, it is not shown in Figure 3. The
maximum likelihood (ML) estimation methodwas used for the current model as therewas no violation of the multivariate normal-ity assumption. In addition, the model withthe covariate path was properly overidentified,with 45 known parameters to 19 unknownparameters.
The hypothesized model did not fit thedata well, χ2(25, N = 104) = 45.97, p = .01,CFI = .87, RMSEA = .09, CI [.05, .13]; basedon modifications suggested by the program,coparent’s childbirth worry and coparent’sworry frequency were both removed from themodel, and a direct path was added between
41.050.0
0.88
49.0*22.0
0.36*** −0.54***
77.00.62***
−0.28***
*91.0−
Mother’s Childbirth
Worries
Mother’s Relative Worry
Father’sRelativeWorry
Anxiety
PositiveAffect
Depression
RelationshipSatisfaction
Father’s Childbirth
Worries
0.90−0.35***
Figure 2. Final model for expectant mothers.*p < .05 **p < .01 ***p < .001.
*41.0
−0.24* 0.19* 0.60*** 0.76
***43.0
−0.49*** 0.87 **72.0***33.0
29.0
Father’sChildbirthWorries
Father’sRelative Worry
Anxiety
PositiveAffect
Depression
Relationship Satisfaction
0.89
Figure 3. Final model for expectant fathers.*p < .05 **p < .01 ***p < .001.

12 S. N. Biehle and K. D. Mickelson
father’s childbirth worries and depression. Asshown in Figure 2, the modified model was agood fit to the data, χ2(7, N = 104) = 6.92,p = .44, CFI = 1.00, RMSEA = .00, CI [.00,.12]; furthermore, examination of the modelrevealed that all the individual pathways weresignificant at p < .05. As the initial and mod-ified models were not nested, the Akaikeinformation criterion (AIC) values were com-pared, with the lowest value suggesting thatthe modified model was the better fitting ofthe two models (AIC initial model = −4.03;AIC modified model = −7.08). The modi-fied model suggests that expectant fathers’childbirth worry and worry frequency wereboth related to more anxiety, which was, inturn, related to less positive affect and moredepression, and subsequently less relationshipsatisfaction. A test of the indirect associa-tion on relationship satisfaction was signifi-cant for worry frequency (b = .23, SE = .09,t = −2.65, p < .05). In addition, a directlink was found with expectant fathers’ child-birth worries being related to more depression(Table 6).
Discussion
Every first-time expectant parent will tell youthat pregnancy is a time filled with excitementand worry. Although worry is a natural part ofthe experience, the literature provides us withlittle more than what expectant parents worryabout. In addition, of the sparse literature thathas been conducted on worries, the focus has
primarily been on the expectant mother. Thisstudy is unique in the examination of worriesduring pregnancy in both mothers and fathers,and the potential implications that worriescan have for the well-being and relationshipsatisfaction of soon-to-be parents. We foundthat overall mothers worried more aboutrelationship and baby issues, whereas fathersworried more about security issues. Type ofworry was also found to be an important pre-dictor of well-being for both expectant moth-ers and fathers. However, what a partner wor-ries about was not found to be related to anyof the coparent’s outcomes. Surprisingly, onlyone marginal result emerged for mismatchof worries between partners. Finally, expec-tant parents’ childbirth worries and worryfrequency were also examined. As expected,mothers were found to worry more aboutchildbirth issues and reported greater worryfrequency than fathers. However, childbirthworries and worry frequency were found tobe important for both expectant mothers’ andfathers’ well-being and relationship satisfac-tion. We discuss the implications and futuredirections of the main study findings below.
Sex differences in worries
In support of the first hypothesis regarding sexdifferences in pregnancy worries, we foundthat mothers and fathers worry about differentthings, although the majority of both moth-ers and fathers reported worrying about thebaby as their top worry. Expectant mothers
Table 6. Correlations for individual-level study variables for fathers and mothers (N = 208individuals)
Expectant fathers
Expectant mothersChildbirth
worriesWorry
frequency Anxiety DepressionPositiveaffect
Relationshipsatisfaction
Childbirth worries 0.01 −0.17 −0.08 −0.10 −0.11 −0.10Worry frequency 0.14 −0.07 −0.15 −0.07 0.11 −0.26∗∗Anxiety 0.07 −0.23∗ 0.06 0.05 −0.09 −0.16Depression 0.05 −0.23∗ −0.07 0.05 −0.02 −0.22∗Positive affect −0.04 0.09 0.09 −0.03 0.06 0.21∗Relationship satisfaction −0.07 0.12 −0.09 −0.05 0.10 0.38∗∗∗
∗p < .05. ∗∗p < .01. ∗∗∗p < .001.

Worries in expectant parents 13
were found to worry more about their baby’shealth, whereas fathers worried more aboutthe financial implications of having a baby. Asthis study demonstrates, pregnancy is a periodof time that is still experienced differentlyby expectant mothers and fathers. They havetheir own unique concerns about the impend-ing arrival of the new baby, despite the emerg-ing view of pregnancy and parenthood as anevent that couples experience together. Forexpectant fathers, pregnancy may highlightthe need to become more responsible, espe-cially financially, for their expanding family.For expectant mothers, pregnancy may high-light potential changes in the marital relation-ship as they transition to parenthood and herfocus shifts to caring for the baby. More-over, where the prior literature has primarilybeen descriptive with reports of what expec-tant mothers (and less often fathers) are wor-ried about, this study found that mothers andfathers were differentially impacted by theirworries. As hypothesized, fathers who wor-ried about security issues had higher anxietythan fathers who worried about baby issues,and mothers who worried about relationshipissues reported more depression and lowerpositive affect than mothers who worriedabout baby or security issues. This study isthe first to examine both worry type in expect-ing couples and its association with perinatalwell-being.
Taken together, these sex differences inpregnancy worry are consistent with gen-der stereotypes about men being focused onachievement and finances, whereas womenare focused more on relationships (e.g.,Broverman, Vogel, Broverman, Clarkson, &Rosenkrantz, 1972). These results also expandthe literature on worries during pregnancy bysuggesting that it is not only important howmuch you worry but also what you worryabout that is linked to your perinatal well-being. One reason this result is important isthat well-being during pregnancy has beenfound to be a precursor to postpartum well-being in both mothers and fathers (Green,1998; Morse, Buist, & Durkin, 2000; O’Hara,Schlechte, Lewis, & Varner, 1991). Thus, animportant future direction will be to examine
the longitudinal impact of pregnancy wor-ries and perinatal well-being on postpartumdistress.
Relationship of spousal worries
Our study is the first, to our knowledge,to investigate the relationship of coparent’sworries on their partners. Contrary to ourhypothesis, however, there was a lack offindings for coparent’s worry—there was norelation between coparent’s worry type andpartner’s well-being or relationship satisfac-tion, and only one marginal finding for mis-match between partners on worry type andwell-being. Specifically, we found that fathersreported marginally more positive affect whenthey mismatched with their wife on worrytype. Does this relative lack of results sug-gest that coparent worries play no role in apartner’s well-being? We think not; rather,we believe that coparent worry may play agreater role in partner well-being postpartum.After the baby is born, it may be more impor-tant for parents to “be on the same page” interms of what their focus is—parenting thebaby. However, due to the lack of literatureinvestigating this aspect of the transition toparenthood, little is known about postpartumworries in fathers and mothers. Future studiesneed to examine the potential implications ofcoparent worries in the postpartum period.
Childbirth worries and worry frequency
In addition to overall pregnancy worries,this examined the role of childbirth worriesand worry frequency. As predicted, expectantmothers reported more worries about thechildbirth process and higher levels of worryfrequency than fathers. However, throughSEM, we found that the overall modelswere similar for both expectant mothers andfathers. Specifically, as individuals worrymore about childbirth their anxiety increases,their well-being decreases, and, as a conse-quence, fathers and mothers report less satis-faction with their coparent relationship. Theonly major difference in the two models isthat coparent’s worry frequency was relatedto less anxiety for mothers—whereas neither

14 S. N. Biehle and K. D. Mickelson
coparent childbirth worry nor coparent’s worryfrequency was related to any of the outcomesfor fathers. The prior literature provides littleexplanation for why expectant mothers mayhave less anxiety if they have fathers who feelas though they worry more frequently thanother expectant parents. One potential expla-nation may be that as fathers worry more,they are taking on more of the responsibili-ties and are more involved during pregnancy,which allows their wives to have lower levelsof anxiety as they realize they are not alone.Additional studies are needed to explore thisrelationship more in-depth across the transi-tion to parenthood.
Limitations and future directions
Several caveats of this study should beaddressed. One potential concern is the oper-ationalization of worry solely in terms of thecognitive process and separating out the emo-tional process of anxiety as an intermediatemechanism. Some may argue that worry andanxiety should be combined. However, asbivariate correlations in this study revealed,worry frequency and childbirth worry wereonly moderately correlated with anxiety. Thus,in concurrence with other researchers (e.g.,Affonso et al., 1999; Bruhn, 1990), we believethat worry and anxiety are separate, distinctconstructs. Another potential limitation of thisstudy is the possible confounding of well-being in women during pregnancy. It maybe that expectant mothers were experiencingheightened anxiety or depression because ofthe hormones associated with pregnancy—inother words, pregnant women may be morereactive to worries during pregnancy becauseof the hormonal changes they are experienc-ing. However, as recent studies have shownless support for the importance of hormonesas influential predictors of postpartum depres-sion (e.g., Righetti-Veltema, Conne-Perreard,Bousquet, & Manzano, 1998), one can assumethat the women’s well-being cannot be com-pletely explained by hormonal changes. Apotential strength of this study, in fact, is theexamination of multiple dimensions of well-being: depression, anxiety, and positive affect.The dimension of positive affect has been
especially neglected in the literature on thetransition to parenthood and worries. Positiveaffect is an important aspect of an individ-ual’s well-being such that positive emotionscan broaden an individual’s range of cop-ing strategies, which is important to expec-tant parents preparing for a stressor such asthe transition to parenthood (e.g., Aspinwall,2001). Therefore, it is important to understandpotential factors that could impact positiveaffect during pregnancy in soon-to-be mothersand fathers.
A third limitation is the cross-sectionalnature of the study design. As a result, causalrelationships between the predictors and out-comes cannot be determined and the structuralpath models need to be replicated with lon-gitudinal data. It is possible that problemsin a marriage could lead to marital worriesor that worries could lead to marital prob-lems. However, given the constraints of thisstudy, the temporal nature of these relation-ships is unclear. Although this study was oneof the first to examine the perinatal impli-cations worries during pregnancy have onmothers and fathers, additional research isneeded to expand this work. Because thisstudy only examined worries during the preg-nancy period, it would be beneficial forfuture studies to investigate how the pro-cess of worrying changes across the transitionto parenthood. For example, we found thatexpectant mothers worried about the baby’shealth, but expectant fathers’ top worry con-cerned money. After a couple’s baby is born,little is known about how worries affect thecouple. It may be that worries become moredifferentiated between fathers and mothers asthey encounter different experiences in parent-ing, or they may become more similar as theyare both dealing with the needs of the baby. Inaddition, during pregnancy a majority of theworries that parents are concerned with areabout potential unknowns that could happenwith the baby, delivery, or with adjustmentto parenthood. However, after the baby isborn, less of the worries that parents are con-fronted with are about unknown possibilitiesand more about real concerns they are facing.Therefore, it is possible that due to the natureof worries during pregnancy compared to the

Worries in expectant parents 15
postpartum period, the impact of worries onparent’s well-being could play out differently.A final limitation concerns the nature of thesample used. Because the study consisted pri-marily of White, middle-class couples experi-encing their first pregnancy, it is unclear howmuch these results would generalize to othercouples. It may be that middle-class coupleshave more resources to deal with the transitionthan those with lower incomes or educationand therefore may experience fewer worriesor worries of a different nature than otherdemographics. Therefore, additional studiesare needed to examine the impact of socialcontext on worries during pregnancy.
In addition, although there is much litera-ture on the transition to parenthood and post-partum depression, it is unclear if worryingduring pregnancy or in the postpartum periodcould lead to more postpartum distress. How-ever, one recent study has found that peri-natal levels of distress in both mothers andfathers were predictive of postpartum distress(Morse, Buist, & Durkin, 2000). Despite thefact that the literature suggests worrying canbe beneficial because of the potential to evokecoping responses, it may be that worryingabout things out of your control could lead toworse outcomes. It is also unclear how dis-cussion of worries within the couple couldrelate to marital satisfaction. Perhaps knowl-edge about a partner’s worries (albeit differentfrom one’s own worries) could be an indicatorof communication between the partners, andbeing able to comfort a partner who is wor-ried about an issue could represent a specifictype of spousal support that is importantduring stressful situations. Further expansionin the examination of coparent worries isneeded. One potentially interesting futuredirection would be to examine the coparent’sperspective of what (and how much) theybelieve their partner worries about to deter-mine whether they are aware of their part-ner’s worries. Relatedly, it would be fruitfulto examine the impact of one coparent’s men-tal health on their partner’s well-being—as itmay be that the topic of a coparent’s worriesis less important than how much distress theyexperience from their worrying. Finally, in thefuture it will be useful to examine what role,
if any, is played by agreement versus dis-agreement on worries. In other words, does itmatter if partners worry about the same thingsor different things? As our study and theseideas for future research suggests, more sys-tematic dyadic research is needed on the roleof coparent effects.
Another important aspect of future researchon worries would be to examine worries in amore systematic way. For example, it wouldbe helpful to have more specific informationfrom participants about their worries. Insteadof only getting a list of the participant’s topworries, it might be beneficial to have infor-mation about the amount of worry on differenttypes of issues and how much of a threat theyperceive each type of worry to be. In addition,it would also be helpful to have participantsrate how much control they felt they had overeach type of worry. For example, a partici-pant who is worried about their baby’s healthmay feel that it is completely out of their con-trol, but an expectant parent who is worriedabout preparing for the baby may feel thatis a situation that is under their control. Per-ceived controllability of worries may help toclarify which types of worries could be detri-mental to the mental health of an expectantparent.
Conclusion
This study is the first, to our knowledge,that has systematically examined the role ofpregnancy worries on well-being and relation-ship satisfaction in both expectant mothersand fathers. Although there is an abundantliterature on the transition to parenthood, amajority of the studies have focused primarilyon the postpartum period with less attentionon perinatal well-being and relationship sat-isfaction. Therefore, this study adds to theliterature by examining the potential factorsthat could be related to first-time parents dur-ing the pregnancy period. We found that whileboth personal worries and childbirth wor-ries were important, coparent’s worries didnot play a major role in their partner’s peri-natal well-being or relationship satisfaction.Furthermore, our models suggest that thecognitive aspect of worry is related to the
16 S. N. Biehle and K. D. Mickelson
emotional response, which in turn is relatedto relationships. These findings support andextend the prior literature that suggests thatpersonal well-being, specifically depressionand anxiety, can be related to relationshipsatisfaction (e.g., Whisman, Uebelacker, &Weinstock, 2004). The next step is to deter-mine if these processes carry over to the post-partum period of the transition to parenthood.
References
Affonso, D. D., Liu-Chiang, C. Y., & Mayberry, L. J.(1999) Worry: Conceptual dimensions and relevanceto childbearing women. Health Care for Women Inter-national, 20, 227–236.
Alesina, A., Tella, R. D., & MacCulloch, R. (2004). In-equality and happiness: Are Europeans and Americansdifferent? Journal of Public Economics, 88,2009–2042.
Andrews, V. H., & Borkovec, T. D. (1988). The differ-ential effects of induction of worry, somatic anxiety,and depression on emotional experience. Journal ofBehavior Therapy and Experimental Psychiatry, 19,21–26.
Areskog, B., Kjessler, B., & Uddenberg, N. (1982). Iden-tification of women with significant fear of childbirthduring pregnancy. Gynecologic and Obstetric Investi-gation, 13, 98–107.
Aspinwall, L. G. (2001). Dealing with adversity: Self-regulation, coping, adaptation, and health. In A.Tesser & N. Schwarz (Eds.), Blackwell handbookof social psychology: Intraindividual processes (pp.591–614). Malden, MA: Blackwell.
Belsky, J., & Kelly, J. (1994). The transition to parent-hood: How a first child changes a marriage why somecouples grow closer and others apart. New York:Dell.
Belsky, J., Spanier, G., & Rovine, M. (1983). Stabilityand change in a marriage across the transition toparenthood. Journal of Marriage and the Family, 45,567–577.
Bentler, P. M. (2006). EQS 6 structural equations pro-gram manual. Encino, CA: Multivariate Software.
Bogels, S., & Phares, V. (2008). Fathers’ role in theetiology, prevention, and treatment of child anxiety: Areview and new model. Clinical Psychology Review,28, 539–558.
Borkovec, T. D., Robinson, E., Pruzinsky, T., & DePree,J. A. (1983). Preliminary exploration of worry: Somecharacteristics and processes. Behavior Research andTherapy, 21, 9–16.
Broverman, I. K., Vogel, S. R., Broverman, D. M.,Clarkson, F. E., & Rosenkrantz, P. S. (1972). Sex-role stereotypes: A current appraisal. Journal of SocialIssues, 28, 59–78.
Bruhn, J. G. (1990). The two sides of worry. SouthernMedical Journal, 83, 557–562.
Derogatis, L. R. (1994). Symptom Checklist-90-R: Admin-istration, scoring, and procedures manual (3rd ed.).Minneapolis, MN: National Computer Systems.
Entwisle, D., & Doering, S. (1981). The first birth: Afamily turning point. Baltimore, MD: Johns HopkinsPress.
Feldman, S. S., & Nash, S. C. (1984). The transition fromexpectancy to parenthood: Impact of the first bornchild on men and women. Sex Roles, 11, 61–78.
Glazer, G. (1980) Anxiety levels and concerns amongpregnant women. Research in Nursing and Health, 3,107–113.
Gove, W.R. (1980). Mental illness and psychiatric treat-ment among women. Psychology of Women Quarterly,4, 345–362.
Green, J. M. (1998). Postnatal depression or perinataldysphoria? Findings from a longitudinal community-based study using the Edinburgh Postnatal DepressionScale. Journal of Reproductive and Infant Psychology,16, 143–155.
Harville, E. W., Savitz, D. A., Dole, N., Herring, A. H.,& Thorp, J. M. (2009). Stress questionnaires andstress biomarkers during pregnancy. Journal ofWomen’s Health, 18, 1425–1433.
Heinowitz, J. (1982). Pregnant fathers: How fathers canenjoy and share the experiences of pregnancy andchildbirth. Englewood Cliffs, NJ: Prentice Hall.
Hendrick, S. S. (1988). A generic measure of relationshipsatisfaction. Journal of Marriage and the Family, 50,93–98.
Hobbs, D. F., & Cole, S. P. (1976). Transition to parent-hood: A decade replication. Journal of Marriage andthe Family, 3, 723–731.
Jackson, D. L. (2003). Revisiting sample size and thenumber of parameters: Some support for the N:qhypothesis. Structural Equation Modeling, 10,128–141.
Janis, I. L., & Leventhal, H. (1965). Psychological as-pects of physical illness and hospital care. In.B. B. Wolman (Ed.), Handbook of clinical psychol-ogy. New York: McGraw-Hill.
Kessler, R. C., McGonagle, K. A., Zhao, S., Nelson,C. B., Hughes, M., Eshleman, S., . . . Kendler, K. S.(1994). Lifetime and 12-month prevalence of DSM-III-R psychiatric disorders in the United States:Results from the National Comorbidity Survey. Ar-chives of General Psychiatry, 51, 8–19.
Larsen, R. J., Diener, E., & Emmons, R. A. (1986). Af-fect intensity and reactions to daily life. Journal ofPersonality and Social Psychology, 51, 803–814.
Lawrence, E., Rothman, A. D., Cobb, R. J., & Bradbury,T. N. (2008). Marital satisfaction across the transitionto parenthood. Journal of Family Psychology, 22,41–50.
Lowe, N. K. (2000). Self efficacy for labor and child-birth fears in nulliparous pregnant women. Jour-nal of Psychosomatic Obstetrics and Gynecology, 21,219–224.
McCann, S. J. W., Stewin, L. L., & Short, R. H. (1991).Sex differences, social desirability, masculinity, and
Worries in expectant parents 17
the tendency to worry. Journal of Genetic Psychology,152, 295–301.
McDowell, I. (2006). Measuring health: A guide to ratingscales and questionnaires. New York: Oxford Univer-sity Press.
McNair, D., Lorr, M., & Droppleman L. F. (1981). Man-ual for the Profile of Mood States. San Diego, CA:EdITS.
Morris, L. W., Davis, M. A., & Hutchings, C. H. (1981).Cognitive and emotional components of anxiety.Literature review and a revised worry-emotionalityscale. Journal of Educational Psychology, 73,541–555.
Morse, C. A., Buist, A., & Durkin, S. (2000). First-timeparenthood: Influences on pre- and postnatal adjust-ment in fathers and mothers. Journal of Psychoso-matic Obstetrics and Gynecology, 21, 109–120.
Nolen-Hoeksema, S. (1996). Chewing the cud and otherruminations. In R. S. Wyer (Ed.), Advances in socialcognition (pp. 135–144). Mahwah, NJ: Erlbaum.
O’Hara, M. W., Schlechte, J. A., Lewis, D. A., & Varner,M. W. (1991). A controlled prospective study of post-partum mood disorders: Psychological, environmen-tal, and hormonal variables. Journal of AbnormalPsychology, 100, 63–73.
Ohman, S. G., Grunewald, C., & Waldenstrom, U. (2003)Women’s worries during pregnancy: Testing the Cam-bridge Worry Scale on 200 Swedish women. Scandi-navian Journal of Caring Sciences, 17, 148–152.
Petersen, J., Paulitsch, M., Guethlin, C., Gensichen, J., &Jahn, A. (2009). A survey on worries of pregnantwomen—Testing the German version of the Cam-bridge Worry Scale. BMC Public Health, 9, 490–499.
Radloff, L. S. (1977). The CES-D scale: A self-reportdepression scale for research in the generalpopulation. Applied Psychological Measurement, 1,385–401.
Righetti-Veltema, M., Conne-Perreard, E., Bousquet, A.,& Manzano, J. (1998). Risk factors and predictive
signs of postpartum depression. Journal of AffectiveDisorders, 49, 167–80.
Robichaud, M., Dugas, M. J., & Conway, M. (2003).Gender differences in worry and associated cognitive-behavioral variables. Journal of Anxiety Disorders,17, 501–516.
Rosenfield, S. (2000). Gender and dimensions of theself: Implications for internalizing and externalizingbehavior. In E. Frank (Ed.), Gender and its effectson psychopathology (pp. 23–36). Washington, DC:American Psychiatric Press.
Salovey, P., Rothman, A. J., Detweiler, J., & Steward, W.(2000). Emotional states and physical health. Ameri-can Psychologist, 55, 110–121.
Stavosky, J. M., & Borkovec, T. D. (1988). The phe-nomenon of worry: Theory, research, treatment andits implications for women. Women and Therapy, 6,77–95.
Tallis, F., Davey, G. C. L., & Capuzzo, N. (1994). Thephenomenology of non-pathological worry: A pre-liminary investigation. In G. C. L. Davey & F. Tallis(Eds.), Worrying, perspectives on theory, assessment,and treatment (pp. 61–89). New York: Wiley.
Tavris, C., & Wade, C. (1984). The longest war: Sexdifferences in perspective (2nd ed.). San Diego, CA:Harcourt Brace Jovanovich.
Westman, M. (2001). Stress and strain crossover. HumanRelations, 54, 557–591.
Westman, M., & Etzion, D. (1995). Crossover of stress,strain and resources from one spouse to another.Journal of Organizational Behavior, 16, 169–181.
Whisman, M. A., Uebelacker, L. A., & Weinstock, L. M.(2004). Psychopathology and marital satisfaction: Theimportance of evaluating both partners. Journal ofConsulting and Clinical Psychology, 72, 830–838.
Wood, W., Conway, M., Pushkar, D., & Dugas, M. J.(2005). People’s perceptions of women’s and men’sworry about life issues: Worrying about love, accom-plishment, or worry? Sex Roles, 53, 545–551.