Embed Size (px)
Citation preview
Mtdun/~ (1994) 10,14&156 0 Longman Group Ltd 1994 Midwifery
Women’s views of their postnatal care by midwives at an Adelaide Women’s Hospital
Georgina E. Stamp and Caroline A. Crowther
Objective: to determine the characteristics of a sample of women giving birth in one hospital in South Australia and these women’s perceptions of the usefulness of the advice and care that they were given during the puerperium Design: survey using questionnaires, incorporating Lipsett’s (1984) questions, administered before the women left hospital and at six weeks postdelivery. Setting: one hospital in South Australia. Purtici~ants: a sample of convenience of 235 women completed the hospital questionnaire and 222 (95%) returned the six weeks postpartum questionnaire. Findings: the women’s ages ranged from 17-44 years, 86% were living in a stable relationship and 42% were primiparous. Most women (74%) made comments on the helpfulness of midwives. The midwife provided emotional support (57%)) answered questions (32%) and gave information (30%). However, midwives’ attitudes were perceived as insensitive (18%) and judgemental (9%). Midwives gave conflicting advice (lo?’ ) o and 40% of the women made one or more comments about midwife unhelpfulness. Sixteen per cent of the women made no comment on the helpfulness of the midwife. Implications forpractice: contact with midwives in the early postnatal period is an ideal time for helpful advice and support to be given but midwives are not always perceived as fulfiling this part of their role. There is a need to address the issue of conflicting advice.
INTRODUCTION
During the past 15 years considerable dissatis- faction has been expressed by women with all aspects of their birth experience and perinatal care, coupled with calls for increased support and more involvement in decision making (Mickle-
Georgina E Stamp RN, RM, ACMI. Midwife Researcher/Visiting Midwife, Caroline A Crowther MD, FRACOG, FRCOG, DDU. Senior Lecturer, University of Adelaide, Queen Victoria Hospital, 160, Fullarton Road, South Australia 5067.
(Requests for offprints to GE) Manuscript accepted 3 November 1994
thwait et al, 1978; Cartwright, 1979; Kirke, 1980; Oakley, 1980; McIntyre, 1982; Lipsett, 1984; Jacoby, 1988; Reid & Garcia, 1989; Armstrong & Feldman, 1990; Lumley, 1990; Health Depart- ment of Western Australia, 1990; Green et al, 1990; Percival, 1991; House of Commons, 1992).
There are difftculties associated with measur- ing, or even defining, ‘satisfaction’ which may be affected by a number of issues. These include a woman’s ‘loyalty’ to her particular birth and the way it was conducted, whether the questioner was directly involved in her care, and timing of the questioning, as satisfaction ratings early in the puerperium may overestimate positive effects (Cartwright, 1979; Shearer, 1983; Lumley, 1985).
148

MIDWIFERY 149
Findings in a UK study of 825 women assessing their childbirth expectations and experiences indicated that obtaining information and feeling in control correlated with women’s postpartum feelings of emotional wellbeing (Green et al, 1990).
Important effects have been reported over
time. In a study following up 15-20 years after the birth of their first child Simkin (1991) found women’s recall of the experience was vivid. Those expressing long-term satisfaction had felt in con- trol, remembering positively their care providers’ words and actions, and feeling that their confi- dence and self esteem had been increased, whilst women with lower satisfaction ratings did not report positive associations. McIntyre (1982) pointed to ‘troubled communications’ between pregnant women and their medical and mid- wifery attendants with conflicting information and a preoccupation with rules predominating postnatally. In a study in two London hospitals a high percentage of women questioned postnatally stated that they were not informed of reasons for procedures such as induction of labour and cae- sarean section with 65% saying they had received no information at all about breast feeding (Kirke, 1980). More recently, Jacoby (1988) reported that 21% of a large random sample found it rather dif- ficult, or very difficult, to get all the information they wanted postnatally, and 14% found feeding advice unhelpful.
A tremendous amount of attention is focused
on the actual birth experience and the postnatal period can come as an anticlimax for a woman. Physically she needs to recover, particularly if she is one of the increasing number having a cae- sarean birth (King, 1993). It is during this crucial time that a woman will seek support and reassur- ance as she cares for and establishes a relationship with her new baby, yet conflicting messages in hospital may confuse her and erode her confi- dence (McIntyre, 1982; Lipsett, 1984; Health Dept Victoria, 1990). On returning home and expected to care for the baby, she may find her- self on her own, especially if her family of origin is elsewhere, her partner is working, or if she is a single parent. Even if she has been well prepared with information, she and her partner frequently report shock at the changes in their lifestyle and
relationship (Oakley, 1980; Southern Community Health Services Research Unit, 1990; Health Dept Victoria, 1990).
There is sufftcient evidence from overviews and trials that increased support and involving women in decisions relevant to their care results in im- proved satisfaction and outcomes (Oakley, 1985; Elbourne et al, 1989; Kennell & Klaus, 1992) but no study was found which reports that these find- ings have been implemented.
In reviewing the literature it was noted that there was no South Australian data to support or refute the findings of other researchers, particu- larly in respect of women’s perceptions of their midwifery care. Therefore a study investigating women’s perceptions of midwifery care, postnatal mood and breast feeding rates was conducted in South Australia. A further aim of the study was to assess whether perceptions of care changed over a period of time. Reported in this paper are the characteristics of a sample of women giving birth at an Adelaide Women’s Hospital and their per- ceptions of the usefulness of advice and care they received from midwives during the puerperium.
METHODS
A prospective descriptive survey using both quan- titative and qualitative methods was undertaken. Lipsett (1984) conducted a study investigating Australian women’s perceptions of their postnatal care. After asking four open ended questions she divided the responses into specific categories in order to quantify the data. The Lipsett questions were used in this study after the birth and at six weeks postpartum, the only modification being substitution of the words ‘nurse’ with ‘student midwife’ and ‘sister’ with ‘midwife’. Women com- pleted questionnaires commenting on the care they had received in the time since the birth of their baby at both assessment times. The ques- tions were:
‘Who was most helpful?’ ‘What did the midwife or student midwife do or say that was helpful?’ ‘What did the midwife or student midwife do or say that was unhelpful?’

150 MIDWIFERY
‘What could the midwife or student midwife have done that would have been more helpful?’
Responses were placed into specific categories relating to aspects of physical and supportive mid- wifery care received by women such as emotional support and breast feeding help used by Lipsett. Randomly selected qualitative data were assigned to these categories by another midwife uncon- nected with the study with a high level of agree- ment reached. The questions were tested on a pilot group of five women and were found to be acceptable to them.
Women were considered eligible to participate if they gave birth to a singleton baby of at least 37 weeks gestation, gave informed consent and were fluent in English. Previous enrolment in another postnatal research project automatically excluded women from selection. The available research funding was not sufftcient to cover translators and interpreters for non-English speaking women who were therefore ineligible to participate. The midwife researcher (GS) was not involved in the provision of direct midwifery care. This was con- sidered important in minimising potential bias
from women’s responses (Cartwright, 1979; Shearer, 1983; Lumley, 1985). Women who met the inclusion criteria and who gave birth between July and December 1990 were invited postnatally by the researcher to participate in the study. The
naire in a sealed envelope in an internal letter box addressed to the researcher or handed it per- sonally to her. In order not to miss those who took early discharge the women were enrolled at differ- ent days postpartum. The range of days of recruit- ment was 2-10 days, mean 4.29 (SD 1.93).
In order to give the women the opportunity to describe any care they received in the community, as well as to reflect on their care by midwives in hospital, women were sent another questionnaire asking the same Lipsett questions, and prefaced by the same words ‘since the birth of your baby’, at six weeks postpartum. However, the women were not asked to discriminate between their experiences in hospital and since discharge from hospital. As part of the larger study they also com- pleted a 10 point self-esteem scale (Rosenberg, 1965), the Edinburgh postnatal depression scale (EPDS) (Cox et al, 1987) and questions about baby feeding method at this time.
Epinfo software was used for the database and for analysis of the data. Student’s t-test was used to assess significance between continuous variables and the Chi-square test and odds ratios were used for non-continuous variables.
Permission to undertake the study was obtained from the Queen Victoria Hospital and the University of Adelaide Research and Ethics Committees.
researcher visited the wards, usually on week day mornings, and frequently on weekend mornings FINDINGS
study was undertaken Aboriginal women consti- tuted 2% of the population giving birth in the hospital (Queen Victoria Hospital, 1990-l) and
when the hospital was quieter. After time to con-
around 2% of the population of pregnant
sider carefully and to discuss the study with her
Australian women (Lancaster, 1989).
partner or family, the woman signed consent and was enrolled in the study. She then completed a questionnaire, some time before discharge, high-
lighting her perceptions of postnatal care to date. Fifteen women declined to take part, three of
these were Aboriginal women. At the time the
Characteristics of the study women
Two hundred and thirty five women agreed to take part in the study, of whom 222 (95%) returned a questionnaire at six weeks postpartum. This high response rate was achieved by sending a postal reminder to 37 (16%) women, and 24 (10%) were followed up with phone calls.
The women’s ages ranged from 17-44 years, with the mode in the 26-30 age group (Table 1). The majority (86%) of the women were married or liv- ing in a stable relationship. Primiparous women made up 42% of the sample. In Australia approxi- mately 50% of women have private health insur- ance for obstetrics. This entitles them to an
Women were assured of the total confidentiality of their responses. Although the accompanying signed consent form could identify a woman, she usually placed it with the completed question-
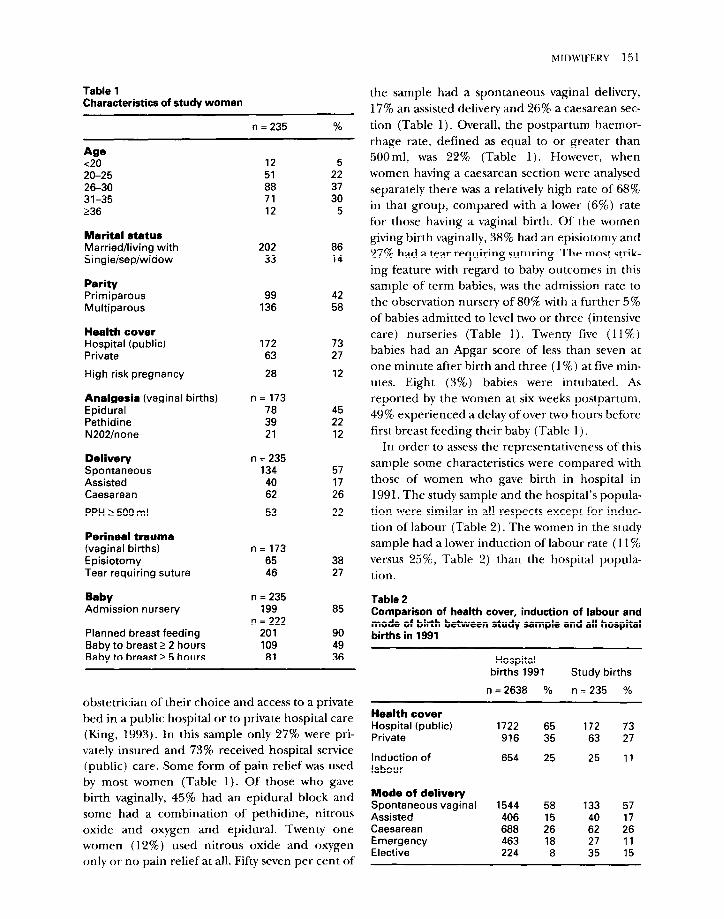
Table 1 Characteristics of study women
n = 235 %
Age <20 20-25 26-30 31-35 236
12 51 88 71 12
Marital status Married/living with Singlelsepiwidow
202 33
Parity Primiparous Multiparous
99 42 136 58
Health cover Hospital (public) Private
High risk pregnancy
172 73 63 27
28 12
Analgesia (vaginal births) n= 173 Epidural 78 Pethidine 39 N202lnone 21
Delivery Spontaneous Assisted Caesarean
PPH 2 500 m I
n = 235 134 40 62
53
Perineal trauma (vaginal births) Episiotomy Tear requiring suture
n= 173 65 46
Baby Admission nursery
Planned breast feeding Baby to breast 2 2 hours Baby to breast 2 5 hours
n = 235 199
n = 222 201 109 81
5 22 37 30
5
86 14
45 22 12
57 17 26
22
38 27
85
90 49 36
obstetrician of their choice and access to a private bed in a public hospital or to private hospital care (King, 1993). In this sample only 27% were pri- vately insured and 73% received hospital service (public) care. Some form of pain relief was used by most women (Table 1). Of those who gave birth vaginally, 45% had an epidural block and some had a combination of pethidine, nitrous oxide and oxygen and epidural. Twenty one women (12%) used nitrous oxide and oxygen only or no pain relief at all. Fifty seven per cent of
MIDWIFERY 151
the sample had a spontaneous vaginal delivery, 17% an assisted delivery and 26% a caesarean sec-
tion (Table 1). Overall, the postpartum haemor- rhage rate, defined as equal to or greater than 500m1, was 22% (Table 1). However, when women having a caesarean section were analysed separately there was a relatively high rate of 68% in that group, compared with a lower (6%) rate for those having a vaginal birth. Of the women giving birth vaginally, 38% had an episiotomy and 27% had a tear requiring suturing. The most strik- ing feature with regard to baby outcomes in this sample of term babies, was the admission rate to the observation nursery of 80% with a further 5% of babies admitted to level two or three (intensive care) nurseries (Table 1). Twenty five (11%) babies had an Apgar score of less than seven at one minute after birth and three (1%) at five min- utes. Eight (3%) babies were intubated. As reported by the women at six weeks postpartum, 49% experienced a delay of over two hours before first breast feeding their baby (Table 1)
In order to assess the representativeness of this sample some characteristics were compared with those of women who gave birth in hospital in 1991. The study sample and the hospital’s popula- tion were similar in all respects except for induc- tion of labour (Table 2). The women in the study sample had a lower induction of labour rate (11% versus 25%, Table 2) than the hospital popula- tion.
Table 2 Comparison of health cover, induction of labour and mode of birth between study sample and all hospital births in 1991
Health cover Hospital (public) Private
Induction of labour
Hospital births 1991 Study births
n = 2638 % n = 235 %
1722 65 172 73 916 35 63 27
654 25 25 11
Mode of delivery Spontaneous vaginal 1544 58 133 57 Assisted 406 15 40 17 Caesarean 688 26 62 26 Emergency 463 18 27 11 Elective 224 8 35 15
152 MIDWIFERY
Women’s perceptions of postnatal Table 4
care Who women found most helpful postnatally
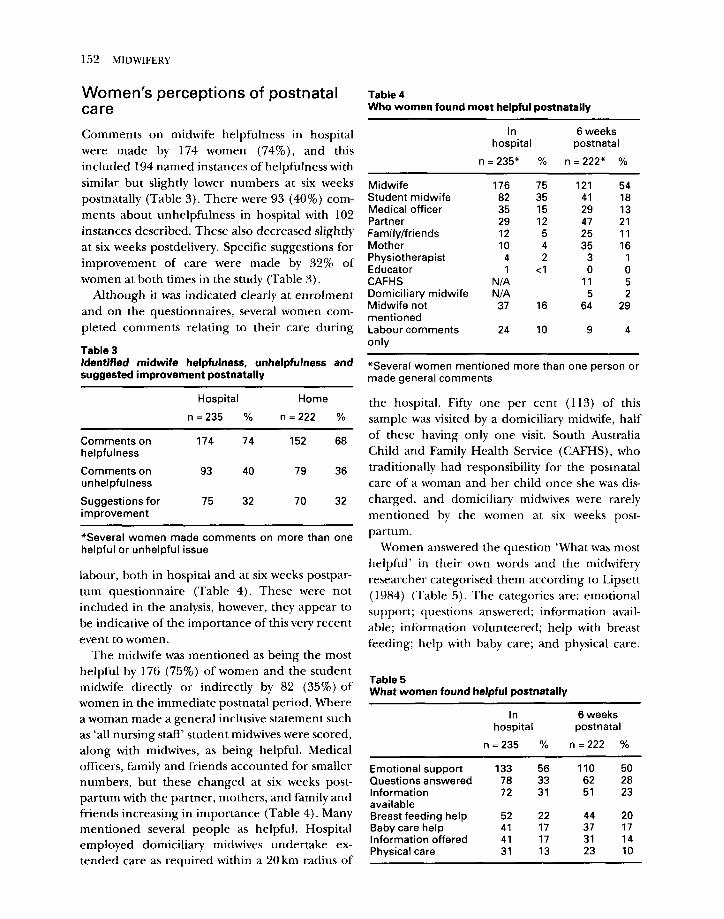
Comments on midwife helpfulness in hospital were made by 174 women (74%)) and this included 194 named instances of helpfulness with similar but slightly lower numbers at six weeks postnatally (Table 3). There were 93 (40%) com- ments about unhelpfulness in hospital with 102 instances described. These also decreased slightly at six weeks postdelivery. Specific suggestions for improvement of care were made by 32% of women at both times in the study (Table 3).
In 6 weeks hospital postnatal
n =235* % n=222* %
Although it was indicated clearly at enrolment and on the questionnaires, several women com- pleted comments relating to their care during
Student midwife Medical officer Partner Family/friends Mother Physiotherapist Educator CAFHS Domiciliary midwife Midwife not mentioned Labour comments only
176 75 121 54 82 35 41 18 35 15 29 13 29 12 47 21 12 5 25 If 10 4 35 16 4 2 3 1 1 <I 0 0
N/A 11 5 N/A 5 2
37 16 64 29
24 10 9 4
Table 3 Identified midwife helpfulness, unhelpfulness and suggested improvement postnatally
*Several women mentioned more than one person or made general comments
Hospital Home
n = 235 % n =222 %
Comments on helpfulness
Comments on unhelpfulness
Suggestions for improvement
174 74 152 68
93 40 79 36
75 32 70 32
*Several women made comments on more than one helpful or unhelpful issue
labour, both in hospital and at six weeks postpar- tum questionnaire (Table 4). These were not included in the analysis, however, they appear to be indicative of the importance of this very recent event to women.
The midwife was mentioned as being the most helpful by 176 (75%) of women and the student midwife directly or indirectly by 82 (35%) of women in the immediate postnatal period. Where a woman made a general inclusive statement such as ‘all nursing staff student midwives were scored, along with midwives, as being helpful. Medical officers, family and friends accounted for smaller numbers, but these changed at six weeks post- partum with the partner, mothers, and family and friends increasing in importance (Table 4). Many mentioned several people as helpful. Hospital employed domiciliary midwives undertake ex- tended care as required within a 20 km radius of
the hospital. Fifty one per cent (113) of this sample was visited by a domiciliary midwife, half of these having only one visit. South Australia Child and Family Health Service (CAFHS), who traditionally had responsibility for the postnatal care of a woman and her child once she was dis- charged, and domiciliary midwives were rarely mentioned by the women at six weeks post- partum.
Women answered the question ‘What was most helpful’ in their own words and the midwifery researcher categorised them according to Lipsett (1984) (Table 5). The categories are: emotional support; questions answered; information avail- able; information volunteered; help with breast feeding; help with baby care; and physical care.
Table 5 What women found helpful postnatally
In 6 weeks hospital postnatal
n =235 % n =222 %
Emotional support 133 56 110 50 Questions answered 78 33 62 28 Information 72 31 51 23 available Breast feeding help 52 22 44 20 Baby care help 41 17 37 17 Information offered 41 17 31 14 Physical care 31 13 23 10
MIDWIFERY 153
The majority of women in hospital (133, 57%) found emotional support most helpful. Examples of comments were:
-Unhurried help and support, treated me with respect and dignity.
- Made me feel as much part of things as pos- sible.
-Always there to sit down for a chat, very re- assuring.
In hospital some women appreciated their questions being answered (78, 33%) while for others believing information was available if needed was important (72,31%) :
quendy reported unhelpful interactions. Examples of comments were:
-The midwife said my baby has a ‘temper’. This was not the reason why my baby was cry- ing.
-Some squeezed my breasts and pushed the baby’s head down until it frightened her and me.
-There was one episode of conflicting advice, lots of cuddles versus not picking up the baby when upset, which really upset me.
-Conflicting advice, bossed and ordered around to do things their way.
- Overly critical and overbearing, unwilling to
-Any questions asked were answered politely admit a problem existed.
and happily. - One treated me as if I didn’t know anything
-Left all options to me, gave good informa- and made me feel I was doing it all wrong.
tion first. - Sometimes staff so busy, unable to attend to
- Day to day baby care help. my needs, or forgot.
-To follow my instincts when it comes to what - Some nurses forget they are our babies and
a baby needs. our confidence is lost through this.
At six weeks postpartum the distribution of what was considered most helpful was similar.
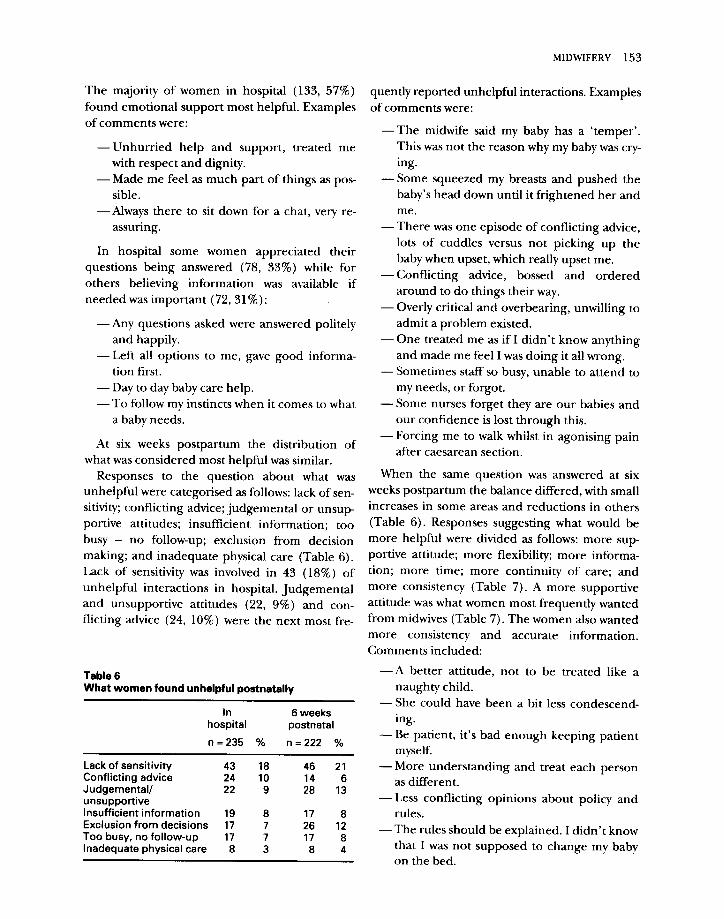
Responses to the question about what was unhelpful were categorised as follows: lack of sen- sitivity; conflicting advice; judgemental or unsup- portive attitudes; insufficient information; too busy - no follow-up; exclusion from decision making; and inadequate physical care (Table 6). Lack of sensitivity was involved in 43 (18%) of unhelpful interactions in hospital. Judgemental and unsupportive attitudes (22, 9%) and con- flicting advice (24, 10%) were the next most fre-
Table 6 What women found unhelpful postnatally
In 6 weeks hospital postnatal
n =235 % n =222 %
Lack of sensitivity 43 18 46 21 Conflicting advice 24 10 14 6 Judgemental/ 22 9 28 13 unsupportive Insufficient information 19 8 17 8 Exclusion from decisions 17 7 26 12 Too busy. no follow-up 17 7 17 8 Inadequate physical care 8 3 8 4
-Forcing me to walk whilst in agonising pain after caesarean section.
When the same question was answered at six weeks postpartum the balance differed, with small increases in some areas and reductions in others (Table 6). Responses suggesting what would be more helpful were divided as follows: more sup- portive attitude; more flexibility; more informa- tion; more time; more continuity of care; and more consistency (Table 7). A more supportive attitude was what women most frequently wanted from midwives (Table 7). The women also wanted more consistency and accurate information. Comments included:
-A better attitude, not to be treated like a naughty child.
-She could have been a bit less condescend- ing.
- Be patient, it’s bad enough keeping patient myself.
- More understanding and treat each person as different.
-Less conflicting opinions about policy and rules.
-The rules should be explained. I didn’t know that I was not supposed to change my baby on the bed.

154 MIDWIFERY
Table 7 What women said would have bean more helpful postnatally
In 6 weeks hospital postnatal
n = 235 % n =222 %
More information 20 9 More time 19 8
More continuity of care 9 4 More consistency 9 4
More supportive attitude 40 17
25
45
11
20 More flexibility 26 11 30
16
14
7
15 7 9 4
in collaboration with appropriate Aboriginal agencies (Aboriginal Health Organisation, 1989) and Aboriginal women themselves would have been much better accepted. This may well be war- ranted in the future.
Surveys indicating that most women are satis- fied with their care are often used as evidence that nothing needs changing (Oakley, 1992). Oakley
-I would have liked more accurate informa- tion and to be consulted more. Lack of infor- mation made me feel powerless, there was not enough support early on.
-Some are gifted, some are not - more consis-
tend to say they are satisfied. Lipsett (1984) points out that in any survey of services where improve- ment is sought, complaint is of more concern than approval. In Lipsett’s study (1984) approval outnumbered complaint by three to one. Nevertheless, in response to recurring themes of dissatisfaction with conflicting advice, postnatal
to
care was organised in a more integrated manner
(1992) that if asked argues choose, people pick what they know, and that most people are fairly conservative. If asked about something they will
-1 think continuity of care would be helpful with a concerted attempt to provide more consis-
and set standards about things. tency (Lipsett, 1991). Using Lipsett’s instrument, satisfaction was found to outnumber dissatisfac- tion by less than 2: 1 in this study, with a somewhat high proportion (40%) (Table 3) commenting
the findings cannot be generalised. However, there are some lessons that can be learnt from the study.
DISCUSSION
This study utilised a sample of convenience of less than 10% of the women who delivered in one year in one hospital in South Australia, therefore
The hospital employs Aboriginal Liaison Officers to assist in supporting and communicat- ing the needs of Aboriginal women in the hospi- tal. Those from remote areas in particular are often fearful and confused, particularly as their admission is likely to be related to a perinatal problem (Aboriginal Women of Central Australia, 1985). It is a limitation of this study that the researcher did not communicate with Aboriginal Liaison Offricers before approaches to Aboriginal women were made. Given that all three Aboriginal women approached refused to take part, the project may not have been seen to be relevant or culturally acceptable (Aboriginal Women of Central Australia, 1985; Gosden, 1992). However, there is little doubt that research
worrying, considering that it is midwives who are with women around the clock in hospital. Thirty two per cent of the women made suggestions for improving the postnatal midwifery care (Table 3). A finding similar to that from a Western Australian survey (Health Department of Western Australia, 1990). In this latter study 30% of respondents nominated improvements post- natally, 36% of which involved attitudes and
on unhelpfulness. That 75% of women men-
behaviour of midwives.
tioned satisfaction with midwives should not be a cause for complacency. In particular, when the 10% commenting on labour only are excluded, there remains 16% who did not mention a mid- wife or student midwife as helpful at all. This is
A common thread emerges from studies investi- gating women’s perceptions of their care (Cartwright, 1979; Lipsett, 1984; Seguin et al, 1989; Percival, 199 1; Health Dept Victoria, 1990; Green et al, 1990; House of Commons, 1992). Women want appropriate information, to feel in control, to be actively involved and to be treated with sensitivity. Frequently these basic needs are not met. In this study a significant number of

MIDWIFERY 155
women had their stay in hospital marred by insen-
sitive and judgemental attitudes, conflicting advice and were excluded from decision making by midwives . Comments about midwives having a preoccupation with policies and rules were com- mon. Many hospitals have a considerable number of policies, presumably for the safety and well- being of women and babies, but are some merely an attempt by institutions to protect themselves against liability? For example, there is a prohibi- tion against a woman changing her baby on her bed, yet this is one of the few places a woman can claim as her own personal space in hospital.
indeed, are the women they care for (Flint &
Polengeris, 1987). Several Australian hospitals are now providing
and evaluating this form of care (Brodie, 1993; Rowley, 1993; Queen Elizabeth Hospital Adelaide, personal communication). Continuity of care provided by a small team of midwives requires committed, willing and dedicated staff but there are increasing signs that this style of care may be a means of starting to address the problems of con- flicting advice and fragmentation of care so fre- quently reported by women.
Further investigation of such issues, the rationale for their existence and their effects on women is
Acknowledgements
needed. The authors wish to thank the women who generously gave their views and to whom we owe it to consistently monitor
Few women who deliver at this institution are our standards of care. Financial support came from the
likely to receive more than one postnatal home Queen Victoria Hospital Foundation in the awarding of a
visit from a domiciliary midwife, comparing un- Midwifery Fellowship. Guidance and support was given by Elizabeth Wood, Lesley Barclay, leffrey Robinson, Maggie
favourablv with visits UD to four weeks nostdeliverv Haertsch, Hilda Baktian, Wendy &ldsworthy, l%h 1 1
conducted by community midwives in the UK Waddington and Jane Freeman&. Brett Hay produced
(UKCC 1991). This leaves a gap in services pro- slides and John Hardy helped with data management. We also thank the midwives and ward clerks from the postnatal
vided at a crucial time for women and babies. The floors, Kerena Eckbert and Meg Phythian of Clinical
low rate of comments from the respondents on Information ServicesY Queen Victoria Hospital, Irene
care received from midwives after discharge could Wanganeen, Aboriginal Liaison Officer, Women and Children’s Hospital, and Tim Agius and Graham Brice of
have been a function of the questionnaire, which the Aboriginal Health Council of South Australia.
the respondents may have associated predomi- nantly with time spent in hospital. Community services postpartum (CAFHS) were curtailed in
References
1989). Effectively this means that a routine post- Aboriginal Women of Central Australia 1985 Congress
natal home visit is not provided except by referral Alukura by the Grandmother’s Law. Model of a Healthy Public Policv. Alukura. Alice Sorings. Northern ,I 1 0’
or request. The telephone advice and counselling Territory
service reports increasing demand, suggesting an Aboriginal Health Organisation 1989 Aboriginal Health
unmet community need. Research Ethnics Committee Inaugural Bulletin. Aboriginal Health Organisation, Adelaide, South
The considerable contact with midwives in the Australia
Armstrong P, Feldman S 1990 A wise birth. New York: earlv Dostnatal oeriod nrovides an ideal onnortu- William Morrow and Comnanv
J L 1 1 11
nity for helpful information and support in hospi- Brodie P 1993 Team midwif&y, the Westmead experience.
tal, but are midwives sometimes perceived as not Birth Issues 2(l): 7-10
providing enough of this because they are Cartwright A 1979 The dignity of labour? A study of
childbearing women and induction. London: Tavistock
stressed? This study did not address the feelings of Publications
midwives but a small pilot study in South Australia Cox J L, Holden J M, Sagovsky R 1987 Detection of
Dostnatal deoression - develooment of the 10 item suggested that midwives may find postnatal nurs- Edinburgh Postnatal Depression Scale (EPDS). British
ing (sic) stressful and that further research into Journal of Psychiatry 154: 732-786
this area is warranted (Summers, 1990). Evidence Elbourne D, Oakley A, Chalmers I 1989 Social and
from a randomised controlled trial, however, pyschological support during pregnancy. In Chalmers I. Enkin M, Keirse M J N C (eds) Effective Care in
showed that midwives working in teams providing Pregnancy and Childbirth. Oxford: Oxford University
continuity of antepartum, intrapartum and post- Press
Flint C 1986 Sensitive midwifery. London: Heinemann partum care are more satisfied by their work as, Medical Books

156 MIDWIFERY
Flint C, Polengeris P 1987 The Know Your Midwife Report. 49 Peckarman’s Wood, Sydenham Hill, London SE26
Gosden G 1992 Women’s talk: conversations about pregnacy, birth, motherhood and community. Distributed by Dianne C&den, 36 Lower Coast Road, Stanwell Park NSW 2508, Australia
Green J M, Coupland VA, KitzingerJ V 1990 Expectations, experiences and psychological outcomes of childbirth: a prospective studyof women. Birth 17( 11):15-24
Health Denartment ofvictoria 1990 Havine a babv in Victoria’- final report of the ministerial &iew of birthing services in Victoria (Chairperson J Lumley). Health Department of Victoria, Melbourne, Victoria
Health Department of Western Australia 1990 Report of the ministerial task force to review obstetric neonatal & Gynaecological services in Western Australia (Chairperson KA Michael) Health Department of Western Australia, Perth, Western Australia
House of Commons 1992 Health Committee, Second Report, Maternity Services. HMSO, London
Jacoby A 1988 Mothers’ views about information and advice in pregnancy and childbirth: findings from a national study. Midwifery 4: 103-l 10
Kennel1 M H, Klaus J H 1992 Continuous emotional support in labour in a US hospital: a randomized controlled trial. Journal of the American Medical Association 265( 17): 2197-2201
King J F 1993 Obstetric intervention and the economic imperative. British Journal of Obstetrics and Gynaecology 100: 303-304
Kirke P N 1980 Mothers’ views of obstetric care. British Journal of Obstetrics and Gynaecology 87: 1029-1033
Kitzinger S 1989 Childbirth and society. In Chalmers I, Enkin M, Keirse M J N C (eds) Effective Care in Pregnancy and Childbirth. Oxford: Oxford University Press
Lancaster PA L 1989 Birth defects in Aborigines. The Medical Journal of Australia 151: 241-242
Lipsett R 1984 The midwife - help or hindrance? Australian Journal of Advanced Nursing l(2): 7-14
Lipsett R 1991 What are the challenges for the next generation of midwives: 1990 -onwards? Australian College of Midwives Inc. Journal 4(3): 15-18
Lumley J 1985 Assessing satisfaction with childbirth. Birth 12(2): 141-145
McIntyre S 1982 Communications between pregnant women and their medical and midwifery attendants. Midwives’ Chronicle and Nursing Notes 95: 387-394
Micklethwait Lady, Beard R, Shaw K 1978 Expectations of a pregnant woman in relation to her treatment. British Medical.Journal 2: 188-191
Oakley A 1980 Women confined - towards a sociology of childbirth. Oxford: Martin Robertson
Oakley A 1985 Social support: the ‘soft’ way to improve birthweight? Social Science and Medicine 21: 1259-1268
Oakley A 1992 Perspectives of the users of the services. International Journal of Technological Assessment in Health Care8(Suppl 1): 112-122
Percival P 1991 Midwifery care -women’s perceptions presentation at the 7th Biennial Conference of the Australian College of Midwives Incorporated. ACMI, 260, Albert Street, East Melbourne, Victoria 3002
Queen Victoria Hospital 1990-l Clinical Information Services QVH Report. Queen Victoria Hospital, Adelaide
Rowley M 1993 A randomized controlled trial of continuity of midwife care vs routine midwifery care. Presentation and abstract: Proceedings of 11 th Annual Congress of Australian Perinatal Society. July 2&23 Hobart, Tasmania
Reid M, Garcia J 1989 Women’s views of care during pregnancy and childbirth. In Chalmers I, Enkin M, Keirse M J N C (eds) Effective Care in Pregnancy and Childbirth. Oxford: Oxford University Press
Rosenberg M 1965 Self-esteem scale from: society and the adolescent self image, Princeton, NewJersey: Princeton University Press
Shearer M 1983 Editorial: the difficulty of defining and measuring satisfaction with perinatal care. Birth 10(2): 77
Simkin P 1991 Just another day in a woman’s life? Women’s long-term perceptions of their first birth experience. Birth 18(4): 203-210
Summers A 1990 Are midwives stressed in postnatal nursing? Australian College of Midwives Inc. Journal 3(l): 11-14
Seguin L, Therrien R, Champagne Fetal 1989 The components of women’s satisfaction with maternity care. Birth 6(3): 109-113
South Australian Health Commission 1991 Pregnancy Outcome in South Australia 1991. South Australian Health Commission Epidemiology Branch, South Australia
Southern Community Health Services Research Unit 1990 ‘Nothing or no-one could have told me what it was going to be like’, the third and final report of the New Parenthood Project on the first year of parenting. SCHSRU Adelaide, South Australia.
UKCC 1991 Midwives’ rules, UKCC, London





























