Embed Size (px)
Citation preview

2007; 29: 558–565
Why medical students should learnhow to teach
M. DANDAVINO, LINDA SNELL & JEFFREY WISEMAN
McGill University, Canada
Abstract
Background: We reviewed the medical-education literature in order to explore the significance and importance of teaching
medical students about education principles and teaching skills.
Aims: To discuss reasons why formal initiatives aimed at improving teaching skills should be part of the training of all physicians,
and how it could begin at the medical-student level.
Description: In this article, we propose several reasons that support formal undergraduate medical training in education
principles: (1) medical students are future residents and faculty members and will have teaching roles; (2) medical students may
become more effective communicators as a result of such training, as teaching is an essential aspect of physician–patient
interaction; and (3) medical students with a better understanding of teaching and learning principles may become better learners.
We suggest that exposure to teaching principles, skills, and techniques should be done in a sequential manner during the
education of a physician, starting in medical school and continuing through postgraduate education and into practice. We outline
learning objectives, teaching strategies, and evaluation methods for medical-education components in an undergraduate
curriculum.
Conclusion: Medical students’ informal teaching activities accompany, facilitate, and complement many important aspects of
their medical education. Formally developing medical students’ knowledge, skills, and attitudes in education may further stimulate
these aspects.
Introduction
‘Doctor’ in Latin means ‘teacher’—and, indeed, teaching is one
of the key activities of a physician. Physicians are called upon
to teach their students and colleagues, as well as other health
professionals. When discussing diagnoses and care plans, they
teach patients, and there is evidence that patient education has
a positive effect on health outcomes (Kurtz et al. 2003).
Medical students regularly participate in study groups
during courses and prior to examinations, thus assuming
informal teaching roles. This type of peer-assisted education
seems to be effective and may make students better learners
(Topping 1996; McKeachie & Svinicki 2006). Medical students
also teach in other settings, as they become sources of
health information for family, friends, and, during their
clerkship, for patients.
Despite its universality, teaching is a skill that physicians
receive little formal training about (Craig & Page 1987;
Bing-You & Sproul 1992; Morrison & Hafler 2000). The need
to instruct faculty members, and more recently residents, about
how to teach is well described in the literature. There are
numerous papers and books describing novel initiatives to
improve teaching skills and describing the evaluation of
these for both faculty and residents (Morrison & Hafler 2000;
Busari & Scherpbier 2004). Many of the general principles
of faculty development apply to the development of
student teaching-skills workshops (Steinert et al. 2006).
There is, however, a surprisingly limited amount of literature
about formal attempts to facilitate the development of medical
students’ teaching skills (Paiva et al. 1982; Craig & Page 1987;
Bing-You & Sproul 1992; Nestel & Kidd 2002; Pasquale &
Pugnaire 2002; Moseley et al. 2002; Bardach et al. 2003;
Morrison et al. 2003). The few papers available note the
importance of introducing teaching skills prior to residency,
and a few describe elective activities involving small numbers
of students. All report the enthusiasm of medical students have
about acquiring these skills. Only a few medical schools
currently incorporate teaching skills into their undergraduate
curriculum.
Practice points
. Teaching is a key activity of physicians, and is a skill that
can be used by students early in their medical education.
. Medical students who learn how to teach may also
become more effective communicators, as teaching is an
essential aspect of the physician–patient interaction.
. Medical students with a better understanding of teaching
and learning principles may become better learners.
. Exposure to teaching principles, skills, and techniques
should be in a sequential manner during the education
of a physician, starting in medical school and continuing
throughout postgraduate education and into practice.
Correspondence: Dr Mylene Dandavino, Resident’s Office, Montreal Children’s Hospital, 2300 Tupper, Montreal, Quebec, Canada, H3H 1P3.
Tel: 514 448 0995; fax: 514 412 4311; email: [email protected]
558 ISSN 0142–159X print/ISSN 1466–187X online/07/060558–8 � 2007 Informa UK Ltd.
DOI: 10.1080/01421590701477449
Med
Tea
ch D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
B W
uerz
burg
on
10/2
9/14
For
pers
onal
use
onl
y.

In this paper we discuss, on the basis of our review of the
literature, reasons why formal initiatives to improve teaching
skills should be part of the training of all physicians and should
begin at the medical-student level. We also suggest learning
objectives and formats for implementing a Teaching Skills
Improvement Program (TSIP).
Methods
We conducted literature searches of the MEDLINE (1966 to
June 2006), CINAHL (1982 to June 2006) and ERIC (1966 to
June 2004) databases, using a structured search strategy
with the following keywords in various combinations:
‘medical’; ‘student(s)’; ‘teacher’; ‘resident’; ‘education’; and
‘undergraduate’.
Papers that addressed programs to improve medical
students’ teaching skills were selected and reviewed
(Table 1). Reference lists were browsed to find additional,
relevant references. Most of the articles found were descriptive
studies, opinion pieces, or reports of pedagogical experiences,
with no evaluation component. Many papers discussed the
teaching skills of residents and faculty members, but only
a few studies involved medical students as teachers (Paiva
et al. 1982; Craig & Page 1987; Bing-You & Sproul 1992; Nestel
& Kidd 2002; Pasquale & Pugnaire 2002; Moseley et al. 2002;
Bardach et al. 2003; Morrison et al. 2003). Through a Google�
search, bibliographies that listed literature reviews about
residents-as-teachers were found. Finally, key papers from
the literature on educational theory (Collins et al. 1991;
Ericsson et al. 1993; Chi et al. 1994; Topping 1996; Williams
& Deci 1998; Chi 2000; Ryan & Deci 2000; Misch 2002;
Sobral 2004; Issenberg et al. 2005; McKeachie & Svinicki 2006)
were selected after a search on ERIC and Google�, using the
terms ‘peer teaching’, ‘peer tutoring’, ‘students teaching
students’, ‘students as teachers’, and ‘to teach is to learn
twice’. Themes from the literature were used to develop the
rationale, objectives, and learning activities for a proposed
program to improve the teaching skills of medical students.
Results
Eight papers specifically addressed improving teaching skills
of medical students (Table 1).
One was an opinion survey about students’ future teaching
roles (Bing-You & Sproul 1992). Three obtained student
reactions to residency teacher-training initiatives (Paiva et al.
1982; Moseley et al. 2002; Morrison et al. 2003). Four others
described sessions or electives of varying lengths,
with outcomes including positive student ratings of the
activity, improved self-perceptions of their teaching, and
student involvement in teaching as co-tutors (Craig & Page
1987; Nestel & Kidd 2002; Pasquale & Pugnaire 2002;
Bardach et al. 2003).
Discussion
From the complete literature review, three themes emerged
supporting a TSIP for students, which are discussed below.
Our review of the literature also inspired ideas for the content
Table 1. Papers about teaching medical students how to teach.
ArticleStudy type, educational intervention, and number of
students participating (if applicable) Outcome
Bardach et al. 2003 Description of four 1-hour, classroom-based ‘Teach How
to Teach’ sessions for final-year students, teaching
‘intern-specific skills’, with an evaluation of post-course
reaction
Students ‘strongly endorse’ program, thought it would be
useful for residency, and listed strengths. All agreed that
‘formal instruction in teaching should be a required part
of medical education’.Bing-You & Sproul 1992 Opinion survey about future teaching roles (n¼ 97) Found that medical students are interested both in learning
teaching skills and teaching during medical school and
residencyCraig & Page 1987 Description of elective course entitled ‘Teaching in Medicine’
and students’ responses to the elective (n¼8)
Objectives were to design an instructional session,
demonstrate effective teaching behaviors, evaluate
own teaching behaviors. All students rated the course as
‘excellent’Morrison et al. 2003 Evaluation of a 60-hour, longitudinal elective entitled
‘Introduction to Clinical Teaching’ (n¼49)
Students enacted and participated in OSTEs testing
residents. Students believed that it helped improve
resident teaching and prepare them to become better
teachers.Moseley et al. 2002 Description of a 4-week elective, ‘Clinical Skills
Center Attending’ (n¼ 6) and survey of student
responses to elective
Students reported that it better prepared them for residency,
and that they would recommend it to other students.
Authors suggested that it is an effective method to
develop teaching skills and help students understand the
nature and function of academic clinical medicine.Nestel & Kidd 2002 Description of the evaluation of a workshop designed
to prepare students for work as peer tutors (n¼ 28)
Students became co-tutors for first-year students
Paiva et al. 1982 Description of a one-week elective entitled ‘Teaching
Role in Residency’ and survey of student response to
elective (n¼24)
A year after the elective, 85% of respondents thought the
elective contributed to their self-confidence about
assuming teaching responsibilities. Authors suggested
that preparation of teaching role should start during
residency.Pasquale & Pugnaire 2002 Description of a week-long elective entitled ‘Physician as
Teacher’ and survey of students’ response to elective;
15% of the fourth-year class enrolled.
Most (90%) of the students agreed or strongly agreed that
the course provided useful knowledge and skills.
Medical students learning how to teach
559
Med
Tea
ch D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
B W
uerz
burg
on
10/2
9/14
For
pers
onal
use
onl
y.

of a proposed TSIP, and for a process to incorporate such
a program into an undergraduate curriculum.
Why teach medical students how to teach
Several themes emerge in the literature that support instructing
medical students in how to teach: (1) medical students are
future residents and faculty members who will have teaching
roles; (2) as teaching is an essential aspect of physician-patient
interaction, medical students may become more effective
communicators as a result of such training; and (3) medical
students with a better understanding of teaching and learning
principles may become better learners.
1. Medical students are future residents and faculty members
who will have teaching roles. Clinical teachers play a crucial
role in the education of future physicians. It is important that
faculty members see one of their roles as that of a teacher
(Busari et al. 2003). This ‘identification’ may influence their
desire to teach and improve their teaching skills, satisfaction
with teaching, and ultimately, student learning. Early identifi-
cation of physicians to this teaching role may help improve
overall clinical teaching (Busari et al. 2003).
However, attending faculty are not the only physicians with
teaching responsibilities. Residents play a central role in the
education of their colleagues and medical students, often
spending many hours a week teaching (Bordley & Litzelman
2000; Morrison & Hafler 2000; Busari & Scherpbier 2004). It is
estimated that residents spend as much as 25% of their work
time in teaching activities, including supervising, instructing,
and evaluating medical students and junior residents (Seely
1999). Resident–teachers contribute to medical students’
learning in ways that complement the contributions made by
attending faculty, as they are closer to the student experience
and remember more clearly what it was like, and what worked
for them (Bordage & Lemieux 1991; McKeachie & Svinicki
2006). Residents themselves have identified teaching as an
important, but undervalued, part of their responsibilities and
their own education (Bordage & Lemieux 1991; Bing-You &
Harvey 1995).
In order to teach effectively, residents need to be familiar
with basic adult-learning principles and with the broad array
of teaching techniques that can be used during case
presentations, structured lectures, and informal team
discussions. The techniques that help improve faculty
members’ teaching are also effective in improving residents’
teaching. Formal instruction may enable residents to be more
effective teachers, and seems to increase their enjoyment of
teaching (Wipf et al. 1995; Wipf et al. 1999; Busari &
Scherpbier 2004). However, until recently, residents were
only rarely taught how to teach. In 1993, a US survey showed
that only 20% of internal-medicine residency programs
featured teaching-skills units, despite the fact that
residents provided 62% of inpatient teaching of medical
students (Bing-You & Tooker 1993). The proportion of
programs featuring teaching skills has no doubt increased
since then, but it is likely that many programs still lack formal
teaching training for their residents.
Medical students themselves perceive residents as having
a significant teaching role. They have estimated that a third of
their teaching is performed by residents (Bing-You & Sproul
1992). One survey showed that the great majority of medical
students expressed a desire to have definite teaching
responsibilities as residents (Barrow 1966), but also expressed
an interest in learning teaching techniques and even teaching
other medical students (Bing-You & Sproul 1992).
Despite the efforts made by residency programs,
studies suggest that residents too often assume teaching
responsibilities with insufficient formal preparation (Bordage
& Lemieux 1991; Tacci 1998). This is probably due, in part, to
the fact that gathering residents for a teaching-skills program
requires considerable resources, and can conflict with patient
care and on-call responsibilities (Bing-You & Sproul 1992).
One solution to this problem would be to offer teaching-skills
training in medical school. The methods used to train residents
and faculty should also be applicable to medical students.
Providing teaching training in the formal setting of the
undergraduate medical curriculum would be a way to help
ensure that all postgraduate trainees, at entry in their program,
have a basic knowledge of adult-education principles
and teaching strategies, and are ready for their teaching
responsibilities. It would also help medical students realize
that an important aspect of their physician identity will be
teaching, and thus move this role from the hidden to the
formal curriculum.
2. Medical students may become more effective communica-
tors, as teaching is an essential aspect of physician-patient
interaction. The literature on doctor–patient communication
has established the value of competent communication in
enhancing patients’ satisfaction, adherence, functional status,
and clinical outcomes (Bensing et al. 2000; Cegala &
Lenzmeier Broz 2002). Experts agree that communication is
a learned skill rather than a personality trait, and that one
can be taught to communicate more effectively. They also
agree that experience alone is a poor teacher in this area
(Kurtz 2002). Many medical-school curricula in Europe
and North America now include the teaching of
communication skills.
A large part of the doctor–patient interaction involves
teaching. With the recent emphasis on patient empowerment,
and with patient desire for more autonomy in medical
decision-making, the importance of this type of interaction is
even greater (Roter 2000; Kurtz 2002). The process of
providing medical information, including rationale and
options, is ‘teaching’. When one looks at the learning
objectives of communication-skills improvement programs,
the word ‘patient’ could be readily exchanged for the word
‘student’. Some examples include the eliciting of patients’
knowledge of the subject, assessment of patients’ expectations
and desire for information, summarizing information for the
patient, effectively managing the interview, using facilitating
techniques, probing for patient’s understanding, and
encouraging patients’ responses (Wipf et al. 1995). In fact,
the same five principles that Kurtz (2002) defines effective
communication with can be used to characterize
effective teaching: ensuring interaction, not just transmission;
M. Dandavino et al.
560
Med
Tea
ch D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
B W
uerz
burg
on
10/2
9/14
For
pers
onal
use
onl
y.

reducing unnecessary uncertainty; planning and thinking in
term of outcomes; demonstrating dynamism; and following
a helical (iterative), rather than a linear, model. The physician–
teacher helps by equipping his learners or patients with what
they need to help themselves; this includes not only
information, but also confidence in the value of their own
contribution (Roter 2000).
Many national organizations stress the importance of the
physician’s role in facilitating learning in others, including their
peers, patients, and students. As stated in the objectives of the
Graduate Medical Education Core Curriculum Project of
Association of American Medical Colleges in 1999: ‘Patient
care and the education of patients, peers and students require
the blending of a variety of skills [for] the physician and
communicator and teacher, [including] . . . effective commu-
nication, leadership, collaboration, team participation, and
teaching’. The communicator and scholar roles of CanMEDS
similarly imply a teacher role for the physician, as do the UK
recommendations on undergraduate medical education in
‘Tomorrow’s doctors’ (General Medical Council 2003).
A medical school that includes initiatives to improve teaching
skills in its curriculum would prepare its graduates for
communication with patients, encourage patient-centered
care, and would be at the forefront of medical education by
applying the guidelines of these national organizations to the
undergraduate setting.
Training medical students in teaching and communication
skills would also be a way to make up for the small amount
of time allowed for communication-skills training during
residency and practice (Hulsman et al. 1999).
3. Medical students with a better understanding of teaching
and learning principles may become better
learners. Residents and faculty, while teaching, might
improve not only their teaching skills, but also their theoretical
knowledge and clinical competence (Darosa 2001). Residents
considered by medical students to be ‘better’ teachers have
been shown to be more effective learners than those evaluated
by students as ‘less effective’, Being an effective learner may
result in these young teachers becoming more knowledgeable
physicians (Apter et al. 1988; Steward & Feltovitch 1988; Busari
& Scherpbier 2004).
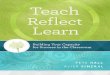
There is evidence in the literature of a ‘teacher–learner
duality’; that is, teaching is linked to learning on the part of the
teacher. The most relevant factors, illustrated in Figure 1,
include social interaction, self-explanation, deliberate practice
with feedback, and metacognition.
The social interactions (or learning context) that teacher–
learners are exposed to are linked to their motivation to learn.
This motivation may be intrinsic or extrinsic: both types seem
to stimulate learning (Sobral 2004). An intrinsically motivated
individual participates in an educational activity because it is
interesting and pleasurable—in other words, for personal
reward. An extrinsically motivated learner does so for an
external reward, for example, better marks, more resources, or
to conform to rules. Learners’ motivation is a complex mixture
of these two types of motivation and is highly dependant on
social and other contexts (Misch 2002). Self-determination
theory argues that intrinsic motivation is directly linked to
autonomy which favours the development of self-awareness
and self-regulation of learning (Ryan & Deci 2000; Sobral
2004). In addition, when medical students are given the
autonomy to choose how they learn, they show better
understanding of complex concepts and humanistic care
(Williams & Deci 1998). In the self-explanation effect, students
asked to explain learning material to themselves or others
demonstrated a better understanding of that material. This is
believed to occur through learners’ detection and repair
of defective mental models (Chi et al. 1994; Chi 2000).
In response to learners’ questions, teachers must generate
sensible self-explanations before offering explanations to their
students, and this self-explanation stimulates further learning
on the part of the teacher. Deliberate practice with feedback
has been shown to lead to learning (Ericsson et al. 1993;
Issenberg et al. 2005). Teaching can be seen as the deliberate
practice of a thinking or procedural skill. ‘Deliberate’ implies
that effort and time is spent on developing the skill: this is
critically dependent on motivation to persist at it. For the
student teacher, feedback is added to deliberate practice when
the student teacher, in formulating explanations, realizes that
his or her understanding of previously learned concepts is not
as solid or coherent as previously believed.
Self-awareness, or metacognitive awareness, is the ability to
reflect on and accurately assess one’s own attitudes, skills, and
knowledge (Gregory 1998; Paris and Winograd 1998). While
teaching others, self-awareness involves reflection about what
learning strategy one should use and how to use it (Collins
et al. 1991). The medical trainees aware of this teaching
process may modify their own learning behaviour to adapt to
their own learning needs.
Thus, teaching can stimulate further learning by the
teacher, because teaching involves an interplay of
three processes: metacognitive awareness; deliberate practice
“To teach is to learn twice”—theoretical mechanisms.
Social interaction(Intrinsic–extrinsic motivation balance)
Teacher self-awareness and self-regulation (metacognition)
Deliberate practice with feedback
Teacher self-explanation(repairing mental models)
Teacher teaching
Teacher learning
Figure 1. ‘To teach is to learn twice’—theoretical
mechanisms.
Medical students learning how to teach
561
Med
Tea
ch D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
B W
uerz
burg
on
10/2
9/14
For
pers
onal
use
onl
y.

with feedback; and self-explanation. These three are all linked
to each other and, as a group, can be stimulated or inhibited by
motivation provided by social interactions and context. Hence,
according to education theory, motivated medical students
learning about and applying teaching principles may become
more active participants in their own learning process.
Putting this concept into practice, it has been shown that
formal teaching responsibility improves residents’ knowledge
acquisition more than self-study or attending lectures
(First et al. 1992). Studies suggest that residents perceive
that teaching medical students (whether preparing lectures,
stimulating students’ critical thinking, or reflection on
knowledge) is beneficial for their own learning (Apter et al.
1988; Busari et al. 2002). A trend has been demonstrated for
residents rated as better teachers by students to perform better
on in-training examination scores (Seely 1999). The process of
preparing to teach may help them organize and solidify their
knowledge (Bensing et al. 2000).
What to include in a program to improve theteaching skills of medical students
1. General principles. There are several principles derived
from medical-student communication-skills education that can
be applied to a TSIP (Laidlaw et al. 2002). First, this program
should integrate teaching skills with other abilities, such as
communication skills. It should focus on and adapt to skills
that medical students have already acquired or will require
at that point of their training. Second, the program should
be supported and taught outside the classroom setting.
This allows opportunities for the application and practice of
teaching skills, as well as appropriate acknowledgment,
feedback, reward, and evaluation of the desired behaviours
and skills in the clinical setting. Third, a teaching
skill improvement effort should extend from pre-clinical
training through clerkship, and ideally even into residency.
A TSIP spread over a four- or five-year curriculum would make
the sequential introduction of concepts easier and would allow
for a better continuity than a few unrelated teaching
improvement activities.
As Collins et al. (1991) suggest in their influential essay
on cognitive apprenticeship, it is important to consider
sequencing in any teaching activity, in order to structure
learning and to preserve meaningfulness. First, global skills
should be taught before local skills, to allow for the building
of a conceptual map of the target skill or process. Second,
complexity should be increased gradually to construct
a sequence of tasks such that more and more of the skills
and concepts necessary for expert performance are acquired.
Third, progressively increasing diversity enables students to
construct a sequence of tasks in which a wider range of
strategies are required. Fourth, teaching skills and the rationale
behind them should be made explicit to those learning them.
Finally, students should practice these teaching skills with
an appropriate balance of support (‘scaffolding’) and
independence (‘fading’) from their supervisors. Students
should be given the opportunity to practice the skills learned
in a ‘real’ setting, e.g. by co-leading small groups, or being
peer tutors for junior students learning procedural skills.
A TSIP should respect these guidelines.
2. Learning Objectives. We suggest several general objec-
tives for a TSIP (Table 2). The literature on resident and faculty
TSIPs was reviewed and objectives were adapted to the
medical student context. Some of these objectives may already
be part of medical school curricula. Most of the rest reflect
modifications of current objectives, based on published
communication skill teaching initiatives (Makoul 2001;
Laidlaw et al. 2002; Stone et al. 2002). Only a few would
likely be new additions to any specific curriculum.
The general objectives of a TSIP should be threefold.
First, such a program should provide medical students with
knowledge about the basic principles of education and
effective teaching. Second, it should improve their education
skills and their appropriate use of teaching strategies, including
self-directed learning. Third, it should aim at changing the
attitudes they may have towards teaching in order for them to
not only recognize the importance of the physician-as-teacher
role, but to also decrease the anxiety they may have about the
teaching responsibilities they will have early in residency.
Content areas can also be derived from the literature.
The content areas that have been defined and used in the past
for resident teaching-skills programs (Snell 2002) should be
appropriate for medical students, with modifications of content
based on the student context. For instance, in medical school,
the students might concentrate on teaching skills that they
would use then, such as leading small groups; in their
preclinical years, they might concentrate on presentation
Table 2. Proposed general and specific learning objectives of a student TSIP.
General objectives Specific objectives
Knowledge about education
and teaching
Outline the principles of adult learning theory and describe
how this applies to teacher-student and physician-patient interactions
List the components of effective teaching
Identify and demonstrate strategies in self-directed
learning to achieve the goal of life-long learningEducation skills and
teaching strategies
Share information effectively with colleagues and patients
Use teaching strategies effectively to facilitate learning
Facilitate self-directed learning in themselves and facilitate
it in the people they are teachingAttitudes towards
teaching
Recognize the importance of their roles as a teacher
Increase satisfaction with teaching and decrease anxiety
about teaching
M. Dandavino et al.
562
Med
Tea
ch D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
B W
uerz
burg
on
10/2
9/14
For
pers
onal
use
onl
y.

skills; and in clinical years, they might concentrate on teaching
in clinical contexts (e.g. at the bedside, hands-on skills).
How to introduce a TSIP into a medical-schoolcurriculum
1. Typical learning activities and strategies. To implement
and integrate a TSIP into a curriculum, it is essential to provide
a consistent, evidence-based framework for teaching and
evaluating teaching skills. On the basis of the content of
current teaching-skills training of residents and the experience
of communication-skills teaching literature, we propose one
model where a TSIP is integrated longitudinally into a typical
medical-school curriculum (Table 3).
A TSIP could and should include a wide range of learning
activities, similar to the current communication-skills training
offered by most medical schools. Some activities could be
formal lectures and small-group discussion about medical
education. Adopting the entirety of this curriculum may seem
a large commitment; however, its introduction could be
sequential and begin by targeted modifications and additions
to existing curricula. We suggest that a ‘core’ minimum would
be to include activities about large-group presentation skills,
small-group discussions, teaching procedural skills, and giving
feedback, each linked to the basic education principles. These
are all areas where the medical student has experience as
a learner, and a potential opportunity to teach peers or more
junior students. Teaching-skills training could be incorporated
into problem-based learning (e.g. how would you explain the
diagnosis to this patient?). Role-play, standardized patients,
and web-based modules could also be used for practice, and
Objective Structured Teaching Exams (OSTE) used for
evaluation (Morrison et al. 2003). Each of the core clinical
rotations could also introduce teaching-skills training specific
to their context.
Moreover, there are many opportunities in the current
medical-education curriculum that could be used to improve
their teaching skills. For example, at the end of a problem-
based learning session, students could be asked to comment
about the discussion that just occurred, and about what were
the low and high learning points, and why. A professor could,
at the end of her lecture, explain the different teaching
strategies she chose to use and why. Students could be asked
to write up or role-play exactly how they would explain
a diagnosis to a patient, and then give feedback on each
others’ performances.
2. Evaluation. As with any other curriculum innovation,
a TSIP should be evaluated, in order to determine program
impact, justify resources, improve the program, and highlight
its importance (Darosa 2001). Ideally, three major types of
evaluation should be conducted: reaction evaluation (whether
participants are satisfied with the program); evaluation of
learning (whether participants know more about education
after training); and evaluation of outcomes (whether partici-
pants now teach better) (Darosa 2001). The first years of
residency may be the best time to assess the impact of a TSIP,
although ongoing evaluation can be performed throughout
medical school.
Reaction evaluation would be conducted to judge the
quality of a TSIP program from the participant’s perspective.
This could be achieved by means of questionnaires or
interviews, for example. Evaluation of learning would
determine the extent of behavioural change that can be
attributed to the program. This could be assessed using an
OSTE with standardized students, self-assessment instruments,
learner feedback, or observation. Lastly, the evaluation of
outcomes would determine the impact the program had on the
environment and whether the programs goals were achieved.
Medical students should have achieved the general objectives
mentioned above. Ideally, the outcome evaluation should
determine whether medical students who have completed
a TSIP have become better teachers, better physicians, and
better learners. However, measuring these outcomes might be
difficult, and a direct link to a TSIP would be difficult to prove.
Therefore, surrogate measures may be more feasible. These
have previously been described by Darosa (2001). For
example, evidence of new educational initiatives, enhanced
learning environments, and enhanced patient education could
be the result of the positive impact of a TSIP.
Table 3. Sample longitudinal student TSIP.
Learners Teaching-program focus Methods Student evaluation
Preclinical
years
Principles of teaching and learning (e.g. adult
learning, learning styles, learning
environment)
Formal lectures, small group tutorials,
teaching-skills techniques incorporation
into problem-based learning clinical cases
Questions about principles
in written exams
Developing core teaching skills (e.g. presenta-
tion skills, leading small-group discussions)
Small group tutorials, didactic material,
role-play, feedback, and practice with
standardized patients or students
Objective Structured
Teaching Exam (OSTE)
Clinical
years
Consolidating core principles & teaching skills
learned
Small group sessions, plus didactic material via
self-study or web based modules
Ongoing observation,
of teaching skills
included in evaluations
at the end of each core rotation
evaluationClinical teaching skills (e.g. one-one-one
tutoring, teaching in specific clinical con-
texts, teaching procedural skills, giving
feedback)
Context appropriate for each of the core
rotations (e.g. learning how to teach proce-
dural skills in a surgical rotation)
All years In-depth study and practice of one or more of
the aspects described above
Elective in medical education Elective evaluation form,
assessing if specific
goals of elective achieved.
Medical students learning how to teach
563
Med
Tea
ch D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
B W
uerz
burg
on
10/2
9/14
For
pers
onal
use
onl
y.

Conclusion
The literature provides several reasons why we should train
future physicians to be teachers as early as medical school.
Teaching, as with other forms of patient–physician commu-
nication, is a core clinical skill that requires ongoing training,
practice, and feedback throughout the medical-education
continuum (Makoul 2001). Medical students recognize the
importance of receiving training in teaching skills. They feel
uncomfortable taking on teaching responsibilities without
formal preparation, and this adds to the anxiety associated
with beginning residency.
The few published studies about instructing medical
students in how to teach suggest positive outcomes are
associated with these curriculum innovations. There is,
however, a need for more data in this area. Whether or not
incorporating teaching skills programs into undergraduate
medical curricula leads to better development of professional
values and behaviour are issues that have yet to be addressed.
Educational theory, published studies of residents’ TSIPs,
and the few available studies of students’ TSIPs all support the
implementation and evaluation of organized, longitudinal
programs throughout medical school to improve students’
teaching skills. These programs have the potential to help
graduates be better teachers, better learners, and better
physicians.
Acknowledgements
The authors would like to thank Dr Y. Steinert and
Dr P. McLeod for their useful insights and comments.
Notes on contributors
MYLENE DANDAVINO, MDCM, BSc, MSc, is a fourth-year Chief Resident
in general pediatrics at the Montreal Children’s Hospital, McGill University.
This paper is the result of a medical education elective she did as a final-
year student.
LINDA SNELL, MD, MHPE, FRCP, RACP, is a general internist and medical
educator at McGill University.
JEFFREY WISEMAN, MD, MAEd, FRCP, is a general internist and medical
educator at McGill University.
References
Apter A, Metzger R, Glassroth J. 1988. Residents’ perceptions of their role as
teachers. J Med Educ 63:900–905.
Bardach NS, Vedanthan R, Haber RJ. 2003. ‘Teaching to teach’: enhancing
fourth year medical students’ teaching skills. Med Educ 37:1031–1032.
Barrow MV. 1966. Medical student opinions of the house officer as a
medical educator. J Med Educ 41:807–810.
Bensing JM, Verhaak PF, van Dulmen AM, Visser AP. 2000.
Communication: the royal pathway to patient-centered medicine.
Patient Educ Couns 39:1–3.
Bing-You RG, Harvey BJ. 1995. Factors related to residents’ desire and
ability to teach in the clinical setting. Teach Learn Med 3:95–100.
Bing-You RG, Sproul MS. 1992. Medical students’ perceptions of
themselves and residents as teachers. Med Teach 14:133–138.
Bing-Your RG, Tooker J. 1993. Teaching skills improvement programmes in
US internal medicine residencies. Med Educ 27:259–265.
Bordage G, Lemieux M. 1991. Semantic structures and diagnostic thinking
of experts and novices. Acad Med 66:S70–S72.
Bordley DR, Litzelman DK. 2000. Preparing residents to become more
effective teachers: A priority for internal medicine. Am J Med
109:693–696.
Busari JO, Prince KJ, Scherpbier AJ, van der Vleuten CP, Essed GG. 2002.
How residents perceive their teaching role in the clinical setting: a
qualitative study. Med Teach 24:57–61.
Busari JO, Scherpbier AJ. 2004. Why residents should teach: A literature
review. J Postgrad Med 50:205–210.
Busari JO, Scherpbier AJ, van der Vleuten CP, Essed GG. 2003. The
perceptions of attending doctors of the role of residents as teachers of
undergraduate clinical students. Med Educ 37:241–247.
Cegala DJ, Lenzmeier Broz, S. 2002. Physician communication skills training:
A review of theoretical backgrounds, objectives and skills. Med Educ
36:1004–1016.
Chi M. 2000. Self-explaining expository texts: The dual processes of
generating inferences and repairing mental models, in: R. Glaser (Ed.)
Advances in Instructional Psychology: Educational Design and
Cognitive Science (New Jersey, Lawrence Erlbaum Associates).
Chi MTH, Leeuw ND, Chiu M-H, Lavancher C. 1994. Eliciting
self-explanations improves understanding. Cog Sci 18:439–477.
Collins A, Brown JS, Holum A. 1991. Cognitive apprenticeship: making
thinking visible. Am Educ 6:38–46.
General Medical Council, 2003. Tomorrow’s doctors: recommendations on
undergraduate medical education. Available at: http://www.gmc-uk.
org/education/undergraduate/tomdoc.pdf (accessed 12 June 2007).
Craig JL, Page G. 1987. Teaching in medicine: an elective course for
third-year students. Med Educ 21:386–390.
Darosa DA. 2001. Residents as teachers: evaluating programs and
performance, in: J. Edward, J. Friedland & R. Bing-You (Eds),
Residents’ Teaching Skills (New York, Springer).
Ericsson KA, Krampe RT, Tesch-Romer C. 1993. The role of deliberate
practice in the acquisition of expert performance. Psycholog Rev
100:363–406.
First LR, Lauerman R, Fenton T, Herzog L, Snyder JD. 1992. Learning by
teaching. A resident-taught oral therapy program for acute diarrhea.
Clin Pediatr (Phila) 31:602–607.
Frank JR, Jabbour M, Frechette D, Marks M, Valk N, Bourgeois G. 2005.
Report of the CanMEDS Phase IV Working Groups (Ottawa, The Royal
College of Physicians and Surgeons of Canada).
Hulsman RL, Ros WJ, Winnubst JA, Bensing JM. 1999. Teaching clinically
experienced physicians communication skills. A review of evaluation
studies. Med Educ 33:655–668.
Issenberg SB, McGaghie WC, Petrusa ER, Lee Gordon D, Scalese RJ. 2005.
Features and uses of high-fidelity medical simulations that lead to
effective learning: a BEME systematic review. Med Teach 27:10–28.
Kurtz S, Silverman J, Benson J, Draper J. 2003. Marrying content and
process in clinical method teaching: enhancing the Calgary-Cambridge
guides. Acad Med 78:802–809.
Kurtz SM. 2002. Doctor–patient communication: principles and practices.
Can J Neurol Sci 29:(Suppl 2) S23–S29.
Laidlaw TS, MacLeod H, Kaufman DM, Langille DB, Sargeant J. 2002.
Implementing a communication skills programme in medical school:
Needs assessment and programme change. Med Educ 36:115–124.
Makoul G. 2001. Essential elements of communication in medical
encounters: The Kalamazoo consensus statement. Acad Med
76:390–393.
McKeachie WJ, Svinicki M. 2006. McKeachie’s Teaching Tips: Strategies,
Research, and Theory for College and University Teachers (Boston,
Houghton Mifflin).
Misch DA. 2002. Andragogy and medical education: Are medical students
internally motivated to learn? Adv Health Sci Educ Theory Pract
7:153–160.
Morrison EH, Hafler JP. 2000. Yesterday a learner, today a teacher too:
residents as teachers in 2000. Pediatrics 105:238–241.
Morrison EH, Lewis EM, Gabbert CC, Boker JR, Kumar B, Harthill M. 2003.
Evaluating a ‘service elective’ in clinical teaching for medical students.
Med Teach 25:662–663.
Moseley TH, Cantrell MJ, Deloney LA. 2002. Clinical skills center attending:
an innovative senior medical school elective. Acad Med 77:1176.
Nestel D, Kidd J. 2002. Evaluating a teaching skills workshop for medical
students. Med Educ 36:1094–1095.
M. Dandavino et al.
564
Med
Tea
ch D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
B W
uerz
burg
on
10/2
9/14
For
pers
onal
use
onl
y.

Paiva RE, Kienzler LM, Anderson MB. 1982. Preparation for the teaching
role in residencies: An elective for medical students. J Med Educ
57:792–794.
Paris SG, Winograd P. 1998. The role of self-regulated learning in contextual
teaching: Principles and practices for teacher preparation: Preparing
Teachers to Enhance Student Success in the Workplace and Beyond
ERIC Document Reproduction Service No: ED 427263. Accessed
21 July 2007. Available from http://www.eric.ed.gov/ERICDocs/
data/encdocs2sql/content_storage.01/0000019b/80/17/4e/54.pdf. In
Contextual Teaching and Learning Group on Educational Affairs,
Association of American Medical Colleges. AAMC GME Core
Curriculum Project: Draft for comment, Washington, DC, Association
of American Medical Colleges, 1999.
Pasquale SJ, Pugnaire MP. 2002. Preparing medical students to teach. Acad
Med 77:1175–1176.
Roter D. 2000. The enduring and evolving nature of the patient-physician
relationship. Patient Educ Couns 39:5–15.
Ryan RM, Deci EL. 2000. Self-determination theory and the facilitation of
intrinsic motivation, social development, and well-being. Am Psychol
55:68–78.
Schrow G. 1998. Promoting general metacognitive awareness. Instr Sci
26:113–125.
Seeley AJE. 1999. The teaching contributions of residents. Can Med Assoc J
161(10):1239.
Snell L. 2002. Planning and implementing a teaching-skills improvement
program for residents. J. Edward, J. Friedland & R. Bing-You (Eds),
Residents’ Teaching Skills (New York, Springer).
Sobral DT. 2004. What kind of motivation drives medical students’ learning
quests? Med Educ 38:950–957.
Steinert Y, Mann K, Centeno A, Dolmans D, Spencer J, Gelula M,
Prideaux D. 2006. A systematic review of faculty develop-
ment initiatives designed to improve teaching
effectiveness in medical education: BEME Guide No. 8. Med
Teach 28:497–526.
Steward DE, Feltovitch PJ. 1988. Why residents should teach: the parallel
processes of teaching and learning, in: JC. Edwards & RL. Marier (Eds),
Clinical Teaching for Medical Residents: Roles, Techniques, and
Programs (New York, Springer).
Stone S, Ellers B, Holmes D, Orgren R, Qualters D, Thompson J. 2002.
Identifying oneself as a teacher: the perceptions of preceptors. Med
Educ 36:180–185.
Tacci JA. 1998. The resident as teacher: a neglected role. J Am Med Assoc
280:934.
Topping KJ. 1996. The effectiveness of peer tutoring in further and higher
education: a typology and review of the literature. High Educ
32:321–345.
Williams GC, Deci EL. 1998. The importance of supporting autonomy in
medical education. Ann Intern Med 129:303–308.
Wipf JE, Orlander JD, Anderson JJ. 1999. The effect of a teaching skills
course on interns’ and students’ evaluations of their resident–teachers.
Acad Med 74:938–942.
Wipf JE, Pinsky LE, Burke W. 1995. Turning interns into senior residents:
Preparing residents for their teaching and leadership roles. Acad Med
70:591–596.
Medical students learning how to teach
565
Med
Tea
ch D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
B W
uerz
burg
on
10/2
9/14
For
pers
onal
use
onl
y.