Embed Size (px)
Citation preview
Form FL_0001
Workers Compensation Insurance Claims Kit
150 Camelot Drive P.O. Box 1029
Fond du Lac, WI 54936-1029888-576-2438
societyinsurance.com
Thank you for placing your workers compensation coverage with Society Insurance. It is our privilege to assist you in this vital area of your business. Our goal is to provide you the very best service in our industry while keeping the cost of workers compensation insurance at an affordable level. We have been doing so since 1915. Help us provide your injured employees with the timely service they deserve by promptly reporting all claims to us. For your convenience, we can accept your claim information via telephone. To submit a claim, please call 888-576-2438 to speak to a live representative. If you are calling after hours, you may press 9 at the prompt to be connected to a claims representative. This Workers Compensation Claims Kit will help you with the claims process if you need to file a claim. The following items are included in the kit:
A Workers Compensation Claims Handbook containing information on how you can provide the best possible care to your injured employee and help us reduce claim costs for you.
A Workers Compensation Return to Work Program Handbook to help you in establishing and implementing a return to work program.
Forms for use during the claims process that will help us to complete a thorough claims investigation and take advantage of any cost-containment measures that may apply to your claim.
Where applicable, mandatory postings supplied by your state. If these notices apply to you, please post them in a prominent area of the workplace.
If you would like to access electronic versions of the handbooks or forms, you may visit societyinsurance.com and navigate to our Workers Compensation Claims page. As always, your agent is an excellent resource for any general questions, or questions you may have regarding the information in this package. Please feel free to contact us if you have any additional questions regarding the claims process. Sincerely,
Rick W. Parks, CPCU President and CEO Society Insurance
LB-0382 (REV 11/15) RDA 10183
Tennessee Bureau of Workers’ Compensation 220 French Landing Drive, I-B
Nashville, TN 37243-1002 FORM C-42
EMPLOYEE’S CHOICE OF PHYSICIAN
An employer must provide a partially-completed form listing at least three physicians to an employee upon the report of a workplace injury. The employee must complete and then sign and date the section below that indicates the physician chosen. A copy of the fully-completed form should be provided to the employee with the original kept on file by the employer. If the employee refuses to accept medical services from the chosen physician, the employee’s rights to benefits may be delayed. NOTE: Employees traveling more than 15 miles one way to or from medical treatment may seek reimbursement of their travel expenses from the insurance carrier.
TO BE COMPLETED BY THE EMPLOYER:
Employer __________________________________________________________________ Date of Injury _____________________
Employer Contact ____________________________________ Phone _________________ Email ____________________________
Physician Name _____________________________________________________ Phone ___________________________________
Address _________________________________________ City ___________________________ State ______ Zip _____________
Physician Name _____________________________________________________ Phone ___________________________________
Address _________________________________________ City ___________________________ State ______ Zip _____________
Physician Name _____________________________________________________ Phone ___________________________________
Address _________________________________________ City ___________________________ State ______ Zip _____________
TO BE COMPLETED BY THE EMPLOYEE:
I have selected the following physician from the list provided to me by my employer:
Physician Name ______________________________________________________ Date Selected ____________________________
Employee Name ______________________________________________________ Appt Date/Time __________________________
Address _________________________________________ City ___________________________ State ______ Zip _____________
Phone _________________________________________ Email _______________________________________________________
Employee Signature _________________________________________________________ Date _____________________________
FL_6068_TN
Workers’ Compensation law requires this notice to be posted in a conspicuous place at the work site at all times.
LB-0922 (REV. 4/18) Authorization No. 337545 RDA 10183
TENNESSEE WORKERS’ COMPENSATION INSURANCE
POSTING NOTICE How to Report Work-Related Injuries
What should be done if injured at work?
Employee 1. Immediately report the injury to the
employer representative named below.
2. Select a treating physician from a panel provided by your employer.
3. If you have questions or problems, contact the employer representative or the Bureau of Workers’ Compensation.
Employer 1. Complete your company’s internal
“Workplace Injury form” and notify your workers’ compensation insurance company immediately, even if you have concerns about the validity of the claim.
2. Offer a panel of physicians to the employee via Form C-42 available on the Bureau’s website. In cases of emergency, call an ambulance and provide this form as soon as the injured employee has stabilized.
___________________________________________________________________________________ Printed name and title of the employer representative to be notified in the event of a work-related injury
___________________________________________________________________________________ Printed name of an alternative employer representative to be notified in the event of a work-related injury
___________________________________________________________________________________ Telephone number of employer representative to notify in event of a work-related injury
___________________________________________________________________________________ Address of employer representative to notify in event of a work-related injury
The Tennessee Bureau of Workers’ Compensation is
available to help both employees and employers.
220 French Landing Dr. 1-B Nashville, TN 37243-2667
800-332-2667 615-532-4812 TTD: 800-332-2257 tn.gov/workerscomp
FL_6071_TN
La ley de Compensación a Trabajadores exige que se publique este aviso en un lugar visible en el centro de trabajo en todo momento.
LB-0922 (REV. 4/18) Autorización No. 337545 RDA 10183
SEGURO DE COMPENSACIÓN A TRABAJADORES DE TENNESSEE
PUBLICACIÓN DE AVISO Cómo informar de lesiones laborales
¿Qué se debe hacer en caso de lesión laboral?
Empleado 1. Informe inmediatamente de la lesión al
representante del empleador indicado aquí abajo.
2. Seleccione un médico tratante del panel provisto por su empleador.
3. Si tiene alguna pregunta o problema, comuníquese con el representante de empleadores de la Oficina de Compensación a Trabajadores.
Empleador 1. Complete el formulario interno de su
empresa de “Lesión laboral” y notifique a su aseguradora de compensación a trabajadores inmediatamente, incluso aunque tenga dudas acerca de la validez de la reclamación.
2. Ofrezca un panel de médicos al empleado a través del Formulario C-42, disponible en el sitio web de la Agencia. En casos de emergencia, llame a una ambulancia y proporcione este formulario en cuanto el empleado lesionado se haya estabilizado.
___________________________________________________________________________________ Nombre en letra de molde y título del representante del empleador a ser notificado en caso de una lesión laboral
___________________________________________________________________________________ Nombre en letra de molde del representante del empleador alterno a ser notificado en caso de una lesión laboral
___________________________________________________________________________________ Número de teléfono del representante del empleador a ser notificado en caso de una lesión laboral
___________________________________________________________________________________ Dirección del representante del empleador a ser notificado en caso de una lesión laboral
La Oficina de Compensación a Trabajadores de
Tennessee está disponible para ayudar a empleados y
empleadores. 220 French Landing Dr. 1-B Nashville, TN 37243-2667
800-332-2667 615-532-4812 TTD: 800-332-2257 tn.gov/workerscomp
FL_6072_TN
LB—3265 (4/2018) RDA 10183
STATE OF TENNESSEEBUREAU OF WORKERS’ COMPENSATION
220 FRENCH LANDING DRIVE NASHVILLE, TENNESSEE 37243-1002
(615) 741-2395 1-800-332-2667
Notice of Employer Rights and Responsibilities in a Workers’ Compensation Claim
Your workers’ compensation insurance policy covers medical and partial wage-replacement benefits for any covered employee who sustains a compensable work-related injury or illness. This document, produced by the Tennessee Bureau of Workers’ Compensation and provided by your insurance carrier or TPA, is designed to give you a better understanding of your role and responsibilities under the workers’ compensation system.
Your workers’ compensation adjusting entity is ___________________________________________________ Society Insurance(Printed name of carrier, self-insured or TPA)
and your primary contact there is ______________________________________________________________ Mariel Bohnsack, Sr. Work Comp Claims Rep, 888-576-2438 [email protected](Printed name, title and contact information of primary contact)
• Notice of a work-related injury or illness Your employees have the right to report workplace injuries or illnesses. Their violation of your company’s policy regarding how quickly it must be reported is not sufficient grounds to prevent an injured worker from receiving worker’s compensation benefits. Employers must refrain from denying a claim or refusing to acknowledge an employee’s report of an injury because of how quickly it was reported. The insurance carrier must be notified of all alleged workplace injuries to allow the carrier to assign an adjuster to investigate the claim. If an injury is not reported within the timeframes defined in the workers’ compensation act, the adjuster will take the steps it believes is appropriate to protect the employer’s rights.
o Employees injured at work are entitled to receive medical treatment at no expense to them. Employers are entitled to guide treatment by providing the injured employee with a panel of at least three physicians who are willing and able to treat the injury and located within his/her community. The panel must be provided on an Employee Choice of Physician Form C-42, available on the “Forms” link on the Bureau’s website www.tn.gov/workerscomp. Employers must provide the panel within three (3) business days of the employee notifying his/her employer of their injury. The employee should indicate the physician selected, sign the form and return it to the employer. Failure to timely provide a valid panel of physicians may subject the employer to a penalty assessed by the Bureau.
o Employers should provide the injured employee with a copy of the Beginner’s Guide to Tennessee Workers’ Compensation, available on the Bureau’s website. This document provides important basic information to the employee and answers several commonly asked questions.
o Employers should immediately notify their insurance carrier after an injury is reported. Employers should report the injury to their insurance adjuster even if the injury is unwitnessed or suspicious. The adjuster will determine the claim’s compensability. Failure to immediately report the injury to the adjuster may subject an employer to a penalty assessed by the Bureau.
o Employers are allowed to request a written statement from the employee reporting the injury. Having this statement will assist the insurance adjuster if an investigation is necessary.
o Employers should immediately work to eliminate the likelihood of someone else being injured in the same manner.
o If the injured employee is disabled and unable to work his/her normal job or usual number of hours, the employee may be entitled to receive temporary disability (partial wage replacement) benefits. The insurance adjuster will need the employer to provide a wage history for the injured employee on a Wage Statement Form C-41, available on the Bureau’s website.
FL_6092
LB—3265 (4/2018) RDA 10183
• Notice to your employees The Tennessee workers’ compensation law requires all covered employers to display the Posting Notice available on the “Forms” link on the Bureau’s website. This notice provides your staff with the name and title of the person designated by the employer as the primary contact to receive reports of workplace injuries and illnesses. Your workers’ compensation insurance carrier should also provide you with a copy of this form when you purchase or renew your policy.
• Best Practices to Consider Implementing Employers can create a positive workers’ compensation culture and help build a relationship of trust and mutual aid with employees. Here are some practices that you should consider.
o If one of your employees is injured at work, reinforce his/her value to you by becoming an advocate rather than an adversary. Be a resource when injured employees have questions or concerns.
o Encourage your employees to report their injuries as soon as possible. Delays in reporting injuries negatively affect recovery.
o Let your staff know how much you rely on them and want them to return. Stay in contact with injured employees during their recovery period if they are unable to work. Call them, email them, text them—even consider sending a “Get Well” card to them. It will be one of the best investments you can make in improving your workers’ compensation culture and outcomes.
o Focus your workers’ compensation goals on “workers’ recovery”. Provide work to your injured employees that comply with a treating physician’s restrictions, if possible. If an employer considers an employee as disabled, the employee will view themselves as disabled, too. And, studies prove that the longer an injured worker stays off work, the less likely they are to return to work. Work to help your injured employees return to their health and to their jobs as quickly as possible. It is good for everyone!
o Provide the employee with a copy of the signed Form C-42 and assist the employee with making the appointment with the chosen physician.
o Remember, it is the responsibility of the insurance adjuster to “accept” or “deny” a workers’ compensation claim, but he/she will need your assistance. Assist the insurance adjuster in investigating any claim in which you have doubts. Obtain witness statements. Take photos of the site of the injury. Do not automatically deny your employees their rights to report a claim just because you have doubts. Failure to timely provide appropriate benefits may subject an employer to a penalty assessed by the Bureau.
o Injured employees will often have questions about their benefits, their rights and what to expect. The Bureau has an Ombudsman Program designed to assist employees with these, and other questions if they are not represented by an attorney. Ombudsmen can be reached by calling 800-332-2667 or by emailing [email protected]. The Bureau’s website has information helpful to employers and injured employees. Share these resources with your supervisors before someone is injured and with injured employees after a claim is made.
o Perform an analysis concerning how injured employees have been treated in the past. If your employees routinely hire attorneys to obtain their workers’ compensation benefits, work to discover why they believe that they need legal representation. Is it a reflection of their fears that can be overcome by improving the workplace culture or is it a misconception that can be overcome by training and education?
o Create a culture of safety. Stress job safety in staff meetings and new hire orientations. Recruit a Safety Committee. Work to eliminate potential injuries before they occur.
o Consider participating in the Tennessee Drug Free Workplace Program. The program is designed to increase productivity for Tennessee employers and promote safe worksites for employees by promoting drug- and alcohol-free workplaces. There are financial benefits available to employers for participating and additional information is available on the Bureau’s website.
o Lead by example. Don’t complain about the process. Encourage your employees to keep you informed about any changes to their ability to work. Let them know that you want them, and will help them, to recover and return to work as quickly as possible.
Visit the Bureau’s website at: www.tn.gov/workerscomp
FL_6092
TENNESSEE DRUG-FREE WORKPLACE
PREMIUM CREDIT PROGRAM APPLICATION
Date Application Received
Departmental Use Only
This form should be completed by the Employer and must be signed by an owner/officer of the company. After reading and understanding the Rules and Guidelines for Participating Employers (Chapter 0800-2-12) please answer all questions that apply. You may also refer to the Additional Instructions section located on the back of this form before submitting this application.
IMPORTANT: All applications MUST BE COMPLETE, LEGIBLE and SIGNED or they will be RETURNED . Copies will not be accepted. Include the completed original copy of this form plus one photocopy of the completed form, a copy of PROOF OF COVERAGE and a self-addressed, stamped #10 envelope addressed to your Workers’ Compensation Insurance Carrier orAgent of Record for your workers’ compensation policy. Keep a copy of this form for your records.
Part A-Type of Form (check one): New Application Renewal Termination/Rescission Changed Ins Carrier
Part B-Applicant Information:
I. Company Name___________________________________________________________FEIN:____________________________________
Mailing Address__________________________________________________City______________________State & Zip________________
Business Address __________________________________________________City ____________________ State & Zip ______________
Phone #____________________________________________________Fax #_________________________________________________
Email address_____________________________________________________________________________________________________
Nature of Business___________________________________________ Number of Full-time & Part-time Employees_________ /_________
Workers’ Compensation Insurance Carrier_______________________________________________________________________________
Mailing Address__________________________________________________City______________________State & Zip________________
Name of Substance Abuse Program Administrator_________________________________________________________________________
Date written policy statement was provided to all employees____/____/____ Effective date of your program____/_____/____
II. Drug Testing Program: (Required on all applications.)Name of Testing Laboratory____________________________________________________ City, State_____________________________
Name of Medical Review Officer (MRO)___________________________________________ City, State_____________________________
Lab Certification: SAMHSA____________CAP-FUDTAP___________Other___________MRO Phone:_____________________________
III. Education and Employee Assistance Program: (Required on all applications.)
Please provide the date you conducted or plan to conduct an annual minimum two-hour of Workplace Substance Abuse Recognition training for supervisory personnel. ____/____/____ , ____/____/____
Please provide the date you conducted or plan to conduct an annual minimum one-hour of Workplace Substance Education and Awareness Program for all your employees. ____/____/____ , ____/____/____
Are employees required to use a designated employee assistance program for substance abuse treatment? Yes No
If yes, how many of your employees used it for substance abuse treatment in the past twelve 12 months? _________
If no, do you maintain & post the required list of local employee assistance programs or substance abuse treatment centers? Yes No
Part C - Renewal Applicants Only:IV. Date Previous Program Began ____/____/____ How many employees used it for substance abuse treatment in the past 12 months? ______
Name of Testing Laboratory____________________________________________________ City, State_____________________________
Name of Medical Review Officer (MRO)___________________________________________ City, State_____________________________ Lab Certification: SAMHSA____________CAP-FUDTAP___________Other___________MRO Phone:_____________________________
Number of tests performed in past 12 months for each of the following: Job Applicants: Positive____ Total____ Routine Fitness for Duty: Positive____ Total____ Post work accident: Positive____ Total____
EAP Follow-up: Positive____ Total____ Reasonable Suspicion: Positive____ Total____ Random (optional): Positive____ Total____
Part D - Termination / Rescission of Participation by Employer:V. Date Previous Program Began____/____/____ How many employees used it for substance abuse treatment in the past 12 months?_______
Number of tests performed in past 12 months for each of the following: Job Applicants: Positive____ Total____ Routine Fitness for Duty: Positive____ Total____ Post work accident: Positive____ Total____
EAP Follow-up: Positive____ Total____ Reasonable Suspicion: Positive____ Total____ Random (optional): Positive____ Total____
LB -0393 (REV 03/09) PG . 1 OF RDA 101832Reason for Termination / Rescission____________________________________________________________________________________
FL_6073
VI. Additional Instructions
All applications for the Tennessee Drug-Free Workplace Program must include (1) the completed original copy of this form plus one photocopy of the completed form, (2) a copy of proof of coverage and (3) a self-addressed, stamped #10 envelope addressed to your Workers' Compensation Insurance Carrier or Agent of Record for your workers' compensation policy. Applications must be mailed to the Department of Labor and Workforce Development at the address indicated below. Anytime an employer who is currently receiving the premium credit changes carriers for their Workers' Compensation Insurance, items (1), (2) and (3) must be resubmitted to the Department of Labor and Workforce Development. If an employer is a member of a Self-Insured Workers' Compensation Pool Program or is Totally Self-Insured for Workers' Compensation Coverage, items (1), (2) and (3) should be mailed to the Department of Labor and Workforce Development according to the instructions above, with a self-addressed, stamped #10 envelope addressed to either your pool program's administrative office or the department or person at your company who is responsible for the administration of your Drug-Free Workplace Program. Keep a copy of this form for your records. Employers should properly document their compliance with the Rules and Guidelines established for participation. You may be asked to supply documentation to support your compliance when denying workers' compensation benefits to an employee pursuant to the provision of the Tennessee Drug-Free Workplace Program (50-9-100 et. seq.). There will be a charge for additional copies of an employer's Tennessee Drug-Free Workplace Application. All requests must be in writing on your company's letterhead and submitted via facsimile at 615-532-1468. Billing will be done on a monthly basis. Renewals - In order to continue to receive the premium credit for each subsequent policy year, THIS APPLICATION MUST BE RENEWED ANNUALLY. By the anniversary date of their Workers' Compensation insurance policy, a new copy of this form must be completed by the employer and submitted with items (1), (2) and (3). Applications must be mailed to the Department of Labor and Workforce Development at the address indicated below. Termination/Rescission of Program - Any employer who wishes to terminate their participation in the Tennessee Drug-Free Workplace Program must provide a new completed copy of this form to the Department of Labor and Workforce Development according to the instructions above.
Applications, Renewals and Terminations are not accepted by facsimile.
VII. Penalties for Misrepresentation of Compliance
An Employer who misrepresents compliance with their Tennessee Drug-Free Workplace Program shall be subject to an additional premium for purposes of reimbursement of any previously granted discount. (T.C.A. Section 50-6-418)
An Employer’s good-faith effort to fulfill certain criteria for certification will be taken into consideration when determining whether the Employer has complied substantially with certification criteria.
VIII. Employer Certification: (Required on all applications.)
I hereby certify that all provisions and requirements of the Tennessee Drug-Free Workplace Program as established by T.C.A. Sections 50-9-100 et. seq. have been met and implemented. I have read and do understand the Penalties for Misrepresentation of Compliance.
_________________________________________________________________________________________________________________________
Owner/Officer’s Signature & Title Name in Print Date
_________________________________________________________________________________________________________________________
Owner/Officer’s Mailing Address Phone Number
LB -0393 (REV 03/09) PG . 2 OF RDA 101832
Mail Directly to: Tennessee Department of Labor & Workforce Development Division of Worker’s Compensation Drug-Free Workplace Program220 French Landing Drive
37243-1002 Nashville, TN Commissioner or his designee, DRUG-FREE WORKPLACE PROGRAM Tennessee Department of Labor & Workforce Development DATE ACCEPTED
The Tennessee Department of Labor & Workforce Development is committed to the principles of equal opportunity and equal access.
For comments or questions regarding the Tennessee Drug-Free Workplace Program or for alternative print copies of this form, call: 1-800-332-2667 (TDD) during regular business hours. Or visit our website at www.state.tn.us/labor-wfd/dfwp.html
NCCI ID#
FL_6073
Form FL_0003_TN
Employer's Claim Reporting Checklist
Page 1 of 1
P.O. Box 1029, Fond du Lac, WI 54936-1029 Phone (888) 576-2438 • Fax (920) 922-1071
Important: This form is for the employer's use.
1. Address the immediate medical needs of your injured employee. The employer is to provide a panel of three doctors from which the employee shall select one (1). Both parties should complete the Form C-42 Agreement Between Employer/Employee Choice of Physician. This is your proof that your injured employee was offered a choice of physician. If you need assistance completing this form, please contact Society Insurance.
2. If any injury occurs that may be covered by your policy, let Society Insurance know as soon as possible. Please remember to contact us even when your injured employee will not require immediate medical treatment. Late reporting may result in fines.
3. Provide your injured employee with a copy of the Pharmacy Program Letter of Intent document. This letter is a temporary card that will allow your injured employee to receive an initial supply of medication. A permanent plastic card will be issued to them once the claim is set up.
4. Let us know if your injured employee's treatment will require any of the following: • An MRI, CT scan, or other diagnostic testing • Use of durable medical equipment (such as crutches or a knee brace) • Physical or occupational therapy • Chiropractic care
5. Have your injured employee's supervisor complete the Supervisor Incident Report. Be sure to secure the name, address, and phone numbers of any witnesses to the incident.
6. Set aside any materials or machinery that may have contributed to or caused the injury. Secure the name, address, and phone numbers of anyone you feel may be responsible for the injury. We may be able to seek recovery from a responsible party.
7. Provide your injured employee with a copy of the Attending Physician's Return to Work Recommendations Record. Please provide us with a completed copy of this form or any information you receive regarding return to work, or anticipated return-to-work dates. Please let us know if there will be no lost time involved with the claim.
8. Please let us know if you have any type of light-duty work available that you will be able to offer your injured worker when they are capable of returning to work.
9. Phone in your claim to a claim representative at 888-576-2438. If you know your policy number, please have it available when you call in. Please provide wage information on claims with lost time from work or those that have the potential for lost time. Do not delay your filing if the information is not readily available.
10. You may submit a First Report of Injury, along with any medical documentation that has been received, directly to Society Insurance at the address below. If you chose this method for submitting your claim, please keep a copy for your records.
Society Insurance 150 Camelot Drive P.O. Box 1029 Fond du Lac, WI 54936-1029 Phone: 888-576-2438 Fax: 920-922-1071 Note: Always keep a supply of First Report of Injury forms on hand. You can obtain additional forms from our
office. Please see the Claims Kit computer screen pull-outs for additional information regarding items contained on this checklist.

Form FL_0004_TN
Injured Worker's Claim Reporting Checklist
Page 1 of 1
P.O. Box 1029, Fond du Lac, WI 54936-1029 Phone (888) 576-2438 • Fax (920) 922-1071
Important: This form is for the injured worker's use.
1. If necessary, seek immediate medical attention for your injuries. Notify your employer if you feel your injuries were caused by your job duties, even if you do not plan on seeking immediate medical treatment.
2. Request a copy of the Pharmacy Program Letter of Intent from your employer. This letter will allow you to receive an initial supply of any medication that is needed for your injuries. A permanent plastic card will be issued to you once your claim is set up.
3. Let your claim representative know if your treatment has included or will likely include any of the following: • An MRI, CT scan, or other diagnostic testing • Use of durable medical equipment (such as crutches or a knee brace) • Physical or occupational therapy • Chiropractic care
4. Help your employer secure the names of any witnesses to your incident. Help your employer identify any materials or machinery that you feel may have contributed to or caused your injury.
5. Request a copy of the Attending Physician's Return to Work Recommendations Record from your employer. It is your responsibility to ensure that this document is completed by your physician and given to your employer immediately following every appointment.
6. The employer is to provide a panel of three doctors from which the injured worker shall select one (1). Both parties should complete the Form C-42 Agreement Between Employer/Employee Choice of Physician. If you need assistance completing this form, please contact Society Insurance.
7. Request that your employer submit the First Report of Injury to us as soon as possible. We prefer to receive the information by phone or fax.
8. Your claim representative may contact you to obtain additional information that may be needed to complete the investigation of your claim. You may contact your claim representative at any time with questions regarding your claim:
Society Insurance 150 Camelot Drive P.O. Box 1029 Fond du Lac, WI 54936-1029 Phone: 888-576-2438 Fax: 920-922-1071
9. Promptly complete and return any forms that you receive from your claim representative. These forms can be returned to us in the postage-paid envelope that you will receive with the forms.
10. Please contact your claim representative immediately following every appointment. This will help us expedite payment of any lost-time benefits that may be owed, as well as provide prompt payment of any medical bills related to your claim.
LB-0379 (REV 11/15) FL_6074 RDA 10183
Tennessee Bureau of Workers’ Compensation 220 French Landing Drive, I-B
Nashville, TN 37243-1002 800-332-2667
FORM C-31 MEDICAL WAIVER AND CONSENT
This form is not required for injuries occurring on or after July 1, 2014
THIS MEDICAL AUTHORIZATION FORM ONLY PERMITS THE EMPLOYER OR THE BUREAU OF WORKERS’ COMPENSATION TO OBTAIN MEDICAL INFORMATION THROUGH ORAL OR WRITTEN COMMUNICATION, INCLUDING, BUT NOT LIMITED TO, CHARTS, FILES, RECORDS, AND REPORTS IN THE POSSESSION OF A MEDICAL PROVIDER AUTHORIZED BY THE EMPLOYER PURSUANT TO T.C.A. § 50-6-204 AND A MEDICAL PROVIDER THAT IS REIMBURSED BY THE EMPLOYER FOR THE EMPLOYEE’S TREATMENT.
I, ______________________________, having filed a claim for workers' compensation benefits, do hereby authorize (Printed Patient Name)
______________________________________________________ to furnish to my employer or my employer’s (Name of Medical Provider)
representative, and/or the Bureau of Workers' Compensation any information or written material reasonably related to my
work-related injury of _____________________for which I am claiming compensation. I further authorize the release of (Date of Injury)
the same information to me or my attorney. The authorization includes, but is not restricted to, a right to review and obtain copies of all records, x-rays, x-ray reports, medical charts, prescriptions, diagnoses, opinions and courses of treatment.
A photocopy of the authorization may be accepted in lieu of the original.
__________________________________________________________________________________________________ Patient Signature Date Date of Birth
THE USE OF THIS FORM IS REQUIRED UNDER THE PROVISIONS OF THE
TENNESSEE WORKERS' COMPENSATION LAW AND MUST BE
COMPLETED AND FILED WITH YOUR INSURANCE CARRIER
IMMEDIATELY AFTER NOTICE OF INJURY.
IT IS A CRIME TO KNOWINGLY PROVIDE FALSE, INCOMPLETE OR MISLEADING INFORMATION TO ANY PARTY TO A WORKERS' COMPENSTAION TRANSACTION FOR THE PURPOSE OF COMMITTING FRAUD. PENALTIES INCLUDE IMPRISONMENT, FINES AND DENIAL OF INSURANCE BENEFITS. IF YOU HAVE QUESTIONS, THE STATE NOW HAS A BENEFIT REVIEW SYSTEM WHERE A WORKERS' COMPENSATION SPECIALIST CAN PROVIDE ASSISTANCE. CALL 1-800-332-2667 (TTD).
TENNESSEE DEPARTMENT OF LABOR AND WORKFORCE DEVELOPMENT EMPLOYER'S FIRST REPORT OF WORK INJURY OR ILLNESS
JURISDICTION CLAIM # (STATE FILE #)
CLAIMS ADM CLAIM # (INSURER CLAIM #)
OSHA LOG CASE #
NAME OF INSURANCE CARRIER
CLAIMS ADMIN FIRM NAME (IF DIFFERENT FROM CARRIER)
CLAIMS ADJUSTER NAME
CLAIM HANDLING OFFICE ADDRESS LINE 1 AND LINE 2
EMPLOYER NAME
EMPLOYER ADDRESS LINE 1 AND LINE 2
CITY
INSURED NAME (PARENT CO. IF DIFFERENT THAN EMPLOYER)
CLA
IMS
AD
M/C
ARR
IER
EMPL
OY
ERPO
LICY
EMPL
OY
EE
CLAIM TYPE CODEMED ONLY INDEMNITY BECAME LOST TIME BECAME MED ONLY NOTIFY ONLY TRANSFER
FULL TIME /REGULAR PART TIME PIECE WORKER SEASONAL VOLUNTEER APPRENTICE FULL TIME APPRENTICE PART TIME
MALE FEMALE UNKNOWN
MARRIED SEPARATED UNKNOWN
UNMARRIED, SINGLE, DIVORCED
WEEKLY BI-WEEKLYMONTHLY
HOURLY DAILY
WIDOW WIDOWER MOTHER
DAUGHTER SON
SISTER BROTHER HANDICAPPED CHILD
CARRIER FEIN
FEIN OF CLMS ADM
CLMS ADJ PHONE #
EMPLOYER FEIN
POLICY NUMBER
STATE ZIP
ZIPSTATECITY
Form FL_6064
SIC CODE PHONE NUMBER
NATURE OF BUSINESS
INSURED REPORT # EMPLOYER LOCATION
EFF DATE
EXP DATE
EMPLOYMENT STATUS CODE
GENDEREMPLOYEE LAST NAME
FIRST
SELF INSURED ?YES NO
YES NO
NOYES
NOYES
PMAMAM PM
ADDRESS LINE 1 AND LINE 2
MI
PHONE INCL AREA CODE
NUMBER OF DAYS WORKED PER WEEK
DEPARTMENT REGULARLY WORKED
OCCUPATION DESCRIPTION
HOW INJURY OR ILLNESS OCCURRED. DESCRIBE THE INCIDENT INCLUDING WHAT THE EMPLOYEE WAS DOING JUST BEFORE, THE PART OF THE BODY AFFECTED AND HOW, AND OBJECT OR SUBSTANCE THAT DIRECTLY HARMED THE EMPLOYEE.
ZIPSTATECITY
ZIPSTATECITY ZIPSTATECITY
SSN DATE OF BIRTH DATE OF HIRE
SALARY CONTINUED IN LIEU OF COMPENSATION
MARITAL STATUS NCCI CLASS CODE
WAGE $
WA
GE
ACC
IDEN
T/IN
JURY
TREA
TMEN
TO
THER
FULL WAGES PAID FOR DATE OF INJURY
DATE OF INJURY
DATE EMPLOYER NOTIFIED OF INJURY
DATE CLAIM ADM NOTIFIED OF INJURY
DATE LAST DAY WORKED
DATE DISABILITY BEGAN
DATE OF DEATH (IF APPLICABLE)
RETURN TO WORK DATE (IF APPLICABLE)
COULD NOT BE DETERMINEDTIME OF INJURY TIME EMPLOYEE BEGAN WORK ON INJURY DATE
BODY PART AFFECTED CODE NATURE OF INJURY CODE CAUSE OF INJURY CODE
IF DEATH CLAIM, GIVE # DEPENDENTS FOR EACH RELATIONSHIPFATHER TOTAL # DEPENDENTS
PREMISES?DID INJURY/ILLNESS OCCUR ON EMPLOYER'S
ADDRESS WHERE INJURY OCCURRED (IF OTHER THAN EMPLOYER'S PREMISES)
ZIPSTATECITYCOUNTY OF INJURY
ADDRESS LINE 1 AND LINE 2 ADDRESS LINE 1 AND LINE 2
NO MEDICAL TREATMENTINITIAL TREATMENT
MINOR BY CLINIC/HOSPITALMINOR BY EMPLOYER HOSPITALIZED > 24 HRS
EMERGENCY CAREFUTURE MAJOR MEDICAL/LOST TIME ANTICIPATED
DATE PREPARED
PHYSICIAN NAME HOSPITAL OR OFF SITE TREATMENT NAME
PREPARER'S NAME & TITLE PREPARER'S COMPANY NAME PHONE NUMBER
Page 1 of 1
PERIOD
Society Insurance 39-0711880
(888) 576-2438
PO BOX 1029 Fond du Lac WI 54936
/ /
/ /
/ / / /
/ /
/ /
/ /
/ /
/ /
/ /
/ /
/ /
FL_0018A
FL_0018A
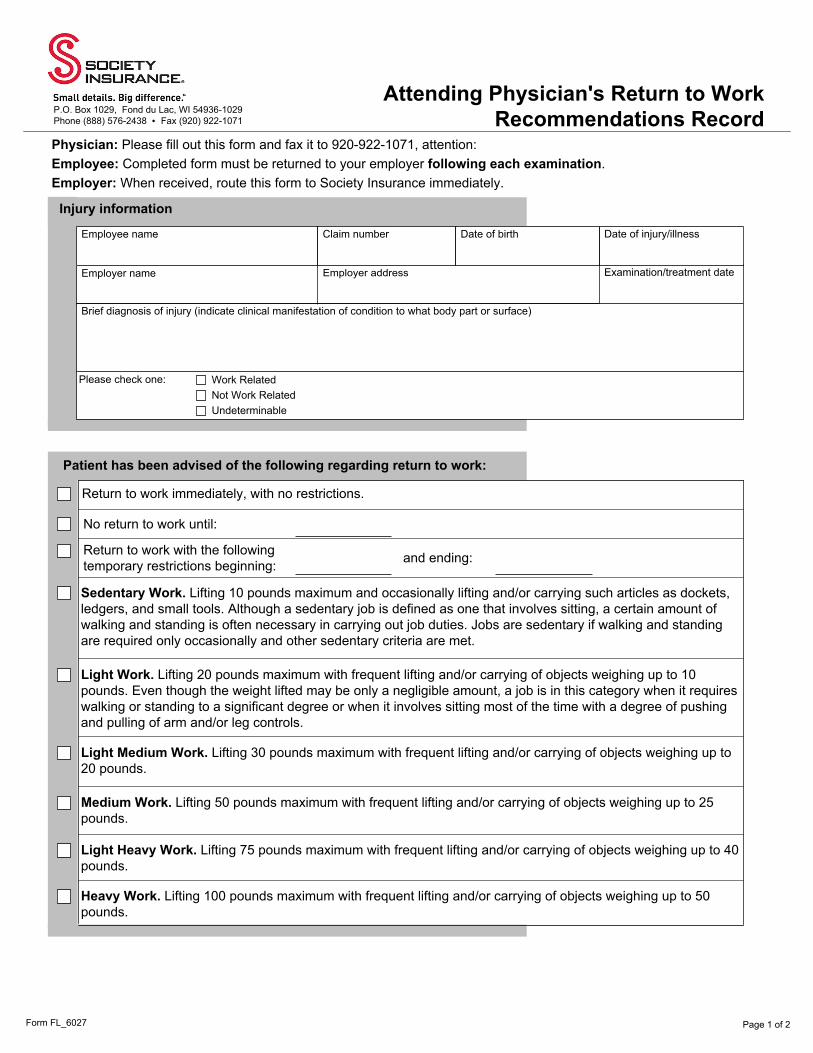
Form FL_6027
Attending Physician's Return to Work Recommendations Record
Page 1 of 2
P.O. Box 1029, Fond du Lac, WI 54936-1029 Phone (888) 576-2438 • Fax (920) 922-1071
Physician: Please fill out this form and fax it to 920-922-1071, attention: Employee: Completed form must be returned to your employer following each examination. Employer: When received, route this form to Society Insurance immediately.
Injury information
Employee name Claim number Date of birth Date of injury/illness
Employer name Employer address Examination/treatment date
Brief diagnosis of injury (indicate clinical manifestation of condition to what body part or surface)
Please check one: Work RelatedNot Work RelatedUndeterminable
Patient has been advised of the following regarding return to work:
Return to work immediately, with no restrictions.
No return to work until:
Return to work with the following temporary restrictions beginning: and ending:
Sedentary Work. Lifting 10 pounds maximum and occasionally lifting and/or carrying such articles as dockets, ledgers, and small tools. Although a sedentary job is defined as one that involves sitting, a certain amount of walking and standing is often necessary in carrying out job duties. Jobs are sedentary if walking and standing are required only occasionally and other sedentary criteria are met.
Light Work. Lifting 20 pounds maximum with frequent lifting and/or carrying of objects weighing up to 10 pounds. Even though the weight lifted may be only a negligible amount, a job is in this category when it requires walking or standing to a significant degree or when it involves sitting most of the time with a degree of pushing and pulling of arm and/or leg controls.
Light Medium Work. Lifting 30 pounds maximum with frequent lifting and/or carrying of objects weighing up to 20 pounds.
Medium Work. Lifting 50 pounds maximum with frequent lifting and/or carrying of objects weighing up to 25 pounds.
Light Heavy Work. Lifting 75 pounds maximum with frequent lifting and/or carrying of objects weighing up to 40 pounds.
Heavy Work. Lifting 100 pounds maximum with frequent lifting and/or carrying of objects weighing up to 50 pounds.

Form FL_6027 Page 2 of 2
Number of consecutive hours patient can perform specified activity during an 8-hour work period
6-8 4-5 1-3 0Sitting
Standing
Walking
Pushing
Pulling
Climbing
Bending
Kneeling
Reaching
Grasping
Weight-handling frequencies per hour
15 or more 10-14 1-9 0Lifting/carrying less than 10 pounds
Lifting/carrying 10-20 pounds
Lifting/carrying 20-50 pounds
Lifting/carrying 50-100 pounds
Patient discharged? YesNo
Next scheduled examination/treatment date
Comments and Notes
Attending physician's signature Date Phone Fax
Print Name Address
Attending physician
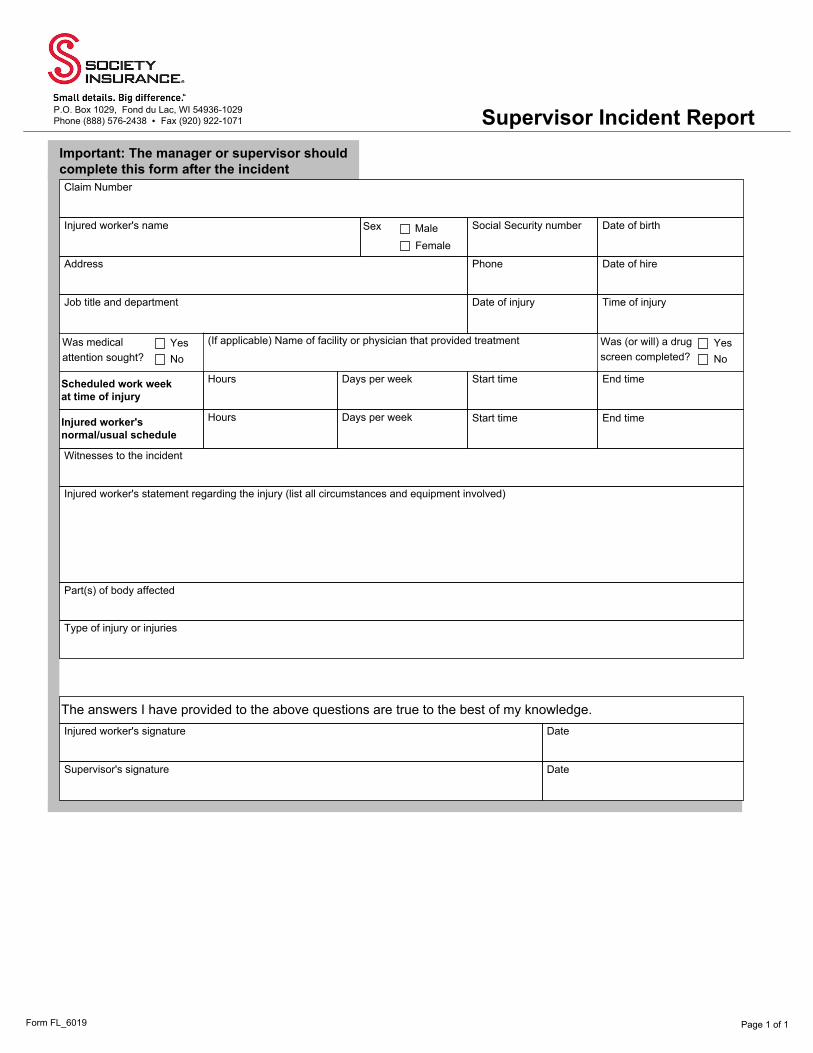
Form FL_6019
Supervisor Incident Report
Page 1 of 1
P.O. Box 1029, Fond du Lac, WI 54936-1029 Phone (888) 576-2438 • Fax (920) 922-1071
Important: The manager or supervisor should complete this form after the incidentClaim Number
Injured worker's name Sex MaleFemale
Social Security number Date of birth
Address Phone Date of hire
Job title and department Date of injury Time of injury
Was medical attention sought?
YesNo
(If applicable) Name of facility or physician that provided treatment Was (or will) a drug screen completed?
YesNo
Scheduled work week at time of injury
Hours Days per week Start time End time
Injured worker's normal/usual schedule
Hours Days per week Start time End time
Witnesses to the incident
Injured worker's statement regarding the injury (list all circumstances and equipment involved)
Part(s) of body affected
Type of injury or injuries
The answers I have provided to the above questions are true to the best of my knowledge.Injured worker's signature Date
Supervisor's signature Date
Form FL_6017
Witness Statement Form
Page 1 of 2
P.O. Box 1029, Fond du Lac, WI 54936-1029 Phone (888) 576-2438 • Fax (920) 922-1071
Injured worker's name Claim number
Injured worker's information
Name Address
Home phone Cell phone
Employer Job title
Your information
Date of incident Time of incident What is your relationship to the injured worker? Did you see the incident?
YesNo
What work was being performed when the incident occurred?
Please explain what you saw.
Where were you in relation to the injured employee when the incident occurred? Did you have a clear view of the incident?
Incident information
Page 2 of 2Form FL_6017
How did the injured employee act after the incident? Did they say anything to you?
Did the injured employee show you where they were hurt?
Did you see anyone else who may have seen what happened? If yes, please include names and phone numbers.
Was anything said to you by anyone other than the injured employee? If yes, who said something? When did they say it? What did they say?
Did you discuss anything regarding the injury with anyone? If yes, who did you discuss it with? When did you discuss it? What did you discuss?
Did the injured employee ever mention any prior problems with the injured area to you? If yes, when did they mention it?
Incident information continued
Witness signature Date
Form FL_6018
Job Analysis
Page 1 of 2
P.O. Box 1029, Fond du Lac, WI 54936-1029 Phone (888) 576-2438 • Fax (920) 922-1071
Employment Information
Employee name Claim number Employer name
Job title Supervisor interviewed? YesNo
If yes, list supervisor name
Was the employee hired with any restrictions?
YesNo
If yes, explain the restrictions
Typical work hours per week Overtime? YesNo
Break? YesNo
If yes, list frequency
Body movements at work
RarelyOccasionally (1/3 or less)
Frequently (1/3 to 2/3)
Continuously (2/3 or more)
Sitting
Standing
Walking
Vertical reaching at or above shoulder height
Bending/stooping/squatting
Crawling/kneeling
Close-distance hearing
Near/far vision
DrivingDescribe the driving involved
Weights handled (lbs.) Item
Alone or assisted? Push/pull/lift?
Times per day Distance moved
1-10
11-20
21-50
More than 50
Page 2 of 2Form FL_6018
Hand coordination
Is the injured worker right or left handed? Right Left
Movement required Tool/machine Left Right BothFine manipulation
Hand twisting
Power gripping
Simple grasping
Physical surroundings
Work inside Percentage performed inside: Work outside Percentage performed outside:Work around moving machinery?
YesNo
If yes, describe
Check each of the following that the employee comes in contact with:
Strong odor
Mist
Fumes
Steam
Describe fumes
Air conditioning Dust
Additional comments or observations
Signature Date completed
Form FL_6020
Transitional Return to Work Log
Page 1 of 1
P.O. Box 1029, Fond du Lac, WI 54936-1029 Phone (888) 576-2438 • Fax (920) 922-1071
Transitional return to work log
Claim Number Injured worker's name Supervisor
Date Hours Worked
In Out
Tasks performed Comments regarding injured worker's tolerance of modified-duty tasks
Initials
Sunday Injured worker
Supervisor
Monday Injured worker
Supervisor
Tuesday Injured worker
Supervisor
Wednesday Injured worker
Supervisor
Thursday Injured worker
Supervisor
Friday Injured worker
Supervisor
Saturday Injured worker
Supervisor
I clearly understand, take responsibility for, and acknowledge the limitations my physician has placed on me while participating in this temporary transitional work program.
Physician's name
Injured worker's signature Date
Form FL_0016
PPO Network Providers
Page 1 of 1
P.O. Box 1029, Fond du Lac, WI 54936-1029 Phone (888) 576-2438 • Fax (920) 922-1071
To reduce costs, we use a Preferred Provider Organization (PPO) network for our bill-review process. This document will help you to identify some of the medical providers in your area that have agreed to discount their services for the treatment of your injured worker. All states allow employers to seek emergency medical assistance for an injured worker on the day of the injury. The choice of medical services varies from state to state. In some states, the employer has the choice to select medical care; in other states, the employee has that choice. In either case, there are specific rules and limitations on the selection of medical services. Our network look-up system will help you locate members of the PPO network quickly and accurately. Use of these providers may result in lower claim costs for you. Visit this site to find a network medical provider in your area: https://www.viiad.com/societyinsurance/compass/provider_search_main.asp * *Inclusion on this site is not an endorsement of quality assurance or availability. If you require further assistance in identifying a medical provider, please call us at 888-576-2438.
Page 1 of 1Form FL_6069
FORM C-41TENNESSEE DEPARTMENT OF LABOR AND WORKFORCE DEVELOPMENT
Division of Workers' Compensation 220 French Landing Dr.
Nashville, Tennessee 37243-1002
It is a crime to knowingly provide false, incomplete or misleading information to any party to a workers' compensation transaction for the purpose of committing fraud. Penalties include imprisonment, fines and denial of insurance benefits. Employee:__________________________ SSN: _____________ State File#: _______________________ Insurer Claim #: _______________________ Date of Injury: _______________________________
In order to determine the correct rate of compensation to be paid to the above injured party, please fill in the schedule below and return it promptly. This information is required by law and no agreement for payment of compensation can be made until it has been received. Please complete 52 weeks prior to date of accident.
Please describe allowances of any character made in lieu of wages that must be deemed a part of employee's earnings: _______________________________________________________________
If the average weekly wage is not based on fifty-two weeks of earnings proceeding the date of injury, please show your computation below:__________________________________________________
Rate per Day______________ Rate per Hour__________ Average per Week_______________ I hereby certify that the above is a true and correct account, as taken from our time books or payroll records, of the wages paid to the above-named injured employee for the periods indicated. Date _______________ 20 _____ Employer ______________________________________________ Name of Preparer & Title ___________________________________________________________________ Phone, Fax, Email _________________________________________________________________________
LB-0384 (REV. 01/08) RDA 10183
WAGE STATEMENT
WEEK NO. DAYS
WEEK ENDING GROSS WAGES
1234567891011121314151617181920212223242526
WEEK NO. DAYS
WEEK ENDING GROSS WAGES
2728293031323334353637383940414243444546474849505152
TOTAL PAID
/ /
Form FL_0017
Risk Control Services
Page 1 of 1
P.O. Box 1029, Fond du Lac, WI 54936-1029 Phone (888) 576-2438 • Fax (920) 922-1071
Our customers call Risk Control when they have something pressing on their minds, whether it relates to employee safety or evaluating trends in their insurance claims. They look for honest, objective, experienced, and thoughtful advice to address their concerns. As a policyholder, you are entitled to use Risk Control Services to help you control your workers compensation exposures. We help our customers identify and evaluate hazards that might cause insurance losses or otherwise disrupt their business. We use our broad experience in risk control to recommend business solutions to our customers and assist them in avoiding or mitigating these potential losses. These are our fundamental principles: Use a collaborative and consultative approach By working with our customers, we develop a fact-based view of the hazards affecting their business and provide consultative advice to successfully eliminate the hazards. Use our broad expertise to provide superior value We rely upon the technical diversity of our people - not a single consultant - to provide our customers with superior service. Build sustainable improvements for our customers We provide educational materials and value-added services that build knowledge and support for the customer to sustain their risk control program over the long term. Build a trusting relationship We want to earn the trust of our customers and agency partners. We do this by consistently providing professional service with absolute integrity. Below is a brief overview of the many value-added services available through Risk Control. • OSHA 10-hour and 30-hour training • Review of machine guarding procedures • Forklift training • Onsite visits • Safety video library • Customized training • Hazard identification • Safety handouts • Safety program development • Safety recommendations • Ergonomic assistance • Claims analysis If you have any questions or desire assistance in controlling your accident and illness exposures, please call our Risk Control Services department at 888-576-2438. Many of our resources are immediately available for your review in the Risk Control section of societyinsurance.com.